Embed Size (px)
Citation preview

PCI of LAD CTO to facilitate sternal re-entry impeded by LIMA graft for surgical evacuation of mediastinal mass
Amerjeet Banning, Rohit Sirohi (Interventional fellows, case assistants)
Ian Hudson (Consultant in charge of patient)
Gail Richardson (Consultant assistant for antegrade approach)
James Spratt* (Co Operator for retrograde approach)
Tony Gershlick (Operator for antegrade and retrograde approach)
Glenfield Hospital, University Hospitals of Leicester NHS Trust
* Forth Valley Acute Hospitals NHS Trust, Edinburgh
National Institute for Health Research,
Leicester Cardiovascular Biomedical
Research Unit

NO CONFLICT OF INTEREST TO DECLARE

Case Summary
• 61yr male
• 1 year history of progressive dyspnoea on exertion with peripheral oedema, clinical evidence of significant right heart failure
Past Medical History
• CABG 2001: LIMA graft to LAD and RIMA graft to RCA
• Mediastinal haematoma evacuated with Right VATS and pericardiectomy in 2004.
• PCI to RCA 2005 for stable angina and occluded RIMA graft
Echocardiogram
• Normal Left and Right Ventricular function
• No valvular pathology

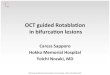
Stress MRI Heart: • Severe compression of anterior RV free wall, extending along undersurface of Right Ventricle. • Ventricular Interdependence consistent with a constrictive physiology • Ischaemia within the anterior and anteroseptal territories

Mediastinal Mass

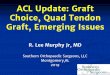
Coronary Angiography

Coronary Angiography
LIMA

Surgical review for removal of mass • Mediastinal mass size and position not suitable for percutaneous drainage
• Open surgical excision of pericardial mass:
- risk of LIMA graft damage with consequent anterior wall infarction or intractable VT during division of LIMA graft
- Surgical risk of perioperative mortality at least 10%
Coronary MDT discussion PCI to CTO LAD: improve antegrade supply to distal LAD and reduce
surgical risk from potential LIMA graft injury
Summary: Mediastinal mass compressing RV leading to constrictive physiology

• Antegrade wire escalation with PT Graphix, Progress 40, Progress 80, Pilot 200, Confianza Pro
• Unable to re- enter distal true lumen
Antegrade approach for CTO LAD (retrograde imaging via LIMA)

Compressive haematoma in left main stem
• Stenting of LMS-LCx, using guideliner to deliver balloons and stents • LMS-LCx stented with 3.0x16mm and 3.5x16mm Synergy stent

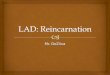
Retrograde Approach from LIMA-LAD, Reverse CART 10 weeks later
• 7F bi-femoral access, 7F EBU3.75 guide catheter to LMS, 7F IMA guide catheter to LIMA • PT Graphix wire positioned into LCx

1. Corsair (RG) to distal LAD via LIMA

3.5x16mm Synergy Stent in LMS
2. Fielder XT (RG) knuckle in sub-intimal space

3. Confianza Pro 12 followed by Miracle 3 (AG) into to sub-intimal space

4. Balloon inflation (AG) on Miracle3 wire to enlarge sub-intimal space

5. Guideliner (AG) via LMS stent struts into sub-intimal space
6. Knuckle wire from RG Corsair to AG guideliner
7. Corsair (RG) into the guideliner
8. RG3 (RG) from retrograde catheter into antegrade catheter and externalised

5. Guideliner (AG) via LMS stent struts into sub-intimal space
6. Knuckle wire from RG Corsair to AG guideliner
7. Corsair (RG) into the guideliner
8. RG3 (RG) from retrograde catheter into antegrade catheter and externalised

9. 3x28mm Synergy Stent into LAD


Final Result

Repeat Coronary Angiogram 2 weeks later

Clinical Progress
• Plan for surgery to remove mass 3 months post PCI
Reviewed by cardiothoracic surgeons • Improved effort tolerance with no dyspnoea. • No signs of right heart failure - in light of symptom improvement surgical intervention deferred - for re-evaluation if symptoms recur

Possible reasons for clinical improvement • Not related to change in mediastinal mass:
- repeat CT confirms no change in size of mass
• Improved flow in LAD following PCI

Learning points
This case illustrates:
• An interesting indication for PCI of LAD CTO with a patent LIMA graft
• reverse CART using a LIMA graft with use of a guideliner to facilitate capture of retrograde corsair through a stented segment.
• Potential issues of stent disruption when performing retrograde procedures in previously stented segments.