Embed Size (px)
Citation preview
187CT
CEDirected Reading
This article is a Directed Reading. Your access to Directed Reading quizzes for continuing education credit is determined by your membership status and CE preference.
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
Within a year of the develop-ment of the world’s first whole-body computed tomography (CT) scanner,
physicians performed the first CT-guided interventional procedure.1 Studies that followed linked CT-guided percutaneous drainage and biopsy pro-cedures to better patient outcomes and reduced cost when compared with sur-gery.1-5 Demand for interventional radi-ography procedures increased, and CT-guided percutaneous abscess drain-age (PAD) evolved from an experimen-tal treatment into a standard protocol for drainage of intra-abdominal abscesses.1 Because CT technologists play a vital role in assisting the physi-cian and patient, the need for technolo-gists with the knowledge and skills essential to CT-guided abscess drainage procedures has increased.2
An abscess is an encapsulated col-lection of purulent (infected) material resulting from a failed attempt by the body to kill organisms in a concen-trated area.1 This focused response
is significant because it might not be possible to visualize an infection with CT imaging before the formation of an abscess.1 Fluid collections that respond the most favorably to PAD are well-defined, confined to a single compart-ment, filled with low-viscosity fluid, and easily accessible.2 Intra-abdominal abscesses can be intraperitoneal, ret-roperitoneal, or visceral and are typi-cally categorized by their anatomical location.3 If left undrained, abdominal abscesses have a high risk for fatality.3 Before CT was introduced to diagnose and guide drainages of intra-abdominal abscesses in 1975, patients were dying from undiagnosed and untreated abscesses.1,4,5 Mortality rates ranged from 45% to 100% depending on location and origin of the abscess.3
Intra-abdominal abscesses formerly required open surgical intervention.6 While effective, open surgery is inva-sive and requires general anesthesia.1 Patients must be stable enough to tolerate surgery, and the underlying factors contributing to the abscess
After completing this article, the reader should be able to:Describe the common locations and pathological origins of intra-abdominal abscesses.Discuss factors that influence the choice of guidance modality.List typical procedural steps for CT-guided drain placement.Explain procedural indications and contraindications.Discuss complications of drain placement.Describe topics for further research about CT-guided abscess drainage.
Intra-abdominal abscesses arise from complications of surgery and disease. Computed tomography (CT) facilitates abscess drainage procedures while reducing the risks and costs associated with surgery. These procedures require collaboration to ensure positive patient outcomes. To perform their role in CT-guided intra-abdominal abscess drainage, radiologic technologists must understand patient care, instrumentation, imaging techniques, and underlying disease processes specific to the anatomical site. Once these considerations are grasped, CT technologists can help radiologists and administrators to determine cost-effective instrumentation and quality control specific to the patient and institution.
Benjamin W Roberts, MFA, R.T.(R)(T)(CT)
CT-guided Intra-abdominal Abscess Drainage

188CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
CT-guided Intra-abdominal Abscess Drainage
drainage procedures, including studies that compared ultrasonography with CT guidance procedures and various drainage instrumentation.5 The literature sur-rounding early development of the procedure reveals lively debates between surgeons and interventional radiologists, as well as debates among interventional radiologists about techniques.1,10 As CT technology progressed, an increasing number of studies concluded that CT images of intra-abdominal abscesses were more accurate and detailed and provided greater tissue depth than ultrasonography with the added advantage of delineating f luid collections from nearby structures.3,11-13 CT emerged as the modality of choice for drainage of intra-abdominal abscesses.1,3 The ongoing development of CT-guided drain placement procedures is motivated by improved patient outcomes and the pioneering efforts that have informed radiology practice since the discovery of x-rays.1
PAD has had a significant positive impact on patient care, but the procedures are expensive.14 The costs of medical radiography have risen faster than overall medical costs, and studies have reported that medical imaging costs are rising faster than overall inflation of the gross domestic product or worker wages.14,15 To determine whether these expenses correspond to better value and standards of patient care, researchers evalu-ated improvements in technology, best practices, and patient outcomes.14 Value assessments of PAD must analyze numerous variables, including1,3,14: Effectiveness. Efficiency. Diagnosis. Whether the department is physician owned or
hospital owned. Patient population. Quality. Safety. Setting.A survey of medical imaging costs in North Carolina
found that diagnostic imaging accounted for 9.7% to 11.5% of the total per-member-per-month medical expenses from 2005 through 2013.14 Specialty modali-ties such as CT, magnetic resonance imaging, and positron emission tomography with CT accounted for more than 50% of the costs during the 8-year period.14
can complicate the operation.1 With the advent of CT-guided drainage procedures, more patients who could tolerate surgery were referred to the imaging department.6 Since 1995, the Society of Cardiovascular and Interventional Radiography has recommended percutaneous drainage of infected f luid collections as a minimally invasive alternative to surgical drain-age.7 PAD is considered standard treatment for intra-abdominal abscesses, and a review of the literature revealed a wide array of outcomes.6
During PAD procedures, detailed, real-time CT images guide the placement of a small catheter into the abscess, through which the purulent material can be drained and antibiotics administered.1 Real-time CT imaging can include CT-fluoroscopy, conventional CT, or a combination of both depending on the institution, physician, and technologic factors. Success rates for PAD range from 27% to 93%, indicating a need for meticulous technique and accurate CT-guided needle placement.6
HistoryCT-guided percutaneous drainage grew from the
fusion of CT imaging with percutaneous catheterization procedures first developed for angiography.6 In 1953, Sven-Ivar Seldinger, MD, introduced a technique for arterial catheter insertion assisted by a f lexible metal guidewire, which still is widely used.8 Two decades after Seldinger’s work, the first diagnostic CT scan was performed on a patient using a brain scanner developed by Godfrey Hounsfield.1,2,9 The diagnostic power of CT was apparent, and a year later, in 1974, Robert Ledley, DDS, developed the first whole-body CT scanner at Georgetown University.9 As health care providers recog-nized the life-changing significance of CT imaging, the number of CT scanners installed worldwide increased.2,9
Building on early success with CT-guided lung biopsies, John R Haaga, MD, and colleagues modified Seldinger’s angiography technique to accommodate CT-guidance of needle aspiration and drainage proce-dures at Cleveland Clinic and Case Western Reserve School of Medicine.1,4 They published their findings in 1977 and concluded that CT was valuable for detecting and guiding drainage of intra-abdominal abscesses.4 Haaga et al’s study came at the beginning of an explo-sion of research into interventional, or percutaneous,

189CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
Roberts
postoperative septic complications and increased the overall mean length of stay in the hospital (15.8 days vs 12.2 days).22 Another study reported that performing PAD before surgery resulted in a lower rate of post-operative complications and ultimate stoma creation compared with the surgery-only group.21 Conflicting study results and the complex nature of disease pro-cesses make determining cost-effective best practices for treatment of intra-abdominal abscesses impossible to generalize.
Nevertheless, individual and institutional cost con-siderations such as time, resources, education needs, efficiency standards, and patient care variables often guide clinical decisions related to CT-guided proce-dures.1 Therefore, to perform their role in CT-guided intra-abdominal abscess drainage, radiologic technolo-gists must understand patient care, imaging techniques, and underlying disease processes specific to the ana-tomical site. Once these considerations are grasped, CT technologists can assist radiologists and administrators to determine cost-effective instrumentation and quality control specific to the patient and institution.1,3
Anatomy and Pathophysiology Liver
The liver is the largest organ in the abdomen; it is highly vascularized and lies predominately in the upper right quadrant, partially enclosed by the ribs.23,24 Normal Hounsfield units range from 38 HU to 80 HU on noncontrast-enhanced images, but within an indi-vidual patient, the range is narrow, having a uniform appearance on CT.2,23 As a result of the liver’s homog-enous appearance, the radiologist might request intrave-nous (IV) contrast administration to aid abscess local-ization.1,2 Depending on the abscess location, the ribs, the liver’s proximity to the diaphragm and lungs, and patient movement during breathing can be obstacles to catheter placement.1,3 Therefore, care is needed to prevent puncturing the lungs during PAD procedures.1 The CT technologist assisting with percutaneous liver drainage procedures must be able to differentiate between f luid in the lung and superior liver abscesses on CT images. Other skills required for percutaneous liver drainage procedures include gantry angulation, contrast administration, and patient immobilization.1,3
The North Carolina figures are consistent with national data collected by the American College of Radiology, which reports that the costs of medical imaging account for 10% of all U.S. health care costs.16
Nevertheless, gaps exist in the literature surround-ing value assessments between PAD and surgery. For example, the Patient-Centered Outcomes Research Institute was established by the Patient Protection and Affordable Care Act to address questions of compara-tive treatments’ effectiveness, but it has no mandate to study cost effectiveness.17 In addition, physicians and patients also focus on the choice of treatment rather than on cost. One study reported that only 36% of physicians believe they have a “major responsibility” to reduce health care costs,18 and another study indicated that most patients are unwilling to consider costs when making medical decisions for themselves.19
Individual institutions must balance these discrep-ancies against their own costs in time, education, and available resources.1 Busy radiology departments might find it difficult to allocate the equipment and human resources required for a special procedure schedule, and radiologists might need to reduce their diagnostic work-load to perform time-consuming patient procedures.1 Institutions also must weigh education costs for staff and physicians, and innovations in teaching technol-ogy can provide creative and cost-effective responses to education concerns.1,2,20 For example, one group of researchers developed open source software called the Image-Guided Surgery Toolkit, which when used with a Web camera and an anatomic phantom constructed from LEGO blocks, provides hands-on physician train-ing for CT-guided navigation.20
Another factor in accurately understanding the costs of PAD and comparing interventional radiology proce-dures with surgical alternatives relates to the sampled patient population and underlying disease processes. For example, some debate exists whether PAD should be used to treat Crohn disease−related intra-abdominal abscesses.21,22 Because of the disease process, surgery is seldom avoided.21 Questions persist as to whether preoperative percutaneous drainage of Crohn disease−related abscesses could decrease the rate of sepsis or the need for stoma creation.21 One study concluded that preoperative PAD did not decrease the rate of

190CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
CT-guided Intra-abdominal Abscess Drainage
differentiation between the head of the pancreas, the small bowel, and the stomach.2
Pancreatic abscesses can result from secondary infections of pancreatic phlegmon or from pseudocysts associated with pancreatitis.3 Pancreatic phlegmon is a spreading inflammation of tissue containing areas of necrosis.3 Pseudocysts develop early in acute pancreatitis as unencapsulated fluid collections.3 Contrast-enhanced CT can aid differentiation in the origins of pancreatic f luid collections.2 Percutaneous drainage of pancreatic abscesses and pseudocysts remains an area of controver-sy in the literature, and success depends on case-specific details such as location, number of f luid collections, and fluid viscosity.25 Consequently, researchers have suggested computationally estimating parameters for percutaneous drainage of acute pancreatitis to further assist grading or scoring pancreatic abscesses for assess-ment by the multidisciplinary team of interventional radiologists, interventional endoscopists, and surgeons dedicated to management of acute pancreatitis.25
SpleenThe spleen lies in the left upper quadrant, partially pro-
tected by the left lower posterior ribs.24 Its superior surface abuts the left hemidiaphragm, and the organ is surround-ed by the peritoneum.23 Accessory spleens are a normal anatomical variant, ranging in size from a few millimeters to several centimeters and having identical attenuation values and contrast enhancement to a normal spleen.1 CT has a sensitivity of 96% in the diagnosis of splenic abscess.3 IV contrast is required to enhance abscesses of the spleen and distinguish an abscess from a splenic infarct.1 With appropriate injection techniques and timing, peak splenic attenuation values reach 100 HU to 150 HU during the arterial phase, but the values fall to 60 HU to 100 HU during the venous phase, making the attenuation values of the spleen closer to those of the liver.23
Splenic abscess is a rare condition with an autopsy incidence of 0.14% to 0.70%.3 However, the worldwide incidence is increasing because of an increasing number of immunocompromised patients.1 Causes of splenic abscess include bacterial endocarditis, complications of sickle cell disease, AIDS/HIV, and trauma.3 Research on percutaneous drainage of splenic abscesses identi-fies a number of contraindications to PAD, including
Liver abscesses form when infection is not cleared by the organ’s initial inf lammatory response.13 These infections are usually fatal if left untreated.13 Causes of pyogenic liver abscesses include surgery, trauma, cancer, biliary tract disease, or bacteremia resulting from a compromised immune system.3,13 Depending on the conditions and origins, the liver can form a single abscess or multiple sights of infection.3 Researchers who compared single-site and multiple-site infections have concluded that single-site liver abscesses mostly originate in the crypt cells of the liver, and Klebsiella pneumoniae is the main bacterium isolated.14 Multiple-site liver abscesses usually origi-nate in the biliary system, and Escherichia coli is the leading microorganism.14
Understanding these distinctions might aid imag-ing guidance and patient positioning as well as provide protocols for IV contrast administration during the drainage procedure. As with most abscesses, liver abscesses are best drained by the shortest route possi-ble.1 Depending on the location of the abscess, the radi-ologist might require help from the patient, instruct-ing him or her to suspend respiration as the needle is advanced.1 Access routes must be planned to avoid the pleural space, hepatic vessels, and gallbladder.1
PancreasThe pancreas extends across the abdomen imme-
diately posterior to the stomach within the retroperi-toneum at the level of the kidneys.23,24 The organ can assume several basic shapes, but the most common is a tapered wedge in which the head of the pancreas is larger than the tail.24 The size, shape, and specific loca-tion are unique to each patient.2 CT is the modality of choice for imaging the pancreas.2 The organ has a distinct feathery appearance on CT, roughly 30 HU to 50 HU.23 CT scans of patients with acute pancreatitis can demonstrate altered pancreatic density, duct dilata-tion, pancreatic edema, or f luid collections.23 Because it can be difficult to differentiate the pancreas from the duodenum, the radiologist might request oral contrast administration.2,3 Positive oral contrast can obscure the presence of calculi common to chronic pancreatitis.2 Therefore, using a negative oral contrast such as water as well as rapid administration of IV contrast can aid

191CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
Roberts
nutrients and expels waste.24 The abdominopelvic por-tions of the alimentary canal are the stomach, small intestine, large intestine, and rectum.24 The abdomen comprises many interrelated systems working together, and organs related to accessory function include the liver, gallbladder, and pancreas.24 The large intestine travels from the cecum to the ascending, transverse, descending, and sigmoid colon, and then from the rectum to the anus.24 The vermiform appendix marks a critical divergence in the passage of the alimentary canal and is a possible site of infection.24 The axillary passage descends from the cecum inferior to the termi-nus of the ileum at the ileocecal valve.24
Enteric abscesses, pockets of infection within the abdominopelvic alimentary canal, are most often related to disease processes of the large intestine.3 As in Crohn disease, percutaneous drainage of infec-tious pockets created by disease processes of the colon seem to play a temporizing role in treatment—a tem-porary course of action, conforming to the needs of circumstance—before definite surgical intervention.3 Other abscess-forming infectious processes of the large intestine include appendicitis and diverticulitis.3 Nevertheless, abscesses can occur as complications of infection, secondary complications of surgery, or as separate spontaneous processes (eg, Crohn disease).3 In abscesses related to enteric processes, CT guidance pro-vides the necessary visualization of f luid collections in relation to neighboring bowel to avoid traversing bowel loops with the drainage catheter.10 The radiologist might require the technologist’s assistance positioning the patient on the scan table to avoid traversing loops of bowel while accessing the abscess.1
Musculoskeletal SystemThe intra-abdominal muscles of primary concern
for abscess formation are those that combine to form the iliopsoas compartment, namely the psoas major and iliacus muscles.27 The superior portion of the psoas muscles attach to the lateral surfaces of T12 through L5 vertebrae, supporting the spinal column.24 As the name suggests, the iliacus muscles originate in the iliac fossa of the pelvis.24 The psoas major unites with the iliacus at the level of the inguinal ligament to cross the hip joint and connect with the femur at the lesser trochanter.24
multilocular abscesses, septations, and abscess rupture with bleeding.25
KidneysKidneys are approximately as long and wide as a
human fist (4.5 in 3 in, and ~1.25 in thick).24 The right kidney often is longer and narrower than the left, and because of their position in relation to the liver, the right kidney is lower than the left. The kidneys are suspended by retroperitoneal connective tissue at the level of the third lumbar vertebra. Each kidney is rotated about 30° anteriorly toward the aorta along its long axis.24 The kidneys are enveloped in perinephric fat encased in a dense connective tissue sheath, or renal fascia.23 The organs are composed of fatty tissue con-taining lymphatics, arteries, veins, nephron cells unique to the kidneys, and a drainage system composed of the renal pelvis and calyxices.23
Renal abscess is highly correlated to underlying renal disease with predisposing conditions, including nephro-lithiasis, hydronephrosis, and septicemia.3,26 They might rupture externally or internally, presenting as a peri-nephric abscess or draining into the collecting system respectively.3 CT is currently the modality of choice for renal evaluation.2 Patients are generally positioned prone on the examination table to permit approaching the renal abscess while avoiding spinal erector muscles, the small bowel, colon, liver, and spleen.1 PAD is an effective treatment for renal and perinephric abscess, but in cases of urinary obstruction caused by renal cal-culi or tumor, the physician might perform a percutane-ous nephrostomy for increased access.3 Percutaneous nephrostomy is similar to PAD with 3 general excep-tions1: Once the collecting system is penetrated, a small
sample of f luid is aspirated for culture. A small amount of low-osmolality contrast media
(LOCM) is injected through the same needle to allow direct visualization.
A nephrostomy catheter is placed within the renal pelvis, not the abscess.
Digestive SystemDigestion works as accessory glands secrete enzymes
into the alimentary canal, which in turn absorbs

192CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
CT-guided Intra-abdominal Abscess Drainage
to confirm and document that no adjacent uninvolved anatomy was damaged by the procedure.1
Versatility or scanning flexibility is an added advan-tage of CT-guidance.1 Scanner tables allow for flexibility in patient positioning, entry point selection, needle direc-tion, and instrumentation.1,2 Flexibility of patient posi-tioning can aid patient comfort, which is critical for coop-eration during the procedure.2 The flexibility of entry point selection can allow the patient to lie in a prone, lateral, or supine position.1,3 In addition, CT imaging is not hampered by extra pillows under the head, back, or knees.1 Changing patient position seldom creates a change in image quality.1,2 An added benefit of changing patient position is that anatomy shifts accordingly, which might permit better pathways for the needle.1,3
Use of ionizing radiation is the primary disad-vantage of CT guidance.1 For example, in 2006, CT examinations made up 15% of all radiologic examina-tions in the United States, and yet CT accounted for 50% of the total medical imaging radiation exposure.29 These numbers appear to be on the rise, with a 10% annual increase in CT use in the United States.29 This data is particularly alarming when considered in the light of recent studies indicating that 0.5% to 3% of all cancer cases could be linked to medical radiation exposure.30-32 Consequently, radiation exposure from CT examinations has come under public scrutiny, and
The iliopsoas muscles combine their efforts to support the skeleton while standing, walking, and running.24
Abscess of the iliopsoas compartment can originate from surgery, trauma, or through infection from spinal osteomyelitis, tuberculosis (TB), renal infection, or inflammatory bowel disease.27 Vertebral involvement of pyogenic iliopsoas abscess is rare in all cases except tuberculous abscess, and in the past, patients with iliopsoas tuberculous abscess were treated operatively even though surgery was associated with a 40% fail-ure or recurrence rate.28 Percutaneous drainage under CT-guidance evolved as a safe and effective alternative.27
Considerations CT technology measures the attenuation of an x-ray
beam by all natural and artificial materials within the human body, reconstructing the measurements in a wide array of 2-D, 3-D, or even 4-D representations.2 CT is sensitive to subtle differences in material den-sity.2,3 By pairing a wide array of images with imag-ing sensitivity, CT allows a great deal of versatility in percutaneous drainage instrumentation.1 IV contrast administration can delineate vascularity, anatomic space, or an abnormal structure.2,3 Longitudinal CT scans (eg, topograms, scouts) can simulate conventional radiographs, assisting visualization of instruments dur-ing insertion or manipulation, and CT-fluoroscopy pro-vides real-time imaging of small mobile masses, breath-ing, or abnormalities.1
The accuracy of CT-guidance relates to the geo-metric representations of both the needle and the anat-omy.1 CT images allow for needle localization in the planes of the x, y, and z axes as illustrated in Figure 1.1 Measurements of angles and depth can be made in all 3 dimensions by considering both the information on the image and the table position.1,2 The precision of these measurements is less limited by the machine than it is by the manual dexterity of the physician and accuracy of the imaging technologist.1 Three-dimensional guid-ance is a definite advantage of CT over f luoroscopy and ultrasonography.1,3,6 In complex procedures, such as drainages of the rectum or psoas muscles, 3-D recon-structions and sagittal or coronal views can be created.1 Accurate needle placement is critical for complete drainage.1,3 CT allows for postplacement assessment
y
x
z
z
yx
Figure 1. During localization, the x and y axes are determined by the computed tomography (CT) images, and the z axis measure-ments are related to table position.

193CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
Roberts
essential during percutaneous procedures; therefore, technical excellence and mutual respect are critical to successful patient outcomes.2
Preprocedure TasksThe procedure room should be prepared before the
patient arrives in the department.2 Cleanliness is essen-tial.1 The technologist should: Disinfect the CT gantry, scan table, and tray
tables.2
Inspect the room for potential contaminates.2 Verify enough lead aprons are available for the
physician, staff, and patient.1
Confirm all lead aprons are clean and free of any defects.1
Check the availability of gloves, emesis basins, sample cups, and suction supplies.2
Ensure a metallic skin marker and skin marking are pen available for localization.2
Prepare the procedure tray while maintaining the sterile field (see Box).2
Drainage needles are expensive, and the radiologist should choose the needle.1,3 Technologists should wait until the interventional radiologist is ready for needle insertion to open the sterile packaging to avoid waste.2
Once the room and instruments are prepared, the technologist should warm up the scanner and con-firm that daily calibrations have been completed to ensure consistent and reliable scanner performance.2,9 It might be necessary to free disk space on the scan-ner computer; some CT f luoroscopy protocols fail to initiate if disk space is exceeded, leaving the tech-nologist to troubleshoot a computer error during the procedure.2,9 It also is important to review the patient’s medical record for the necessary laboratory studies and patient preparation orders.1,2 As a final step, the technologist should communicate with the patient’s attending nurse or physician to coordinate care.2 Use of a checklist to prep the room ahead of the patient’s arrival can help avoid potential problems, freeing the technologist to focus on patient care.
The technologist must establish a good first impres-sion to gain the patient’s trust and accommodate his or her needs.2 Quality patient care begins with good communication.2 Customer service initiatives can
the government has responded with regulations. The Joint Commission recommended increased oversight of quality assurance and dose optimization.33 Although CT-guided PAD accounts for a small percentage of total radiologic examinations, patients could receive higher doses during CT-guided procedures.34 CT technolo-gists must modify protocols to ensure the minimum radiation exposure while maintaining adequate image quality.2
Therefore, technologists must understand the technical factors controlling radiation exposure in the CT suite.2,9 CT exposure is directly proportional to x-ray tube current, the square of the tube voltage, and exposure time.35 Often, CT-guided procedures are per-formed using scanning parameters set for diagnostic imaging.1,36 The CT technologist should discuss these parameters with the radiologist to determine whether high-resolution images are needed for the procedure.1,36 Research by Lucey et al revealed that a reduction of 30 mA in tube current during CT-guided procedures can reduce patient dose 6 to 8 times without compro-mising the success of the procedure.36 In a related study, a reduction in tube voltage to 100 kV with a fixed tube current of 15 mA resulted in a 95% reduction in expo-sure during CT-guided lung biopsies.37 Recent work by Rezazadeh et al determined that increased noise level and reduced voltage did not hinder successful comple-tion of CT-guided percutaneous drainages.38 The results suggested that reducing tube voltage to 80 kV, instead of the conventional 120 kV with automated tube current adjustment allowed adequate image quality in 86% of cases, while reducing dose by 57% to 73%.38
Limiting radiation dose underscores the importance of acting on behalf of the patient and using the modality best suited to achieve favorable results for percutane-ous drainage procedures.2 Improved visualization and instrumentation should guide the choice of modality—not ease or convenience.1 Everyone assisting in these procedures must work together as a team to minimize risk.2 This means recording preprocedure “time outs” and taking necessary precautions to prevent injury, wrongful use, contamination, and misuse of radia-tion.1 Should the physician choose to terminate the procedure, the technologist must support the decision.1 Interprofessional communication and collaboration is

194CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
CT-guided Intra-abdominal Abscess Drainage
technologist must provide the most up-to-date infor-mation on all documentation because improper com-munication can result in error, and the patient’s chart might contain incomplete or incorrect information.1-3 Before the procedure, the technologist should ask the patient about medications that might alter coagulation or platelet function.2 Routine coagulation studies do not detect the presence or activity of platelet inhibitors.1,2 For example, one study of laboratory work for bleeding due to needle biopsy confirmed serious alteration and risk of the coagulation status in patients taking aspirin-like compounds.1
Patients being treated with low-molecular-weight heparin and patients with systemic lupus erythemato-sus require extreme caution.1,2 Methods for assessing the degree of anticoagulation of low-molecular-weight heparin are not readily available at many hospitals, and clinicians might not be aware of the required test.1 Patients with systemic lupus erythematosus can have falsely elevated laboratory values due to the presence of circulating antibodies.1 The ordering physician might assert that there are few risks with such patients and ask that the procedure be performed in spite of the elevated values.1 These situations are difficult because the legal consequences of procedural complications falls on the attending radiologist, not the referring clinical physi-cian.1 When questions about patient coagulation factors arise, one option for the radiologist is to perform a bed-side assessment of bleeding at the entrance site before the procedure continues.1
CT technologists should familiarize themselves with the patient’s history and related imaging examinations to facilitate positioning, scanning, and other technical factors.1,2 They should ensure that the procedure room is free from distractions, that all information is correct, and that documentation is complete and accurate.2 Whenever possible, the attending radiologist should be introduced to the patient.1,2,39 The radiologist will discuss the procedure in depth and answer questions.1 Once the radiologist has reviewed the rationale, alterna-tives, methods, sensations, and postprocedure routine with the patient, family, or legal guardian, the informed consent is signed, and the procedure can begin.1
Patient consent does not always guarantee patient cooperation.1,2 Lack of cooperation can cause procedural
provide evidence-based practices for facilitating com-munication.39 AIDET, which stands for acknowledge, introduce, duration, explain, and thank you, is a tool that has gained wide use in hospitals. Developed by the Struder Group, AIDET is designed to leave nothing open to interpretation, and it aligns the patient’s percep-tions with those of the health care team.39 In addition, it is critical to verify the patient’s identity with at least 2 (and if possible 3) identifiers, verify the procedure, and properly label all paperwork with patient identification stickers, times, date, and other pertinent information.2
The radiologist will review the medical and drug history, as well as prior imaging examinations, to ensure the proper procedure has been chosen.1,3 The
Box
Percutaneous Drainage Procedure Supplies2,3
Personal protective equipment (face shields, sterile gowns, sterile gloves, foot coverings)Sterile 4 4 inch gauze spongesSterile drapeSterile needles (18-, 20-, 22-G)Sterile syringes (5 mL to 60 mL)ScalpelChoice of procedure needles Spinal needles (18-G to 22-G) Chiba (20-G to 22-G; 15 cm to 20 cm) Cutting needles (14-G to 18-G) Franseen (18-G to 20-G)Metallic skin markersSkin marking penBetadineLidocaine (1%)Pigtail catheter (8-14 French)Fascial dilators (7-13 French)Guide wiresAmplatz wireSpecimen tubes for laboratory studiesAerobic and anaerobic culture tubesFormalin or nonbacteriostatic salineStopcocksSuture (nylon or Prolene)Drainage bag and connecting tubingTape
Abbreviation: G, gauge.

195CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
Roberts
emotionally upset and the radiologist might administer a hypnotic or a sedative.1 Technologists also should be familiar with their institution’s sedation and emergency response protocols.2 This is important in the event that visualization of the abscess requires IV contrast media administration. Technologists must be prepared to respond with basic life support and assist in stabilizing the patient if cardiac or respiratory distress occurs.2 In addition, the health care team should ensure appropri-ate venous access for medications at all times—espe-cially during LOCM injection.2 Contrast injection pro-tocols differ according to institution, scanner protocols, patient needs, and the visualization requirements of the interventional radiologist.1,2 An adequate volume of LOCM given at an appropriate f low rate and flow duration is essential to producing high-quality images.2 Although institution-specific IV contrast protocols often call for a uniform dose regardless of an adult’s size, the foundations for this practice are unclear.2
Megibow et al conducted research on 463 patients, randomizing them into 1 of 4 weight-based LOCM dose categories and concluded that a weight-based dose at 1.5 mL/kg of LOCM can provide acceptable scans in most patients, with significant cost savings.40 Yanaga et al yielded similar results in a study dedicated to weight-based doses of LOCM in patients suspected of having pancreatic tumors, concluding that weight-based dosing provides satisfactory enhancement.41 Neither of these studies report on cost. Nevertheless, the technologist must work with the radiologist to determine which dose system is best for the patient.2
Critical thinking is key at each point in CT-guided PAD. The technologist and radiologist must remem-ber that even though PAD has been proven effective, some patients are better suited for surgical drainage.1 Percutaneous drainage of fungal infection, infected hematomas, echinococcal disease, surgical infections, and pancreatic abscesses, as well as failed percutaneous drainage procedures, are areas of controversy.1 Types of abscesses vary, and studies with proper controls can be difficult to establish.42 In addition, significant contro-versy exists at many institutions about the appropriate-ness of PAD for abscesses with disease processes his-torically treated surgically (eg, abscesses of the pancreas and kidney).1,10
complications, and CT technologists should gauge the personality of each patient to determine how to encour-age cooperation.2 If a patient refuses or is unable to remain still during the procedure, difficulties can arise including infection, injury, and an unsuccessful proce-dure.1,2 For example, when the radiologist and the radiol-ogy nurse deliver local anesthesia in the area of the drain placement and along the needle pathway, the patient might flinch or move if the area is not correctly anesthe-tized.1,3 This movement could produce a tear, bleeding, or pneumothorax.1 While anesthetization is not the CT technologist’s role, it is appropriate for technologists to assist by drawing up medications, preparing the patient’s skin, ensuring patient immobilization, and documenting the procedure.2
One way the technologist can aid patient coopera-tion is planning for proper positioning because the patient’s position on the table can either hinder or help drainage procedures.1,2 The technologist usu-ally knows the CT scanner and table parameters better than others involved in the procedure.1,2 The radiologist will assess whether the patient should be positioned head first, feet first, prone, supine, or in a lateral recumbent position.1 The technologist should determine the support devices necessary to comfort-ably immobilize the patient.2 The radiologist and the technologist must consider how the patient’s position on the z-axis of the table could affect the ability to adequately image the area of interest.1,2
With proper planning, the technologist can ensure that vital sign monitoring wires, suction tubing, IV lines, and other equipment will not interfere with patient comfort or the radiologist’s control of instru-ments.2 The patient should be placed in a position that is most comfortable within the limits of the radi-ologist’s planned needle trajectory.1,2 The position is patient specific, but pillows under the knees and shoul-ders are almost always helpful.2 Warm blankets can increase the patient’s comfort, but technologists should avoid contaminating sterile fields with the blankets.2 In addition, patients requiring abscess drainage might be febrile, and in these cases a sheet is preferable to a warm blanket.2
In spite of the health care team’s best efforts, some patients who require this procedure become

196CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
CT-guided Intra-abdominal Abscess Drainage
orientation along the x- and y-axes might affect instru-mentation of the long needles often required for drain placement.1,2 Patient dose and image quality are related to this positioning consideration as Toth et al demon-strated.43 They found that failure to center a patient to the CT gantry isocenter can result in increased noise and patient dose. Studies on CT phantoms showed that miscentering the patient by as little as 3 cm increased surface dose by 18% and noise by 6%.42 These increases likely are linked to degradation in the performance of the scanner’s bowtie filter.2,43 Nevertheless, a compro-mise must be reached in consideration of the patient’s dose, image noise, and the radiologist’s need to main-tain a sterile field while advancing the needle.1
The technologist must assist with designating and maintaining a zero level on the z-axis, programming the scanner for the appropriate scanning protocol, and moving the patient in and out of the gantry efficiently as directed by the radiologist.1,2 One technique is to review closely the abscess on prior studies, zero the scanner as close as possible to the indicated level, perform a pre-liminary scan to include anatomy above and below, and then reset to zero when the radiologist determines the precise level on the z-axis to insert the needle. This final reset to zero can assist in making small adjustments either superior or inferior to the needle’s location on the z-axis. Once the scan is plotted, the radiologist will determine the optimal patient position, the indications for oral or IV contrast media, and the appropriate level for needle puncture.2 Fiducial markers can further aid in determining the needle’s path.1 At other times, the radiologist might use a blunt metal tip—such as the tip of a hemostat—to assist in determining the needle
The Procedure The benefits of CT-guided drainage of intra-
abdominal abscesses lie in the procedure’s simplicity, imaging flexibility, lower risk for complications, and pro-jected cost-effectiveness.1 At the core of these benefits is the appearance of the abscess on CT images.1 An initial diagnostic scan through the area of the abscess indicates the ease or difficulty of drain placement.1,3 In general, abscesses that respond favorably to PAD are those that1,2: Display low density and clear definition without
septations or various pockets of purulent material. Are easily accessible. Contain free-f lowing f luid.Results with septated abscesses are mixed, and vis-
cosity or density of the infected material in the abscess affects drainage.1 At times, PAD is performed under less favorable conditions such as when the f luid collection is poorly defined or multiloculated, composed of dense, necrotic material, or if the patient is deemed a poor candidate for surgery.2 It often is helpful to measure the HU of the abscess’ interior because this value can indicate the viscosity or thickness of the purulent mate-rial.1,2 Although the numbers can vary, an HU close to that of serous f luid (0 -30 HU) is best.1 The radiologist’s planning can be assisted further by image annotations, including a measurement grid, distance, and angle arrows—each applied to the significant images.2
Windowing and leveling can further enhance visual-ization.2 A routine soft-tissue window setting (450 width/50 level) will display most abdominopelvic anatomy adequately.2 The liver might require a nar-rower window setting (150 width/70 level) to improve visibility.2 The display field-of-view should be large enough to include the skin surface over the area to be drained.2 CT provides excellent imaging of abscess cavities, extensions of the f luid collections, air, adjacent anatomy, and most instruments.1 Scout scans can be used as a digital radiograph to further aid visualization, and 3-D capabilities are being explored.1 Nevertheless, imaging preferences vary depending on the radiologist, institution, available technology, and staff education.1
A key technical consideration is the determination of the zero point for the z-axis (see Figure 2).2 As the patient is positioned for this initial diagnostic scan, the technologist should consider how the patient’s
AC
B
Figure 2. Zeroing the CT scanner to the needle insertion point allows for calculations of distance (A), abscess location (B), and angle of insertion (/_ ACB).
197CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
Roberts
The incision time must be recorded.1 Making the initial insertion and positioning the needle requires the radiologist’s concentration, and the technologist should keep distractions to a minimum.2 CT imaging can be repeated at any time to confirm the suitability of the needle entry and route.2 The radiologist might use a foot pedal to initiate CT fluoroscopy scanning as the needle is positioned within the abscess.1 It might be helpful to change the patient’s position, externally manipulate the bowel, or instruct the patient to suspend respiration.1 Having the patient in variable positions can optimize delineation of anatomy.1 Typically, it is the technologist’s responsibility to operate the table controls and to move the patient into the gantry for scanning.2 Sometimes, the radiologist might request a change in the window and level of image display or a contrast injection to further delineate anatomy and needle placement.1,2 The wide latitude of localization and positioning techniques is one aspect of the f lexibil-ity of CT-guided procedures.1 This f lexibility means the technologist must work closely with the radiologist, the patient, and the nurse to ensure success even as differ-ent techniques are employed.1
The interventional radiologist can decide whether to enter the f luid collection in one step with a needle
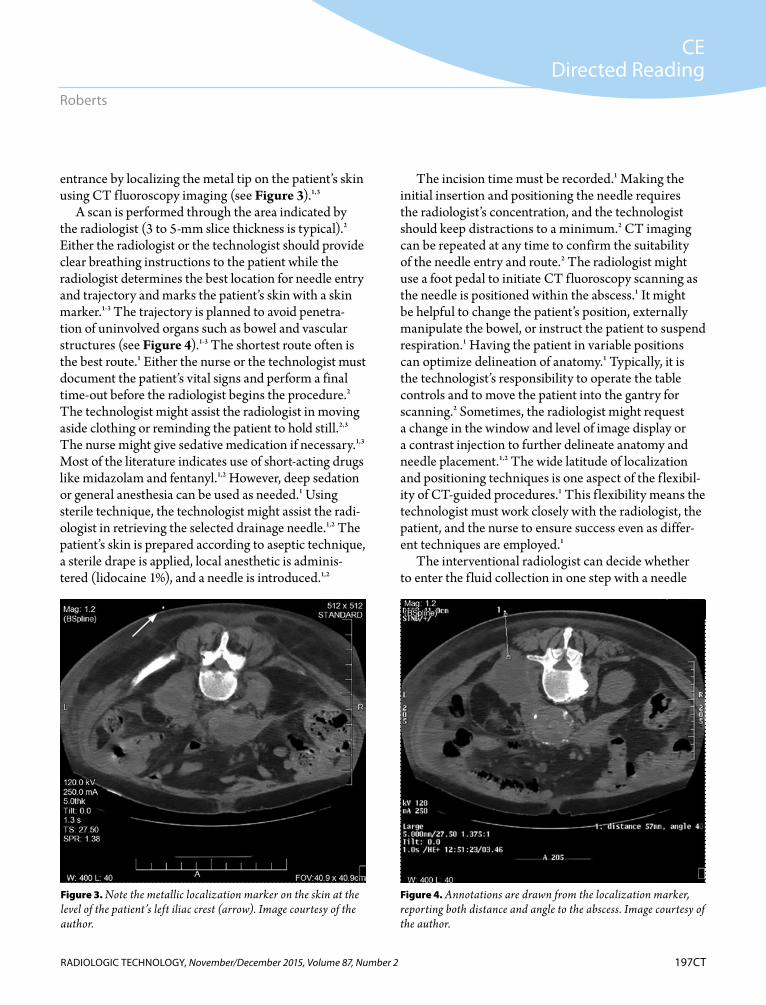
entrance by localizing the metal tip on the patient’s skin using CT fluoroscopy imaging (see Figure 3).1,3
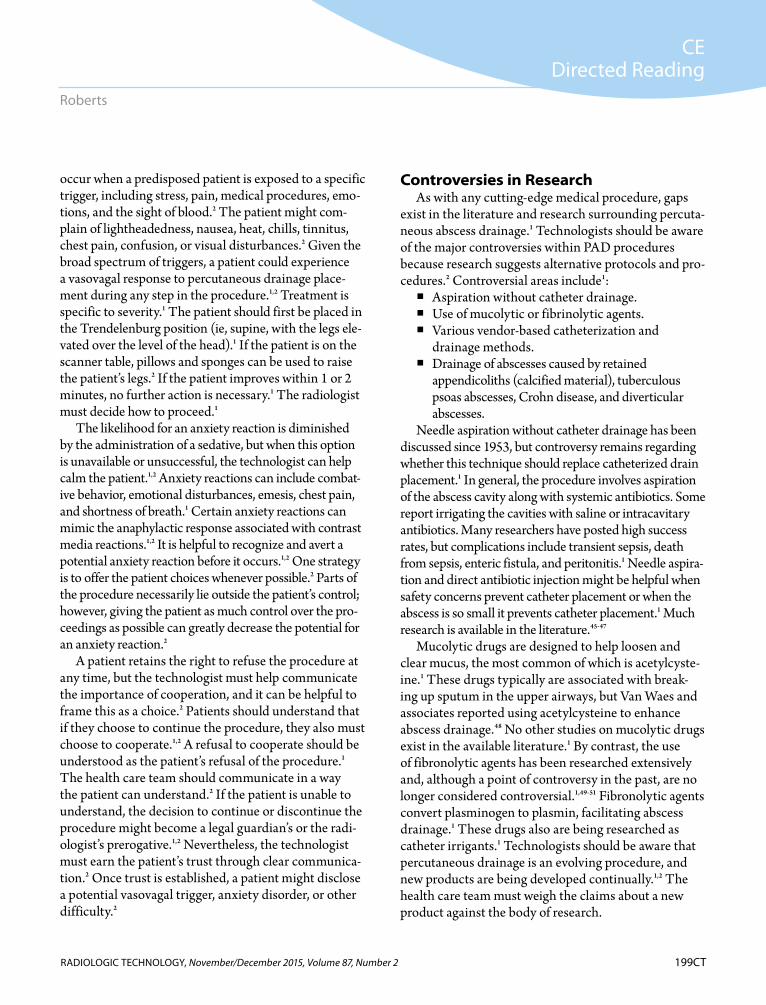
A scan is performed through the area indicated by the radiologist (3 to 5-mm slice thickness is typical).2 Either the radiologist or the technologist should provide clear breathing instructions to the patient while the radiologist determines the best location for needle entry and trajectory and marks the patient’s skin with a skin marker.1-3 The trajectory is planned to avoid penetra-tion of uninvolved organs such as bowel and vascular structures (see Figure 4).1-3 The shortest route often is the best route.1 Either the nurse or the technologist must document the patient’s vital signs and perform a final time-out before the radiologist begins the procedure.2 The technologist might assist the radiologist in moving aside clothing or reminding the patient to hold still.2,3 The nurse might give sedative medication if necessary.1,3 Most of the literature indicates use of short-acting drugs like midazolam and fentanyl.1,2 However, deep sedation or general anesthesia can be used as needed.1 Using sterile technique, the technologist might assist the radi-ologist in retrieving the selected drainage needle.1,2 The patient’s skin is prepared according to aseptic technique, a sterile drape is applied, local anesthetic is adminis-tered (lidocaine 1%), and a needle is introduced.1,2
Figure 3. Note the metallic localization marker on the skin at the level of the patient’s left iliac crest (arrow). Image courtesy of the author.
Figure 4. Annotations are drawn from the localization marker, reporting both distance and angle to the abscess. Image courtesy of the author.

198CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
CT-guided Intra-abdominal Abscess Drainage
Lambiase et al reported results suggesting that immu-nocompetent patients fare better than immunocom-promised patients.44 Success rates are stratified accord-ing to the Acute Physiology, Age, Chronic Health Evaluation (APACHE) score, which was designed to predict mortality in severely ill, hospitalized patients. Betsch et al correlated drainage outcomes to patient APACHE III scores and reported 91% successful PAD with an APACHE III score below 30 points.42 APACHE III scores above 30 demonstrated a drop in clinical success to 64%. The success rate of PAD depends on the abscess etiology, size, complexity, and indication for drainage.42 Given the potential complexity of these infectious processes, complications can arise.1,3
The incidence of complications varies between 5% and 9.8%.1 Complications relate to abscess location and the affected anatomy.1 For example, the lowest compli-cation rates are associated with the liver and the highest with the spleen.1,44 These complications included sepsis after catheter insertion, spontaneous hemorrhage, spill-age of infected material, and fistula formation.1 One of the most common complications of PAD stems from the needle trajectory.1 The radiologist must avoid traversing a solid organ or crossing the pleural space while drain-ing subphrenic abscesses to prevent the spread of infec-tion.1,3 This underscores the technologist’s role of mini-mizing distractions and patient movement as the physi-cian advances the needle. Early removal of the catheter can result in abscess recurrence.1 Complications also can arise from haste.1 Haaga et al gives an example of one physician who skipped CT localization and pene-trated the patient’s femoral vein.1 Errors in needle place-ment can result in infection, blood loss, and trauma.
Proper patient care and machine operation can reduce complications.2 It is the technologist’s duty to assess the patient’s condition and tailor care to his or her needs.2 Technologists should be mindful that it might be the patient’s first drainage procedure, and extra time and effort might be required to put the patient at ease.2 This effort is justified if the technologist can reduce the risk of a vasovagal response, anxiety reaction, or refusal to cooperate.2
Vasovagal responses stem from vasodilation brought on by a disruption of the vagal nerve, resulting in bra-dycardia and hypotension.2 Vasovagal responses can
or drainage catheter or to introduce a needle, advance a guide wire, and then advance the catheter using exchange techniques.1,2 Once the CT image indicates a correct location of the needle or drainage catheter, f luid is aspirated to confirm placement (see Figure 5).2 Once confirmed, the abscess is aspirated and drained as completely as possible, and samples might be taken.1-2 In addition, antibacterial drugs might be directly admin-istered into the abscess via the catheter, which is typi-cally secured in place with suture.1 After the procedure, catheters are placed below the level of the patient to allow gravity to drain the abscess.2 When the abscess is drained completely, the catheter is withdrawn.1,2 In cases where f luid collection is aspirated only for a speci-men or partially drained, the needle is withdrawn and the area bandaged.2
Complications Most authors agree that CT is the modality of choice
for performing drainage procedures, but the success rate for PAD remains a topic of considerable contro-versy.1,3 Success rates vary from approximately 50% to 90%. It is difficult to isolate all the factors that contrib-ute to this range, which include selection criteria, drain-age techniques, and methods for evaluating outcomes.1
Figure 5. A confirmation CT image documenting catheter place-ment within the abscess. Image courtesy of the author.
199CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
Roberts
Controversies in ResearchAs with any cutting-edge medical procedure, gaps
exist in the literature and research surrounding percuta-neous abscess drainage.1 Technologists should be aware of the major controversies within PAD procedures because research suggests alternative protocols and pro-cedures.2 Controversial areas include1: Aspiration without catheter drainage. Use of mucolytic or fibrinolytic agents. Various vendor-based catheterization and
drainage methods. Drainage of abscesses caused by retained
appendicoliths (calcified material), tuberculous psoas abscesses, Crohn disease, and diverticular abscesses.
Needle aspiration without catheter drainage has been discussed since 1953, but controversy remains regarding whether this technique should replace catheterized drain placement.1 In general, the procedure involves aspiration of the abscess cavity along with systemic antibiotics. Some report irrigating the cavities with saline or intracavitary antibiotics. Many researchers have posted high success rates, but complications include transient sepsis, death from sepsis, enteric fistula, and peritonitis.1 Needle aspira-tion and direct antibiotic injection might be helpful when safety concerns prevent catheter placement or when the abscess is so small it prevents catheter placement.1 Much research is available in the literature.45-47
Mucolytic drugs are designed to help loosen and clear mucus, the most common of which is acetylcyste-ine.1 These drugs typically are associated with break-ing up sputum in the upper airways, but Van Waes and associates reported using acetylcysteine to enhance abscess drainage.48 No other studies on mucolytic drugs exist in the available literature.1 By contrast, the use of fibronolytic agents has been researched extensively and, although a point of controversy in the past, are no longer considered controversial.1,49-51 Fibronolytic agents convert plasminogen to plasmin, facilitating abscess drainage.1 These drugs also are being researched as catheter irrigants.1 Technologists should be aware that percutaneous drainage is an evolving procedure, and new products are being developed continually.1,2 The health care team must weigh the claims about a new product against the body of research.
occur when a predisposed patient is exposed to a specific trigger, including stress, pain, medical procedures, emo-tions, and the sight of blood.2 The patient might com-plain of lightheadedness, nausea, heat, chills, tinnitus, chest pain, confusion, or visual disturbances.2 Given the broad spectrum of triggers, a patient could experience a vasovagal response to percutaneous drainage place-ment during any step in the procedure.1,2 Treatment is specific to severity.1 The patient should first be placed in the Trendelenburg position (ie, supine, with the legs ele-vated over the level of the head).1 If the patient is on the scanner table, pillows and sponges can be used to raise the patient’s legs.2 If the patient improves within 1 or 2 minutes, no further action is necessary.1 The radiologist must decide how to proceed.1
The likelihood for an anxiety reaction is diminished by the administration of a sedative, but when this option is unavailable or unsuccessful, the technologist can help calm the patient.1,2 Anxiety reactions can include combat-ive behavior, emotional disturbances, emesis, chest pain, and shortness of breath.1 Certain anxiety reactions can mimic the anaphylactic response associated with contrast media reactions.1,2 It is helpful to recognize and avert a potential anxiety reaction before it occurs.1,2 One strategy is to offer the patient choices whenever possible.2 Parts of the procedure necessarily lie outside the patient’s control; however, giving the patient as much control over the pro-ceedings as possible can greatly decrease the potential for an anxiety reaction.2
A patient retains the right to refuse the procedure at any time, but the technologist must help communicate the importance of cooperation, and it can be helpful to frame this as a choice.2 Patients should understand that if they choose to continue the procedure, they also must choose to cooperate.1,2 A refusal to cooperate should be understood as the patient’s refusal of the procedure.1 The health care team should communicate in a way the patient can understand.2 If the patient is unable to understand, the decision to continue or discontinue the procedure might become a legal guardian’s or the radi-ologist’s prerogative.1,2 Nevertheless, the technologist must earn the patient’s trust through clear communica-tion.2 Once trust is established, a patient might disclose a potential vasovagal trigger, anxiety disorder, or other difficulty.2

200CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
CT-guided Intra-abdominal Abscess Drainage
abscesses was minimally invasive with a few days of recovery and general anesthesia was avoided.54 As new drugs are developed, it is likely that more TB patients will undergo CT-guided abscess drainage.27
Crohn disease is characterized by ulceration in the large intestine, which could result in perforation or fis-tula formation of the bowel wall.1 The literature reports a wide range of morbidity related to Crohn disease (7%-34.7%).21 Nevertheless, intra-abdominal abscess formation is a common complication of the disease with approximately 10% to 20% of patients developing an abscess as a result of disease processes.1,55 Traditional treatment was surgery; however, CT-guided drainage procedures have increased in use.1,3 In the past, stud-ies determined that percutaneous drainage for intra-abdominal abscesses secondary to Crohn disease had a 50% success rate.1,22 Failure can result in complications requiring urgent surgery.22
A 2013 study from Spain yielded a success rate of only one-third in the treatment of Crohn disease with PAD. The authors further reported that surgery performed after failure of PAD resulted in poorer out-comes than immediate surgery.55 In contrast, 95% of patients who received immediate surgical treatment achieved long-term resolution of the intra-abdominal abscess.55 Nevertheless, surgery for Crohn disease–related abscesses involves loss of intestinal function.55 Quality of life must be weighed alongside indications that approximately 80% of all patients with Crohn dis-ease will require some form of treatment during their lifetime.55 Therefore, to improve patient outcomes, alternatives to the surgical treatment of intra-abdom-inal abscesses in Crohn disease continue to interest researchers, even though the effectiveness of PAD in the treatment of Crohn disease remains controversial.55
Similarly, percutaneous drainage of diverticular abscess is simple but controversial because in most patients, successful drainage results in formation of a colonic diverticular fistula.1 Small diverticular abscesses can be treated surgically with a resection of the sig-moid colon and are resolved in a single procedure.1,56 Nevertheless, a retrospective study by Elagili et al of 114 cases of diverticular abscess reported a success rate of 81% for initial percutaneous drainage with 22.5 days as the median duration of drainage.56 The authors
Laparoscopic appendectomy has gained wide acceptance as the most successful procedure for acute appendicitis.52 Nevertheless, this procedure includes an increased risk of dropped apendicoliths, which remain in the surgical site after removal of the appendix.52 Appendicoliths can measure up to 6 cm in diameter.52 These stones form around feces, foreign bodies, veg-etable matter, or barium lodged in the appendix.52As many as one-third of appendectomy specimens contain appendicoliths.51 Whether appendicoliths have a direct association with abscess formation is not yet estab-lished, but early evidence suggests a connection.52
Buckley et al suggest that intra-abdominal abscesses secondary to retained appendicoliths are best treated with formal surgical drainage and removal of the appendicolith for long-term success.52 They conclude that percutaneous drainage has only short-term success because the appen-dicolith remains.52 Radiologic technologists should under-stand the role of image-guided procedures in abscess treatment and consider how new technology might pro-vide extended efficacy for percutaneous procedures.2
According to the World Health Organization, TB is one of the world’s deadliest communicable diseases.53 In 2013, approximately 9 million people were infected and 1.5 million died from the disease.53 Other than the respiratory system, the musculoskeletal system is the most common site.26 Up to 50% of patients who experi-ence skeletal system involvement have TB of the spine, and paraspinal abscess formation has been observed in about 75% of these patients.27 Research is needed on percutaneous drainage of tuberculous psoas abscesses because of the complex nature of TB abscess formation and evolving methods for the procedure.
Dinç et al evaluated CT-guided percutaneous drain-age or aspiration in 21 cases of iliopsoas abscesses of tuberculous origin.27 Six patients (29%) had recurrences within 1 and 3 months after catheter removal. In a retrospective study, Tsagouli et al studied 63 cases of 44 patients treated over 2 years using CT-guided pro-cedures to drain abscesses throughout the body, noting that 12 of the patients had 2 abscesses in 2 different sites and 7 patients had 3 abscesses in as many sites.54 The authors reported no major or minor complications, no recurrence, and all patients had a successful recovery.They further noted that CT-guided drainage of TB

201CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
Roberts
instrumentation, and radiation safety during inter-ventional procedures. As research continues, areas of controversy will be resolved, and new controversies will arise. Regardless, CT technologists must provide preci-sion images, dose-optimization protocols, patient care standards, and documentation while working collabora-tively as part of the health care team.
Benjamin W Roberts, MFA, R.T.(R)(T)(CT), is instructor for the Baptist College of Health Sciences medical radiography program in Memphis, Tennessee.
Reprint requests may be mailed to the American Society of Radiologic Technologists, Communications Department, at 15000 Central Ave SE, Albuquerque, NM 87123-3909, or e-mailed to [email protected].
© 2015 American Society of Radiologic Technologists
References1. Haaga JR, Haaga TL, Wu H. Image-guided interventions:
CT emphasis. In: Haaga JR, Dogra VS, Forsting M, Gilkeson RC, Ha HK, Sundaram M, eds. CT and MRI of the Whole Body. 5th ed. Philadelphia, PA: Mosby; 2009:2411-2644.
2. Romans, LE. Interventional CT and CT fluoroscopy. In: Computed Tomography for Technologists: A Comprehensive Text. Philadelphia, PA: Wolters Kluwer Health; 2011:345-347.
3. Men S, Akhan O, Köroğlu M. Percutaneous drainage of abdominal abscess. Eur J Radiol. 2002;43(3):204-218.
4. Haaga JR, Alfidi RJ, Havrilla TR, et al. CT detection and aspiration of abdominal abscesses. AJR Am J Roentgenol. 1977;128(3):465-474.
5. Gerzof SG, Robbins AH, Birkett DH, Johnson WC, Pugatch RD, Vincent ME. Percutaneous catheter drainage of abdomi-nal abscesses guided by ultrasound and computed tomogra-phy. AJR Am J Roentgenol. 1979;133(1):1-8.
6. Golfieri R, Cappelli A. Computed tomography-guided per-cutaneous abscess drainage in coloproctology: review of the literature. Tech Coloproctol. 2007;11(3):197-208.
7. Bakal CW, Sacks D, Burke DR, et al; Society of Cardiovascular and Interventional Radiology Standards of Practices Committee. Quality improvement guidelines for adult percutaneous abscess and fluid drainage. J Vasc Interv Radiol. 1995;6(1):68-70.
8. Higgs Z, Macafee D, Braithwaite B, Maxwell-Armstrong C. The Seldinger technique: 50 years on. Lancet. 2005; 366(9494):1407-1409. doi:10.1016/S0140-6736(05)66878-X.
published a separate study indicating that diverticular abscesses, which presented technical difficulties for ini-tial percutaneous drainage, could be treated with anti-biotics alone without adverse consequences to patient outcomes.57 More information is needed to determine whether antibiotics alone are a sufficient initial treat-ment for diverticular abscess or whether percutaneous drainage should be recommended. This is in addition to ongoing research about the need for surgical treatment after initial percutaneous drainage.
The controversies surrounding diverticular abscess-es and Crohn disease abscesses illustrate the need for technologists to review the patient’s history, prior stud-ies, and clinical presentation because they assist physi-cians with CT imaging and CT-guided procedures.2 Technologists should be aware of these controversies, practice interprofessional communication, and demon-strate mutual respect to others on the health care team to provide excellent patient care.
ConclusionCT-guidance techniques have revolutionized percu-
taneous procedures, and CT is the established modality of choice for intra-abdominal abscess drainage.1,2 The history of CT-guidance procedures reveals a legacy of research-driven innovation. Practice-based research is needed to establish the cost effectiveness and best prac-tices of PAD. Nevertheless, CT provides the flexibility, imaging accuracy, and speed necessary for efficient patient care in an ever-evolving health care system.1
Percutaneous procedures continue to increase in fre-quency and complexity, with good success rates, leading some to conclude that image-guided abscess drainage procedures will preserve interventional radiology as a subspecialty.1,58 Advances in iterative reconstruction, 3-D reconstruction, and computer-assisted diagnosis promise reduced radiation dose, increased imaging detail, and increased planning accuracy.1,2 Early testing indicates that some form of robotic guidance is forth-coming.1,58 The future of percutaneous procedures is promising for CT technologists, but dedication to ethics and excellence must be encouraged to guarantee positive patient outcomes.2
Technologists must work with physicians, nurses, and administrators to advocate for cleanliness, proper
202CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
CT-guided Intra-abdominal Abscess Drainage
Sundaram M, eds. CT and MRI of the Whole Body. 5th ed. Philadelphia, PA: Mosby; 2009:1308-1311.
24. Frank ED, Long BW, Smith BJ. Abdomen. In: Merrill’s Atlas of Radiographic Positioning and Procedures. Vol 2. 12th ed. St Louis, MO: Elsevier Mosby; 2012:81-94.
25. Liu WH, Wang T, Yan HT, et al. Predictors of percutane-ous catheter drainage (PCD) after abdominal paracentesis drainage (APD) in patients with moderately severe or severe acute pancreatitis along with fluid collections. PLoS One 2015;10(2):e0115348. doi:10.1371/journal.pone.0115348.
26. vanSonnenburg E, Wittich GR, Goodacre BW, Casola G, D’Agostino HB. Percutaneous abscess drainage: update. World J Surg. 2001;25(3):362-372.
27. Dinç H, Ahmetoğlu A, Baykal S, Sari A, Sayil O, Gümele H. Image-guided percutaneous drainage of tuberculous iliopsoas and spondylodiskitic abscesses: midterm results. Radiology. 2002;225(2):353-358.
28. Procaccino JA, Lavery JC, Fazio VW, Oakley JR. Psoas abscess: difficulties encountered. Dis Colon Rectum. 1991;34(9):784-789.
29. Mettler F, Thomadsen B, Bhargavan M, et al. Medical radia-tion exposure in the U.S. in 2006: preliminary results. Health Phys. 2008;95(5):502-507. doi:10.1097/01.HP.0000326 333.42287.a2.
30. Berrington de Gonzáles A, Darby S. Risk of cancer from diag-nostic x-rays: estimates for the UK and 14 other countries. Lancet. 2004;363(9406):345-351.
31. Einstein A, Henzlova M, Rajagopalan S. Estimating risk of cancer associated with radiation exposure from 64-slice computed tomography coronary angiography. JAMA. 2007;298(3):317-323.
32. Fazel R, Krumholz H, Wang Y, et al. Exposure to low-dose ionizing radiation from medical imaging procedures. N Engl J Med. 2009;361(9):849-857. doi:10.1056/NEJMoa0901249.
33. The Joint Commission. Radiation risks of diagnostic imag-ing. Sentinel Event Alert, Issue 47. 2011;24(47):1-4.
34. Tsalafoutas I, Tsapaki V, Triantopoulou C, Gorantonaki A, Papailiou J. CT-guided interventional procedures without CT fluoroscopy assistance: patient effective dose and absorbed dose considerations. AJR Am J Roentgenol. 2007;188(6):1479-1484.
35. Curry TS, Dowdey JE, Murry RC. Christensen’s Physics of Diagnostic Radiology. 4th ed. Philadelphia, PA: Lippincott Wiliams & Wilkins; 1990:522.
36. Lucey B, Varghese J, Hochberg A, Blake M, Soto J. CT-guided intervention with low radiation dose: feasibility and experi-ence. AJR Am J Roentgenol. 2007;188(5):1187-1194.
37. Smith J, Jin D, Watkins G, Miller T, Karst J, Oyoyo U. Ultra-low-dose protocol for CT-guided lung biopsies. J Vasc Interv Radiol. 2011;22(4):431-436. doi:10.1016/j.jvir.2011.01.431.
9. Seeram E. Computed tomography: an overview. In: Computed Tomography: Physical Principles, Clinical Applications, and Quality Control. 3rd ed. St Louis, MO: Elsevier Saunders; 2009:1-28.
10. Haaga J, Alfidi RJ, Weinstein A. Percutaneous catheter drain-age of abdominal abscess [letter to the editor]. N Eng J Med. 1982;306(2):106-108. doi:10.1056/NEJM198201143060213.
11. Gazelle GS, Mueller, PR. Abdominal abscess. Imaging and intervention. Radiol Clin North Am. 1994:32(5):913-932.
12. Eisenberg PJ, Dawson SL. Percutaneous treatment of abdominal abscesses. In: Baum S, Pentecost MJ, eds. Abram’s Angiography: Interventional Radiology. Vol. 3. London: Little Brown and Company, 1997:925-938.
13. Johannsen EC, Sifri CD, Madoff LC. Pyogenic liver abscess. Infect Dis Clin North Am. 2000;14(3):547-563.
14. Bradley D, Bradley KE. The value of diagnostic medical imaging. N C Med J. 2014;75(2):121-125.
15. Smith-Bindman R, Miglioretti DL, Larson EB. Rising use of diagnostic medical imaging in a large integrated health sys-tem. Health Aff. 2008;27(6):1491-1502. doi:10.1377 /hlthaff.27.6.1491.
16. Overutilization of medical imaging. National Decision Support Company Web site. http://www.acrselect.org/prob lem.html. Accessed February 23, 2015.
17. Patient Protection and Affordable Care Act. Pub L No. 111-148, 124 Stat 741. 42 USC 1230e-1. http://www.gpo.gov /fdsys/pkg/PLAW-111publ148/pdf/PLAW-111publ148.pdf. Accessed August 12, 2015.
18. Tilburt JC, Wynia MK, Sheeler RD, et al. Views of US physicians about controlling health care costs. JAMA. 2013;310(4):380-388. doi:10.1001/jama.2013.8278.
19. Sommers R, Goold SD, McGlynn EA, Pearson SD, Danis M. Focus groups highlight that many patients object to clini-cians’ focusing on costs. Health Aff. 2013;32(2):338-346. doi:10.1377/hlthaff.2012.0686.
20. Güler Ö, Yaniv Z. Image-guided navigation: a cost effec-tive practical introduction using the Image-Guided Surgery Toolkit (IGSTK). Conf Proc IEEE Eng Med Biol Soc. 2012;2012:6056-6059. doi:10.1109/EMBC.2012.6347375.
21. Xie Y, Zhu W, Li N, Li J. The outcome of initial per-cutaneous drainage versus surgical drainage for intra-abdominal abscesses in Crohn’s disease. Int J Colorectal Dis. 2012;27(2):199-206. doi:10.1007/s00384-011-1338-x.
22. Bafford A, Coakley B, Powers S, et al. The clinical impact of preoperative percutaneous drainage of abdominopelvic abscesses in patients with Crohn’s disease. Int J Colorectal Dis. 2012;27(7):953-958. doi:10.1007/s00384-011-1401-7.
23. Ha HK, Park SH, Lee SS, Kim AY. Gastrointestinal tract. In: Haaga JR, Dogra VS, Forsting M, Gilkeson RC, Ha HK,
203CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
Roberts
53. World Health Organization. Global Tuberculosis Report 2014. http://www.who.int/tb/publications/global_report /en/. Published 2014. Accessed May 5, 2015.
54. Tsagouli P, Sotiropoulou E, Filippousis P, Sidiropoulou N, Georgiadi V, Thanos L. Contribution of computed tomog-raphy guided percutaneous drainage of tuberculous cold abscesses adjunctive to pharmaceutical anti-tubercular treat-ment. Eur J Radiol. 2012;81(3):562-565. doi:10.1016/j .ejrad.2011.02.048.
55. Lobatón T, Guardiola J, Rodriquez-Moranta F, et al. Comparison of the long-term outcome of two therapeutic strategies for the management of abdominal abscess compli-cating Crohn’s disease: percutaneous drainage or immediate surgical treatment. Colorectal Dis. 2013;15(10):1267-1272. doi:10.1111/codi.12419.
56. Elagili F, Stocchi L, Ozuner G, Mody R, Baker M, Kiran R. Predictors of postoperative outcomes for patients with diverticular abscess initially treated with percutaneous drainage. Am J Surg. 2015;209(4):703-708. doi:10.1016/j.amj surg.2014.05.018.
57. Elagili F, Stocchi L, Ozuner G, Kiran R. Antibiotics alone instead of percutaneous drainage as initial treatment of large diverticular abscess [published online ahead of print November 23, 2014]. Tech Coloproctol. 2015;19(2):97-103. doi:10.1007/s10151-014-1250-9.
58. Haaga JR. Imaging-guided microsurgery and the future of radiology. AJR Am J Roentgenol. 2000;175(2):303-304. doi:10.2214/ajr.175.2.1750303.
38. Rezazadeh S, Co S, Bicknell S. Reduced kilovoltage in com-puted tomography-guided intervention in a community hospital: effect on the radiation dose. Can Assoc Radiol J. 2014;65(4):345-351. doi:10.1016/j.carj.2014.04.002.
39. Scott J. Utilizing AIDET and other tools to increase patient satisfaction scores. Radiol Manage. 2012;34(3):29-33.
40. Megibow A, Jacob G, Heiken JP, et al. Quantitative and qualitative evaluation of volume of low osmolality contrast medium needed for routine helical abdominal CT. AJR Am J Roentgenol. 2001;176(3):583-589.
41. Yanaga Y, Awai K, Nakayama Y, et al. Pancreas: patient body weight tailored contrast material injection proto-col versus fixed dose protocol at dynamic CT. Radiology. 2007;245(2):475-482.
42. Betsch A, Wiskirchen J, Trübenback J, et al. CT-guided percutaneous drainage of intra-abdominal abscesses: APACHE III score stratification of 1-year results. Eur Radiol. 2002;12(12):2883-2889. doi:10.1007/s00330-002-1398-y.
43. Toth T, Ge Z, Daly M. The influence of patient centering on CT dose and image noise. Med Phys. 2007;34(7):3093-3101.
44. Lambiase R, Deyoe L, Cronan J, Dorfman G. Percutaneous drainage of 335 consecutive abscesses: results of primary drainage with 1-year follow-up. Radiology. 1992;184(1):167-179.
45. Green BT. Splenic abscess: report of six cases and review of the literature. Am Surg. 2001;67(1):80-85.
46. Giorgio A, de Stefano G, Di Sarno A, Liorre G, Ferraioli G. Percutaneous needle aspiration of multiple pyogenic abscess-es of the liver: 13-year single-center experience. AJR Am J Roentgenol. 2006;187(6):1585-1590.
47. Ch Yu S, Hg Lo R, Kan PS, Metrweli C. Pyogenic liver abscess: treatment with needle aspiration. Clin Radiol. 1997;52(12):912-916.
48. van Waes P, Feldberg M, Mali WP, et al. Management of loculated abscesses that are difficult to drain: a new approach. Radiology. 1983;147(1):57-63.
49. Haaga JR, Nakamoto D, Stellato T, el al. Intracavitary uro-kinase for enhancement of percutaneous abscess drainage: phase II trial. AJR Am J Roentgenol. 2000;174(6):1681-1685.
50. Lahorra JM, Haaga JR, Stellato T, Flanigan T, Graham R. Safety of intracavitary urokinase with percutaneous abscess drainage. AJR Am J Roentgenol. 1993;160(1):171-174.
51. Park JK, Kraus FC, Haaga JR. Fluid flow during percutane-ous drainage procedures: an in vitro study of the effects of f luid viscosity, catheter size, and adjunctive urokinase. AJR Am J Roentgenol. 1993;160(1):165-169.
52. Buckley O, Geoghegan T, Ridgeway P, Colhoun E, Snow A, Torreggiani W. The usefulness of CT guided drainage of abscesses caused by retained appendicoliths. Eur J Radiol. 2006; 60(1):80-83.

204CT RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
Directed Reading Quiz
continued on next page
1. Intra-abdominal abscesses can be:1. intraperitoneal.2. retroperitoneal.3. nonvisceral.
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
2. Before computed tomography (CT)-guided drainage for abscesses was used, mortality rates from undiagnosed and untreated abscesses ranged from ______ % to ______ %. a. 25; 50b. 45; 75c. 45; 100d. 50; 95
3. Causes of pyogenic liver abscesses include: 1. surgery.2. trauma.3. cancer.
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
4. The leading microorganism in multiple-site liver abscesses is:a. Klebsiella pneumoniae.b. Mycobacterium tuberculosis.c. Streptoccocus.d. Escherichia coli.
CT-guided Intra-abdominal Abscess Drainage
Read the preceding Directed Reading and choose the answer that is most correct based on the article.
Renewed through Jan. 1, 2021*
To earn continuing education credit: Take this Directed Reading quiz online at asrt.org/drquiz. Or, transfer your responses to the answer sheet on Page 644 and mail to:
Processing Center, 2908 Stewart Creek Blvd., Charlotte, NC 28216.
New and rejoining members are ineligible to take DRs from journal issues published prior to their most recent join date unless they have purchased access to the quiz from the ASRT. To purchase access to other quizzes, go to asrt.org/store.
* Your answer sheet for this Directed Reading must be received in the ASRT office on or before this date. Some quizzes are renewed and the expiration date extended. Check online at asrt.org/drquiz or call Member Services at 800-444-2778.
15806-03 1.5 Category A creditsOriginal Expiration Date: Dec. 31, 2017*Approved by MDCB.Check MDCB.org for details.
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
Directed Reading Quiz
continued on next page
205CT
10. Research by Lucey et al revealed that a reduction of 30 mA in tube current during CT-guided procedures can reduce patient dose ______ to ______ times without compromising the success of the procedure.a. 2; 4b. 4; 6c. 6; 8d. 8; 10
11. Routine coagulation studies do not detect the presence or activity of platelet inhibitors.a. true b. false
12. In the event that a patient becomes emotionally
upset during a drainage procedure, the radiologist might administer which type of medication?a. anticoagulantb. emeticc. amphetamined. hypnotic
13. Which factors are essential to the production of high-quality images during low-osmality contrast media injection?
1. volume2. flow rate3. flow duration
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
5. ______ oral contrast and ______ administra-tion of IV contrast can aid differentiation between the head of the pancreas, the small bowel, and the stomach.a. Positive; rapid b. Negative; rapid c. Positive; slow d. Negative; slow
6. Unencapsulated fluid collections that develop early in acute pancreatitis are called:a. pseudocysts. b. biliary obstructions. c. pancreatic phlegmon.d. pancreatic hematomas.
7. Which of the following might be a normal anatomical variant of the spleen visible on CT images?a. horseshoe spleen b. pseudospleenc. accessory spleend. fatty infiltrate
8. During drainage of digestive system abscesses, CT guidance provides the visualization necessary to avoid traversing which of the following with the drainage catheter?a. bowel loops b. lung pleurac. bladderd. liver
9. Longitudinal CT scans can simulate:
a. axial slices.b. radiographs.c. coronal slices.d. fluoroscopy.

RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
Directed Reading Quiz
continued on next page
206CT
19. The first treatment for a vasovagal response is to:a. administer oxygen through a nasal cannula.b. place the patient supine and elevate the head.c. administer fluids through the patient’s
intravenous line.d. place the patient in the Trendelenburg position.
20. According to the article, which communication strategy can the health care team use to help patients avoid an anxiety reaction? a. speaking quietlyb. maintaining eye contactc. speaking loudlyd. offering choices
21. The presence of which of the following might necessitate needle aspiration and direct antibiotic injection without catheter placement? a. large abscessb. tuberculosis (TB)c. small abscessd. Escherichia coli
22. Which of the following types of drugs facilitate drainage during PAD procedures?a. antibacterial b. fibronolytic c. anticoagulant d. antibiotic
23. As many as ______ of appendectomy specimens have been shown to contain appendicoliths.a. one-fourthb. one-thirdc. two-thirdsd. three-fourths
14. In general, abscesses displaying which of the following qualities respond most favorably to percutaneous abscess drainage (PAD)? a. low density with septationsb. high density with septationsc. low density without septationsd. high density without septations
15. Which range of Hounsfield units in the interior of the abscess indicates serous purulent material?a. 0 to 30 b. 15 to 45 c. 30 to 60 d. 45 to 75
16. Studies on CT phantoms showed that miscentering the patient by ______ cm increased surface dose by 18% and noise by 6%.a. 1b. 2c. 3d. 4
17. Betsch et al correlated drainage outcomes to APACHE III scores and reported 91% successful PAD with scores below ______ points.a. 15 b. 20 c. 25 d. 30
18. The lowest PAD complication rates are associated with which organ(s)? a. liverb. spleenc. kidneys d. pancreas
RADIOLOGIC TECHNOLOGY, November/December 2015, Volume 87, Number 2
Directed Reading Quiz
207CT
24. Other than the respiratory system, which of the following systems is the most common site of TB?a. digestive b. lymphatic c. neurological d. musculoskeletal
25. Patients with Crohn disease can develop:1. perforation of the bowel wall.2. fistula in the bowel wall.3. intra-abdominal abscesses.
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3





















![A Rare Case of Anorectal Abscess due to Foreign Ingested ...A].pdf · the patient’s perianal abscess was drained. Due to the presence of gaseous, purulent drainage from the perianal](https://img.dokumen.tips/doc/110x75/60858a3928e9e201eb61b9d8/a-rare-case-of-anorectal-abscess-due-to-foreign-ingested-apdf-the-patientas.jpg)






