Embed Size (px)
Citation preview

Gynecologic Oncology 112 (2009) 490–495
Contents lists available at ScienceDirect
Gynecologic Oncology
j ourna l homepage: www.e lsev ie r.com/ locate /ygyno
Patients with a history of epithelial ovarian cancer presenting with a breast and/oraxillary mass
Amer K. Karam a, Michelle Stempel a, Richard R. Barakat b, Monica Morrow a, Mary L. Gemignani a,⁎a Breast Service, Department of Surgery, Memorial Sloan-Kettering Cancer Center, 1275 York Avenue, MRI Suite 10-26, New York, NY 10065, USAb Gynecology Service, Department of Surgery, Memorial Sloan-Kettering Cancer Center, 1275 York Avenue, New York, NY 10065, USA
⁎ Corresponding author. Fax: +1 212 794 5812.E-mail address: [email protected] (M.L. Gemign
0090-8258/$ – see front matter © 2008 Elsevier Inc. Aldoi:10.1016/j.ygyno.2008.11.006
a b s t r a c t
a r t i c l e i n f oArticle history:
Objective. A breast and/o Received 12 September 2008Available online 20 December 2008Keywords:Ovarian cancerEpithelial ovarian cancerAxillary massBreast axillary mass
r axillary mass in a patient with epithelial ovarian cancer (EOC) may be due to anEOC breast metastasis or a second primary breast cancer. We sought to review our experience with patientswith a history of EOC presenting with a breast and/or axillary mass to determine if clinical features differedbetween these entities.
Methods. Between 1/90 and 10/07, 29 women with epithelial EOC presented with a breast or axillarymass, including 10 patients with EOC metastatic to the breast and/or axilla and 19 patients with a secondprimary breast cancer following their original EOC diagnosis. Clinicopathologic factors/survival wereretrospectively abstracted from medical records.
Results. The mean EOC disease-free survival (DFS) was 14.9 mo versus 77.4 mo (Pb0.001) for patientswith recurrent epithelial ovarian cancer metastatic to the breast and/or axilla and patients with a secondprimary breast cancer, respectively. Similarly, the mean interval between diagnosis of EOC and the breastand/or axillary event was 31.2 mo versus 70.7 mo for those patients who had metastatic recurrent EOC andthose patients with breast cancer (P=0.02). Patients with a second primary breast cancer were more likely tobe diagnosed on mammogram and have a family history of breast and ovarian carcinoma than patients withmetastatic EOC to the breast and/or axilla (14/19 [73.7%] versus 2/9 [22.8%], P=0.02; and 12/18 [66.7%] versus2/10 [20%], P=0.05, respectively). Median overall survival for patients with EOC metastasis was 26 mo butwas not yet reached for those patients with a second primary breast cancer. On univariate analysis, anovarian cancer DFS of 12 mo or more and the performance of breast/axillary surgery were associated with asignificantly longer overall survival (P=0.01 and 0.02, respectively), whereas an elevated CA125 level at thetime of the breast/axilla event and the presence of EOC metastases to the breast and axilla were significantnegative predictors of survival (P=0.01 and 0.05, respectively).
Conclusion. The interval between EOC diagnosis and the breast and/or axilla event, an elevated CA125level, and a family history of breast and/or ovarian cancer may help differentiate patients with metastaticEOC to the breast and/or axilla from those patients with a second primary breast cancer. The presence of ametastatic EOC portends a poor prognosis.
© 2008 Elsevier Inc. All rights reserved.
Introduction
Epithelial ovarian cancer (EOC) is the second most commongynecologic malignancy and approximately 70% of patients presentwith stage III or IV disease [1]. Complete clinical remission can beachieved in as many as 80 to 90% of patients at initial presentationwith the use of maximal surgical cytoreduction and platinum-basedchemotherapy [2,3]. The majority of patients with stage I or stage IIEOC and approximately 15 to 20% of womenpresentingwith advancedstage EOC can be expected to survive beyond five years, and may becured after initial therapy [4]. In patients with a history of ovariancarcinoma who present with a breast and/or axillary mass the
ani).
l rights reserved.
differential diagnosis includes a second primary breast cancer or ametastatic recurrence of the original ovarian carcinoma. We sought toreview our experience with patients with a history of EOC presentingwith a breast and/or axillary mass to determine if clinical features atpresentation and prognosis differed between these entities.
Patients and methods
After Institutional Review Board approval, an institutional data-base at Memorial Sloan Kettering Cancer Center was used toretrospectively identify all patients with a history of epithelial ovariancancer who later presented with a breast and/or axillary massbetween 1/1/1990 to 10/1/2007. Patients with synchronous breastand ovarian carcinomas and patients initially presenting with anovarian carcinoma metastatic to the breast or axillary lymph nodes

Table 1Patient details
Patient Age at EOCdiagnosis
EOCstage
EOC surgeryresidualdisease
Breast oraxillarymass
Detectionmethod
Interval betweenEOC diagnosisand breast/axilla event(months)
Breast/axilladiagnosis
Presence ofother metastasesat the timeof breast/axilla event
Breast/axillasurgery
Family historyof breast/ovarian cancer
Overallsurvival(months)
Statusat lastfollow-up
1 36 3 Microscopic Both Physicalexam
27.2 RecurrentEOC
No ALND Breast cancer 85 AWD(ovary)
2 48 3 ≤1 cm Axilla CT 18.4 RecurrentEOC
Abdominal andregional lymphnodes
None None 25.6 AWD(ovary)
3 56 3 N1 cm Breast Physicalexam
10.8 RecurrentEOC
Abdominal,regional lymphnodes, liver andlung
None None 19.6 DOD(ovary)
4 58 3 ≤1 cm Axilla CT 14.7 RecurrentEOC
No ALND None 56.6 DOD(ovary)
5 53 3 ≤1 cm Breast Mammogram 23.7 RecurrentEOC
Abdominal andregional lymphnodes
None None 30.3 AWD(ovary)
6 55 4 n/a Breast 52.6 RecurrentEOC
n/a Lumpectomy Ovarian cancer 53.2 n/a
7 60 3 N1 cm Breast CT 32.6 RecurrentEOC
Abdominal,regional lymphnodes, liver, lungand bone
None None 33.8 DOD(ovary)
8 69 4 microscopic Axilla Mammogram 27.7 RecurrentEOC
Regional lymphnodes
ALND None 133.4 AWD(ovary)
9 73 3 ≤1 cm Both Physicalexam
8.7 RecurrentEOC
n/a Lumpectomy,ALND
None 16.3 DOD(ovary)
10 76 3 n/a Breast Physicalexam
95.8 RecurrentEOC
No Lumpectomy None 121.8 DOD(ovary)
11 50 3 microscopic Breast Physicalexam
18.0 Secondprimarybreastcancer
No Mastectomy,SLNB, ALND
None 24.7 NED
12 33 3 N1 cm Breast Physicalexam
44.6 Secondprimarybreastcancer
No Lumpectomy,ALND
Breast cancer,BRCA1mutationcarrier
89.3 DOD(ovary)
13 63 1 n/a Breast Mammogram 18.5 Secondprimarybreastcancer
No Lumpectomy,ALND
Breast andovarian cancer,BRCA testingnegative
180.5 AWD(breast)
14 45 3 N1 cm Both Mammogram 119.2 Secondprimarybreastcancer
No Mastectomy,ALND
Breast cancer,BRCA testingresult n/a
152.6 AWD(breast)
15 73 1 Microscopic Breast Mammogram 38.2 Secondprimarybreastcancer
No Lumpectomy,SLNB
Breast cancer 44.1 NED
16 53 3 ≤1 cm Breast Physicalexam
58.0 Secondprimarybreastcancer
No Lumpectomy,SLNB, ALND
None 86.8 DOD(breast)
17 44 3 ≤1 cm Breast Mammogram 63.3 Secondprimarybreastcancer
No Mastectomy,SLNB, ALND
Ovarian cancer 122.4 NED
18 57 1 Breast Mammogram 61.0 Secondprimarybreastcancer
No Lumpectomy,SLNB, ALND
None 120.3 AWD(breast)
19 56 3 N1 cm Axillla Physicalexam
225.0 Secondprimarybreastcancer
No ALND Breast cancer 231.4 NED
20 56 2 Microscopic Breast Mammogram 39.8 Secondprimarybreastcancer
No Lumpectomy,SLNB
n/a 108.6 AWD(ovary)
21 63 3 Microscopic Breast Mammogram 39.7 Secondprimarybreastcancer
No Lumpectomy,SLNB
Breast cancer 108.3 NED
(continued on next page)(continued on next page)
491A.K. Karam et al. / Gynecologic Oncology 112 (2009) 490–495

Table 1 (continued)
Patient Age at EOCdiagnosis
EOCstage
EOC surgeryresidualdisease
Breast oraxillarymass
Detectionmethod
Interval betweenEOC diagnosisand breast/axilla event(months)
Breast/axilladiagnosis
Presence ofother metastasesat the timeof breast/axilla event
Breast/axillasurgery
Family historyof breast/ovarian cancer
Overallsurvival(months)
Statusat lastfollow-up
22 71 1 n/a Breast Mammogram 52.6 Secondprimarybreastcancer
No Lumpectomy,SLNB
None 97.0 DOD(ovary)
23 63 3 N1 cm Breast Mammogram 28.4 Secondprimarybreastcancer
No Lumpectomy,SLNB, ALND
Breast cancer 88.2 NED
24 54 2 ≤1 cm Breast Mammogram 241.0 Secondprimarybreastcancer
No Lumpectomy,SLNB
Breast andovarian cancer,BRCA1mutationcarrier
n/a n/a
25 55 2 Microscopic Breast Mammogram 81.3 Secondprimarybreastcancer
No Lumpectomy,SLNB, ALND
Breast andovarian cancer,BRCA testingnegative
119.0 NED
26 53 3 N1 cm Breast Mammogram 130.7 Secondprimarybreastcancer
No Mastectomy,SLNB, ALND
None 248.4 NED
27 48 3 N1 cm Breast CT 18.8 Secondprimarybreastcancer
No Mastectomy,SLNB, ALND
Breast cancer 43.6 DOD(breast)
28 59 2 Microscopic Breast Mammogram 39.7 Secondprimarybreastcancer
No None Breast cancer 41.5 AWD(breastandovary)
29 54 3 ≤1 cm Breast Mammogram 24.8 Secondprimarybreastcancer
No Lumpectomy,SLNB
None 26.8 NED
Table 2Clinicopathologic characteristics at the time of EOC diagnosis
Characteristic N (%)
Age at initial presentation (years)Mean (SD) 56.3 (10.2)
RaceAsian 2 (6.9)Hispanic 1 (3.4)Caucasian 26 (89.7)
BMI (kg/m2)Median (range) 26.5 (17.8–45.5)
Ovary DFS (months)Median (range) 29.3 (7.5–180.5)
Ovarian cancer histologySerous 18 (62.1)Mucinous 1 (3.4)Endometrioid 6 (20.7)Clear cell 1 (3.4)Other 2 (6.9)N/A 1 (3.4)
Ovarian cancer stageI 4 (13.8)II 4 (13.8)III 19 (65.5)IV 2 (6.9)
Ovarian cancer residual disease≤1 cm 19 (65.5)N1 cm 8 (27.6)N/A 2 (6.9)
Ovarian cancer recurrenceNo 13 (44.8)Yes 16 (55.2)
Table 1 (continued)
492 A.K. Karam et al. / Gynecologic Oncology 112 (2009) 490–495
were excluded. The medical records were retrospectively reviewedand patient demographics as well as presenting features, surgicalprocedures, adjuvant therapy, follow-up and status of the ovariancancer and the breast mass were assessed and recorded.
Stage at initial ovarian cancer diagnosis was retrospectivelyassessed based on the International Federation of Gynecology andObstetrics (FIGO) staging system for ovarian carcinoma [4]. Tumorhistology was obtained from review of pathology reports. Operativereports were reviewed to assess the extent of cytoreduction at initialdiagnosis and breast and/or axillary surgery. Optimal cytoreduction atinitial diagnosis was defined as conditions in which individualresidual tumor nodules measuring ≤1 cm remained after cytoreduc-tion. This definition was chosen based on current GynecologicOncology Group (GOG) definition for initial cytoreduction [5]. Theovarian cancer disease-free survival (DFS) was defined as the timefrom completion of initial therapy to the diagnosis of recurrentdisease. Overall survival (OS) was calculated from the time of thebreast event until the date of last follow-up or death. Disease status atthe time of last follow-up was coded as without evidence of disease,alive with disease breast, alive with disease ovary, dead of diseasebreast, dead of disease ovary or dead of other disease.
Statistical analysis
Descriptive statistics were performed to assess frequency distribu-tions in the study population. Fisher's exact and theWilcoxon sum-of-ranks tests were used to compare variables between metastaticovarian carcinoma and dual primary cases. There were 10 variablesanalyzed for possible prognostic value to predict overall survival.These variables were age at ovarian cancer diagnosis, tumor type,cytoreduction at initial surgery (≤1 cm versus N1 cm), platinum based

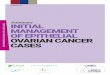
Fig. 1. Overall survival (OS) based on the pathology of the breast and/or axilla mass.
Table 3Variables differentiating ovarian breast metastases from second primary breast cancers
Variable Ovarian metastasis Breast cancer P value
Age at ovarian cancer diagnosisMean years (SD) 58.4 (12) 55.3 (9.4) 0.41
Ovarian cancer histologySerous n (%) 6 (60.0) 12 (66.7)Non-serous n (%) 4 (40.0) 6 (33.3) 1.00
Ovarian cancer stageI, II n (%) 0 (0) 8 (42.1)III, IV n (%) 10 (100) 11 (57.9) 0.03
Ovarian cancer residual disease≤1 cm n (%) 6 (75) 13 (68.4)N1 cm n (%) 2 (25) 6 (31.6) 1.00
Ovarian cancer DFSMean months (SD) 14.9 (6.6) 77.4 (49.4) b0.001
Interval ovarian breast/axilla eventMean months (SD) 31.2 (26) 70.7 (65.1) 0.02
Axillary massYes n (%) 5 (50.0) 2 (10.5)No n (%) 5 (50.0) 17 (89.5) 0.03
Breast/axilla tumor sizeMean cm (SD) 2.8 (1.3) 1.9 (1.1) 0.06
CA 125 at breast and/or axillary eventb35 IU/mL n (%) 4 (57.1) 11 (73.3)≥35 IU/mL n (%) 3 (42.9) 4 (26.7) 0.63
Detection methodMammogram n (%) 2 (22.2) 14 (73.7)Other n (%) 7 (77.8) 5 (26.3) 0.02
Family history of breast/ovarian cancerYes n (%) 2 (20.0) 12 (66.7)No n (%) 8 (80.0) 6 (33.3) 0.05
493A.K. Karam et al. / Gynecologic Oncology 112 (2009) 490–495
chemotherapy, time to first recurrence, interval between ovariancancer diagnosis and the breast event, presence of metastasis outsideof the breast and/or axilla at the time of the breast event, size of thebreast/axillary tumor, breast and/or axillary surgery, adjuvant therapyfollowing breast event. Survival interval probabilities were calculatedby the product-limit method of Kaplan and Meier, and differences insurvival were assessed by the log–rank test. Factors found to besignificant on univariate analysis were then evaluated using multi-variable Cox-proportional hazards methods. P values≤0.05 wereconsidered to be statistically significant.
Results
Twenty nine patients meeting the study inclusion criteria wereidentified (Table 1). The clinicopathologic characteristics of the entirepatient cohort are listed in Table 2. The median age at diagnosis ofovarian cancer was 56 years (range 33.0–76.0 years), and the mediantime to the development of a breast mass was 39.7months (range 8.7–240.9 months) post diagnosis of ovarian carcinoma. Sixteen (55.2%)patients were known to have had a recurrence of their ovarian
Table 4Univariate and multivariate analysis of overall survival
Variable Univariate analysis Multivariateanalysis
OR 95% CI P value P value
Age at EOC diagnosis≥55 0.76EOC stage≥ III 0.24Serous EOC 0.62Residual EOCN1 cm 0.29EOC platinum based chemotherapy 0.83EOC DFS≥12 months 0.12 0.03–0.56 0.01 0.84CA125≥35 at breast/axilla event 8.50 1.49–48.38 0.02 0.12Axillary mass 0.92Breast/axilla surgery 0.04 0.00–0.46 0.01 0.96Breast/axilla tumor sizeb2 cm 0.86EOC breast metastases 3.84 1.02–14.48 0.05 0.81
carcinoma at the time that the breast mass occurred. Fourteen (48.3%)patients had a family history of breast and/or ovarian cancer. Twentytwo (75.9%) patients presented with a breast mass, 4 (13.8%) had anaxillarymass, and 3 (10.3%) had both a breast and an axillarymass. Themedian tumor size was 2.0 cm (range 0.4–5.5 cm). In eight (27.6%)patients the breast and/or axillary mass was discovered on physicalexamination whereas in 20 (69.0%) patients the mass was firstobserved on imaging studies, most commonly mammography (n=16).The etiology of the mass was recurrent EOC in 10 (34.5%) cases, whilethe remaining 19 (65.5%) patients had a second primary breast cancer.Four (13.8%) did not undergo breast and/or axillary surgery, due towidely metastatic recurrent EOC at the time of the breast and/oraxillary event. For those patients with a second primary breast cancer,6 (31.6%) had stage I disease, 9 (47.4%) had stage II disease and 3(15.8%) had stage III disease with one remaining unstaged patients.Eleven patients (57.9%) with a second primary breast cancer wentthrough genetic counseling. Five patients elected to undergo BRCAmutation testing and 2 patients were found to be BRCA1 mutationcarriers. None of the patients with ovarian metastases to the breastwent through genetic counseling or were tested for BRCA mutations.The median follow-up after the breast and/or axillary event was31.1 months (range, 0.7–161.9 months). At last follow-up, five (17.2%)patients were alive with evidence of ovarian cancer, 3 (10.3%) werealive with evidence of breast cancer, and one (3.5%) patient was alivewith evidence of both breast and ovarian cancer. Seven (24.1%)patients died of ovarian cancer, 2 (6.9%) patients died of breast cancer,and 2 (6.9%) patients were lost to follow-up. The remaining 9 patientswere alive and disease free.
Table 3 summarizes the analysis of factors that differentiate thosepatients with recurrent ovarian cancer metastasizing to the breast oraxilla from those patients with a primary breast cancer. The mainfindings are that themean EOC DFS as well as the interval between the
Fig. 2. Overall survival (OS) based on the CA 125 level at the time of the breast and/oraxilla event.

494 A.K. Karam et al. / Gynecologic Oncology 112 (2009) 490–495
diagnosis of EOC and the breast and/or axillary event weresignificantly shorter for those patients with metastatic EOC than forthose with a second primary breast cancer. All ten of the patients withrecurrent EOC metastatic to the breast or axilla had a history of stageIII EOC whereas a significant proportion of patients with a secondprimary breast cancer had a history of stage I or II EOC. Patients with asecond primary breast cancer were more likely to be diagnosed onmammogram and have a family history of breast and ovariancarcinoma than patients with metastatic EOC to the breast and/oraxilla. Conversely patients with metastatic EOC to the breast and/oraxilla were more likely to present with an axillary mass than patientswith a second primary breast cancer. The median overall survival forpatients with EOC metastasis was 26 months and was not yet reachedfor those patients with a second primary breast cancer (P=0.03).
To identify characteristics and findings that may influence overallsurvival we performed both univariate and multivariate analysis(Table 4). Univariate analysis identified an ovarian cancer DFS of12 months or more and the performance of breast/axillary surgery asbeing associated with a significantly longer overall survival (P=0.01and 0.02, respectively), whereas an elevated CA 125 level at the time ofthe breast/axilla event and the presence of EOC metastases to thebreast and axilla were significant negative predictors of survival(P=0.01 and 0.05, respectively). Age at the time of EOC diagnosis,optimal cytoreduction at the time of the EOC diagnosis, EOC stage, theuse of platinum based chemotherapy, the presence of an axillary massand the size of the breast/axilla mass were not predictive of survival.In multivariate analysis, however, none of the variables retained asignificant association with overall survival.
The association between overall survival and EOC DFS, breastand/or axilla surgery, the presence of metastatic EOC to the breastand/or axilla and an elevated CA 125 level at the time of the breast/axilla event was further examined using Kaplan–Meier survivalanalysis. For patients with an initial ovarian cancer DFS of less than12months themedianOSwas 56.6months,whereas for those patientswith an EOC DFS of 12 months or more the median OS was not yetreached (P=0.005). For those patients not undergoing breast/axillasurgery the median OS was 8.8 months, whereas for those patientswhounderwent surgery themedianOSwas not yet reached (Pb0.001).For those patients with recurrent EOC metastatic to the breast and/oraxilla the median OS was 26 months and was not reached for thosepatients with a second primary breast cancer (P=0.03, Fig.1). Similarlyfor those patients with an elevated CA 125 level at the time of breast/axilla event, the median OS was also 24.8 months and was not yetreached for those patientswith a normal CA 125 level (P=0.005, Fig. 2).
Discussion
Studies addressing the long-term outcomes of patients withovarian cancer are limited due to the poor survival seen with latestage ovarian cancer, which accounts for the majority of newlydiagnosed cases. The advent of more aggressive surgical approachesand the use of platinum and taxane based chemotherapy havearguably improved the 5-year overall survival for such patients [2,3].Patients that have been diagnosed with EOC are aggressively followedwith frequent physical examinations as well as radiologic andserologic studies, raising the possibility of detecting a breast and/oraxillary abnormality. Breast and ovarian cancer share severalenvironmental and hereditary risk factors, which could explain theincreased risk of subsequent malignant breast tumors described afterovarian cancer [6]. Conversely, the incidence of breast involvement byother solid malignancies is quite low, accounting for 0.5 to 1.2% of allbreast neoplasms [7–9] with up to 3% of ovarian cancer patients notedto have breast metastases on autopsy [10].
For those patients with a history of EOC who present with a breastand/or axillary mass, an accurate diagnosis should be made becausethe treatment of primary and secondary breast tumors differs. We
found that similarly to prior studies, metastatic disease to the breast ismore likely to present with an axillary mass, thus calling attention tothe lymphatic mode of EOC recurrence, and to be associated withmetastatic disease at the time of diagnosis [11]. Conversely, patientswith a second primary breast cancer were more likely to have ahistory of stage I or II ovarian cancer than patients with breastmetastases due to the lower likelihood of recurrence that is associatedwith early stage EOC as well as the increased number of at-risk years.Patients with a second primary breast cancer were also more likely tohave their tumor detected on mammography than patients withbreast metastases. For the latter, a mass on physical examination or oncomputed tomography was a more common presentation, as haspreviously been reported [12], suggesting a difference in screeningpractices between these two groups with a resumption of screeningmammography in long term EOC survivors. As expected, womenwitha second primary breast cancer were more likely to have a familyhistory of breast and/or ovarian cancer, although this could be due tothe more scrupulous documentation of cancer family history in thosepatients who presented with a second primary breast cancer.
With a median overall survival of just over 2 years, patients whopresented with a metastatic breast and/or axillary mass face a grimprognosis, a finding that has been echoed in 2 other studies examiningthe outcome of patients with metastatic breast and axillary masses[11,12].
In our study, on univariate analysis, variables that were predictorsof improved survival included a prolonged EOCDFS beyond 12months,a normal CA 125 level at the time of the breast event, a diagnosis of asecond primary breast cancer and breast/axillary surgery. Thesedifferences, however, did not hold in the multivariable model, likelydue to the limited number of patients in the analysis and the inherentselection bias that a retrospective analysis introduces in such a smallgroup of patients. This reflects that patients with second primarybreast cancer were more likely to undergo breast/axillary surgery. It isimportant to point out that all 4 patients who did not undergo breast/axillary surgery had widely metastatic ovarian cancer at the time ofthe breast and/or axillary event, which may have contributed to thedecision not to proceed with surgery. Two of these patientssuccumbed to their EOC shortly following the breast and/or axillaryevent (1.2 and 8.8 months, respectively).
Seven of our 19 patients with a second primary breast cancersuffered from a breast cancer recurrence, and 2 died of breastcarcinoma. This rate of recurrence was not unexpected since 12/19patients had positive nodal disease, reflecting either amore aggressivetumor biology, lack of screening due to the prior diagnosis of EOC orlimitations on adjuvant breast cancer therapy imposed by previousovarian cancer therapy. We also found that 4 patients with a secondprimary breast cancer suffered from a recurrence of their original EOC,and 2 died of their disease, emphasizing the need for continuedovarian cancer surveillance in these patients.
In summary, patients with a history of EOC who present with abreast and/or axillary mass may have developed either a secondprimary breast cancer or a metastatic recurrence of their original EOC.It is our practice to continue routine breast cancer screening in ourpatients who are ovarian cancer survivors. On the other hand,screening practices are left to the discretion of the treating physicianand the patient following a recurrence of the EOC. Patients who havefamily histories suggestive of hereditary breast and ovarian cancer areoften referred to genetics and/or our special surveillance program forscreening. A history of recurrent or advanced stage EOC, the presenceof an axillary mass or a shorter interval between the original EOCdiagnosis and the breast and/or axillary event are more likely toindicate metastatic breast involvement. Conversely, patients whosebreast tumor was noted on mammogram, patients with a prolongedinterval between their original EOC diagnosis and the breast and/oraxillary event, and patients with a family history of breast and/orovarian carcinoma were more likely to have developed a second

495A.K. Karam et al. / Gynecologic Oncology 112 (2009) 490–495
primary breast cancer. It remains, however, advisable for clinicians toobtain a biopsy of the breast and/or axillary mass in order to confirmthe diagnosis. In the event of a second primary breast cancer, it wouldbe prudent for the clinician to refer the patient for genetic counseling.The occurrence of EOC metastatic to the breast portends a poorprognosis likely secondary to the presence of concomitant widespreadmetastases. Patients with a second primary breast cancer fare betterbut are still at risk of developing a recurrence of their original EOC aswell as their second breast cancer.
Conflict of interest statementThe authors declare that there are no conflicts of interest.
References
[1] Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer statistics, 2008. CACancer J Clin 2008 (Mar–Apr;58(2):71–96.
[2] Ozols RF, Bundy BN, Greer BE, Fowler JM, Clarke-Pearson D, Burger RA, et al. PhaseIII trial of carboplatin and paclitaxel compared with cisplatin and paclitaxel inpatients with optimally resected stage III ovarian cancer: a Gynecologic OncologyGroup study. J Clin Oncol 2003 (Sep 1;21(17):3194–200.
[3] Vasey PA, Jayson GC, Gordon A, Gabra H, Coleman R, Atkinson R, et al. Phase III
randomized trial of docetaxel-carboplatin versus paclitaxel-carboplatin as first-line chemotherapy for ovarian carcinoma. J Natl Cancer Inst 2004 (Nov 17;96(22):1682–91.
[4] Heintz AP, Odicino F, Maisonneuve P, Quinn MA, Benedet JL, Creasman WT, et al.Carcinoma of the ovary. FIGO 6th Annual Report on the Results of Treatment inGynecological Cancer. Int J Gynaecol Obstet 2006 (Nov;95(Suppl 1):S161–92.
[5] Chi DS, Eisenhauer EL, Lang J, Huh J, Haddad L, Abu-Rustum NR, et al. What is theoptimal goal of primary cytoreductive surgery for bulky stage IIIC epithelialovarian carcinoma (EOC)? Gynecol Oncol 2006 (Nov;103(2):559–64.
[6] Shah S, Evans DG, Blair V, Burnell LD, Birch JM. Assessment of relative risk ofsecond primary tumors after ovarian cancer and of the usefulness of doubleprimary cases as a source of material for genetic studies with a cancer registry.Cancer 1993 (Aug 1;72(3):819–27.
[7] Hajdu SI, Urban JA. Cancers metastatic to the breast. Cancer 1972 (Jun;29(6):1691–6.
[8] McIntosh IH, Hooper AA, Millis RR, Greening WP. Metastatic carcinoma within thebreast. Clin Oncol 1976 (Dec;2(4):393–401.
[9] Alvarado Cabrero I, Carrera Alvarez M, Perez Montiel D, Tavassoli FA. Metastases tothe breast. Eur J Surg Oncol 2003 (Dec;29(10):854–5.
[10] Abrams HL, Spiro R, Goldstein N. Metastases in carcinoma; analysis of 1000autopsied cases. Cancer 1950 (Jan;3(1):74–85.
[11] Recine MA, Deavers MT, Middleton LP, Silva EG, Malpica A. Serous carcinoma of theovary and peritoneum with metastases to the breast and axillary lymph nodes: apotential pitfall. Am J Surg Pathol 2004 (Dec;28(12):1646–51.
[12] Williams SA, Ehlers II RA, Hunt KK, Yi M, Kuerer HM, Singletary SE, et al.Metastases to the breast from nonbreast solid neoplasms: presentation anddeterminants of survival. Cancer 2007 (Aug 15;110(4):731–7.