Embed Size (px)
Citation preview
PatientSafetyStrategyfortheNationalHealthSystem
2015-2020Period
HEALTH2015MINISTRYOFHEALTH,SOCIALSERVICESANDEQUALITY
PatientSafetyStrategyfortheNationalHealthSystem.2015-2020
2
PatientSafetyStrategyfortheNationalHealthSystem
2015-2020Period SANIIDAD2015
MINISTERIODESANIDAD,SERVI HEALTH2015
MINISTRYOFHEALTH,SOCIALSERVICESANDEQUALITY

3
DocumentapprovedbytheInstitutionalPatientSafetyStrategyCommittee
ApprovedbytheNationalHealthSystemInterterritorialCouncilonJuly29,2015.
4
PatientSafetyStrategyfortheNationalHealthSystem
2015-2020Period

5
MINISTRYOFHEALTH,SOCIAL
SERVICESANDEQUALITY
Technicalcoordinationanddrafting
– YolandaAgraVarela.HeadofthePatientSafetyUnit.Sub-directorateGeneralofQualityandCohesion
Sub-directorateGeneralofQualityand
Cohesion:
– PalomaCasadoDurandez.DeputyDirectorGeneralofQualityandCohesion
– InésPalancaSánchez.HeadoftheAccreditationandAuditsUnit
– MaríaJoséGarcíaDíaz.SectionChief.PatientSafety.
– CarmenÁlvarezGonzález.ServiceChief.AccreditationandAudits
DirectorateGeneralofPublicHealth,
QualityandInnovation:
– JoséJavierCastrodezaSanz.DirectorGeneralofPublicHealth,QualityandInnovation
SCIENTIFICCOORDINATION:
– CarlosAibarRemón.HeadofthePreventiveMedicineServiceoftheLozanoBlesaUniversityHospitalClinic.Zaragoza
– PilarAstierPeña.FamilyMedicinePhysician.CaspeHealthCenter.AragonHealthService
– MercedesCarrerasViñas.FormerSubdirectorofCitizenAssistanceandQualityoftheGalicianHealthService.SantiagodeCompostela
– JuanIgnacioGómez-ArnauDiazCañabate.HeadoftheAnesthesiaServiceoftheAlcorconFoundationUniversityHospital.Madrid
– MariaJoséOteroLópez.InstitutefortheSafeuseofMedications(ISMPSpain).UniversityofSalamancaHealthcareComplex-IBSAL
– MercedesPalomarMartínez.ClinicalDirectoroftheCriticalCareUnitsoftheArnaudeVilanovaandSantaMaríadeLéridaHospitals.Lérida
INSTITUTIONALTECHNICALCOMMITTEE
OFTHEHEALTHREGIONS
– ANDALUSIA:ConcepciónBarreraBecerra
– ARAGON:JulianMozotaDuarte– ASTURIAS:ManuelValledorMéndez– BALEARICISLANDS:CarlosCampillo
Artero-BASQUECOUNTRY:EnriquePeiróCallizo– CANARYISLANDS:PalomaGarciade
Carlos– CANTABRIA:TriniValleMadrazo– CASTILE&LEON:MaríaJoséPérez
Boillos– CASTILE-LAMANCHA:FuencislaMartín
Jusdado– CATALUNYA:JosepDavinsiMiralles– CEUTA/MELILLA: María Antonia Blanco
Galán– EXTREMADURA:YolandaAnesdelAmo– GALICIA:BeatrizPaisIglesias– LARIOJA:AdolfoCestafeMartínez– MADRID:AlbertoPardoHernández– MURCIA:SusanaValbuenaMoya– NAVARRE:IsabelRodrigoRincón– VALENCIA:CristinaMaríaNebotMarzal
6
PARTICIPATINGSCIENTIFICSOCIETIES:
– Spanish Association of Medical
Biopathology (AEBM). María ÁngelesCuadradoCenzual
– Spanish Association of Surgeons (AEC).VictorianoSoriaAledo
– Spanish Academy of Dermatology andVenereology (AEDV). Elena de las HerasAlonso
– Spanish Association of Gastroenterology(AEG).XavierCalvetCalvo
– Spanish Association of Health care RiskManagementandPatientSafety(AEGRIS).JoséMaríaRuízOrtega
– Spanish Association of Mental HealthProfessional Neuropsychiatry (AEN).AmaliaTesoroAmate
– Spanish Association of Perfusionists(AEP).MarisolGarcíaAsenjo
– Spanish Association of Primary PediatricCare(AEPAP).JuanRuízCanelaCáceres
– Spanish Association of Clinical Psychologyand Psychopathology (AEPCP). ConsueloEscuderoÁlvaro
– SpanishAssociationofPediatrics (AEPED).AntonioUrdaCardona
– Spanish Association of Major OutpatientSurgery(ASECMA).MatildeZaballosGarcía
– Federation of Associations of CommunityNursing and Primary Care (FAECAP).MaribelMacianMorro
– NationalGroupfortheStudyandAdvisoryin Pressure Ulcers and Chronic Sores(GNEAUPP).J.JavierSoldevillaAgreda
– SpanishSocietyofAngiologyandVascularSurgery(SEACV).SandraRedondoLópez
– Spanish Society of Allergology and
Clinical Immunology (SEAIC). MarReañoMartos
– Spanish Society of PathologicalAnatomy (SEAP). Antonio MartínezLorente
– Spanish Society of Cardiology (SEC).DomingoMarzalMartín
– SpanishSocietyofCareQuality(SECA).RosaMaríaSalazardelaGuerra
– Spanish Society of Thoracic-Cardiovascular Surgery (SECTCV). JuanBustamanteMunguira
– Spanish Diabetes Society (SED). JuanGirbésBorrás
– Spanish Society of Anesthesiology,Resuscitation and Pain Treatment(SEDAR).FernandoGilsanzRodríguez
– Spanish Society of Expert StomalTherapyNursing(SEDE).MaríaAdelinaFernándezGarcía
– SpanishPainSociety(SEDOLOR).RafaelGálvezMateos
– Spanish Society of Intensive Care andCoronary Care Unit Nursing (SEEIUC).RosaGarcíaDíez
– Spanish Society of Endocrinology andNutrition (SEEN). Elena NavarroGonzález
– Spanish Oncology Nursing Society(SEEO).CarmenVenaFernández
– Spanish Society of CommunityPharmacy (SEFAC). Luís GarcíaSevillano
– Spanish Society of Primary CarePharmacists (SEFAP). Ester AmadoGuirado
7
– Spanish Society of Clinical Pharmacology(SEFC).CristinaAvendañoSolá
– Spanish Society of Hospital Pharmacy(SEFH).InmaculadaTorresLloveras
– SpanishSocietyofMedicalPhysics(SEFM).MariaLuisaEspañaLópez
– Spanish Society of Hematology andHemotherapy (SEHH). Pedro SánchezGodoy
– Spanish Society of Immunology (SEI).JavierCarboneCampoverde
– SpanishSocietyofInfectiousDiseasesandClinical Microbiology (SEIMC). Juan PabloHorcajadaGallego
– Spanish Society of Geriatric Medicine(SEMEG).JuanJoséSolanoJaurrieta
– SpanishSocietyofPrimaryCarePhysicians(SEMERGEN). National Member forPatientArea.AlbertoLópezRocha
– Spanish Society of Emergency Medicine(SEMES).PabloBuscaOstolaza
– SpanishSocietyofFamilyandCommunityMedicine (SEMFYC).MaríadelPilarAstierPeña
– Spanish Society of General Practitionersand Family Physicians (SEMG). JuanaSánchezJiménez
– Spanish Society of Internal Medicine(SEMI).RaquelBarbaMartín
– Spanish Society of Intensive Care, CriticalCareandCoronaryCareUnits(SEMICYUC).FranciscoFernándezDorado
– Spanish Society of Nuclear Medicine andMolecular Imaging (SEMNIM). RaquelJoverDíaz
– Spanish Society of PreventiveMedicine, Public Health and Hygiene(SEMPSPH).HenarRebolloRodrigo
– Spanish Society of Nephrology (SEN).ManuelMacíaHeras
– Spanish Society of Neonatology(SENeo).MónicaRiazaGómez
– Spanish Society of Parenteral andEnteral Nutrition (SENPE). MariolaSirvent
– Spanish Society of Medical Oncology(SEOM).JorgeAparicioUrtasun
– Spanish Society of Radiation Oncology(SEOR).JoséPardoMasferrer
– Spanish Psychiatric Society (SEP).MiguelGutiérrezFraile
– Spanish Society of Pneumology andThoracic Surgery (SEPAR). AlbertoCapelasteguiSaiz
– Spanish Society ofDigestive Pathology(SEPD).SenadorMoránSánchez
– SpanishSocietyofRadiationProtection(SEPR).FranciscoJavierRosalesEspizua
– Spanish Society of Clinical Chemistryand Molecular Pathology (SEQC).FranciscoJavierMéridadelaTorre
– SpanishSocietyofRheumatology(SER).JuanÁngelJoverJover
– Spanish Society of Medical Radiology(SERAM).ÁngelMoralesSantos
– Spanish Society of Vascular andInterventional Radiology (SERVEI).MaríaDoloresFerrerPuchol
– Spanish Union of Scientific NursingSocieties (UESCE). Carmen Luisa DíazÁlvarez
8
NATIONALHEALTHSYSTEMCITIZENHEALTHSCHOOLNETWORK
– AssumpcióGonzálezMestre.CatalunyanHealthInstituteExpertPatientProgram
– SergiBlancafortiAlias.Patients’University– EstibalizGamboaMoreno.OsakidetzaExpertPatientProgram– MercedesCarrerasViñas.GalicianCitizenHealthSchool– LuisMarianoLópezLópez.,CantabrianHealthSchool– PilarVicenteGarcía.CitizenTrainersNetwork– CarmenFerrerArnedo.TechnicalDirectoroftheStrategyforDealingwith
Chronicity
OTHEREXPERTSCONSULTED:
– JesúsAranazAndrés.PreventiveMedicineService.RamónyCajalUniversityHospital.Madrid
– JoaquimBañeresAmella.AvedisDonabedianFoundation.Barcelona– JoséJoaquínMiraSolves.MiguelHernándezUniversity.Alicante– MaríaLuisaRamírezVera.RadioactiveandMedicalExposuresDivision.Nuclear
SafetyCouncil.Madrid– CarlosPrietoMartín.MedicalPhysicsService.HealthResearchInstitute.San
CarlosHospitalClinic.Madrid– EnriqueTerolGarcía.DGSANTE.UnitD2HealthCareSystems.European
Commission.Brussels

9

10
TABLEOFCONTENTS
TABLEOFCONTENTS..................................................................................................................................10PRESENTATION...........................................................................................................................................12INTRODUCTION..........................................................................................................................................14TECHNICALNOTE.......................................................................................................................................161.GENERALASPECTS..................................................................................................................................18
a.Justification.........................................................................................................................................18b.Purposeofthestrategy:mission,visionandoverallobjective..........................................................19c.Targetpopulation...............................................................................................................................19d.Situationanalysis................................................................................................................................20
i. Magnitudeandimpactofhealthcare-relatedharm................................................................20ii. Interventionscarriedoutattheinternationallevel......................................................................29
iii.InterventionscarriedoutintheNationalHealthSystem..............................................................502.STRATEGICLINESOFACTION.................................................................................................................80
� Strategiclineofaction1:Patientsafetyculture,humanandorganizationalfactors,andtraining 80� Strategiclineofaction2:Safeclinicalpractices...........................................................................82� Strategiclineofaction3:Riskmanagementandincidentreportingandlearningsystems.........95� Strategiclineofaction4:Patientandcaregiverparticipationfortheirsafety.............................98� Strategiclineofaction5:Researchintopatientsafety..............................................................100� Strategiclineofaction6:Internationalparticipation.................................................................101
3.EVALUATION.........................................................................................................................................1024.GLOSSARY.............................................................................................................................................1045.ABBREVIATIONS&ACRONYMS............................................................................................................1096.LISTINGOFTABLES...............................................................................................................................1127.LISTINGOFFIGURES.............................................................................................................................1138.BIBLIOGRAPHY......................................................................................................................................114

11

12
PRESENTATION
The Ministry of Health, Social Services and Equality (MSSSI) fosters andpromotesthePatientSafetyStrategyfortheNationalHealthSystem(NHS),whichhasbeen being carried out as of 2005 in collaborationwith theHealth Regions and theInstitutoNacionaldeGestiónSanitaria (INGESA), integrating thecontributionsof thehealthcareprofessionalsandofthepatientsbywayoftheirorganizations.
The objectives of this strategy are initially aimed at promoting and furtherenhancingpatientsafetycultureinthehealthcareorganizations,incorporatinghealthcare risk management, training the professionals and patients in basic aspects ofpatient safety, implementing safepractices andgettingpatients and citizensactivelyinvolved.
After ten years of the Patient Safety Strategy development , this update isbeing set out for a further five-year period (2015-2020), in order to provide anoverviewofwhathaspreviouslybeendoneand to facilitatedecisionmakingon thebasisofaconsensusreachedaboutPatientSafetyfortheNHSforthisnewperiod.
Theprocessofassessingwhathasalreadybeendoneentailsrecognizingthat:theestablishedcollaboration,withtheHealthRegions, hasworkedefficientlyHealthRegions; thecontributionsof theprofessionalsandtheirorganizationhasturnedouttobecrucial;thescientificsocietieshaveplayedakeyrole;andthatthepatientsandtheirorganizationshavebeenaninnovativeelementhavingaffordedthepossibilityofmakingprogressinpatientempowerment.
Theupdatepresentedhereinincorporatesthestrategiclinesofactionalreadysetout,includesthecurrentinternationalrecommendationsonthesubjectofpatientsafety,incorporatestheachievementsandstrongpointsattained,proposesobjectivesand recommendations based on the best available evidence, and proposes anassessmentsystemonthebasisofaconsensuswiththeHealthRegionsHealthRegionswhichwillmakeitpossibletomeasurethescopeofthisnewstrategyinastandardizedmanner.
The process of designing this strategy has beenmade possible thanks to thework of the scientific and technical coordinators of the strategy, the institutional
13
technical committeeof theHealthRegionswhichhaveassumed the commitmentoftaking on this update in a rigorous, thoroughmanner, as well as the professionals,through their scientific societies, and the patients who are taking part with theircontributions and commitment and other experts from organizations interested inpatientsafety.
Iwould like to expressmy gratitude to all thosewho have taken part in thepreparationofthisdocument,whichwillundoubtedlycontributetofurtherenhancingpatientsafetyintheNationalHealthSystem.
AlfonsoAlonsoAranegui
MinisterofHealth,SocialServicesandEquality

14
INTRODUCTION
Further enhancing the quality of the health care provided has always beeninherenttotheNHSprinciples,asisinferredfromSpain’sNationalHealthLaw,TitleIof which includes, as one of the measures to be carried out by the health careadministrations, thatofkeepingacheckonand furtherenhancing thequalityof thehealth care provided at all levels thereof1. This law served as the framework ofreferenceonthesubjectofqualityinthehealthcareservices,whichhasbeenfurtherexpandeduponunder the lawsand regulationsof thedifferentHealthRegionsoverthepastfewyears.
It was within this context and under the protection of the 2003 Law onCohesionandQualitythattheMSSSIbegandevelopingtheNHSPatientSafetystrategyin2005 incollaborationwith theAutonomousCommunityadministrations,basedoninternationalrecommendationsandthoseofSpanishexperts2.Thisstrategy,includedin the 2006 Quality Plan3 has served as a tool and framework of reference for theprocess of deploying programs and actions which have progressively been beingcarriedoutinSpainwithregardtopatientsafety.
One of themost important of this strategy’s achievementsworthy of specialmentionare thatworkingnetworksandalliancescreatedaroundpatient safetywiththe Health Regions and INGESA, (when the text refers to the Health Regionsgenerically it is understood that the INGESA included), the professionals and theirscientific societies, the patients, the academic institutions and other organizationsinterested in this subject, which has favored patient safety being included in thequality plans of the Health Regions and the dissemination of the safety culturethroughout the entire NHS. Projects have additionally been carried out which haveaffordedthepossibilityofgainingabetterknowledgeof thesafety-relatedproblemsaffectingtheNHSandthetoolsforpreventingandkeepingacheckonthem.
Thereisstillagreatdealasyettobedonetowardtrulybringingaboutachangein thecultureof theNHShealthcareorganizationsand inorder for the leaders, theclinicsandmanagementorganizationstobecomethedrivingforcebehindthischangewiththeactualactiveinvolvementofthepatientsandtheircaregivers.
Thepatientsafetystrategypresentedhereincontinuesalongthesamelineasthatwhich has been being carried out to date, retaining the same strategic lines of

15
action and incorporating new objectives and recommendations regarding aspectspending furtherdevelopment. Theprocessofpreparing this strategyhas taken intoaccount: the current recommendations of the international organizations, the dataavailable from ten years of having carried out the patient safety strategy, theinformation and opinions provided by the scientific coordinators for the currentstrategy, the Health Regions, the health care professionals (through the scientificsocietieshavingwishedtocollaborate), thepatients (throughtheNHSCitizenHealthSchools Network) and other experts consulted. This strategy is the consensus onpatient safety of those mainly involved in the quality of the care provided by theNationalHealthSystem.
16
TECHNICALNOTE
Thisdocumentiscomprisedofeightperfectlywell-definedparts.
1. General aspects dealing with the justification of the Patient Safety Strategy, itspurposes, the targetpopulationand thesituationanalysis setoutbywayof themagnitude and impact of the harm associated with the process of health carebeingprovided, inconjunctionwith the interventionscarriedoutat thenationalandinternationallevel.
2. Strategy lines maintaining the basic principles of the patient safety strategyalready in the process of being carried out, incorporating objectives and newrecommendations, on the basis of the assessment made as to the process ofcarrying out the strategy per se, the international recommendations and theopinionsofexperts,professionalsandpatients:
• Line1:Patientsafetyculture,humanandorganizationalfactors
• Line2:Safeclinicalpractices
• Line 3:Managementof the risk involved and systems for notificationandlearningfromtheincidents
• Line4:Participationofthepatientsandcitizensfortheirsafety
• Line5:Researchinpatientsafety
• Line6:Internationalparticipation
3. Evaluation including a brief description of the components of the evaluation ofthisstrategywhichwillcompriseaseparatedocument.
4. Glossary of the terms used in the text related to the safety and quality of thehealthcareprovided.
5. Abbreviationsandacronyms
6. Listoftables
7. Listoffigures
8. Bibliography

17

18
1.GENERALASPECTS
a.Justification
Patientsafety,akeydimensionofqualityofthehealthcare,involvescarryingoutstrategiesforreducingallunnecessaryharmtopatientsassociatedwithhealthcare.
The 1999 American Medical Institute report4 led to several governments andinternationalhealthcareorganizationsmakingpatientsafetyoneoftheirhealthpolicypriorities. Hence, the World Health Organization launched the “Alliance for PatientSafety”in2004,promotingactions,toolsandrecommendationsforfurtherenhancingthesafetyinallcountriesworldwide5.In2006,theCouncilofEuropeurgedcountriesto develop policies, strategies and programs for further enhancing patient safety intheir health care organizations6. In June 2009, the European Council launched the“CouncilRecommendationsonpatientsafety,particularlypreventingandcombattinghealthcare-associatedinfections”7.
Inkeepingwiththeinternationalrecommendations,theMSSSImadethedecisionin 2005 to carry out a patient safety strategy for the NHS in collaborationwith theHealthRegions, respecting and further roundingout the actionswhich are currentlybeingcarriedouttherebyintheexerciseoftheirauthoritiesintheprovisionofhealthcareservices.
Theobjectivesof thisstrategyhavemainlybeenaimedat furtherenhancingthepatient safety culture and health care risk management, the training of theprofessionals, the implementation of safe practices, the active involvement of thepatientsandcitizensandinternationalparticipation.
Theepidemiologicalstudiescarriedoutwithintheframeworkofthisstrategyandthedata from theevaluationof theprogramsandactionspromotedat thenationalandregionallevelaffordprecisevalidknowledgeastothedegreeofpatientsafetyintheNHS2.
Aftertenyearsofcarryingoutthisstrategy,thisupdateisbeingsetoutasatoolfor facilitating the process of analyzing, thought being given to and decisions beingmadeon thebasis of a consensus reached concerningPatient Safety for theNHS inaccordancewiththenewneedssetoutandtakingthecurrentsituationintoaccount.

19
Thestrategypresentedhereinisfocusedalongthesamelinesastheprecedingone, and the strategic lines of action proposed are based on the work previouslycarriedout in theNHSaswellason thecurrent international recommendationsandneedsdetectedbytheHealthRegionsandotherpartieswhohavean interest inthissubject.
b.Purposeofthestrategy:mission,visionandoverallobjective
Vision:
This strategy is aimed at being a reference point element for the furtherenhancementofpatientsafetyintheNHS,takingintoaccounttheevidenceavailablefrom the recommendationsmade, the feasibility of their implementation, aswell astheequityandsustainabilityofthesystem.
Mission:
Setting objectives and making recommendations aimed at minimizing the risksinvolvedintheprocessofprovidinghealthcareandreducinghealthcare-relatedharm.
OverallObjective:
Further enhancing patient safety at all levels in all settings in which care isprovidedintheNationalHealthSystem.
c.Targetpopulation
This strategy targets all patients and citizens for whom health care is providedwithin the NHS, the professionals (both clinical and managerial), the health careorganizationsandprovidersintheNHSandallthoseacademicinstitutionsandagentsinvolvedinfurtherenhancingpatientsafetyinSpain.
20
d.Situationanalysis
i. Magnitudeandimpactofhealthcare-relatedharm
Ø Frequencyofadverseevents
Different epidemiological studies published as of the 1990’s havemade amajorcontributiontowardascertainingthemagnitude, impactandcharacteristicsofhealthcare-relatedadverseevents8,9,10,11,12,13,14,15,16,17,18,19,20..Thedifferentobjectivessetandthe different methodologies employed in these studies are the reason for thedifferencesfoundinthefrequencyofadverseevents(Fig.1).
A systematic review of the year 2008 revealed the average incidence ofhospitalization-related adverse events to have been 9.2% (95% CI: 4.6% – 12.4%), atotalof43.5%(95%CI:39.4%–49.6%),ofwhichcouldhavebeenprevented.Atotalof7% of the adverse events identified could lead to a permanent disability, and 7.4%could be directly related to the patient’s death21. Despite harm apparently beingcaused infrequently to patients, some experts point out that this data may beunderestimated,giventhatthesestudiesdonotincludetheadverseeventsfollowingdischargefromhospital22.Ontheotherhand,someexpertsalsorecommendtheneedofusingdifferentmethodologies soas tobeable tobetterdetect theoccurrenceofadverseevents23.
In the European Union, the frequency of adverse events among hospitalizedpatients is within the 8% - 12% range24, one death being caused for every 100,000inhabitantsperyearasaresultofsaidadverseevents,meaningaround5,000deathsper year. Nevertheless, it seems that these figures could also be underestimated,becausetheyarebasedondatarecordedbytheprofessionals25.

21
Fig.1.Listofstudiesconductedforthepurposeofascertainingtheincidenceofadverseeventsinhospitals
The starting point for ascertaining the magnitude and the determining factorsinvolved in healthcare risk in Spain have been the ENEAS15, APEAS26, EARCAS27 andSYREC28 studies promoted by the MSSSI. The EVADUR29 study carried out by theSpanish Society for EmergencyMedicinehas alsoprovideduseful information in thefieldofemergencycare.
– National Study on Hospitalization-Related Adverse Events (ENEAS Study): Aretrospectivestudyofacohortof5,624patientshospitalizedat24publichospitalsinSpain formore than24hours anddischargedwithin the June4-10, 2005period (allinclusive). A total of 42,714 days of hospital stays were studied. The incidence ofpatientswith adverse events related to the care providedwas of 9.3% (525/5,624),(95%CI: 8.6% -10.1%). The incidence density was of 1.2 adverse events per 100patients/day (95%CI1.1–1.3). Theactual incidenceofpatientswith adverseevents
NewYork
(30,19
5)
Utah/Col
(14,70
0)
Australia
(14,17
9)
Australia
adjusted
NewZealand
(6,579)
U.K.(1
,014)
Denm
ark
(1,097)
Cana
da
(3,745)
Spain
(5,624)
France
(8,754)
Netherland
s(7,926)
Swed
en
(1,967)
Brazil
(1,103)
Tunisia
(602)

22
relateddirectly to thehospital care (not including those referred fromprimary care,externalofficesandcausedatanotherhospital)wasof8.4%(473/5,624),(95%CI:7.7%-9.1%).Addedtotheactualincidencearethosecasesinwhichanadverseeventhadbeenthereasonforadmissiontohospitalinordertooffsettosomedegreethelossesforpost-dischargeadverseevents.
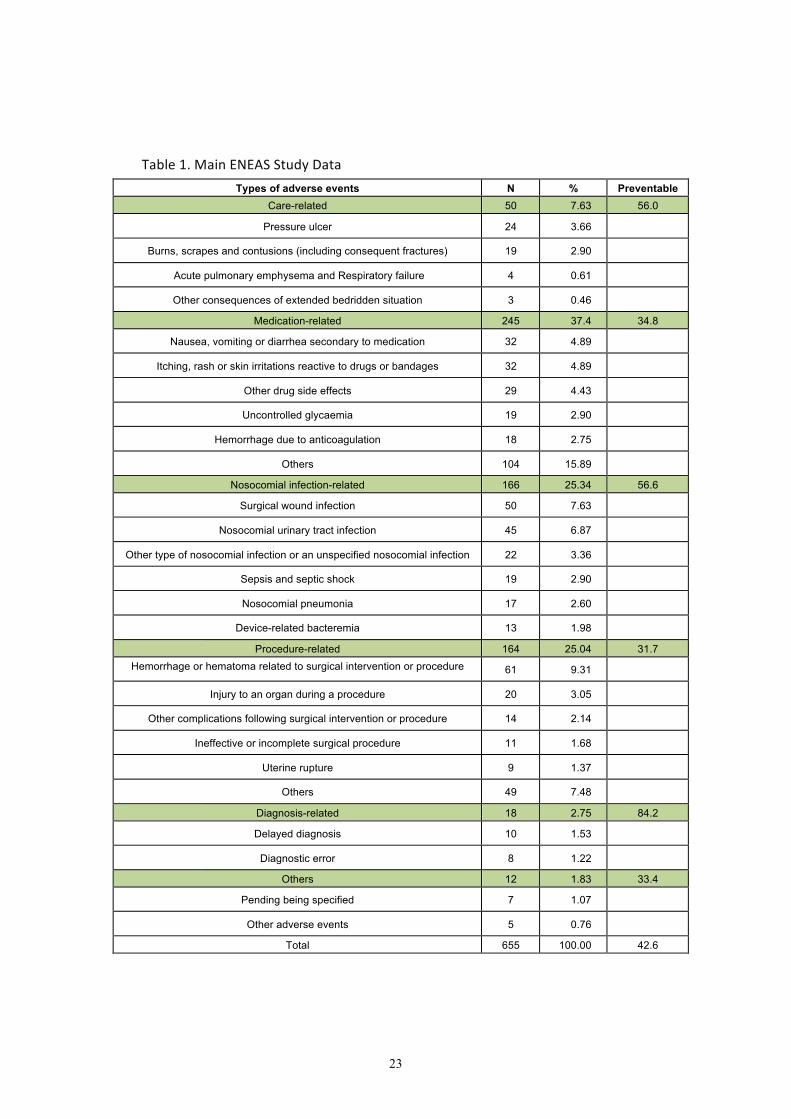
A total of 37.4% of all adverse events were related to the medication, whilstnosocomial infectionsof any type totaled25.3%and25%were related to technicalproblems during a procedure. A total of 45% (n=295) of the adverse events wereconsideredmild,38.9%(n=255)moderateand16%(n=105)severe.Inall,42.8%oftheadverseeventswereconsideredpreventable15,30,31,32.(Table1).
23
Table1.MainENEASStudyDataTypes of adverse events N % Preventable
Care-related 50 7.63 56.0
Pressure ulcer 24 3.66 Burns, scrapes and contusions (including consequent fractures) 19 2.90
Acute pulmonary emphysema and Respiratory failure 4 0.61 Other consequences of extended bedridden situation 3 0.46
Medication-related 245 37.4 34.8
Nausea, vomiting or diarrhea secondary to medication 32 4.89 Itching, rash or skin irritations reactive to drugs or bandages 32 4.89
Other drug side effects 29 4.43 Uncontrolled glycaemia 19 2.90
Hemorrhage due to anticoagulation 18 2.75 Others 104 15.89
Nosocomial infection-related 166 25.34 56.6
Surgical wound infection 50 7.63 Nosocomial urinary tract infection 45 6.87
Other type of nosocomial infection or an unspecified nosocomial infection 22 3.36 Sepsis and septic shock 19 2.90 Nosocomial pneumonia 17 2.60
Device-related bacteremia 13 1.98 Procedure-related 164 25.04 31.7
Hemorrhage or hematoma related to surgical intervention or procedure 61 9.31 Injury to an organ during a procedure 20 3.05
Other complications following surgical intervention or procedure 14 2.14 Ineffective or incomplete surgical procedure 11 1.68
Uterine rupture 9 1.37 Others 49 7.48
Diagnosis-related 18 2.75 84.2
Delayed diagnosis 10 1.53 Diagnostic error 8 1.22
Others 12 1.83 33.4
Pending being specified 7 1.07 Other adverse events 5 0.76
Total 655 100.00 42.6

24
– Study on patient safety in primary care (APEAS Study): A prevalence studyconducted on an opportunity sample from 48 primary care centers in 16 HealthRegions, inwhich452professionals tookpart.A studywas conductedof the96,047patientswhocameinforappointmentsoverthecourseofatwo-weekperiodinJune2007.
Theobservedprevalenceofadverseeventswasof11.18‰oftheprimarycareconsultations(95%CI:10.52–11.85).Theprevalenceofpatientshavingsomeadverseeventwasof10.11‰(95%CI:9.48–10.74).Atotalof6.7%ofthepatientshadmorethan one adverse event. A total of 54.7% (n=606) of the adverse events wereconsideredmild,38.0%(n=421)moderateand7.3%(n=81)severe.
A total of 47.8%of the adverse events (n=530)weremedication-related, 8.4%(n=93)involvinghealthcare-associatedinfectionsofanytype,atotalof10.6%(n=118)beingrelatedtosomeprocedureand6.5%(n=72)tothecareprovided.
Themajority of the adverse events (64.3%)were considered preventable, andsolely5.9%weresevere,themajoritybeingmedication-related33,34.
– Adverseeventsatsocialhealthcentersandnursinghomes(EARCASStudy):Aqualitativestudyconductedinseveralstagesaimedaavailingofaninitialapproachtopatientsafetyinaverage-length-of-stayandextended-stayhospitalsandsocialservicesinSpain,inwhichmorethan950expertsfromnearly100centersandinstitutionsfromallofSpain’sHealthRegionstookpart.
Accordingtothestudyfindings,themostcommonincidentsandadverseeventsarerelatedtothecareprovidedtothepatients,theuseofmedicationandhealthcare-associated infections.Themostoutstanding factorswhichcontribute to theonsetoftheseincidentsandadverseeventsarethoserelatedtothepatient’svulnerability.
Themagnitudeofthisproblem,setoutinthestudyfindings,revealstheneedforidentifyingandcarryingoutstrategiesforfurtherenhancingpatientsafetyinthesocialservicesandmedicalcaresettings27.
– Incidentsandadverseeventsinintensivecaremedicine.Safetyandriskinthecritical patient (SYREC Study):A prospective cohort study conducted on 79 Spanishintensive careunitsbasedon the reportingof incidentsby theprofessionalsproper.The risk of experiencing a harmless incident as a result of being admitted to anintensive care unit, given as a median figure, was of 73%, and a 40% risk ofexperiencing an adverse event. The adverse eventswhich occurredmost frequently

25
werethoserelatedtocareprovidedandhealthcare-associated infections.A totalof90% of all the harmless incidents and 60% of the adverse eventswere classified aspreventableorpossiblypreventable35.
– Adverse events linked to the care provided in Spain’s hospital emergencyservices (EVADUR Study):A prospective study conducted on 21 emergency serviceswithintheOctober–December2009period.Thehealthcareprovidedtoasampleof3,854patientswasfollowedoverthecourseofaseven-dayperiod.Atleast12%ofthepatients forwhom carewas provided in an emergency servicewere affected by anincident, and 7.2% experienced an incident involving harm. Evidence was found ofimproper action in 54.6% of these cases. The factors associated with the incidentswere related to the use of medications, delayed diagnosis and breakdown incommunication.Atotalof70%oftheadverseeventswereconsideredpreventable29.
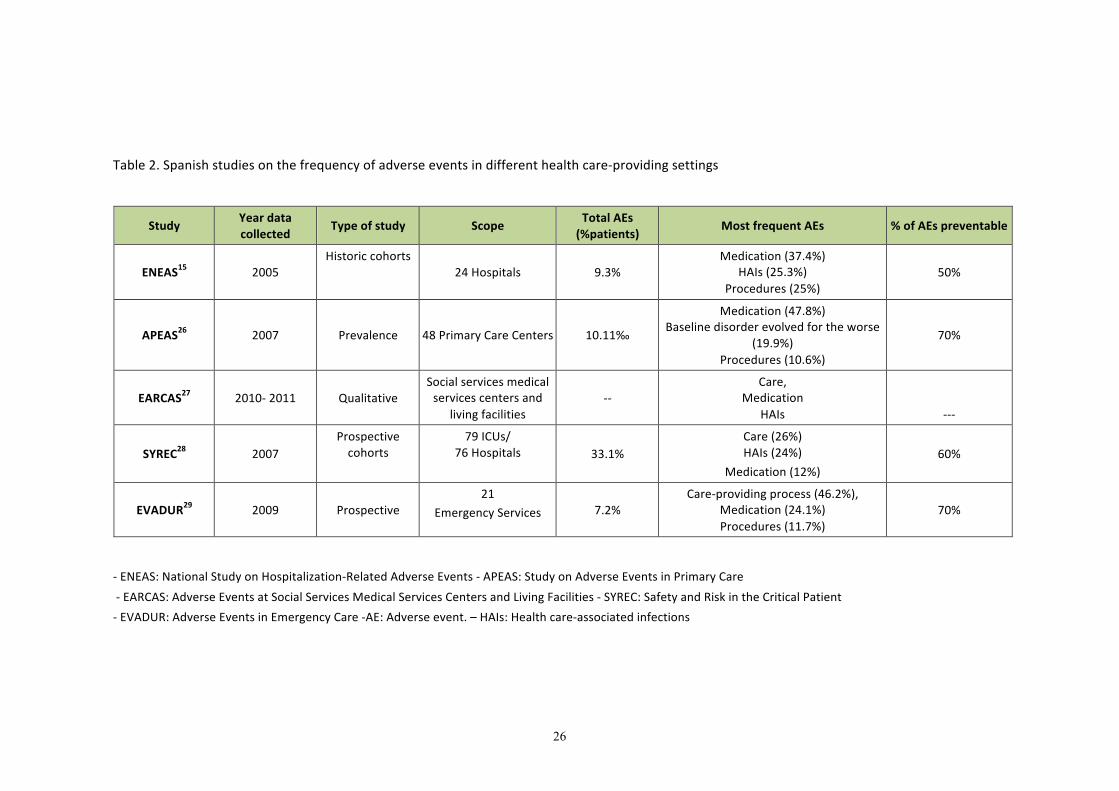
Table 2 provides a summary of the characteristics andmain findings of thesestudies.
26
Table2.Spanishstudiesonthefrequencyofadverseeventsindifferenthealthcare-providingsettings
Study Yeardatacollected Typeofstudy Scope TotalAEs
(%patients) MostfrequentAEs %ofAEspreventable
ENEAS15 2005Historiccohorts
24Hospitals 9.3%Medication(37.4%)
HAIs(25.3%)Procedures(25%)
50%
APEAS26 2007 Prevalence 48PrimaryCareCenters 10.11‰
Medication(47.8%)Baselinedisorderevolvedfortheworse
(19.9%)Procedures(10.6%)
70%
EARCAS27 2010-2011 QualitativeSocialservicesmedicalservicescentersand
livingfacilities--
Care,Medication
HAIs ---
SYREC28 2007Prospectivecohorts
79ICUs/76Hospitals 33.1%
Care(26%)HAIs(24%)
Medication(12%)60%
EVADUR29 2009 Prospective
21
EmergencyServices 7.2%Care-providingprocess(46.2%),
Medication(24.1%)Procedures(11.7%)
70%
-ENEAS:NationalStudyonHospitalization-RelatedAdverseEvents-APEAS:StudyonAdverseEventsinPrimaryCare
-EARCAS:AdverseEventsatSocialServicesMedicalServicesCentersandLivingFacilities-SYREC:SafetyandRiskintheCriticalPatient
-EVADUR:AdverseEventsinEmergencyCare-AE:Adverseevent.–HAIs:Healthcare-associatedinfections

27
According to the results of these studies, it can be said that the incidence ofadverse events related to the careprovided and the spreadby categories in Spain’shospitals is similar to that of the studies conducted in American and Europeancountriesemployingasimilarmethodology.TheENEASStudyservedtomakefollowingthe recommendations based on evidence a strategic priority on theNHS agenda, todisseminate best practices and to put the available knowledge into practice as aguarantee of clinical safety. The APEAS study served the purpose of revealing that,althoughthefrequencyofadverseeventswaslowandseveretoonlyascarcedegreeattheprimary level,themulti-causaletiology,thehighprobabilityofpreventionandtheexistinghighdegree towhichprimary care is frequentedwarrantedundertakingactionsaimedatfurtherenhancingpatientsafetyatthiscare-providinglevel.
Ø Citizenopinions
Atotalof53%ofallEuropeanUnioncitizensareoftheopinionthattheycouldbeharmedonundergoinghospitalcare(40%inoutpatientcare).Additionally,atotalof27% of those surveyed (23% in Spain) stated that either they themselves or theircaregivershavebeenharmedatsometimeintheprocessofhospitalcare36.
In Spain, the Health care Barometer conducted in 2010 revealed that 11.7% ofthose surveyed reported either they, themselves, or their caregivers havingexperienced an error during the consultation with the specialist, 11.5% during ahospitalstay,9.6%inaprimarycareconsultationand8%intheemergencyservices37.
Ø Thecostofadverseevents
Inviewofthedifficultyofassessingthecostoftheharminvolvedinprovidinghealth care and the savings entailed on implementing patient safety programs, arecent publication suggests several tools for assessing the costs associated withadverseeventsandthecost-effectivenessofthepracticesfortheirprevention38.
InSpain,twoarticlespublishedareworthyofspecialmention.Thefirstarticleestimatesthatthecostsofunsafenessrelatedtomedication,nosocomialinfectionandsurgicalproceduresinhospitalizedpatientsin2011hasentailed2.474millioneurosforSpain’sNationalHealthSystem39.ThisarticlebasedonthestudyofcostsofunsafenessconductedbytheMSSSI in200840,forwhichtheresultsasperthehospitalrevenuesandtheConsumerPriceIndexfor2011wereupdated.Thesecondarticleevaluatestheeconomic impactof the incidenceofadverseeventsonhospitalcare inSpainonthebasis of the data at discharge from hospital of patients for whom care has been
28
provided bymeans of admission to the hospitals belonging to the Spanish HospitalCostsNetworkduringthe January1,2008–December21,2010period.The findingsshow the total incremental costs of the adverse events to be 88,268,906 €, anadditional6.7%addedontothetotalhealthcarespendingfigure41.
Inshort,afternearly tenyearsofworkingonpatientsafety inSpain,wecansaythat:
a) Sufficient knowledge exists regarding the frequency and distribution of theadverseevents,aswellasthecontributingfactorsinallareasofhealthcare:acute hospitals, intensive care, emergency care, average-length-of-stay andextended-stayhospitalsandprimarycare.
b) Around9-12%ofthepatientsforwhomcareisprovidedinhospitals,bothinhospitalizationandemergencycare,and1.2%ofthepatientsforwhomcareisprovidedatprimarycarecentersexperiencesomeadverseeventrelatedtothecareprovided.These figuresare similar to those found toexist inothercountries.
c) Thepercentagesofpreventability,weretheavailableknowledgetobeputintopractice,areofmajorimportance,rangingfrom50%to70%dependingonthetypeofadverseeventandcare-providingsettinginquestion.
d) Moderatetohigh-qualityevidenceexistsastotheimportanceandusefulnessof implementing safe practices and procedures. Very little research hashoweverbeendoneontheimplementationandevaluationofthesepractices.Inotherwords:weknowwhatshouldbedone,butwedon’tknowifwearedoingsototheextentitshouldbedone42.
e) It is estimated that the costs resulting from adverse events and theopportunitiesmissedasaresultofnotdoingwhatshouldbedoneadduptoamajorpercentageofhealthcarespending.
f) In short, theadverseevents related to thehealthcareprovidedareapublichealth problem due to their magnitude, far-reaching importance andpreventability.
29
ii.Interventionscarriedoutattheinternationallevel
Patient safetyhasalwaysbeena focalpointof theattentionandeffortsof thehealth care professionals and institutions 43, although the importance thereof wasparticularlybroughttoforeasofthereport“ToErrIsHuman:BuildingaSaferHealthcareSystem”,publishedin1999bytheU.S.MedicalInstitute4.Thisreportservedasaguide for themain international health care organizations for developing strategiesand recommendation for cultivating the control of the preventable harm in healthcare.
INTERNATIONALORGANIZATIONSINTERESTEDINPATIENTSAFETY
Some of themost outstanding international organizations interested in patientsafetywhichhavehadthegreatestinfluenceonSpain’ssafetypoliciesinparticulararethe World Health Organization, the Pan American Health Organization, theOrganization forEconomicCooperationandDevelopment, theEuropeanCouncilandtheEuropeanUnioninstitutions(particularlytheEuropeanCommission).
� WorldHealthOrganization(WHO)
In2004, theWorldHealthOrganization launchedtheWorldAlliance forPatientSafety, currently referred to as the Patient Safety Program,which includes differentchallenges and actions for further enhancing patient safety at the worldwide level,someofthemostoutstandingofwhichare:
o Challenges:
Programsdealingwithsignificantrisksforthepatientsforwhomcareisprovidedwhich are relevant for all of the countries pertaining to the World HealthOrganization:
– Clean care is safer care44. Its top-priority objective is to assure thatimprovinghandhygieneisontheagendaofthehealthcareorganizationsforpromotingthepreventionofhealthcare-associatedinfectionsandtheirconsequences.
– Safe surgery saves lives45. This program revolves around the surgicalchecklistasatoolforfurtherenhancingsafetyinsurgery.
– Combatting antimicrobial resistance46. Third challenge launched by theWorld Health Organization in 2010 for promoting the reasonable use ofantibiotics in humans, in veterinary medicine and agriculture and

30
promoting research in this field. As of May 2014, the World HealthOrganization undertook the commitment of developing a global plan foraction formeeting the challengewith resistance toantibioticsmeans forhumanhealth47.
o Mainactions:
Someofthemainactionsworthyofspecialmentionare:
– Patientsforpatientsafety.AimedatcreatingaPatientsandConsumersforPatientSafetyNetwork48.
– Reportingandlearningsystems49.– Knowledgemanagement50.
– Safeclinicalpractices51.
InFebruary2012,theWorldHealthOrganizationpromotedameetinginGenevaonSafetyinPrimaryCareforthepurposeofanalyzingthedataavailableonfrequency,characteristics and possibilities of prevention and severity of adverse events and toassess the challenges in view of a situation of economic crisis and the possibility ofsettingupcommonstudiesamongcountries52.Theparticipantsplacedtoppriorityona number of recommendations for further enhancing patient safety in primary care(Table3).

31
Table 3. Top-priority recommendations for further enhancing patient safety in primarycare
Top-priorityrecommendationsinprimarycare
Trainingtheprofessionalsinpatientsafety
Promotingpatientsafetystudiesemployingdifferentmethodologies
Developingpoliciesforpromotingpatientsafetyinprimarycare
Improvingthedefinitionsconcerningerrorsandtheirclassification
Facilitatinglearningfrompasterrors
Assuringthatthesystemsforfurtherenhancingpatientsafetyinprimarycareareputintopractice
On the road map to be followed, it was considered important to avail of someguidelinesonpatient safety inprimary carebypromoting a systematic focuson thesameandmakingsuggestionsforimprovementbothinthemanagementaswellasthecare-providingaspects.
The World Health Organization promoted the study Prevalence of adverseevents in Latin American hospitals (IBEAS Study) carried out in collaboration withSpain’s MSSSI and five countries in the region, being the first study to have beencarriedoutona largescale inLatinAmericaformeasuringtheadverseevents inthehospitals.TheIBEASstudypositionedSpainasabenchmarkcountryinpatientsafetyintheSpanish-speakingworld53,54.
• PanAmericanHealthOrganization(PAHO)
The PanAmericanHealthOrganization has been carrying out the CareQualityandPatient SafetyProgram55within the frameworkofwhichdifferentprojectshavebeencarriedout,someofthemostnoteworthyofwhichare:
o SystemsforreportingincidentsinLatinAmericawhichtakeininformationondifferent reporting systems in the region and recommendation for theirimplementationanddevelopment.
o AdverseEventsinpatientsforwhomcareisprovidedintheoutpatientcareservicesinLatinAmerica-AMBEASStudy.Themainobjectiveofthisresearchwastoassessthefeasibilityofcarryingoutthistypeofstudiesintheregion,aswell as ascertaining the frequency, characteristics and preventability ofadverseeventsamongthepopulationunderstudy56.Thisstudywasconducted
32
in response to the interest of the countries in the region in broadening theknowledgeonpatientsafetyandcomprisingpartofthestrategylinessetoutunderResolutionCSP27.R10ofOctober5,2007:“RegionalPolicyandStrategyfortheGuaranteeofQualityinHealthCare,includingpatientsafety”57.
� OrganizationforEconomicCooperationandDevelopment(OECD)
TheOrganization forEconomicCooperationandDevelopment setupaworkingsubgroup of patient safety indicators in 2007 for the purpose of developinghomogeneous indicatorsonthebasisofadministrativedatabaseswhichwouldmakeevaluationandcomparisonamongcountriespossible58,59.
AstudywasconductedwithintheSpanishscopeforthepurposeofdeterminingthe empirical validity of the PS indicators and preventable hospitalization for theevaluationofthequalityofthehealthcareproviders60.
� CouncilofEurope
The Warsaw Declaration for Patient Safety of 2006 recommended includingpatientsafetyasapriorityonthenationalandinternationalagendas,cooperatingwiththeCouncilofEurope61,theEuropeanCommissionandtheWorldHealthOrganizationforassuringtheimplementationofpatientsafetyactions.
Itrecommendedthefollowingstrategylinesbecarriedout:
– Promotingapatientsafetyculturewithasystematicfocus
– Settingupincidentreportingsystemsforlearninganddecision-making
– Getting thepatients and citizensactively involved in furtherenhancingsafety
� EuropeanUnion(EU)
– European Commission. For the purpose of providing the population
withahighdegreeofhealthprotection62andsupportingtheMemberStates in achieving safe health care, the European Commission hascarriedoutdifferent actions, coordinatingor supporting theactivitiesand projects in which the Member States, the professionals andpatientsandmostoftheorganizationsandinstitutionswhichhaveaninterestinthissubjecthavetakenpartorarecurrentlytakingpart.
– LuxembourgDeclarationonPatientSafety.ADeclarationwhicharoseoutofaconferenceorganizedduringLuxembourg’spresidencyof the

33
EuropeanUnion,withtheslogan:“PatientSafety–MakingitHappen!”IncludingspecificrecommendationsonpatientsafetyattheEuropeanUnion,nationalandlocallevels63.
– QualityandPatientSafetyWorkingGroup.AGroupworkingundertheHigh-LevelGrouponHealth Services andMedical Care and set upbyway of a European Commission decision in April 2004. This groupcontributed considerably to the proposal of the Council of theEuropeanUnionRecommendationsonpatientsafetyandhealthcare-associated infections. This group serves as a platform for sharinginformation on actions underway, priorities and innovative solutionswith a view to the EuropeanUnion’s patient safety and care quality-relatedchallenges.ThisgroupiscomprisedofrepresentativesfromtheEuropean Commission, the Member States, the World HealthOrganization, the Organization for Economic Cooperation andDevelopmentandotherinterestedparties64.
– Joint actions of the Member States. Most of the European Unioncountries have been working together on two consecutive projectsfundedbywayoftheEuropeanUnionpublichealthprogram.
o EuropeanUnionNetwork for Patient Safety: EUNetPaS.Carriedout within the 2008-2010 period for the purpose of promotingnetworksforcollaborationinpatientsafetyforsharingknowledgeandexperiencesatthenationalandEuropeanUnionlevels65.
o EuropeanUnionNetworkforPatientSafetyandQualityofCARE:PaSQ. Joint action between the European Commission and theEuropean Union countries aimed at promoting theimplementation of the Council of the European Unionrecommendations, promoting the sharing of knowledge andexperiences in the field of patient safety and care quality andfavoring a sustainable collaboration network in the EuropeanUnionrevolvingaroundcarequalityandpatientsafety66.
34
– Recommendationsof theCouncil of theEuropeanUnion concerning
patient safety, including prevention and control of health care-
associatedinfectionsofJune2009.
ThisRecommendationiscomprisedoftwochapters7:
• Thefirstchapter,devotedtopatientsafety,makesreferencetoanumberofrecommendations,includingthedevelopmentofnationalpolicies,patienttraining,settingupadverseeffects-relatedinformationand learningsystems, thepromotionof theeducationand trainingofhealth care workers and carrying out research. It also invites theMember States to share patient safety-related best practices andknowledge.
• The second chapter, devoted to health care-associatedinfections, recommends that theMember States adopt a strategy forthe prevention and control of health care-associated infections andthat they set up an intersectorial mechanism for the coordinatedimplementationofthisstrategy(measuresatthenationalandregionallevel and at the level of the health institutions: surveillance systems,education and training of professionals and patients, in addition toresearch).
In 2012, the European Commission published an executive reportaddressing the Council on the implementation of these recommendations,based on the answers given by the Member States on a standardizedquestionnaire.Theactions recommendedhadnotbeen fully implementedbyall of the countries, a further one-year time frame therefore having beenallowedfortheimplementationthereof.
Spainwas one of the countrieswhich had implemented 10-12 of thetotal13patientsafety recommendationsmade67. In June2014, theEuropeanCommissionmadeasecondconsolidatedreportontheimplementationoftheCouncilRecommendationsonpatient safetypublic 68. Inviewof the findings,theCommissionsets forthseven(7)suggestedareasat theendof thereportforworkingincollaborationwiththeMemberStates(Table4):
35
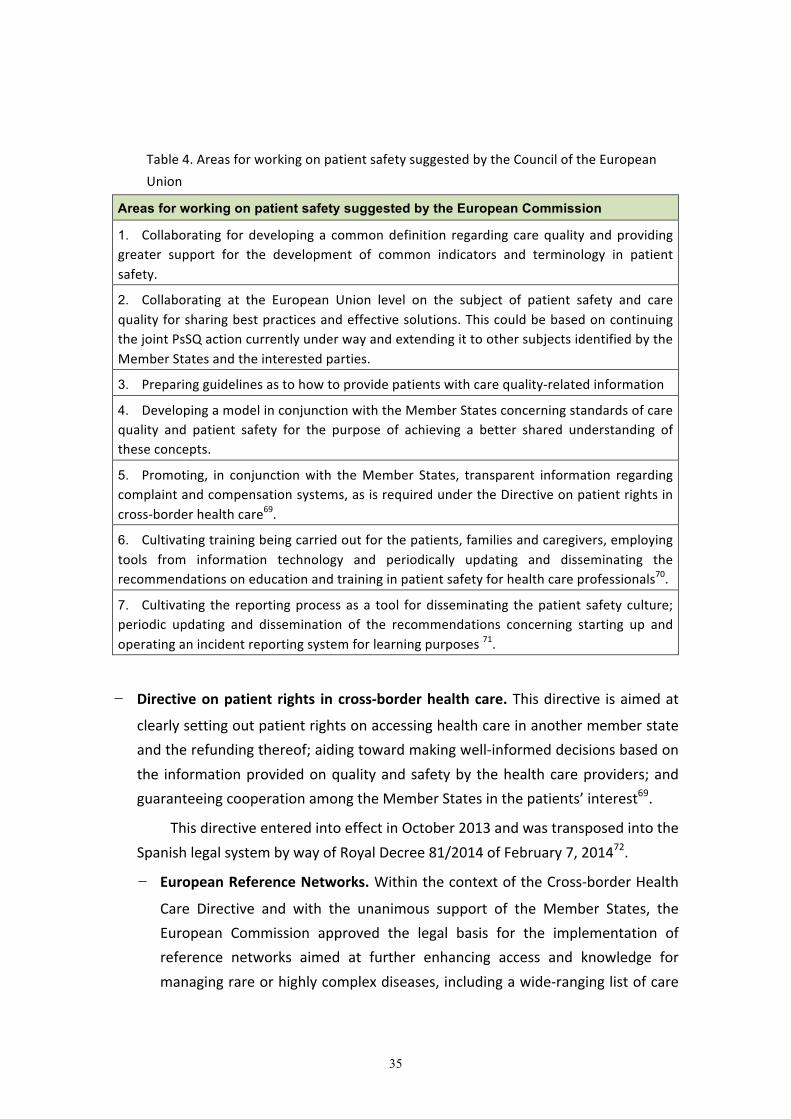
Table4.AreasforworkingonpatientsafetysuggestedbytheCounciloftheEuropeanUnion
Areas for working on patient safety suggested by the European Commission
1. Collaborating fordevelopinga commondefinition regarding carequality andprovidinggreater support for the development of common indicators and terminology in patientsafety.
2. Collaborating at the European Union level on the subject of patient safety and carequalityforsharingbestpracticesandeffectivesolutions.ThiscouldbebasedoncontinuingthejointPsSQactioncurrentlyunderwayandextendingittoothersubjectsidentifiedbytheMemberStatesandtheinterestedparties.
3. Preparingguidelinesastohowtoprovidepatientswithcarequality-relatedinformation
4. DevelopingamodelinconjunctionwiththeMemberStatesconcerningstandardsofcarequality and patient safety for the purpose of achieving a better shared understanding oftheseconcepts.
5. Promoting, in conjunctionwith theMember States, transparent information regardingcomplaintandcompensationsystems,asisrequiredundertheDirectiveonpatientrightsincross-borderhealthcare69.
6. Cultivatingtrainingbeingcarriedoutforthepatients,familiesandcaregivers,employingtools from information technology and periodically updating and disseminating therecommendationsoneducationandtraininginpatientsafetyforhealthcareprofessionals70.
7. Cultivating the reportingprocessasa tool fordisseminating thepatient safety culture;periodic updating and dissemination of the recommendations concerning starting up andoperatinganincidentreportingsystemforlearningpurposes71.
– Directiveonpatient rights incross-borderhealthcare.Thisdirective isaimedat
clearlysettingoutpatientrightsonaccessinghealthcareinanothermemberstateandtherefundingthereof;aidingtowardmakingwell-informeddecisionsbasedonthe informationprovidedonqualityandsafetyby thehealthcareproviders;andguaranteeingcooperationamongtheMemberStatesinthepatients’interest69.
ThisdirectiveenteredintoeffectinOctober2013andwastransposedintotheSpanishlegalsystembywayofRoyalDecree81/2014ofFebruary7,201472.
– EuropeanReferenceNetworks.WithinthecontextoftheCross-borderHealth
Care Directive and with the unanimous support of the Member States, theEuropean Commission approved the legal basis for the implementation ofreference networks aimed at further enhancing access and knowledge formanagingrareorhighlycomplexdiseases,includingawide-ranginglistofcare

36
quality and patient safety-related criteria with which the highly-specializedmedical services centers in the European Unionmust comply in order to beapprovedasmembersofthenetwork73,74.
– The Council’s conclusions on care quality and patient safety: In 2014, theCouncil of the European Union approved some conclusions on this subject,underlining the importance and priority of the patient safety-related policiesandsettingoutthecommitmentofthecountriesastocontinuingworkingonsaid policies, entrusting to the European Commission the organization of apermanent platform for providing sustainability for the joint action and thesharingofbestpracticesamongtheMemberStates75.

37
INTERNATIONALSTRATEGICLINESOFACTIONINPATIENTSAFETY
The international strategies forpatient safetyare focusedmainlyon twomajorareas: the cultural change of the professionals and the implementation of safepractices.
� Patientsafetyculture,humanfactorandtraining
Ascertaining an organization’s patient safety culture is the first step toward itsfurtherenhancement.Thesafetyculture-relatedresearchhasbeenfocusedmainlyonevaluating the safety climate (the safety-related attitudes and perceptions of theprofessionals) and their association with different clinical outcomes, as well as thesatisfactionofbothprofessionalsandpatients76.
Although no clear-cut evidence currently exists concerning the relationshipbetween the safety cultureand thepreventionof adverseevents, some studies findthere to be a correlation between a positive safety climate and a betterimplementationofsafepracticesandbetterclinicaloutcomes77,78.
Theorganizationscommittedtothesafetyculturefocustheireffortsonfourkeyaspects: cultivating the safety culture at all levels; evaluating and promoting a goodsafety-related climate; increasing training in patient safety and the so-called humanfactorsornon-technicalfactorsoftheprofessionals;anddevelopingsafetyelementsattheclinicalunitlevel79.
The importance of the human factor in further enhancing patient safety hasgrown over the past few years, there currently being several experts who arerecommending training the health care professionals in this aspect and favoring theincorporation of the human factor-related principles into the organization by takinginto account physical aspects (design, equipment, etc.), cognitive aspects (theprofessional’s status and situation, communicating skills, teamwork (“from theworkteamtoteamwork”)andorganizationalaspects(theorganization’sculture)80,81,82,83.
Training in patient safety is the first step toward further enhancing the safetycultureand isan indispensableelement inorder for thehealthcareprofessionals tounderstandwhythepatientsafety-relatedinitiativesarenecessaryandhowtheycanput them intopractice. The importanceof training theprofessional is patient safetyhasbeenpointedoutbothbytheWorldHealthOrganization,whichhasdevelopedaspecific curriculum guide84 and by the European Commission, which has recentlypublishedsomerecommendationsinthisregard71.

38
� Safepractices
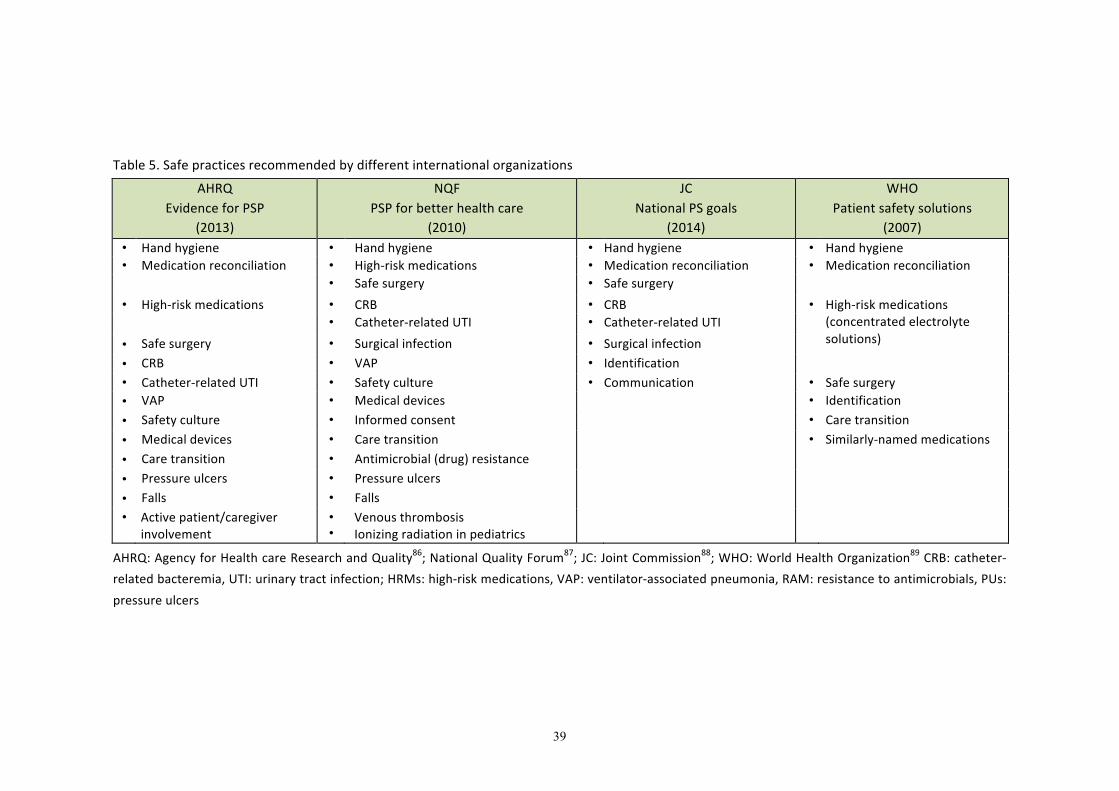
Safe practices are those interventions aimed at preventing or mitigating thenecessaryharmassociated tohealth care and further enhancingpatient safety 42,85.Table 5 provides a brief descriptionof the safe practices recommendedbydifferentinternationalagenciesandorganizationsbasedonthefrequencyofthemostcommonadverse events and the evidence for their control. The practiceswhichmost of theorganizations recommendare thosewhichhave todowith thepreventionofhealthcare-associated infections (especially hand hygiene), safe use of medication, safesurgeryandcare.
39
Table5.Safepracticesrecommendedbydifferentinternationalorganizations
AHRQEvidenceforPSP
(2013)
NQFPSPforbetterhealthcare
(2010)
JCNationalPSgoals
(2014)
WHOPatientsafetysolutions
(2007)• Handhygiene • Handhygiene • Handhygiene • Handhygiene• Medicationreconciliation • High-riskmedications • Medicationreconciliation • Medicationreconciliation
• Safesurgery • Safesurgery • High-riskmedications • CRB • CRB • High-riskmedications
(concentratedelectrolytesolutions)
• Catheter-relatedUTI • Catheter-relatedUTI • Safesurgery • Surgicalinfection • Surgicalinfection • CRB • VAP • Identification • Catheter-relatedUTI • Safetyculture • Communication • Safesurgery• VAP • Medicaldevices • Identification• Safetyculture • Informedconsent • Caretransition• Medicaldevices • Caretransition • Similarly-namedmedications• Caretransition • Antimicrobial(drug)resistance • Pressureulcers • Pressureulcers • Falls • Falls • Activepatient/caregiver
involvement• •
VenousthrombosisIonizingradiationinpediatrics
AHRQ:AgencyforHealthcareResearchandQuality86;NationalQualityForum87;JC:JointCommission88;WHO:WorldHealthOrganization89CRB:catheter-relatedbacteremia,UTI:urinarytractinfection;HRMs:high-riskmedications,VAP:ventilator-associatedpneumonia,RAM:resistancetoantimicrobials,PUs:pressureulcers

40
� Safemedicationuse
Specialinteresthasbeenfocusedontheimportanceofmedicationerrorsonthe
part of different international agencies and organizations, which have stressed the
needofimplementingsafepracticeswhichareeffectiveforreducingtheseerrors.
– In2007,theAmericanMedical Institutepublishedanumberofrecommendations
foralloftheplayersinvolvedinthemedicationusecircuit,afterhavingpointedout
thatatleast1.5millionpreventablemedication-relatedadverseeventsoccurevery
yearintheUnitedStates90.
– TheCouncilofEuropealsopublishedareportwhichincludedathoroughreviewof
thestudiesconductedonmedicationerrorsinEurope,aswellasrecommendations
fortheirpreventionaddressedtohealthcareauthorities, institutions,healthcare
professionalsandthepharmaceuticalindustry91.
– In 2013, the European Medicines Agency organized a meeting92, with the
participation of representatives of all of the agents involved in the notification,
evaluationandpreventionofmedicationerrorsforthepurposeoffacilitatingthe
implementation of new legal provision in Pharmacovigilance in the European
Union93.
Numerous safe practices have similarly been proposed for preventing
medication errors, especially in the hospital setting. These practices involve some
major differences with regard to cost, degree of complexity for implementation,
evidenceofeffectivenessand impactonpatientsafety,different initiativestherefore
having been carried out for selecting the essential practices on which top priority
shouldbeplacedfortheir implementationonthepartofhealthcareauthoritiesand
institutions:
– InMay 2007, theWorldHealthOrganization launched ninemeasureswhich
haveshownthemselvestobeeffectiveforthepurposeofpreventingadverse
events,theimplementationofwhichisconsideredatoppriority89.Severalof
these measures are practices related to the safe use of medications:
prevention of errors due to similar-sounding or similarly-spelled medication
names, control of concentrated electrolyte solutions and medication
reconciliationatcare-providingtransitions.
– In 2013, the Agency for Health care Research and Quality published anupdatedreportontheevidenceofsafepracticesknowntodate,considering
41
the evidence of their effectiveness and the cost and difficulties involved for
theirimplementation86.Fourofthe22practicesselectedhavetodowiththe
medicationarea (settingout a list of abbreviationswhichmustnotbeused,
incorporatingclinicalpharmacistsonthecare-providingteams, implementing
assistedelectronicprescriptionandreconcilingmedication).
– In 2010, theNational Quality Forum published an update of 34 top-prioritysafetypracticesforpreventingcare-providingerrors,groupedinto7functional
categories87, including several practices related to the prevention of
medicationerrors(incorporatingassistedelectronicprescription,verifyingthe
verbal prescriptions, limiting the use of abbreviations, medication
reconciliation, implementing standardized procedures with the high-risk
medications,maintainingriskmanagementprograms,etc.)
– The Joint Commission set out theNational Patient Safety Goals as of 2003whichareobjectivesaimedatpromotingthepreventionoferrorsindifferent
areas in theaccredited institutions88.Theseobjectivesare reviewedannually
andaremaintainedor replaceddependingonwhateverprioritiesmayarise.
The objectives related to the system for use of medications have revolved
around further enhancing the identification of the patients, standardizing
abbreviations, controlling the high-riskmedications, reducingmedications of
similar names being confusedwith one another, properly labeling all of the
medications which are prepared, avoiding free-flow infusion pumps,
reconcilingmedicationsandfosteringtheactiveinvolvementofthepatientsin
theirtreatment.
� Healthcare-associatedinfections
In hospitals, the prevalence of health care-associated infections falls within the
5.7%-19.1%range,withanoverallprevalenceof10.1%.Inthedevelopedcountries,
health care-associated infections affect 5%-15% of all hospitalized patients94. In
Europe,thisprevalencefallswithinthe3.5%-14.8%range,thusmeaningthataround4
millionpeopleperyearareaffectedbyhealthcare-associated infectionsduringtheir
hospital stay, causing 37,000 deaths, 16 million extra days of hospitalization and
approximatelyseventrillioneurosindirectcosts67,95.

42
Healthcare-associatedinfectionsareoftendifficulttotreatduetotheinvolvement
of microorganismmultiresistant to antibiotics, but the evidence shows that around
50%canbepreventedbywayofsafepractices.Therefore,preventingandcombatting
theseinfectionsandresistancetoantibioticsisakeypriorityfordifferentinternational
organizationssuchastheWorldHealthOrganization,theEuropeanCenterforDisease
PreventionandControlandtheEuropeanCommission24.
– TheWorldHealthOrganizationtookuponitselftospearheadthepreventionofhealthcare-associatedinfectionsbywayofitsfirstchallenge“Cleancareissafe
care”44 one of the main components of which was its worldwide campaign:
«Save Lives: Clean YourHands”, aimed at further enhancing the hand hygiene
practices of health care personnel. A person’s hands are the main means of
transmission of the microorganisms causing health care-associated infections,
handhygienecomprisingthesimplest,cheapest,mosthighlyeffectivemeansof
reducingtheseinfections.However,accordingtovariousstudies,thismeasureis
notbeingfollowedbymorethan40%96.Theimplementationofthemultimodal
strategy for further enhancing hand hygiene promoted by the World Health
Organizationisapparentlyimprovingcompliancewithachievingahigherdegree
of hygiene and reducing the rate of multiresistant microorganisms such as
Methicillin-ResistantStaphylococcusAureus(MRSA)andClostridiumdifficile97,98.
The objective of World Hand Hygiene Day, held every May 5th, is to
heightenawareness about theneedof health careprofessionals implementing
the hand hygiene practice at the fitting point in time and in the appropriate
manner (by following the five moments recommended by the World Health
Organization) for the purpose of contributing to reducing the spread of
potentiallylethalinfectionsatmedicalservicescenters.
– TheEuropeanCommissionhasalsobecomeactivelyinvolvedincombattingHAIs
bymeansofdifferent actions and strategies, someof themostoutstandingof
whichare:
¡ The Council of the European Union Recommendation7 on patient safety,
particularlypreventingand combattinghealth care-associated infections. In
thisRecommendation,theMemberStatesareaskedtoadoptandimplement
a strategy for preventing and combattinghealth care-associated infections,
mention being made of a “Plan for action against the growing threat of
bacterialresistances”,whichincludestwelveactionsthatmustbecarriedout

43
by the European Union countries, one of which is the action for
“strengtheninginfectionpreventionandcontrolinhealthcaresettings”.
The latest report published by the European Commission on the
implementationoftheaforesaidrecommendations67invitestheMemberStates
to focus their efforts on monitoring the infections, especially surgical site
infectionandthosecausedonintensivecareunitsandatsocialservicesmedical
services centers. Mention is also made therein as to the need of preparing
national diagnostic guides, setting out actions for continued training of health
care professionals, implementing the definitions of health care-associated
infections and the further enhancement of the diagnostic capabilities of
laboratories.Asapriority,itisrecommendedtoassure:
– A sufficient number of trained professionals devoted to the control of
healthcare-associatedinfectionsatthemedicalservicescenters.
– Capacity for putting precautions into place for isolating hospitalizedpatientsinfectedwhoareshowingrelevantclinicalsignsandsymptoms.
– Standardized surveillance of the consumption of alcohol-based products
forhandhygiene.
TheCommissionhasfundedseveralprojectsonaEuropeanscalewithinthe
frameworksofthe2003-2008and2008-2013HealthPrograms,theobjectivesof
whicharedetailedinTable6.

44
Table6.EuropeanUnionandECDCinitiativesforcombattingHAIsandAMR
Project Objectives
HELICS To set up a standardized health care-associated infection surveillance system and databases (surgical site infection and infection on intensive care units) at the European Union level for pinpointing areas for improvement.
IPSE Reducing the burden of health care-associated infections and the challenge of resistance to antibiotics by developing recommendations, training tools and control indicators.
BURDEN Generating adequate knowledge and awareness among policymakers and society as a whole concerning the social dimension of health care-associated infections and resistance to antibiotics by providing valid, comparable information on the load of morbidity and the costs attributable to these problems in the European Union.
IMPLEMENT Identifying strategies at the individual hospital and country level for reducing health care-associated infections and resistance to antibiotics.
PROHIBIT Analyzing the guidelines and practices currently in effect for the prevention of health care-associated infections, the facilitating factors and barriers for full compliance with the best practices and the effectiveness of the interventions of known effectiveness.
HELICS:HospitalinEuropeLinkforInfectionControlthroughSurveillance99.
IPSE:ImprovingPatientSafetyinEurope100.
BURDEN:BurdenofResistanceandDiseaseinEuropeanNations101
IMPLEMENT:ImplementingStrategicBundlesforInfectionPrevention&Management102
PROHIBIT:PreventionofHospitalInfectionsbyInterventionandTraining103
HAIs-.Healthcare-associatedinfections
AMR:Antimicrobialresistance
ECDC:EuropeanCenterforDiseasePreventionandControl104
In2010,atrans-AtlanticcollaborationwascarriedoutbetweentheEuropean
UnionandtheUnitedStatesaimedatcombattingresistancetoantibiotics.105.The
recommendations resulting from this collaboration have to dowith the need of
creating indicators of structure and process for the use of antibiotics, for use in
bothhumans and in veterinarymedicine, to develop toolswhichwill aid toward
changinghabitsintheiruse,improvinginformationonthebasisofepidemiological
studies, harmonizing the criteria for the interpretation of resistance among the
European and American laboratories, reaching a consensus as to the prevention
tools for thehospital controlprograms,preparinga joint inoculation strategy for
45
preventing health care-associated infections, stimulating the creation of new
antimicrobialdrugsand,ingeneral,sharingtheeffortsandknow-howinthisarea.
– TheEuropeanCenterforDiseasePreventionandControl:ECDCwhichcoordinatesEuropean surveillanceof surgical infections, infectionson
intensive care units and the resistance to antimicrobial drugs,
developed a protocol in 2009 for studying the prevalence of health
care-associated infectionsand theuseofantimicrobialdrugs inacute
hospitalswhichwasputintopracticeintheMemberStatesthroughout
the 2011-2012 period104. The ECDC additionally supports a European
network for health care-associated infection surveillance at the
extendedstayhospitals106.ElEuropeanCenter forDiseasePrevention
andControl sponsors thepreparationof guidelinesand indicators for
the prevention of health care-associated infections and develops
guidelines for preventing and combatting infections by Clostridiumdifficileandbycarbapenemase-producingenterobacteriaceae.
� Safesurgery
Thestudiesconductedforascertainingtheadverseeventsassociatedtosurgery
reveal that 25% of the patients having undergone surgery have experienced
complicationsfollowingsurgery(3%-16%beingmajorcomplications).Inindustrialized
countries, 3%-22% of the adverse events related to surgery at hospitals lead to
disability,involvingdeathratesof0.4%-0.8%108.
Takingthisdataintoaccountandtheactthatatleast50%ofthesurgery-related
adverse events could be prevented by way of safe practices, the World Health
Organization launched a second challenge in 2008: Safe Surgery Saves Lives45Thismultimodal program suggests working in four areas: preventing surgical wound
infection; preventing the wrong site/wrong patient/wrong procedure; further
enhancing the safety of surgical equipment; and safety in handling anesthesia The
results of an international pilot study conducted in 10 countries demonstrated the
effectiveness of the measures recommended109 especially the use of the surgical
checklist.Thislisthasalsoshownareductioninerrorswhentheyareusedinsimulated
crisissituations110.
Despitetheeffortsmade,theimplementationofthesurgicalchecklisthasbeen
incomplete at the international level. The main barrier detected have been:
46
consideringittobeimposedbytheadministration;changeintheorganizationoftimes
onsurgicallistsandpossibledelays;notbeingfullyconvincedofitsusefulness;feeling
of duplicating tasks; lack of adaptation of the list to the center’s circumstance;
embarrassmentandfeelingofridicule.Atdifferenthospitals,greater importancehas
beenplacedontherecordkeepingaspectthanoncompliance,asaresultofwhichthe
checklisthasbeencompletedhowevercarriedoutinadequately111,112whichhasledto
someexpertsaccentuatingtheneedofcomingupwithstrategiesforthecorrectuseof
thesurgicalchecklist113.
Asregardsanesthesia,theEuropeanCouncilofAnesthesiology,incollaboration
withtheEuropeanSociety forAnesthesiology,promotedtheHelsinkiDeclarationonPatient Safety in Anesthesiology, approved in conjunction with the World Health
Organization, the International Federation of Anesthesiology Societies and the
EuropeanPatients’FederationattheEuroanaesthesiameetingheldinHelsinkiinJune
2010. This declaration includes elementary safety –related recommendations which
werealreadybeingimplementedinpart114,115,116.
� Safecare
Nursing care encompasses a number of procedures and techniques requiring
specialprecautionbeingtaken,duenotonlytotheintrinsicrisk involvedinsomefor
patient safety but also due to the volume and scope thereof at all care-providing
levels.Itisthereforenecessaryforstrategiestobesetoutforpreventingcare-related
adverseeventswithasystemforrankingbyprioritiesaccordingtotheirfrequencyof
occurrence,theseverityoftheirconsequencesandtheirpreventability117.
Historically, nursing has taken care related to the prevention of some adverse
eventsverycloselyintoaccount,suchasfallsorpressureulcers,havingreachedquite
a generalized consensus as to their prevention and the use of and heeding risk
assessmentscales118.
� Patientidentificationsafety
Approximately13%oftheerrorsreportedinthesurgicalfieldand67%ofthose
related to the transfusion of blood components have to do with erroneous patient
identification119.Thatiswhysettingoutmeasureforguaranteeingpatientidentification
safety, their samplesandall of their information, isoneof the top-prioritypractices
recommendedbydifferentinternationalorganizations(Table5).

47
For proper patient identification, it is recommended: to use at least two
identifiers (never bed or room number), to promote automated identification, to
alwayschecktoverifythepatient’sidentitypriortoanyprocedureandtogetpatients
andcaregiversactivelyinvolved120.
� ReportingandLearningSystems
The reportingand learning systemsmake itpossible to report thecare-providing
relatedincidentsandtoobtainusefulinformationofthesequenceofeventshavingled
up to the incident in question having occurred, affording the opportunities to learn
lessonsforpreventingthemfromreoccurring.
The main limitation of the reporting and learning systems is infra-notification,
someofthecausesofwhich includetheorganization’s lackofsafetycultureandthe
professionals’ fearof findingthemselves involved in lawsuitsduetoa lackofspecific
lawtoprotectthem.Thisfearhasabearingonthequalityofthedataobtainedfrom
these systems and on the best use beingmade of the information recorded. These
systemshavebeen found tousuallyachieveagreaterdealofactive involvementon
thepartoftheprofessionalswhentheyarevoluntaryandanonymous.
The reporting and learning systems are explicitly recommended by the World
HealthOrganization121andbytheCounciloftheEuropeanUnion7.TheWorldHealth
Organization is currently carrying out a project in collaboration with the European
CommissionandtheMemberStatesforthepurposeofsettingoutamodelofminimal
information for reporting on patient safetywhichwillmake it possible to set out a
commontaxonomyandcomparisonsamongcountries122.
In the report prepared by the European Commission on implementation of the
recommendations put forth by the Council of the EuropeanUnion, it is pointed out
that the reporting and learning system is a useful learning tool which favors the
dissemination of the patient safety culture, provided that the professionals are
properly informed in a timely fashion concerning the problems identified and the
measurestakenforimprovement67.
Tofavorthedevelopmentofincidentreportingsystems,theEuropeanCommission
has recently published a report on findings and recommendations of the European
Unionpatientsafetyincidentreportingsystems71.
48
� Patientandcaregiverparticipation
Thechangeintheprofileofthepatientsandthedevelopmentoftheirentitlement
toautonomyanddecision-making regarding theownhealthentailsbothachallenge
andanopportunity forthehealthsystem.Theparticipationofthepatientshasbeen
moreappreciable in thecaseofchronicdisordersyethasbeen toa lesserdegree in
aspects concerning patient safety. Nevertheless, some experts point out that the
patientscanplayanoutstandingrole inthepreventionof incidents123,thisbeingthe
reason why different international organizations have developed strategies for
promotingtheirparticipationforthesafety.
Theneedofgettingpatientsactivelyinvolvedandempoweredfortheirsafetyhas
beenpointedoutbydifferentinternationalorganizations:
¡ TheWorldHealthOrganizationhasspearheadedpatientparticipationfortheir
ownsafetywiththeprogram“PatientsforPatientSafety”48,startedin2005..
Thisprogramaimstoincorporatethepatient,familyandcommunityvoiceinto
alllevelsofhealthcarethroughengagementandempowerment
TheWorldHealthOrganizationrecommendstocreatemechanismsforgiving
patients theopportunity to takepart in thehealth carepolicies and in their
health process at three levels:macro (by fostering their participation in the
patient safety policies), meso (by means of participation on professional
committees, taking training, etc.) and micro (being provided with clear
informationandsharingdecisionsregardingtheirhealthprocess).124.
¡ The recommendations of the Council of the European Union concerning
patientsafetyurgedtheMemberStates tocarryoutactions for thepurpose
of:
– Gettingthepatients’organizationsactivelyinvolvedinthedevelopmentof
safety-relatedpoliciesandprogramsatalllevels.
– Informing patients on safety standards and measures implemented for
reducingorpreventingadverseeventsandfacilitatingthedecision-making
process.
– Getting complaint procedures and compensation systems under way, as
wellasthetermsandconditionsfortheirimplementation.
However, the latest EuropeanCommission report on the implementationof the
aforementioned recommendations reveals that no progress has been made in this
49
field, and that the term “empowerment” still as yet remains unclear for many
countries67. Different projects funded by the European Commission are aimed at
promoting the sharing of experiences and improving the knowledge on this subject
(PaSQ65,EMPATHIE125,Value+126).
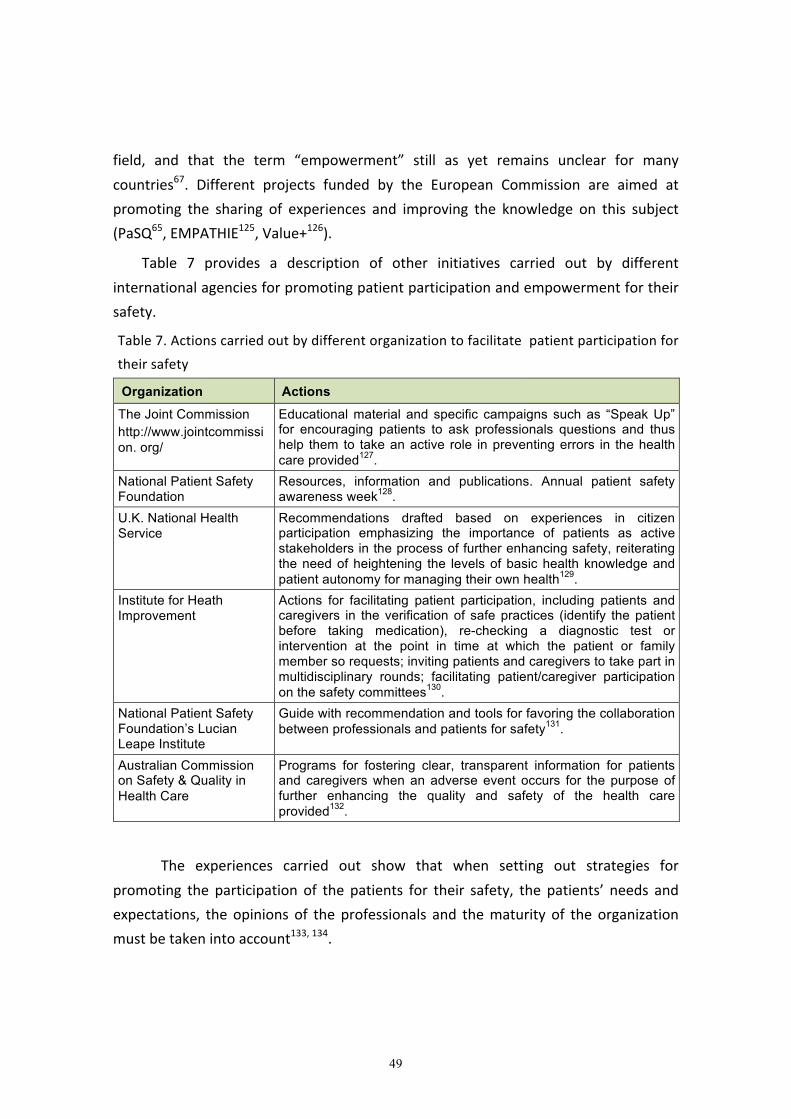
Table 7 provides a description of other initiatives carried out by different
internationalagenciesforpromotingpatientparticipationandempowermentfortheir
safety.
Table7.Actionscarriedoutbydifferentorganizationtofacilitatepatientparticipationfor
theirsafety
Organization Actions
The Joint Commission http://www.jointcommission. org/
Educational material and specific campaigns such as “Speak Up” for encouraging patients to ask professionals questions and thus help them to take an active role in preventing errors in the health care provided127.
National Patient Safety Foundation
Resources, information and publications. Annual patient safety awareness week128.
U.K. National Health Service
Recommendations drafted based on experiences in citizen participation emphasizing the importance of patients as active stakeholders in the process of further enhancing safety, reiterating the need of heightening the levels of basic health knowledge and patient autonomy for managing their own health129.
Institute for Heath Improvement
Actions for facilitating patient participation, including patients and caregivers in the verification of safe practices (identify the patient before taking medication), re-checking a diagnostic test or intervention at the point in time at which the patient or family member so requests; inviting patients and caregivers to take part in multidisciplinary rounds; facilitating patient/caregiver participation on the safety committees130.
National Patient Safety Foundation’s Lucian Leape Institute
Guide with recommendation and tools for favoring the collaboration between professionals and patients for safety131.
Australian Commission on Safety & Quality in Health Care
Programs for fostering clear, transparent information for patients and caregivers when an adverse event occurs for the purpose of further enhancing the quality and safety of the health care provided132.
The experiences carried out show that when setting out strategies for
promoting the participation of the patients for their safety, the patients’ needs and
expectations, the opinions of the professionals and thematurity of the organization
mustbetakenintoaccount133,134.

50
iii.InterventionscarriedoutintheNationalHealthSystem
To make reference to the current patient safety situation in Spain, mention
must necessarily be made of the actions promoted by theMSSSI which have been
beingcarriedoutasof2005within the frameworkof thepatientsafetystrategy3, in
additiontothosecarriedoutbytheHealthRegions,thehealthcarecenters,academic
institutionsandotherorganizationswhichhaveshownaninterestinthissubject2,135.
ThestrategylinesincludedintheNationalPatientSafetyStrategyforthe2005-
2013 period were in keeping with the top-priority objectives thereof: fostering the
patientsafetycultureamongtheprofessionalsandthepatientsatanylevelatwhich
healthcareisprovided,trainingtheprofessional inpatientsafety, implementingsafe
practices, research into adverse events and their conditioning factors and getting
patientsandcitizensactivelyinvolved.
Deployingtheaforementionedstrategyentailedbothapoliticalandeconomic
commitment with all of the regional services, although this strategy has been
implementedtodifferingdegreesfromoneAutonomousCommunitytoanother,and
the funding allocated has ceased to exist as a result of the current economic
restrictions.
A description is provided in following of the actions carried out within the
frameworkofthePatientSafetyStrategyforthe2005-2013period.
51
PATIENT SAFETY STRATEGY LINES CARRIED OUT IN THE NATIONALHEALTHSYSTEM
� Patientsafetyculture,humanfactorandtraining
ForthepurposeofmeetingthefirstobjectiveofSpain’sNationalHealthSystem
QualityPlanStrategyNumber8(topromoteandfurtherthepatientsafetycultureand
knowledgeamongtheprofessionalsandpatientsatany levelatwhichhealthcare is
provided)theMSSSIhasbeenholdingforums,workshops,meetingsandconferences
at the national and international level, has been disseminating news and
recommendationsbywayof itsWebsiteandhasbeendevelopingtrainingcourses in
patientsafetyforprofessionals.
¡ Information and dissemination. The different Health Regions have echoedthese initiatives and have, in turn, carried out seminars, forums,meetings
and have disseminated aspects for furthering and implementing the safety
culture.
The scientific societies have also been holding forums where the
patient safety-related aspects have played a leading role and have also
promoted the implementation of safe practices among the professionals.
Specialmentionmayalsobemadeinthisregardoftheworkwhichisbeing
done by the scientific societies, coordinated by the MSSSI, for identifying
those aspects of the care providedwhich do not provide any added value
andwhichmayentailariskorharmforthepatient136,137,138.
¡ Perception-relatedstudies.TheMSSSIhaspromotedstudiesforthepurpose
ofgettingtoknowthepatientsafetycultureindifferenthealthcaresettings:
– In the field of hospital care, the Hospital Survey for Patient Safetydeveloped by the Agency for Health care Research and Quality wasadaptedintotheSpanishlanguageandvalidated,havingbeenusedona
randomsampleof24oftheacutehospitalsintheNHS.Themainfindings
of this study showed that the professionals considered safety to be
acceptable and acknowledged weak points with regard to “Staffing”,
“Teamwork among units and departments”, “Perception of safety” and
“Hospital Administration support in patient safety”. This study
additionallystressesthattheworkingpaceatmanyhospitalsmayhavea
bearingonpatientsafety139.

52
– In primary care, the Medical Office Survey on Patient Safety Culture(MOSPS)developedby theAgency forHealth careResearchandQualitywasadaptedandvalidated,thenhavingbeengivennationwideto4,344
professionals from215healthcenters in15HealthRegions.Thenursing
professionals showed higher levels of patient safety culture than the
physicians, thephysicianshavingshown, in turn,ahigher level thanthe
alloftheotherprofessionalcategories.Theadministrativestaffmembers
are,according to thesurvey findings, theprofessional category showing
the leastdegreeofpatient safety culture. Similarly, theprofessionals in
positions of responsibility or leadership positions showed a greater
degree of patient safety culture compared to those not holding
leadership positions, those over 40 years of age compared to those
youngerandtheprofessionalswithsmallerquotas(1,000ormorehealth
systemcards)comparedtothosewhohadagreaternumber. Generally
speaking, the perception of patient safety among the primary care
professionalsispositiveonanoverallbasisaccordingtothisstudy140.
¡ Trainingprofessionals
After the efforts made over these past years in training health care
professionalsinpatientsafety,thefollowingassessmentcanbemadeofthe
currentsituation:
– Itisdifficulttoassesstheimpactofthetraining,notonlyatthe
individuallevelbutalsotheinstitutionalrepercussionthereof.In
any case, according to thedata available from theNHS2, there
are a major number of professionals possessing training in
patient safetywho are playing amajor role as instructors and
promotorsofthechangeintheirworksettings.
– Asnowballeffect isbeingcaused,asaresultofboththeboost
provided by the MSSSI and the recommendations from the
WorldHealthOrganizationandfromtheCounciloftheEuropean
Unionandthe interesttakenonthepartoftheHealthRegions
andsomeuniversitiesand institutionsofaprivatenature,who
have carried out training initiatives in patient safety at certain
times.

53
– Although attempts have been made to incorporate patient
safety as transversal training, the truth of thematter is that it
still has not been formally integrated into either the
undergraduate degree training or the specialized training in
healthsciences.
TheMSSSI patient safety web141 is the showcase for the production of
training resources, reports and experiences of different types which have
beenpromotedandcarriedoutoverthesepastfewyears.Onepointworthy
of specialmention in this regard is the base of projects which have been
beingprogressivelycarriedoutasafinalstudyofthesuccessiveeditionsof
the master’s program and of the risk management course. Those of the
latterareavailablefreelyontheaforementionedweb.
It is necessary for themanagers of each institution to set some overall
patient safety-related objectives and for them to support the initiatives of
theclinicalunitsforthesametobeachieved,byfacilitatingtheknowledge
andtoolsappropriateforcarryingouttheseinitiatives.
Itwouldadditionallybedesirable forpatient safety to comprisepartof
the course curricula of the Schools of Health Science and that all of the
professionalsnewlyincorporatedintotheNHSweretoundergobasicentry
leveltrainingontheconceptsandpracticeofcare-providingsafety.
� Safepractices
¡ Safemedicationuse
In themulticenter studieswhichhavebeencarriedout inSpainasof
2005 for the purpose of making an overall analysis of the frequency and
typesofadverseevents indifferenthealthcaresettings, ithasbeen found
thattheadverseeventsrelatedtotheuseofmedicationscomprisea large
percentageofthetotalnumberofadverseeventswhichoccurintheprocess
ofprovidinghealthcare(Table8).

54
Table8.Frequencyoftheadverseeventsduetomedicationsinthemulticenterstudies
conductsatthenationallevel
Study
TotalAEs
(%patients)
Mostfrequent
AEs
AEsduetomedications
Percentageof
totalnumber
Preventable
(%)
ENEAS15 9.3%
Medication (37.4%). HAIs (25.3%) Procedures (25%).
37.4 34.8
APEAS26 10.11‰
Medication (47.8%) Baseline disorder evolving for the worse (19.9%) Procedures (10.6%).
47.8 59.1
EARCAS27
Qualitative study Care. Medication HAIs
_ _
SYREC28 33.1%
Care (26%) HAIs (24%) Medication (12%)
11.6% 58.9%
EVADUR29 7.2%
Care-providing process (46.2%). Medication (24.1%) Procedures (11.7%).
24.1% _
-ENEAS:NationalStudyofAdverseEventsRelatedtoHospitalization
-APEAS:StudyofAdverseEventsinPrimaryCare
-EARCAS:AdverseEventsinSocialservicesmedicalservicescentersandLivingfacilities
-SYREC:SafetyandRiskintheCriticalPatient
-EVADUR:AdverseEventsinEmergencyCare
-AE:AdverseEvent
-HAIs:Healthcare-associatedInfections
Other studies also conducted in Spain have specifically characterized and
analyzed thepreventableadverseeventsdue tomedications indifferenthealthcare
settings and have estimated the frequency of medication errors in the different
processesofthesystemfortheuseofmedications.Table9detailsthemostrelevant
aspects of the findings of these studies, which show the major degree to which
medicationerrorshaveanimpactonthehealthcareprovided.
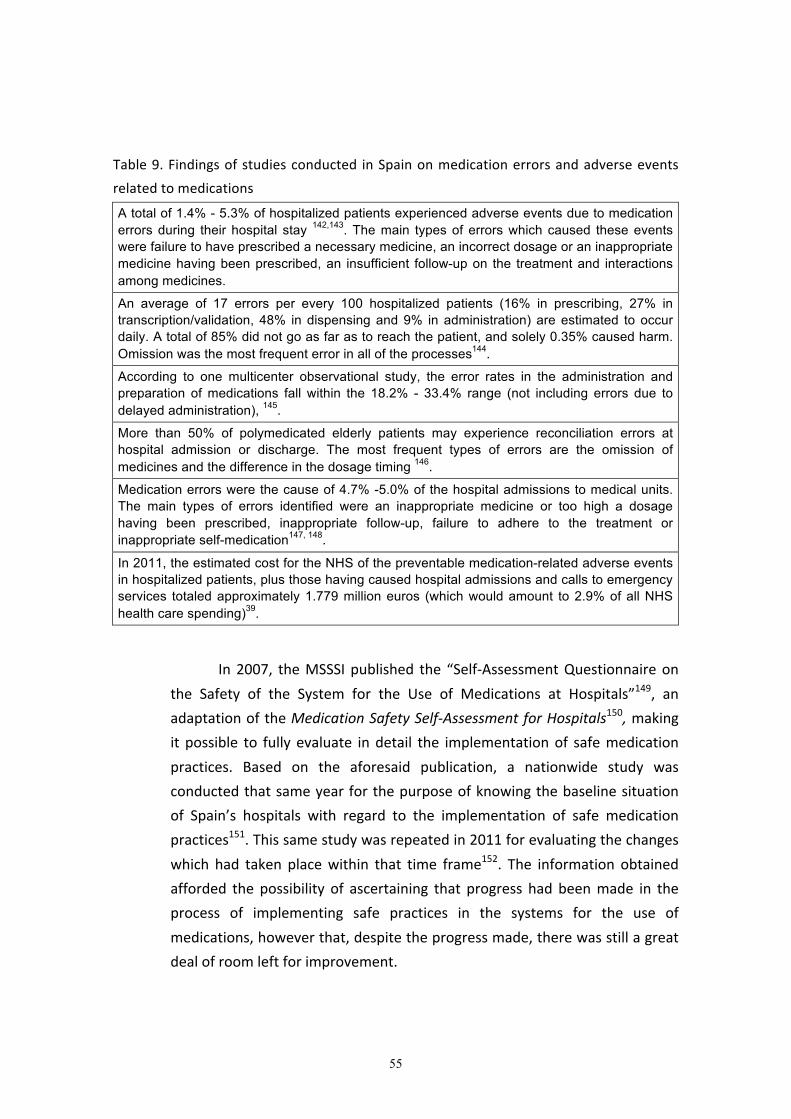
55
Table9.Findingsofstudiesconducted inSpainonmedicationerrorsandadverseevents
relatedtomedications
A total of 1.4% - 5.3% of hospitalized patients experienced adverse events due to medication errors during their hospital stay 142,143. The main types of errors which caused these events were failure to have prescribed a necessary medicine, an incorrect dosage or an inappropriate medicine having been prescribed, an insufficient follow-up on the treatment and interactions among medicines.
An average of 17 errors per every 100 hospitalized patients (16% in prescribing, 27% in transcription/validation, 48% in dispensing and 9% in administration) are estimated to occur daily. A total of 85% did not go as far as to reach the patient, and solely 0.35% caused harm. Omission was the most frequent error in all of the processes144.
According to one multicenter observational study, the error rates in the administration and preparation of medications fall within the 18.2% - 33.4% range (not including errors due to delayed administration), 145.
More than 50% of polymedicated elderly patients may experience reconciliation errors at hospital admission or discharge. The most frequent types of errors are the omission of medicines and the difference in the dosage timing 146.
Medication errors were the cause of 4.7% -5.0% of the hospital admissions to medical units. The main types of errors identified were an inappropriate medicine or too high a dosage having been prescribed, inappropriate follow-up, failure to adhere to the treatment or inappropriate self-medication147, 148.
In 2011, the estimated cost for the NHS of the preventable medication-related adverse events in hospitalized patients, plus those having caused hospital admissions and calls to emergency services totaled approximately 1.779 million euros (which would amount to 2.9% of all NHS health care spending)39.
In2007, theMSSSIpublished the “Self-AssessmentQuestionnaireon
the Safety of the System for the Use of Medications at Hospitals”149, an
adaptationoftheMedicationSafetySelf-AssessmentforHospitals150,making
it possible to fully evaluate indetail the implementationof safemedication
practices. Based on the aforesaid publication, a nationwide study was
conductedthatsameyearforthepurposeofknowingthebaselinesituation
of Spain’s hospitals with regard to the implementation of safe medication
practices151.Thissamestudywasrepeatedin2011forevaluatingthechanges
which had taken placewithin that time frame152. The information obtained
afforded the possibility of ascertaining that progress had beenmade in the
process of implementing safe practices in the systems for the use of
medications,howeverthat,despitetheprogressmade,therewasstillagreat
dealofroomleftforimprovement.

56
Table 10 shows the findings for 2007 and 2011 for the evaluation
itemsincludedonthequestionnairewhicharebest inkeepingwiththetop-
prioritysafepracticesrecommendedbydifferentinternationalorganizations.
The findings are stated in the form of percentages of themaximum figure
possible for each item to be assessed, which reflects their degree of
implementation at the participating hospitals. It was objectively found that
some practices had been implemented to quite a great degree in the NHS
(avoiding verbal prescriptions and dispensing the medicines in individual
doses),andothershadundergonenoticeableincreasesoverthecourseofthe
time frame in question (the incorporationof the e-prescriptionwith clinical
decision-makingsupport,thesettingupofsystemsforreportingandlearning
from medication errors). In other cases, changes of a lesser degree were
observed (avoiding theuseof free-flowpumpsandpreventingerrors in the
connectionofcatheters)orthatthepracticeshadbeenimplementedtoonly
averysmalldegree(validationofalloftheprescriptionsbyapharmacistand
theintegrationthereofintotheclinicalteams).
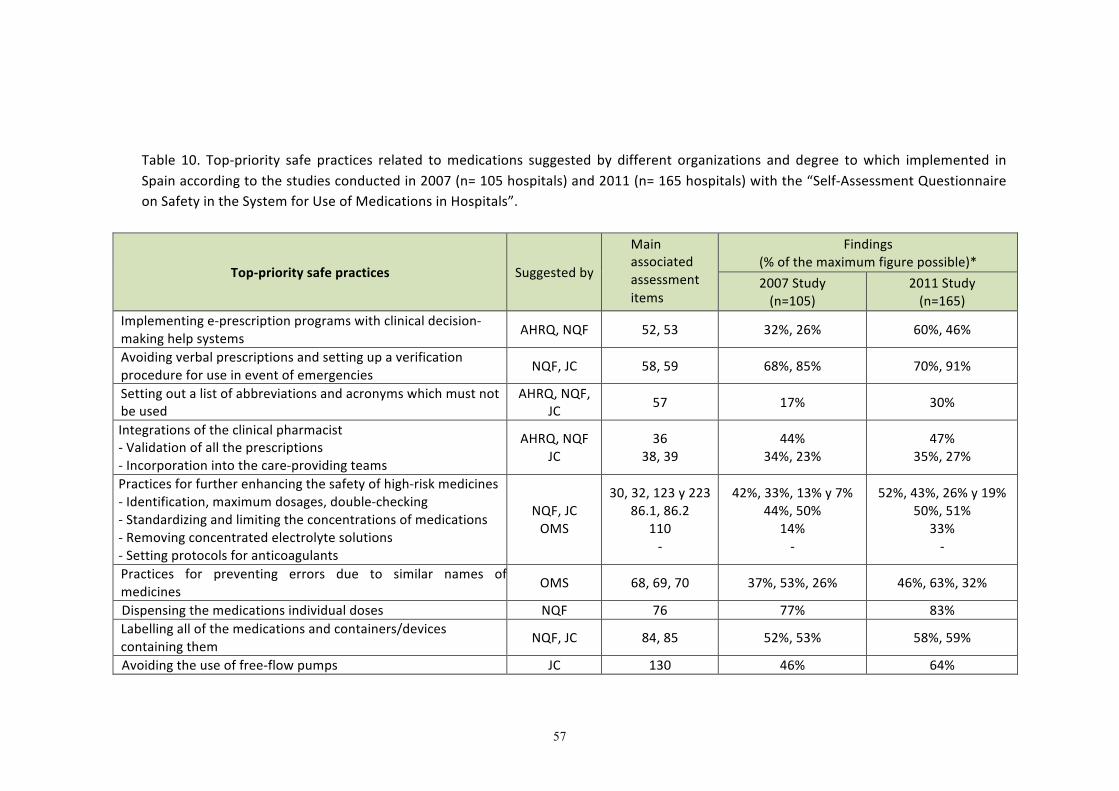
57
Table 10. Top-priority safe practices related tomedications suggested by different organizations and degree towhich implemented inSpainaccordingtothestudiesconductedin2007(n=105hospitals)and2011(n=165hospitals)withthe“Self-AssessmentQuestionnaireonSafetyintheSystemforUseofMedicationsinHospitals”.
Top-prioritysafepractices Suggestedby
Mainassociatedassessmentitems
Findings(%ofthemaximumfigurepossible)*2007Study(n=105)
2011Study(n=165)
Implementinge-prescriptionprogramswithclinicaldecision-makinghelpsystems AHRQ,NQF 52,53 32%,26% 60%,46%
Avoidingverbalprescriptionsandsettingupaverificationprocedureforuseineventofemergencies NQF,JC 58,59 68%,85% 70%,91%
Settingoutalistofabbreviationsandacronymswhichmustnotbeused
AHRQ,NQF,JC 57 17% 30%
Integrationsoftheclinicalpharmacist-Validationofalltheprescriptions-Incorporationintothecare-providingteams
AHRQ,NQFJC
3638,39
44%34%,23%
47%35%,27%
Practicesforfurtherenhancingthesafetyofhigh-riskmedicines-Identification,maximumdosages,double-checking-Standardizingandlimitingtheconcentrationsofmedications-Removingconcentratedelectrolytesolutions-Settingprotocolsforanticoagulants
NQF,JCOMS
30,32,123y22386.1,86.2
110-
42%,33%,13%y7%44%,50%
14%-
52%,43%,26%y19%50%,51%
33%-
Practices for preventing errors due to similar names ofmedicines OMS 68,69,70 37%,53%,26% 46%,63%,32%
Dispensingthemedicationsindividualdoses NQF 76 77% 83%Labellingallofthemedicationsandcontainers/devicescontainingthem NQF,JC 84,85 52%,53% 58%,59%
Avoidingtheuseoffree-flowpumps JC 130 46% 64%
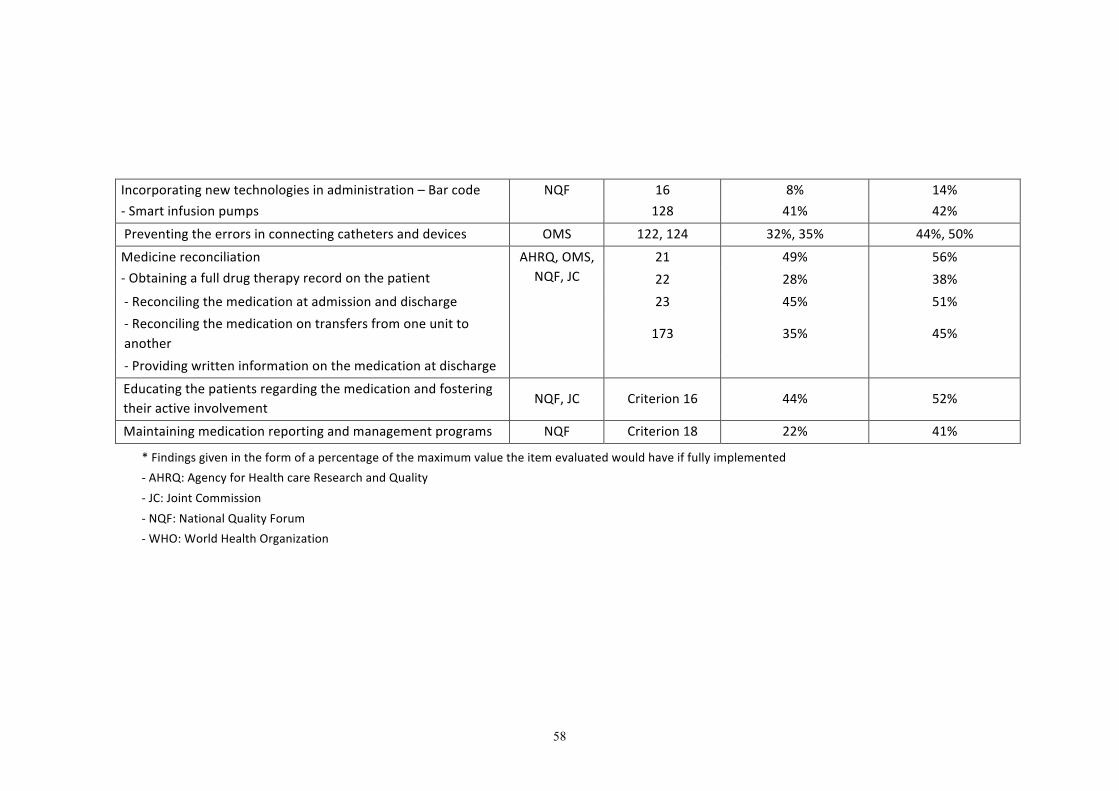
58
Incorporatingnewtechnologiesinadministration–Barcode-Smartinfusionpumps
NQF 16128
8%41%
14%42%
Preventingtheerrorsinconnectingcathetersanddevices OMS 122,124 32%,35% 44%,50%
Medicinereconciliation-Obtainingafulldrugtherapyrecordonthepatient
AHRQ,OMS,NQF,JC
21 49% 56%22 28% 38%
-Reconcilingthemedicationatadmissionanddischarge 23 45% 51%-Reconcilingthemedicationontransfersfromoneunittoanother
173 35% 45%
-Providingwritteninformationonthemedicationatdischarge
Educatingthepatientsregardingthemedicationandfosteringtheiractiveinvolvement
NQF,JC Criterion16 44% 52%
Maintainingmedicationreportingandmanagementprograms NQF Criterion18 22% 41%
*Findingsgivenintheformofapercentageofthemaximumvaluetheitemevaluatedwouldhaveiffullyimplemented-AHRQ:AgencyforHealthcareResearchandQuality-JC:JointCommission-NQF:NationalQualityForum-WHO:WorldHealthOrganization

59
¡ Healthcare-associatedinfections
Thestrategies for thepreventionandcontrolofhealthcare-associated infections
require agile, robust, sustainable systems of multi-faceted, standardized measures
promotingtheimplementationofsafepracticesbymultidisciplinaryteams.
Surveillancesystem
Epidemiological surveillance, understood as a continued, systematic process of
collection,analysis,interpretationanddisseminationofdataoninfectiousdiseasesfor
takingtheappropriateactions153
isthebasisoftheinfectioncontrolprograms.These
systemshaveevolvedfromglobalnosocomialinfectionsurveillanceintoasurveillance
focusing on processes related to the prevention and indicators of health care-
associateddiseases.Thecomparisonof these indicatorshasbeen foundtobeuseful
for setting out measures for the preventing and curtailing health care-associated
infections.
In Spain, the Health Regions are currently using different health care-associated
infection surveillance systems. The most widely-used are the Study of Nosocomial
Infections in Spain (EPINE)154
and the National Study of Surveillance of Nosocomial
InfectioninIntensiveCareMedicineServices(ENVIN-HELICS)155
.
– EPINE is a prevalence register making it possible to study the health care-
associated infections in all of the services throughout the hospital, including the
pediatric population. EPINEwas promoted by the Spanish Society for Preventive
Medicine,PublicHealthandHygiene in1990. In2012,EPINEwasadapted to the
European protocol by contributing data to the “Prevalence Point Surveillance
(PPS)”. In 2004, a total of 269 hospitals were participating, with some 55,700
patientshavingbeenstudied.Theprevalenceof infectionwas7.85%,thesebeing
percentagesprogressively on thedecline since2009 (8.59%).Adeclinehasbeen
foundtoexistinthepercentageofinfectionacquiredathospitaladmissionperse
andofthepatientswhowereadmittedwhoalreadyhadaaninfectionbeforehand,
the most outstanding of which was surgical infection. Respiratory infection has
become more prevalent in 2014 (21.4%, followed by surgical infection (20.9%),
urinary infection (20.1%) and catheter-associated bacteremia (15.3%). The data
also shows a discreet decline in the number of patients undergoing antibiotic
treatmentatthepointintimeofthestudy(45.4%)154
.

60
– ENVIN-HELICSisanincidenceregisterdevelopedin1994bytheSpanishSocietyfor
Intensive Care Medicine, Critical Care and Coronary Care Units (SEMICYUC),
affording the possibility of studying the device-related infections acquired on
intensivecareunits.ThisregisterhasbeencompatiblewithEuropeansurveillance
since 2007156
, although the data published in Spain includes the patients
hospitalizedfor longerthan24hours inApril-June,whilstattheEuropeanCenter
forDiseasePreventionandControl;allofthedatafortheyearisrecorded,butfor
staysoflongerthan48hours148
.
The control of the main infections in critical patients includes ventilator-
associated pneumonia, catheter-related urinary tract infection, primary
bacteremia, encompassing the bacteremia of unknown origins plus catheter-
associatedbacteremiaand,lastly,thebacteremia’ssecondarytootherfocalpoints.
The percentage of patients with infections (device-related infections) dropped
from15.5%in2009to5.7%in2014.Thissignificantdropcoincidesintimewiththe
period when the Zero Bacteremia and Zero Pneumonia programs were
implemented157
. Similarly, the use of antibiotics has decreased on the intensive
careunits from122.1to113.8daysofantibioticper100stays.Carbapenemsare
oneoftheantibioticgroupsmostused.
– The National Health System Health Care-Associated Infection Surveillance
System.TheMSSSI,incollaborationwiththeCarlosIIIHealthInstitute,theHealth
Regions and the scientific societies involved, has prepared a proposal regarding
which a consensus was reached with Spain’s Surveillance Body and which was
approved by the Public Health Commission for a national health care-associated
infections surveillance systemswhichwillmake itpossible toavail of systematic,
homogeneous informationwith a standardizedmethodology for ascertaining the
incidence and characteristics of the health care-associated infections and
facilitatingtheirpreventionandcontrol.
ThisproposalisinresponsetoarequestfromSpain’sCongressofDeputiesfora
National Plan for the Control of Health Care-Associated Infections a158
to be
developedandtherecommendationsfromtheCounciloftheEuropeanUnion7for
bolsteringthesurveillancesystemsactiveat thenational level for thepurposeof
evaluating and focusing the infection prevention and control policies on the
medical services centers. Similarly, there was a widespread feeling among the
61
different health authorities in favor of having a health care-associated infection
surveillancesystemforthehealthcareprovidedbySpain’sNHS.
– Surgicalsiteinfectionsurveillance.Thestudyofsurgicalsiteinfectionincidenceis
representative to a much lesser degree than the two aforementioned registers.
Approximately some 30 hospitals from various Health Regions take part in the
surveillance of the surgical processes suggested by the European Center for
DiseasePreventionandControl. SomeHealthRegions suchasMadrid,Catalunya
and the Basque Country has their own individual surgical infection surveillance
program(VIRAS159
,VINCAT160
andINOZ161
,respectively).
– Outbreaks.Althoughthepresenceofoutbreaksofnosocomialinfectionsshouldbe
notifiedtotheCarlosIIIHealthInstitute,complianceisrenderedtoasmalldegree,
the informationthereforebeingobtainedmainlybywayofscientificpublications
orpresentations.
– Antimicrobial resistance. Spain’sMicrobiology laboratories contribute toplotting
themapofresistancesbywayoftheirdatafrombloodculturesandothersafety
samples.Through theCarlos III Institute, the information is sent to theEuropeanAntimicrobial resistance interactive database (EARS-Net) program, currently
centralized at the European Center for Disease Prevention and Control 162. ThefindingsrankSpainamongthosecountrieshavingthehighestlevelofantimicrobial
resistances,especiallyforgram-negativebacteria,althoughtoalesserdegreethan
Greece,ItalyandPortugal163
.Thelatestdataisfor2011,thefiguresprovidedbeing
lowerthanthefiguresshownintheEPINEregisterfor2014154
.
– Antimicrobialconsumption.Spainprovidestheconsumptionsofantibioticsatthe
extrahospital level,not thedata for theconsumptionat thehospital level, to the
program European Surveillance of Antimicrobial Consumption Network (ESAC-Net164), also coordinated by the European Center for Disease Prevention andControl,whichhasbeenmonitoring theuseofantibiotics foryears.Thenational
dataonuse inhospitalizedpatients isobtainedfromEPINEandENVIN-HELICS. In
general, the data suggests a high degree of use and a high percentage of
treatments in health care-associated infections without any supporting
microbiologicaldocumentationservingasabasis.
Programs for preventing health care-associated infections promoted by the MSSSI,
withintheframeworkofthestrategyforpatientsafety.Someofthemostnoteworthy
oftheseprogramsare:
62
– SpanishNationalHealthSystemHandHygieneProgram.
In2006,Spain joined theWorldHealthOrganization“CleanCare isSafeCare”
campaign,themainobjectiveofwhichistofurtherenhanceadherencetoHand
Hygiene.TheSpanishNHSHandHygieneprogram165,promotedbytheMSSSI,is
beingcarriedoutincollaborationwithalloftheHealthRegionsforthepurpose
offurtherenhancingadherencetoHandHygieneandiscurrentlyimplemented
inmore than80%of thepublichospitalsandmedical servicescenters.Within
theframeworkofthisprogram,aconsensushasbeenreachedconcerningbasic
actions(mainlypromotingtheWorldHealthOrganization’smultimodalstrategy
and trainingof the“5moments”of theprocess)andevaluation indicators for
structure,processandoutcomewhichareevaluatedannually.
Asof2009,WorldHandHygieneDayhasbeenbeingcelebratednationwide
in Spain, with specific actions for professionals and patients in the Health
Regions and medical services centers, following the recommendations of the
WorldHealthOrganizationforthatday.
– Patientsafetyprogramforcriticalcarepatient
TheZeroBacteremiaandZeroPneumoniaprojects157
havemadeitpossible,by
wayofamultifactorialinterventionbasedonthesimultaneousimplementation
of a packageof simple, sustainablemeasures, not only to significantly reduce
theincidenceoftwoofthehighest-impact,highest-costhealthcare-associated
infections,butalsotofavorthenetworkingofmanyprofessionalsandcenters
nationwide and to serve as a reference study ofwhat should be a process of
puttingsafepracticesintopracticeatalllevelsofhealthcare.
– TheZeroBacteremiaProjectobjectiveswere:
a) To reduce the incidence-density rates (IDR) of the catheter-related
bacteremiato<4episodesper1000daysofcentralvenouscatheter.
b) To document all of the episodes of bacteremia, including the
bacteremia’ssecondarytootherfocalpoints,aswellastheetiologyandthe
characteristicsofthepatientswhoexperiencetheseepisodes.
c) To create working groups with leadership abilities which can follow
programsforthepreventionofothernosocomialinfections.
d) Tobolsterthesafetycultureinthemanagementofcriticalpatients.

63
Overthecourseofthe18monthsofthestudy(2009-2010),192ICUsfrom
all of theHealth Regions contributed cases, a 50%drop in the rate having
beenachievedinalltypesofhospitals166
.Itwasestimatedtowardtheendof
2013that384deathshadbeenpreventedand159,630.700€hadbeensaved
onhospitalstays.
– ZeroPneumoniaProject.FollowingthesamesetupasforZeroBacteremia,a
specificpackageofmeasuresandanintegralsafetyprogramwereproposed
in agreement with the Health Regions, the Spanish Society for l Intensive
CareMedicine, Critical Care and Coronary Care Units (SEMICYUC) and the
SpanishSocietyforIntensiveCareNursingandCoronaryCareUnits(SEEIUC).
The main objective was to reduce the IDR of Ventilator-Associated
Pneumonia (VAP) to < 9 episodes x 1000 days of mechanical ventilation
maintainingthesecondaryobjectivesof theZeroBacteremiaProject.More
than 240 ICU’s (80% of all ICUs in Spain) have taken part in the project,
havingachievedarateof lessthan7episodesper1000daysofmechanical
ventilation.Ithasbeenestimatedthat340deathshavebeenpreventedand
164millioneurossaved167
.
– Programs for the Optimization of In-Hospital Use of Antibiotics (PROA): The
Spanish Society for Infectious Diseases and Clinical Microbiology, the Spanish
SocietyofHospital Pharmacyand theSpanishSociety forPreventiveMedicine,
PublicHealthandHygienehavecometoanconsensusandpreparedaprogram
forfurtherenhancingtheprescriptionofantimicrobialdrugsforthepurposeof
reducingtheresistances,whichhasbeenbeingcarriedoutsuccessfullyinseveral
oftheSpanishNHShospitals168.
– Strategicplan foraction for reducing the riskof selectionanddisseminationof
resistances to antibiotics. Coordinated by the MSSSI through the Spanish
MedicinesandMedicalProductsAgency(AEMPS), thisPlancoversbothhuman
and veterinary medicine, having as its objective that of reducing the risk of
selectionanddisseminationofresistancestoantibiotics,alsoaimingatrendering
compliancewiththeEuropeanCommissionCommuniquéofNovember17,2011,
bywayofwhichthememberStateshavebeenrequestedtosetoutaplanfor
actionregardingresistancestoantibiotics,aswellastheConclusionsofCouncil
oftheEuropeanUnionofJune22nd,urgingthatajointapproachbetakentothis
issue169
.
64
TheagenciesandinstitutionswhicharecollaboratinginthisPlaninclude:
TheSpanishMinistryofHealth,SocialServicesandEquality (SpanishMedicines
andMedicalProductsAgency,theSpanishFoodSafetyandNutritionAgencyand
different General Directorates), the Ministry of Agriculture, Food and
Environmental Affairs, Ministry of Economy and Competitiveness (Carlos III
Health Institute), Complutense University of Madrid, Spanish Antibiogram
Committee,ScientificSocietiesinvolvedandOfficialProfessionalOrganizations.
� Surgery
InSpain,theincidenceofadverseeventsduetosurgeryisaround10.5%(8.1%-
12.5%),atotalof36.5%ofwhichwouldbepreventable170
.
In the National Patient Safety Strategy for the 2005-2011 period, it was
recommendedthatactionsbeimplementedforpromotingSafeSurgeryasofJanuary
2008, coinciding with the launching of the World Health Organization’s second
challenge “Safe Surgery Saves Lives”. The basic principles of this challenge were
classifiedinto4areas(1.Thepreventionofsurgicalwoundinfections2.Thesafetyof
anesthesia3.The trainingof safesurgical teams.4Themeasurementof thesurgical
services) aimed at achieving some top-priority objectives for preventing the adverse
events in surgery for which the World Health Organization facilitates as tools the
surgerysafetychecklistandamanualfortheimplementationthereof45.
TheHealthRegionsrecommendedandcontributedinitiativesandstandardsfor
the implementation of the aforementioned list in their hospital networks. Most of
these practiceswere included as recommendations in the document “Surgical Block
Standards and Recommendations”171
published by the MSSSI, which additionally
included theadaptationof the liston thepartof theSpanishSurgeon’sAssociation.
Despitetheseactions,theprocessofimplementingthesafesurgerychecklistinSpain’s
NHShasbeendifficult,incompleteandhighlyvarying.
The World Health Organization’s challenge also proposed a minimum set of
uniform indicators (“vital surgical statistics”) for the national and international
surveillanceofsurgicalcare.Theinformationon“vitalstatistics”isvariableatthelevel
oftheHealthRegions,noregisterexistingforthesestatisticsatthenationallevel.
Someoftheotheroutstandingeffortsincludetherecommendationsonthepart
oftheSpanishSocietyforAnesthesiologyandResuscitationfortheAnesthesiaservices
to adopt the principles of the Helsinki Declaration on Patient Safety in
Anesthesiology116
, which the Spanish Society for Anesthesiology and Resuscitation
65
subscribed in its launching in June 2010. Also worthy of special mention is the
publication of recommendations for the labeling of drugs administered in
anesthesiology and the publication of a pre-procedure anesthesia equipment
checklist172
.
� Safecare
The ENEAS report attributes 7.63% of the adverse events to care-related
causes15. The factors associated with these adverse events comprise useful
informationfortargetingthestrategiesaimedatfurtherenhancingpatientcare.
As a result of the decentralized funding of the Health Regions within the
frameworkofthePatientSafetyStrategywithinthe2005-2011timeframe,ithasbeen
encouragedthatdifferentprojectsandbestpracticesbegottenunderwayinnursing
care which have made it possible to further enhance the aspects related to the
prevention and treatment of pressure ulcers, fail-safe patient identification, the
furtherenhancementofthepreventionofaccidentalfalls,thepreventionofinfection
withtheHandHygienestrategies,thereductionofcatheter-associatedbacteremiaor
ventilator-associatedpneumonia,andthesafeuseofmedications.
Nevertheless, the safe carepracticeshavenotbeen implemented in full, and
thedegreetowhichimplementedhasvariedgreatlynationwide.Someofthepossible
causes may include the nursing care plans barely existing at all and the scarcity of
specificinformationsystemsmakingitpossibletoevaluatethesame.
The reference study on patient safety in regard to the care provided is the
project“StandardsofCareQualityforPatientSafetyinSpain’sNHShospitals,knownas
the “SENECA” study173
, fundedby theMSSSI, basedonwhich different standards of
carequalityforSpain’sNHSwerevoluntarilyevaluated.Thisstudymadeitpossibleto
ascertainthequalityofthecareprovidedrelatedtopatientsafetynationwideandto
recommendanumberofmoreorlesscomplexpracticeswhichwerethenfollowedto
differingdegreesbytheHealthRegions.
Measures aimed at setting out a crisis plan for the propermanagement of severeadverseevents
According to the Gallagher study, a total of 55% of all Canadian and U.S.
physicians acknowledged having made a clinical error174
. In Spain, according to the
ENEASstudydata, itcanbeestimatedthataround15%of thehospitalprofessionals

66
may find themselves involved in an adverse event per year15, although they be a
matterofadverseeventswithoutanysevereconsequencesinmostcases.
When a severe adverse event occurs, the patient is themain victim, but the
professionalsinvolvedarethesecondvictims.Therepercussionsofadverseeventson
the second victimsmay go so far as to leave them incapacitated, seriously affecting
theircarryingouttheirduties,aboveallwhenthere isexternalsocialpressure175
. In
Spain,thereareveryfewstudiesdealingwiththeconsequencesofadverseeventon
professionals176
,itthereforebeingnecessarytolearnfromtheexperiencescarriedout
inothersettings177
. Itwouldbedesirable for themedical servicescenters toavailof
specificstrategieswhichweretoinclude:whatmustonedoandnotdowhenasevere
adverse event occurs; actions for frankly communicating with the patients and
caregivers;proceduresforsupportingtheprofessionalsinvolvedintheadverseevents;
andtheapproachastohowtomanagethecommunicationwiththemediaoncethey
have occurred. The experiences carried out in other countries may be useful for
putting into practice in these situations178, 179,180,181
. Some Health Regions have
developed guidelines for the management of severe adverse events, including the
approachfordealingwiththesecondvictimsinasystematicmanner182
.
Reportringandlearningsystems
TheMSSSIhaspromotedtheReportingandLearningSystemforPatientSafety
(SINASP)183
as a reporting system readily available to the health care professionals
throughtheirregionalhealthservices.AtotalofnineHealthRegionsandtheNational
HealthcareManagement InstituteforCeutaandMelilla (INGESA)arecurrentlyusing
thisreportingsystem,whilstalloftheotherHealthRegionshavedevelopedtheirown
reportingsystems,somepriortotheReportingandLearningSystemforPatientSafety.
Fig.2detailstheincidentreportingsystemsdevelopedinSpain’sNHS, inconjunction
with their characteristics (anonymous, voluntary, type of incident, setting and
accessibilitytopatients).
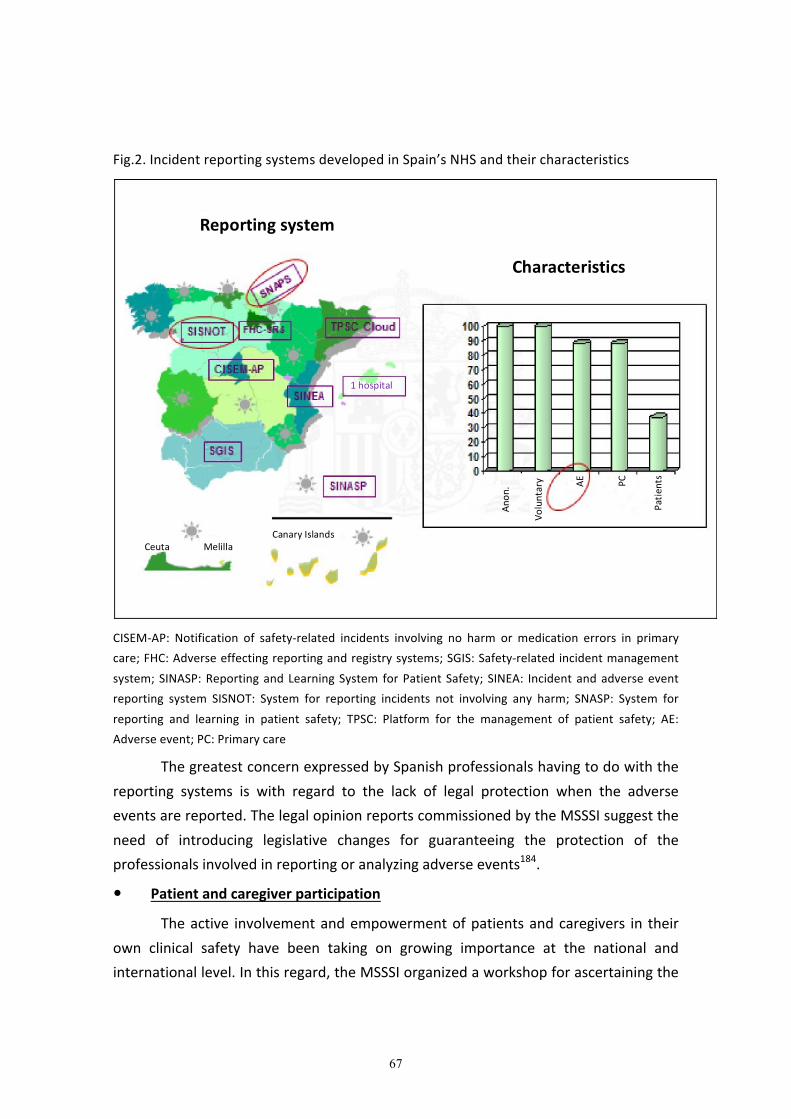
67
Fig.2.IncidentreportingsystemsdevelopedinSpain’sNHSandtheircharacteristics
CISEM-AP: Notification of safety-related incidents involving no harm ormedication errors in primary
care;FHC:Adverseeffectingreportingandregistrysystems;SGIS:Safety-relatedincidentmanagement
system;SINASP:ReportingandLearningSystem forPatientSafety; SINEA: Incidentandadverseevent
reporting system SISNOT: System for reporting incidents not involving any harm; SNASP: System for
reporting and learning in patient safety; TPSC: Platform for the management of patient safety; AE:
Adverseevent;PC:Primarycare
ThegreatestconcernexpressedbySpanishprofessionalshavingtodowiththe
reporting systems is with regard to the lack of legal protection when the adverse
eventsarereported.ThelegalopinionreportscommissionedbytheMSSSIsuggestthe
need of introducing legislative changes for guaranteeing the protection of the
professionalsinvolvedinreportingoranalyzingadverseevents184
.
� Patientandcaregiverparticipation
Theactive involvementandempowermentofpatientsandcaregivers in their
own clinical safety have been taking on growing importance at the national and
internationallevel.Inthisregard,theMSSSIorganizedaworkshopforascertainingthe
Reportingsystem
Characteristics
Anon.
Voluntary
AE
PC
Patients
Ceuta Melilla
CanaryIslands
1hospital
68
opinions, expectations and positioning of experts, representatives of patients’
associations, consumers, users and patient advocates in different Health Regions
concerning this matter and their possible participation in future actions aimed at
preventingrisksandproposingpatientsafety-relatedsolutions.Thisdocumentandthe
CitizenTrainersNetworkdevelopedfollowingtheworkshopmarkedamilestoneinthe
change necessary for getting patients and caregivers actively involved in further
enhancingclinicalsafety.Currently,theCitizenTrainersNetworkhasbeenintegrated
intoSpain’sNHSCitizenHealthSchoolsNetworkpromotedbytheMSSSIandcarried
outincollaborationwiththeHealthRegions186
.
Researchintopatientsafety
Safehealthcarerequiresemployingproceduresandpracticeswhichhavebeen
shown to be effective for reducing the occurrence of mistakes, errors and adverse
outcomesandalsoforgeneratingnewknowledgeastothefactorswhichcontributeto
furtherenhancingpatientsafety.
Patient safety andpatient safety-related incidents the twoopposites sidesof
onesamecoinasyettobeminted:themanagementoftheriskinvolvedinproviding
healthcare.
Thefollowingcanbeconsideredasareasforresearchinpatientsafety187
:
– Quantifyingthemagnitudeandcharacteristicsoftheclinicalrisk
– Improving the comprehension of the factors which contribute to the
occurrenceoftheincidentsrelatedtopatientsafety.
– Evaluatingtheimpactoftheadverseeventsonthehealthsystem.
– Identifying effective, feasible and sustainable solutions for achieving safe
healthcareandpreventingadverseeventsandincidents.
Specialmentionmustbemadeof the fact that a greatnumberof articles and
monographicstudiesonpatientsafetyhavebeenpublishedinSpanishjournalsinthe
fieldofclinicalquality188
.Aneithersystematicnorcompletelythoroughreviewofwhat
hasbeenpublishedoverthepastfewyearsleadsonetotheconclusionthattherehas
beenamajor increase in the amountof researchonpatient safetypublishedat the
national and international level in comparison to earlier time frames189,190
. Despite
thisincrease,itstillcontinuestobenecessarytogeneratevalid,accurateevidenceon
the impactof clinical andorganizational solutionswhichwill furtherenhance safety.
69
Similarly, delving deeper into the epidemiological study of incidents and adverse
eventswillmake it possible to better know the risk factors of the patientswho are
mostexposedtoexperiencingadverseeventsandwillfacilitatetheimplementationof
preventionstrategies.
DEPLOYING THE PATIENT SAFETY STRATEGY IN THE SPANISH NATIONAL HEALTHSYSTEM
For the purpose of availing of updated information on the deployment of
strategies, programs and actions which are being carried out in Spain’s NHS with
regardtopatientsafety,sharinginformationandfosteringthesharingofexperiences,
a questionnaire was sent out to the Health Regions’ in which information was
requestedconcerningorganizationofthepatientsafetystrategy,developmentoflines
ofactionfundedbytheMSSSIupto2012,reportingsystem,patientparticipationand
deploymentinprimarycare.
TheseventeenHealthRegionsandINGESAansweredthesurvey.
The findings are detailed in following, summarized by each dimension of the
questionnaire:
� DevelopmentofthepatientsafetystrategyonthepartoftheHealthRegionswith
regardtoitsorganization:
o A total of 13 Health Regions say they have a Patient Safety Strategy
(72.2%).Therestsaytheyaregoingtodevelopastrategy.
� ActionscarriedoutbytheHealthRegionsforfosteringthesafetyculture:
o Allof theHealthRegionsarecarryingoutpatientsafetytrainingactions,
81%sayingtheycurrentlyhaveaspecificpatientsafetytrainingprogram
inplaceforhealthcareprofessionals.
o Atotalof72.2%oftheHealthRegionssaytheyarefurnishinginformation
to professionals concerning standards, measures for reducing incidents
andbestpracticesinpatientsafety.Therestsaytheyareworkingonthis
aspect.
� Safe practices implemented, recommended in the strategy for patient safety
carriedoutintheNHS.
o Fig. 3 details the information furnishedby theHealth Regions concerning
theimplementationoftheseactivitiesinspecializedcareandinandinFig.4
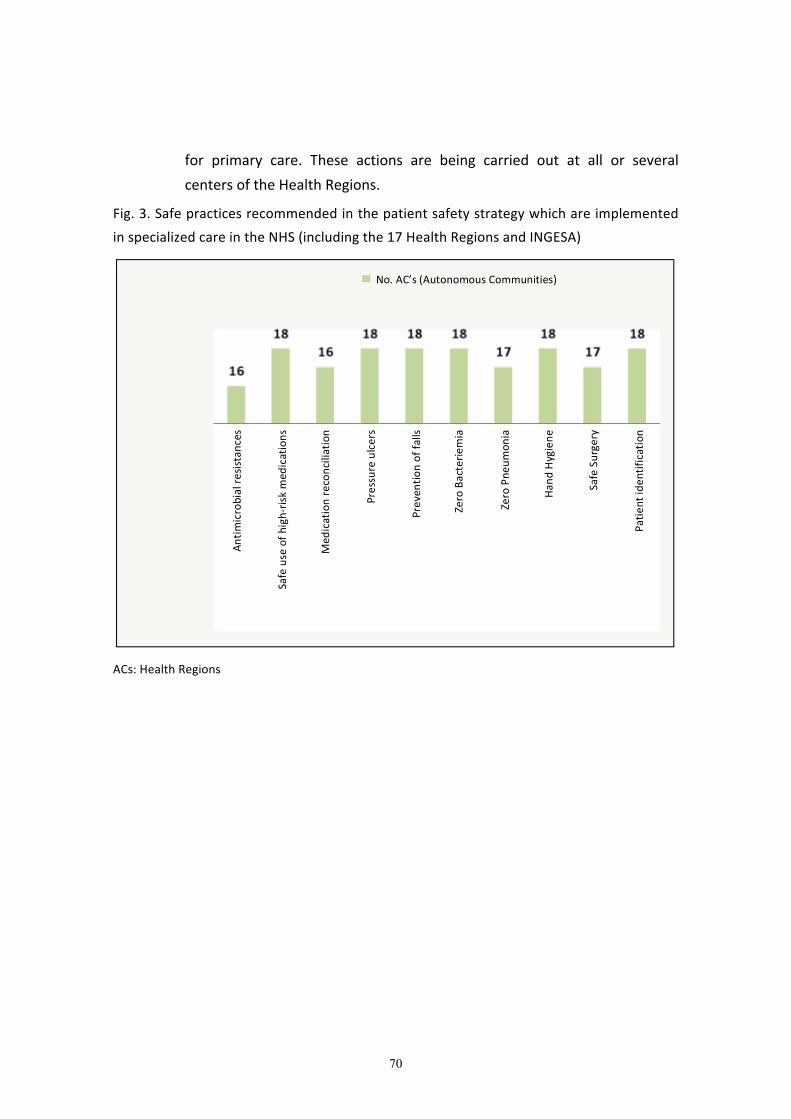
70
for primary care. These actions are being carried out at all or several
centersoftheHealthRegions.
Fig.3.Safepracticesrecommendedinthepatientsafetystrategywhichareimplemented
inspecializedcareintheNHS(includingthe17HealthRegionsandINGESA)
ACs:HealthRegions
No.AC’s(AutonomousCommunities)
Antimicrobialresistances
Safeuseofhigh-riskm
edications
Medicationreconciliation
Pressureulcers
Preventionoffalls
ZeroBacteriemia
ZeroPneumonia
HandHygiene
SafeSurgery
Patientidentification

71
Fig.4.SafepracticesrecommendedinthepatientsafetystrategyimplementedinSpain’sNHS
primarycare(includingthe17HealthRegionsandINGESA)
ACs:HealthRegions
A remarkable difference among Health Regions is noted in the
implementationof theeighteffectivepractices targetingprimarycare, solely
two Health Regions incorporating all eight of these practices, three
incorporating six of the practices and in the lower range, one Autonomous
Communitywithonesinglepracticeimplemented.
In addition to these practices, theHealth Regions implement other safe
practicesinkeepingwiththeobjectivesoftheirstrategies.
Asfarastheimplementationofsafepracticesisconcerned,itmayalsobe
saidthat,withintheframeworkoftheJointActionforPatientSafetyandCare
Quality (PaSQ), twelve Health Regions and 121medical services centers are
taking part in the implementation of the four safe practices recommended:
Multimodal strategy for further enhancing Hand Hygiene, surgical checklist,
medication reconciliation and scale for the early detection of clinical
deterioration in pediatrics191
. The evaluation is made by means of a
questionnaireandspecificindicators.
No.AC’s(AutonomousCommunities)Antimicrobial
resistances
Useofhigh-risk
medications
Medication
reconciliation
Pressureulcers
Preventionoffalls
HandHygiene
SafeSurgery
Patientidentification

72
� AlloftheHealthRegionshavesomesystemforreportingincidentsrelatedtothe
healthcareprovided.Dueto their frequency, theReportingandLearningSystem
forPatientSafetyisthefirst-linesystem.Theimplementationismostlyinhospitals
andprimarycare,althoughthishasalsobeenextended,insomeHealthRegions,to
social services medical services centers, extrahospital emergency services,
psychiatriccenters,etc.
� A total of 50% of the Health Regions stated having informed the Patients’
Associations in theCommunityof thestrategiesorprogramsbeingcarriedout in
patientsafety,atotalof39%nothavingdonesoand12%nothavingansweredthis
question.
o A total of 14 Health Regions answered that there is no stable setup for
patientand/or caregiverparticipation inpatient safety; a totalof3having
answeredthatsuchasetupdoesexistandonenothavingansweredatall.
o Most of the actions carried out have to do with activities involving
informationandtrainingforpatients.
� Deployment of the patient safety strategywithin the primary care setting in the
HealthRegions.
o ThreeHealthRegionssaytheyhaveaspecificpatientsafetystrategyinplace
forprimarycare.
o Atotalof sevenHealthRegionsstate theirorganizational chart includinga
person in charge of patient safety in primary care. In the rest, this is
integratedintotheoverallPatientSafetyStrategy.
� Programs/actions carried out by the Health Regions for promoting research into
patientsafety.
o AtotalofsixHealthRegionsfundspecificlinesofresearchinpatientsafety.
Therestcarryoutresearchprojects inpatientsafetywithintheframework
of general lines of research. Similarly, many of them carry out research
projectswithintheframeworkofcarequalityenhancementprojects.
73
Evaluationofthedeploymentofthepatientsafetystrategy
The Patient Safety Strategy has promoted the creation of elements of safety
infrastructure and the implementation of safe practices at the level of the Health
Regions. During the time frame throughoutwhich the strategy is being carried out,
these elements have been being evaluated byway of a number of indicatorswhich
wereagreedwith the InstitutionalCommittee for theStrategy (representatives from
thedifferentHealthRegions).
Theindicatorsproposedhavebeengroupedinto:patientsafetyindicatorsand
theHandHygieneprogramindicators
� Thepatientsafetyindicatorsmakereferencetothelineswhichhavebeenbeing
promoted in the Health Regions andwhichwere funded up to 2011 byway of
specificagreementsorspecifically-allocatedfundingfortheNHSstrategies(Table
11).
Table11.Patientsafetystrategyindicatorsforthe2010-2013timeframe
Spain’sNHSPatientSafetyIndicators
1. %HospitalshavingaPS-relatedIncidentReportingandLearningSystem
2. %PrimarycarecentershavingaPS-relatedIncidentReportingandLearningSystem
3. %HospitalshavingFunctionalRiskManagementUnitswhichareoperative
4. %PrimarycaremanagementdepartmentshavingFunctionalRiskManagementUnits
5. %HospitalshavingaPatientIdentificationProtocol
6. %Hospitalshavingthesafesurgerychecklistimplemented
7. % Patients having undergone electric surgery regarding whom the safe surgery
checklistisimplemented
8. %Hospitalshavinghigh-riskmedicationprotocolsinplace
9. %Hospitalshavingprotocolsinplaceformedicationreconciliationatdischarge
10. %Hospitals using the self-check safety questionnaire regarding the system for in-
hospitalmedicationuse
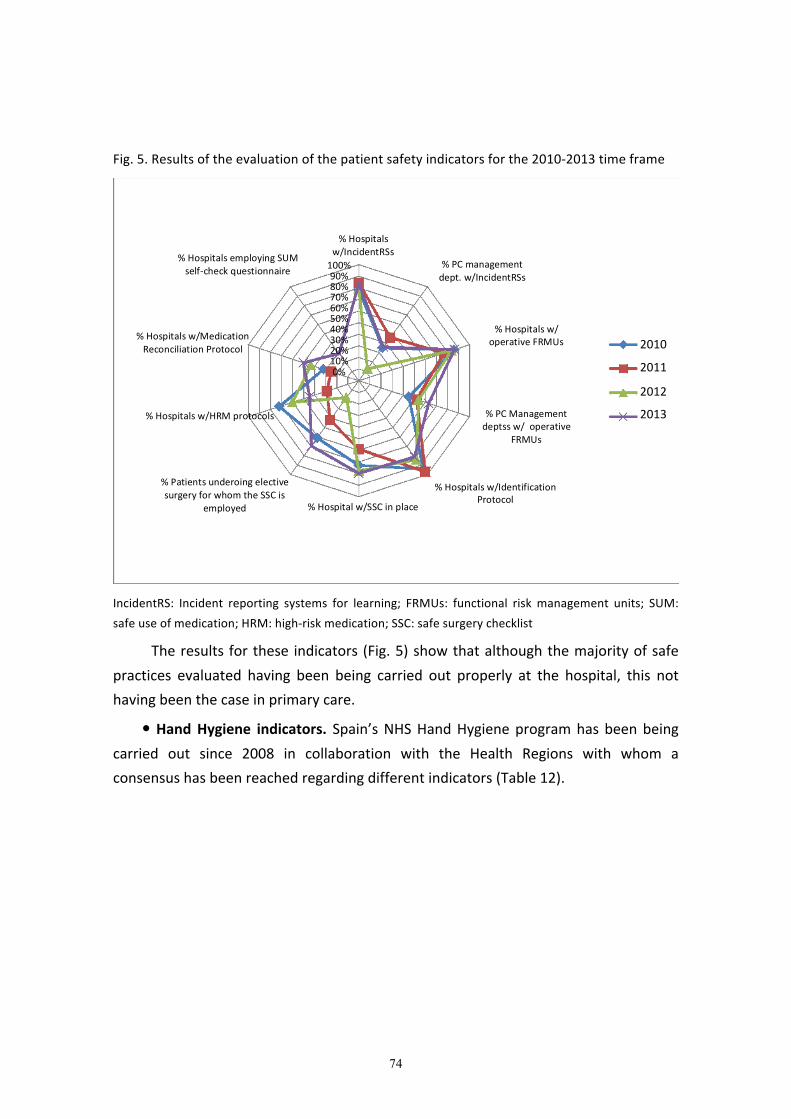
74
Fig.5.Resultsoftheevaluationofthepatientsafetyindicatorsforthe2010-2013timeframe
IncidentRS: Incident reporting systems for learning; FRMUs: functional riskmanagement units; SUM:
safeuseofmedication;HRM:high-riskmedication;SSC:safesurgerychecklist
Theresults forthese indicators(Fig.5)showthatalthoughthemajorityofsafe
practices evaluated having been being carried out properly at the hospital, this not
havingbeenthecaseinprimarycare.
�HandHygiene indicators. Spain’sNHSHandHygieneprogramhasbeenbeing
carried out since 2008 in collaboration with the Health Regions with whom a
consensushasbeenreachedregardingdifferentindicators(Table12).
%Hospitals
w/IncidentRSs
%PCmanagement
dept.w/IncidentRSs
%Hospitalsw/
operativeFRMUs
%PCManagement
deptssw/operative
FRMUs
%Hospitalsw/Identification
Protocol%Hospitalw/SSCinplace
%Patientsunderoingelective
surgeryforwhomtheSSCis
employed
%Hospitalsw/HRMprotocols
%Hospitalsw/Medication
ReconciliationProtocol
%HospitalsemployingSUM
self-checkquestionnaire
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
2010
2011
2012
2013

75
Table12.Spain’sNHSHandHygieneprogramindicators
Spain’sNHSHandHygieneprogramindicators
1. %Bedswithalcohol-basedproductintheroom
2. %Bedsonintensivecareunitswithalcohol-basedproductatcare-providingpoint
3. %Primarycarecenterswithpocketalcohol-basedproductforhomecare
4. %Hospitalshavingtrainingactivitiesinplace
5. %Primarycarecentershavingtrainingactivitiesinplace
6. Consumptionofalcohol-basedproducthospitalization:litersofalcohol-basedproduce
foreverythousandpatientsperday
7. %Bedswithalcohol-basedproductatcare-providingpoint
8. %Hospitalswhichobservecompliancewiththe“5moments”
9. %Hospitalsconductingself-checkaspertheWHOrecommendations
10. %Hospitalshavingtrainingactivitiesinthe“5moments”
Theresultofthemeasurementoftheseindicatorsshowsanimprovementover
thecourseoftimeforallofthemexceptfortheaspecthavingtodowithtraining in
HandHygieneinprimarycare.

76
Fig.6.ResultsoftheevaluationoftheNHSHandHygieneindicators
ABP:alcohol-basedproduct;ICU:intensivecareunit;PCC:primarycarecenter
The consumption of alcohol-based products has been progressively improving
overthepastfewyearsuptothepointofmeetingthestandardsrecommendedbythe
WorldHealthOrganization(Fig.7).
Fig.7. Evolutionof the consumptionofalcohol-basedproduct in theNHS for the2009-2013
period
RoomswithABP
ICUswithABPs
PCCwithABPs
HospitalTraining
Trainingin“5
moments”Hospitals
PCCTraining
ABPcare-providing
point
Compliancew“5
moments”Hospitals
Self-checkHospitals

77
� Indicatorsofspecificprograms
Evaluationshaveadditionallybeenbeingmadeofindicatorsofspecificprograms
suchasSINASP,ZeroToleranceontheintensivecareunits,safeuseofmedication,the
resultsofwhicharedisseminatedbywayoftheMSSSIPatientSafetyWeb192.
� Accreditation
Theperiodicevaluation,whichismadeviatheMSSSI,ofthehospitalsaccredited
for Specialized Health care Training in Health Sciences has included patient safety
criteria which are related to the following clinical practices recommended in the
strategy: Hand hygiene, high-risk medications, medication reconciliations, surgical
checklistandfail-safepatientidentification.
Thedocumentfurnishedbythecenterpropermadeitpossibleforanassessment
tohavebeenmade in2012at the levelofdevelopmentor implementationof these
safepracticesbyemployingthecriteriaincludedinTable13.
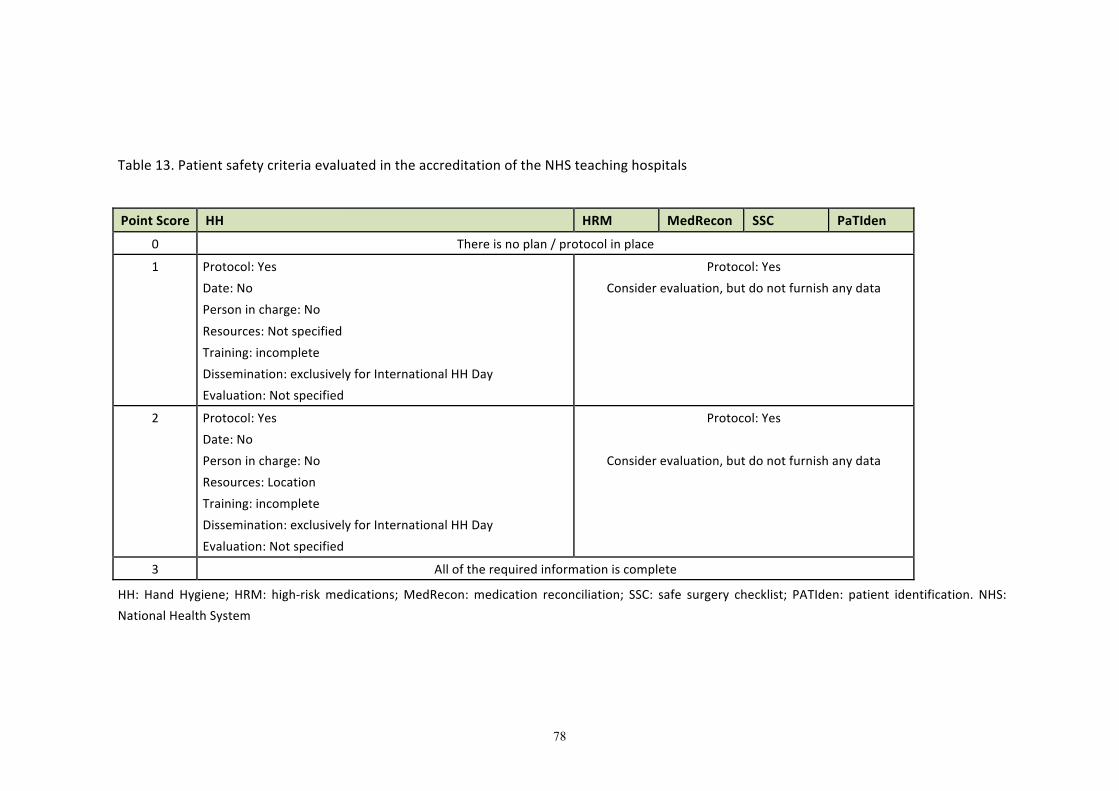
78
Table13.PatientsafetycriteriaevaluatedintheaccreditationoftheNHSteachinghospitals
PointScore HH HRM MedRecon SSC PaTIden
0 Thereisnoplan/protocolinplace
1 Protocol:Yes
Date:No
Personincharge:No
Resources:Notspecified
Training:incomplete
Dissemination:exclusivelyforInternationalHHDay
Evaluation:Notspecified
Protocol:Yes
Considerevaluation,butdonotfurnishanydata
2 Protocol:Yes
Date:No
Personincharge:No
Resources:Location
Training:incomplete
Dissemination:exclusivelyforInternationalHHDay
Evaluation:Notspecified
Protocol:Yes
Considerevaluation,butdonotfurnishanydata
3 Alloftherequiredinformationiscomplete
HH: Hand Hygiene; HRM: high-riskmedications;MedRecon:medication reconciliation; SSC: safe surgery checklist; PATIden: patient identification. NHS:
NationalHealthSystem
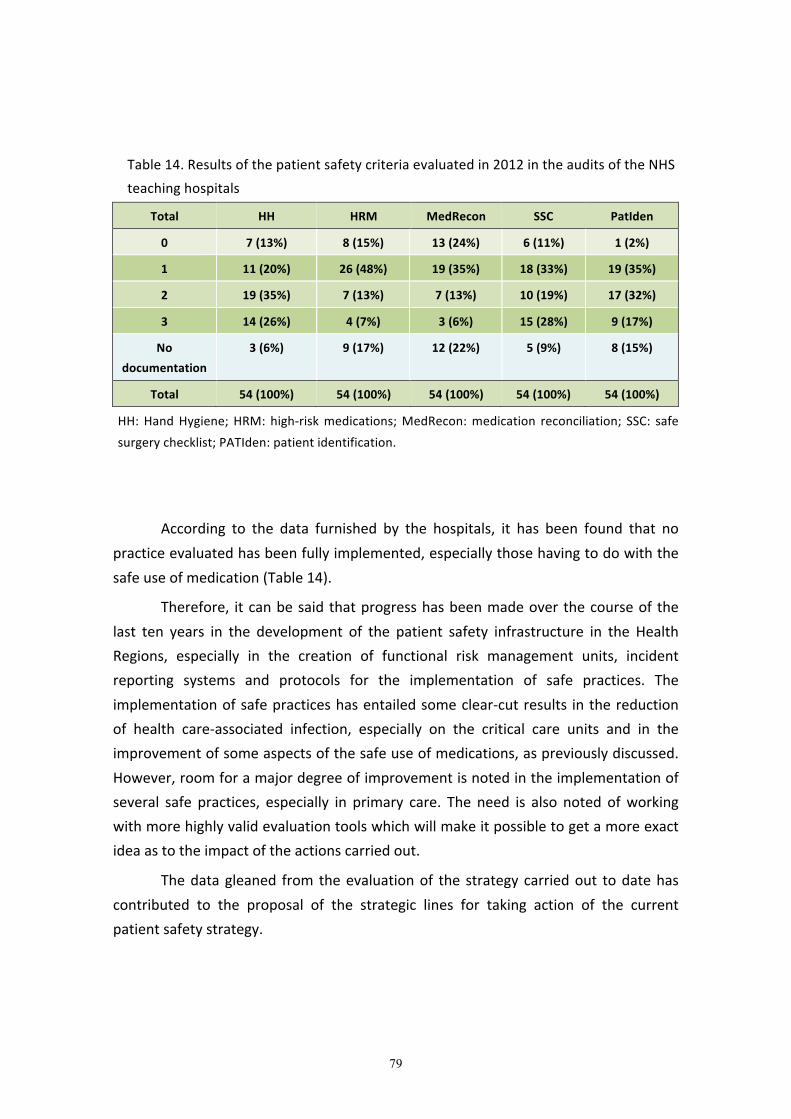
79
Table14.Resultsofthepatientsafetycriteriaevaluatedin2012intheauditsoftheNHSteachinghospitals
Total HH HRM MedRecon SSC PatIden
0 7(13%) 8(15%) 13(24%) 6(11%) 1(2%)
1 11(20%) 26(48%) 19(35%) 18(33%) 19(35%)
2 19(35%) 7(13%) 7(13%) 10(19%) 17(32%)
3 14(26%) 4(7%) 3(6%) 15(28%) 9(17%)
Nodocumentation
3(6%) 9(17%) 12(22%) 5(9%) 8(15%)
Total 54(100%) 54(100%) 54(100%) 54(100%) 54(100%)
HH:HandHygiene;HRM: high-riskmedications;MedRecon:medication reconciliation; SSC: safesurgerychecklist;PATIden:patientidentification.
According to the data furnished by the hospitals, it has been found that nopracticeevaluatedhasbeenfullyimplemented,especiallythosehavingtodowiththesafeuseofmedication(Table14).
Therefore, itcanbesaidthatprogresshasbeenmadeoverthecourseof thelast ten years in the development of the patient safety infrastructure in the HealthRegions, especially in the creation of functional risk management units, incidentreporting systems and protocols for the implementation of safe practices. Theimplementationofsafepracticeshasentailedsomeclear-cutresults inthereductionof health care-associated infection, especially on the critical care units and in theimprovementofsomeaspectsofthesafeuseofmedications,aspreviouslydiscussed.However,roomforamajordegreeofimprovementisnotedintheimplementationofseveral safe practices, especially in primary care. The need is also noted ofworkingwithmorehighlyvalidevaluationtoolswhichwillmakeitpossibletogetamoreexactideaastotheimpactoftheactionscarriedout.
Thedatagleaned from theevaluationof the strategy carriedout todatehascontributed to the proposal of the strategic lines for taking action of the currentpatientsafetystrategy.
80
2.STRATEGICLINESOFACTION
� Strategiclineofaction1:Patiensafetyculture,humanandorganizationalfactors,andtrainingA positive patient safety-related culture in the health care institutions is an
indispensable pre-requisite for preventing and minimizing patient safety-relatedincidentsandbeingabletolearnfrompasterrorsinordertoreducetheprobabilityoftheirreoccurring.
For thepurposeof furtherenhancingpatientsafetyculture, it isnecessary tocontinue carryingout actions aimedatmeasuring andenhancing the safety climate,informingandtrainingallNHSprofessionalsinsafety-relatedaspects,fosteringtrainingineffectivecare,trainingtheworkingteamsinriskmanagement,fosteringleadershipin safety, reporting and learning from the incidents and keeping the professionalsinformation of the details of the evaluation of their medical services centers,stimulatingtheiractiveinvolvementintheenhancementsproposed.
General objective 1: Further enhance patient safety culture, human andorganizationalfactors
Specificobjectives:
1. Promote themedical servicescentersavailingofa safetyplan (theirownorinstitutional)whichactivelyinvolvesalloftheprofessionalsandisknownbyall.
2. Promote the leadership of the professionals for assuring that the patientsafetyplanobjectiveswillbeachieved.
3. Favortheevaluationofthesafetyclimateinthehealthcareorganizationsandthedisseminationof their findings,asanaid in the implementationof safepractices.
4. Fosterbasictraininginpatientsafetyofallofthehealthcareprofessionalsatalllevelsoftheirtraininganddevelopment.
5. Disseminate theknowledgeandexperiencesconcerningpatientsafety toalllevelsoftheNationalHealthSystem.
81
6. Favorthedisseminationofrecommendationsforthepurposeofpreventinghealthcarefrombeingprovidedwhichisofverylittlevalueorisharmfultopatients.
Recommendations:
• Setoutplansforactioninpatientsafetyatthemedicalservicescenterswithannualobjectives,evaluationandplanningfordisseminationoftheresults.
• Incorporate clinical leaders who will promote the implementation,developmentandevaluationof safe clinicalpracticesat the centers/on theunits.
• Includepatientsafetyasoneoftheaspectstobeaddressedintheplansfortakingonnewprofessionals.
• Periodically evaluation, byway of validated tools, the safety climate of theorganization as an aid toward knowing the weak points and strong pointsregardingpatientsafety.
• Reachaconsensusregardingaminimumbasictrainingcurriculuminpatientsafety for the professionals in the NHS which includes concepts on safeclinical practices, communicating, teamwork and health services factorswhichhaveabearingonpatientsafety.
• Promote thebasic training inpatient safetyof thehealthcareprofessionalsduring their undergraduate schooling, specialized training and continuedtraining.
• Identify,disseminateandshareatthenational,regionalandlocallevelsbestpractices,informationandexperiencesonpatientsafetybywayofdifferentmeanssuchascongresses,workshops,conferences,webpages,etc.
• Periodically disseminate the updated recommendations for the purpose ofpreventing unnecessary health care being provided which is of very littlevalueorwhichisharmfulforthepatient.

82
� Strategiclineofaction2:SafeclinicalpracticesDifferent international organizations have recommended different safe
practicesonthebasisof thefrequencyof themost frequentadverseeventsandtheexistingevidencefortheircontrol.WithintheframeworkofthePatientSafetyStrategyandincollaborationwiththeHealthRegions,theMSSSIhasbeenpromotingdifferentsafepracticesinkeepingwiththeinternationalrecommendations.
The safe practices recommended in this strategy are mainly those aimed atpromoting the safe use ofmedications, preventing health care-associated infectionsandpreventingtheharmassociatedwithsurgeryorpatientcareprocedures,whicharethe main factors associated with the adverse events according to the differentepidemiological studies conducted at the national level 5,26,27,28,29. Other practicesrecommended herein, such as appropriate patient identification, effectivecommunicating or the safe use of ionizing radiation also contribute to preventingavoidable adverse events. The inclusion of recommendation on the adequatemanagementofsevereadverseevents is inkeepingwithawidespreadfeeling intheNHSastoitbeingnecessarytodealwiththisproblem.
Generalobjective2.1:Promotesafemedicationuse
The activities of pharmacovigilance, training and updating of physicians andnurses in therapeutics and clinical pharmacology or the prevention of errors in themedicationcircuitsaresomeoftherelevantinitiativesforfurtherenhancingsafetyintheuseofmedications.
Thee-prescription is usefulwhenassociatedwith supporting clinical decision-makingprogramsforreducingtheerrorsresultingfromanincorrectprescriptionandcan also even appreciably enhance the treatments being followed193. The computerapplications can also provide the information and the instructions necessary forcorrectlyadministeringthemedications.
High-risk medications have a greater probability than other types ofmedicationsofbeingassociatedwithadverseeventsof severeconsequences for thepatients. The health care institutions must identify these medications, set outproceduresfortheirsafemanagementinallofthecare-providingprocesses,evaluatethe procedures implemented for specific groups ofmedicines and take specific risk-reducingmeasures.

83
Chronic patients, especially polymedicated patients, are more vulnerable tomedication errors and must therefore be given special care and require a clinicalreview being made of the medication regarding both the effectiveness of thetreatments and the adherence to the same. One internationally recommendedpracticeaimedatreducingmedicationerrorsincare-providingtransitions,particularlyusefulinthesepatients,ismedicationreconciliation.Thisisaformal,multidisciplinaryprocesswhichisaimedatachievingthattheinformationwhichisconveyedconcerningthe medication at the points of care-providing transfer will be one in the same,accurateandcomplete194.Thisprocessmustbecarriedoutwiththeparticipationofalloftheprofessionalsresponsibleforthepatientinquestionandwiththepatientand/orcaregiverproper,wheneverpossible.Thiswouldalsomakeitpossibletoevaluatetheadherenceand/orlackofcomprehensionofthetreatments.
Thepatientsandtheircaregiversplayafundamentalroleinmedicationsafetyand thereforemust be informed so as to be able to assume responsibility for theirtreatment.Thepatientsmustbepreparedtoserveasabarrierforpreventingpossiblemedicationerrorswhichoccurinotherprocesses,especiallyforpreventingtheirownerrorsduringtheprocessesofadministeringthemediationsintheirownhomes.
The analysis and management of the medication errors detected by thehealth care professionals in the course of their activity is an essential strategy forfurtherenhancingthequalityandsafetyofthesystemfortheuseofmediationsandakeyelementforthecreationofasafetycultureatthelocallevelwhichmustcontinuebeingmaintainedforthepurposeoffacilitatingthesharingofexperiences,conveyingthelessonslearnedtotheentireNHSandpreventingthesameerrorsfromonceagainaffectingotherpatientsinthefuture.
Specificobjectives:
1. Promotee-prescriptionsassistedwithclinicaldecision-makinghelpsystemsofproveneffectiveness.
2. Fostertheimplementationofsafepracticeswithhigh-riskmedication.
3. Promotemedicationreconciliationduringthecare-providingtransitions.
4. Encourage initiatives being taken for further enhancing safety in the use ofmedication, especially in polymedicated chronic patients and in pediatricpatients.
84
5. Promotethetrainingofhealthcareprofessionalsconcerningthesafeuseofmedications.
6. Promote the training of the patients/caregivers concerning the use ofmedicationsandtheiractiveinvolvementinthetreatments.
7. Promotethereportingofincidentsrelatedtotheuseofmedicationsthroughtheexistingreportingsystems.
8. Promote the self-evaluation of the safety of the system for the use ofmedicationsatthemedicalservicescenters.
Recommendations:
• Carry out actions for implementing e-prescription programs which includeclinicaldecision-makinghelpsystemswhichare integrated into themedicalservices center information systems and are available for all of theprofessionalsinvolvedinthecarebeingprovidedforthepatientinquestion.
• Set out specific interventions aimedat preventing themost frequent errorsinvolvinghigh-riskmedications.
• Standardize the procedures for preparing and administering injectablemedicinesandparenteralnutrition.
• Systematicallyreviewthemedicationinthepolymedicatedchronicpatientsinordertodetectorpreventadverseevents,guaranteepropermedicationandfurtherenhanceadherencetothetreatment.
• Setout recommendationsconcerning theuseofabbreviations, symbolsandphrasingusedintheprocessofprescribingandadministeringmedicines.
• Determinespecificinterventionsaimedatpreventingmedicationerrorsinthecareprovidedforpediatricpatients(training,disseminationofguides,etc.).
• Reconcile the medication during care-providing transitions, especially inpolymedicatedchronicpatientsand inhigh-riskpatients.This reconciliationmust involve the collaboration of all of the people involved (professionalsresponsible for the patient in question, patient/caregiver, communitypharmacy,etc.).
• Carryouttrainingactionsofferedforthehealthcareprofessionalsconcerningthesafeuseofmedications.
85
• Carry out programs for informing and training the patients/caregivers,especiallythosepolymedicatedorthosetakinghigh-riskmedications,atallofthecare-providinglevels.
• MaintainandfurtherenhancethereportingoferrorsandincidentsinvolvingmedicationswhichoccurintheNHSbywayoftheexistingreportingsystems,includingtheanalysisandevaluationsoftheinformationgeneratedandthedisseminationoffittingrecommendations.
• Create the necessary collaboration with the pharmacovigilance centers sothat the errors involving harm will be notified to the SpanishPharmacovigilanceSystem.
• Conduct periodic self-checks on the safety of the system for the use ofmedications by employing standardized tools and setting outrecommendationforimprovement.
• Increase the surveillance and supervision of the safe use ofmedications onthepartofthepharmacyunitsandservices.
Generalobjective2.2:Promotesafepractices forpreventingandcontrollinghealthcare-associatedinfections
Health care-associated infections affect 5%-10% of all patients admitted toacutehospitalsandinvolveahighrateofmorbimortalityinadditiontoanincreaseincare-providing costs. Theexperience gainedover the courseof the last fewyears inSpain goes to show that the prevention and control of health care-associatedinfections is based on the following aspects: an adequate surveillance system,employingstandardsofcareofproveneffectivenessandtheappropriate,reasonableuseofantibiotics.
Likewise, this experience goes to show a need for an interdisciplinary effortincludingeverything from themanagementandadministrationof the centers to theprofessionalswhoperformtheirprofessionaldutiesinallfieldsofhealthcare.
Health care-associated infections are occasionally related to implantablebiomedicaldevices (catheters,woundvacs,prostheses, implants,etc.), the feasibilityand functionalityofwhich is seriouslycompromisedby infection.Themains typesofhealthcare-associated infectionsarerelatedto invasiveproceduressuchas: surgicalsite infection, catheter-related urinary infection, Central line-associated bloodstreaminfections(CLABSIs)andventilator-associatedpneumonia.

86
Employing specific multimodal strategies has shown itself to be useful inpreventing these infections, it therefore being necessary to continue promoting theprogramswhichhavebeengottenunderwayfortheircontrol.
Concerningreportingoutbreaksornewresistantpathogens,itisnecessarytopromoteearlytransmissionofinformation.
The process of combatting antimicrobial resistance must be approached byway of an effective, multifaceted, multidisciplinary strategy actively involving thedifferentsectorsandprofessionalsfromdifferentspecialties.
Specificobjectives:
1. MaintainandpromotetheexpansionoftheNHSHandHygieneprogramtoallmedicalservicescenters.
2. Maintain and promote the programs for the prevention health care-associated infections in critical patients and alos expanding them to otherareasofhospitalizationusingthesurveillanceandcontrolsystemsinplaceatthemedicalservicescenters.
3. PromoteaprogramforthepreventionandcontrolofsurgicalsiteinfectionattheNHSlevel.
4. Promote and implement programs for the rational, optimized use ofantimicrobialdrugs.
5. Promote the prevention and control of antimicrobial resistances, focusingspecial attention on the control of the diffusion of multiresistantmicroorganisms.
6. Favor multidisciplinary strategies for the early detection and treatment ofsepsis.
7. Promote programs for the prevention and control of infections within thesocialservicemedicalservicescentersetting.
8. Promotethesystemsforthesurveillanceofhealthcare-associatedinfectionsfor making the control of their evolution and the comparability of resultsamongcentersandservicespossible.
87
Recommendations:
• Maintain and consolidate the actions carried out for further enhancingadherence to hand hygiene by professionals and patients/caregivers, inhospitals,primarycareandsocialhealthcareservicesandnursinghomes.
• Carry out actions for the appropriate use of antiseptics anddisinfections atthemedicalservicescenters.
• Set out actions for the proper cleaning, disinfection and sterilization ofmedicalmaterial.
• CarryoutanationalprogramincollaborationwiththeHealthRegionsforthepreventionandcontrolofsurgicalsiteinfectioninselectedprocedures.
• MaintaintheprogramscarriedoutforpreventingandcontrollingCLABSIsandventilator-associatedpneumoniasoncriticalcareunitsaswellasdevelopingsimilar programs in other areas of hospitalization adapted to theircharacteristics.
• Carry out actions for preventing and controlling catheter-related urinaryinfectionsonunitsinvolvingaspecialrisk.
• Maintain and expand the existing programs for the prevention of infectionandtransmissionofmultiresistantmicroorganismtodifferentcare-providingunits,especiallytothosewhicharehigh-risk(criticalcare,dialysis,etc.).
• Carry out programs for optimizing antibiotics in keeping with the StrategyPlan for action for reducing the risk of selection and dissemination ofresistancestoantibiotics.
• Carry out programs for preventing and controlling peripherally-insertedvenouscatheter-associatedphlebitis.
• Setupspecialprogramsforcontrollingandpreventinghealthcare-associatedinfectionsatsocialservicesmedicalservicescentersandlivingfacilities.
• Get specific actions under way for the early detection and treatment ofpatients with sepsis/severe sepsis and septic shock taking into accountmultidisciplinaryinvolvement.
• Set up teams (multidisciplinary teams, as a priority) at themedical servicescenterswhicharespecialized inthesurveillanceandcontrolofhealthcare-
88
associated infections and which are in keeping with the NHS surveillanceprogramsguidelines.
Generalobjective2.3:Promotetheimplementationofsafepracticesinsurgery
The effective implementation of the safe surgery checklist requires specificmultimodal and multidisciplinary strategies which include this checklist beingappropriatelycompletedandusedfordetectingincidentsrevolvingaroundthesurgicalact.Thisisamatterofasimple,efficientandeffectivemeasureforfurtherenhancingpatient safety in the surgical procedure by facilitating full compliance with theuniversal protocol (right patient, right procedure, right site) and the prevention ofsurgical site infection. The safe surgery checklist transcends the simple safetyenhancement check and improves the communications and teamwork involved andshouldbecompletedinfullatleastinelectivesurgery.
Full compliance with the Helsinki Declaration on patient safety inAnesthesiologywould serveas a stimulus forpromoting theuseof the Safe SurgeryChecklistonbeingincludedunderSection4ofsaidDeclaration.
Specificobjectives:
1. PromotetheimplementationandcorrectuseoftheSafeSurgeryChecklist.
2. PromotetheadoptionoftherecommendationsoftheHelsinkiDeclarationonpatientsafetyinanesthesiology.
3. Promote the specific training in non-technical aspects (communication,teamwork,etc.)amongthesurgicalblockprofessionals.
4. Improve communication in the transfer of the patient from the operatingroomstorecoveryorintensivecareunit.
Recommendations:
• CarryoutactionsattheNHSmedicalservicescentersfortheimplementation,adaptation, appropriate use and evaluation of the Safe Surgery Checklist,bothinhospitalsurgeryandextrahospitalsurgery.
• Promote the marking of the surgical site as a routine practice as well asrecommendationstothepatientsinthisregard.
• Disseminate and implement the Helsinki Safety in Anesthesiarecommendations.

89
• Carryouttrainingactionsforthesurgicalblockprofessionalsinnon-technicalaspects(communication,teamwork,etc.).
• DevelopandimplementapatientstatuslistontransferfromoperatingroomtoRecoveryorintensivecareunit,especiallyinpatientswithseveresystemicdisease.
• Carry out measure for improving the prophylaxis of venousthromboembolism.
Generalobjective2.4:Promotetheimplementationofsafepracticesinpatientcare
Theobjectivessuggestedinthisregardhavenotasyetbeenfullyachievedtodate,thedegreetowhichachievedhavingvariedgreatlythroughoutthecountry.Allofthisentailstheneedofsystematicallypromotingproceduresfortheimplementationofsafepracticesofproveneffectivenessinthenursingcareprovidedforthepatients.
Specificobjectives
1. Foster individualizednursingcareplanssuitedtoeachpatient’sneedsbeingcarriedout.
2. Promote the inclusion of patient safety aspects in the care plan on thepatient’smedicalrecordandonthedischargereport.
Recommendations
• Develop a personalized care plan (in hospitalized patients or homecarepatients)whichaddressesat least the followingaspects relevant topatientsafety:
o Preventingfallsandrelatedinjuries
o Preventingpressureulcers
o Preventinghealthcare-associatedinfections
o Safetyinphysicallyrestrainingthosepatientswhosorequire
o Preventingmalnutritionanddehydration,especiallyinelderlypatients
o Preventingbroncho-aspiration
o Safelycaringforfrailpatients
o Preventingandcontrollingpaintheadultsandchildren,tendingtotheneedsandpreferencesofthepatientsandtheircaregivers

90
• Include actions in the care plan for informing the patients and caregiversregardingthecareprovidedandtherisksinvolved.
• Includeinthecareplanforthepatient’smedicalrecordanddischargereportthe evaluation of the patient’s risks due to their clinical situation and theimplementation of the care necessary for the prevention and treatmentthereof.
• Develop specific care plans which include the integral assessment of thepatientsinhomecare,restrainedpatientsandterminalpatients.
Generalobjective2.5:Promotesaferpatientidentification
Theshortcomingsinidentifyingpatientsentailriskswhichmayleadtoincorrectdiagnoses,testsbeingconductedorsurgicalproceduresbeingperformedormedicinesorhemoderivativesbeingadministeredtothewrongpatients.
Safe patient identification of all patients must be guaranteed by means ofappropriatemethodswhichmake it possible to confirm the patient’s identity everytimeaprocedureisperformed,especiallyifitisaninvasiveprocedure195.
Specificobjectives:
1. Promote the safepatient identificationof the right patient, right procedureandrightsite.
2. Promote safepatientidentificationofthepatientswhohavespecificrisks.
3. Assuresafepatientidentificationofbiologicalsamples,whicharedeterminingfactorsforthediagnosis.
4. Fosterthefail-safeidentificationofthepatient’sclinicaldocuments.
Recommendations:
• Developandimplementactionsfor safepatientidentification,including:
o Using at least two unique identifiers for the patient. Preferably usingautomatedmeansofidentification.
o Checking the patient’s identification for each procedure, especially forthosewhicharehigh-risk.
o Settingoutstandardizedsystemsforsafepatientidentificationandthoseentailingspecificrisks.
91
o Training the personnel in the appropriate procedure for identifyingpatientsandtheneedofverifying their identification,at least inviewofanyinterventioninvolvingarisk.
o Getting the patient/caregiver actively involved in the identificationprocess.
o Making an evaluation and conducting a follow-up on the identificationprocess.
• Assure the safe identification of newborns before they leave the deliveryroomandthatthisidentificationbemadeinthepresenceofthemotherorafamilymember,wheneverpossible.
• Check the identification of documents of of each patient during the care-providingprocess.
• Label thebiological samples and imaging tests at theexactpoint in timeatwhichtheyaretaken.
• Set out actions which assure traceability of both solid and liquid biologicalsamples,whetherornottheybereplaceable,whicharedeterminingfactorsforthediagnosis,fromtheveryoutsetofthesamplebeingtaken.
• Determine mechanisms at the hospital and ambulatory level of care, foridentifying unidentifiable patients and suitably distinguishing among thosewhohavesimilaridentifiers(samename,etc.).
Generalobjective2.6:Promotecommunicationamongprofessionals
In the course of the care-providing process, it must be assured that theinformationconveyedamongprofessionalsconcerningthepatient’sclinicalsituationisaccurate,adequateandisprovidedtotherightperson.
Conveying clinical information on patients, especially during the transition ofcare, isahigh-riskprocess inwhich thekeyelement involved iscommunication.Thebreakdowns in communication among professional comprise the factor most ofteninvolvedinsentineleventscauses196.
The standardizationof the communicatingprocedureduring thetransitionsofcare, minimizes the variability of the messages and favors the efficacy of thecommunication,contributingtoalloftheprofessionals involved inthetransferbeingawareofthepatient’soverallsituationandtheerrorsbeingreduced197.
92
Specificobjectives:
1. Promote standardized communication, bothwithin the units and during thetransitionofcareforguaranteeingsafe,continuedcareforthepatients.
Recommendations:
• Carry out actions for the implementation of structured communicatingtechniques.
• Setout actions for effective communicating in a timely fashionof alert andcritical values of diagnostic tests which may be lift-threatening for thepatient.
Generalobjective2.7:Promotethedesignanddevelopmentofstrategiesfordealingwithsevereadverseeventsathealthcarecenters
Whenanadverseeventoccurs,especiallywhenithascausedseriousharmtothe patient, the patients and their familymembers (first victims)must be providedwith support by the organization and must be furnished with the informationappropriate for the circumstances in question (open disclosure), as well as theconsequences and the actions to be carried out for providing a response to theirneeds. In turn, the health care professionals involved in an adverse event (secondvictims)mustbeabletorelyoninstitutionalsupportsoastobeabletoopenlyreportwhathashappenedandmustbefurnishedwithsupportfortheirintegrationintothecare-providingendeavorwithoutanyaftereffects.
Thehealthcareorganizationsshouldtakeaproactivepositionwhichisastepahead of the situations involving conflicts, availing of protocols and procedures foradequately responding to patients and professionals when a severe adverse eventoccurs, additionally taking into account actions for maintaining or restoring theorganization’s(thirdvictim)prestigeandtheconfidenceoftheorganization’susers.
Specificobjectives:
1. Promotestrategiesbeingcarriedoutformanagingsevereadverseeventsandsupportingthevictimsthereof.
2. Promote the training of the professionals for the purpose of being able toappropriatelycarryoutsaidstrategies.
93
Recommendations
• Setoutstrategiesfortheappropriatemanagementofsevereadverseeventswhichwillassure:
o Providing the patients and caregivers who have experienced a severeadverse event with timely, clear, sincere and fitting informationconcerningwhichhashappened,aswellasaplanforprovidingsupportfortheirneeds.
o Offering support to the health care professionals involved in a severeadverseevent.
o Appropriately managing the process of conveying information to theorganization and to the media for the purpose of restoring theconfidenceintheinstitution.
• Carry out training actions for the professionals and the managers of themedicalservicescentersconcerningaspectsofprovidingcareforthepatientsandprofessionalsinvolvedinsevereadverseevents.
General objective 2.8: Promote the safe use of ionizing radiation in clinicalprocedures
Thedevelopmentoftechnologiesemployingradiationinthefieldofmedicinehas given rise to some major improvements in the diagnosis and treatment ofdisorders involving a major benefit for patients. The use of these technologies hasbeenincreasingovertheyearsinsuchawaythatmedicalexposuresarecurrentlyoneof the sources of artificial radiation which contribute the most to the population’sexposure198.
Withinthiscontext, the internationalorganizationssuchastheWorldHealthOrganizationandtheInternationalAtomicEnergyAgency(IAEA)havepromotedPlansforActionfortheRadiologicalProtectionofPatientsinthehealthcaresector199,200.
Therefore, at the national level and on the basis of that which is set forthundertheFrameworkAgreementbetweentheMSSSIandtheNuclearSafetyCouncilconcerningcollaborationonthesubjectsofmedicalexposures, linesofpatientsafetyare proposed in this area for the purpose of promoting the safe, controlled use ofionizingradiationintheNHS.
94
The strategy lines further expandupon thatwhich is set out under the newEuropean Directive on Radiological Protection approved in 2013201, as well as thespecificnationalRegulations202,203,204,205.
The above additional reflect the pillars of the radiological protection ofpatients (aboveall, thosemosthighlyvulnerable, suchaspediatricpatients)and theheightening of awareness and adaptation, in conjunction with the auditing, whichwere agreed at the latest International Conference for Radiological Protection ofPatients206.
Specificobjectives
1. Promote actions for further enhancing the processes justifying the use ofionizingradiation,especiallyinpatientsunder18yearsofage.
2. Promote Patient Safety in the diagnostic and therapeutic proceduresinvolvingtheuseofionizingradiation.
3. Promotethedetectingandpreventionoftheadverseeventsduetoionizingradiation, especial in radiation therapy and in interventional radiologyprocedures.
Recommendations
• Carryoutactionsfortrainingandinformingtheprescribingphysicians intheuseofproceduresinvolvingionizingradiation,especiallyinpatientsunder18yearsofage.
• Set out protocols for conducting diagnostic tests and treatments involvingionizingradiation,especiallyinpatientsunder18yearsofage.
• Setoutprotocols,takingintoaccounttheALARAcriteriafortheoptimizingofradiological protections and the use of updated reference levels for theprocess of conducting diagnostic tests and treatments involving ionizingradiation,especiallyinpatientsunder18yearsofage.
• Make certain that Quality Assurance Programs are carried out in all thoseservicesworkingwith ionizing radiation, especially in the radiation therapyservices, which include risk analyses and management of the incidentsreported.
• Setoutprotocolstobefollowedbypatientswhohavebeengivenhighdosesofradiationininterventionalprocedures.
95
• Furnish patients with prior information concerning the risks related to theprocedureswhichemployionizingradiation.
• Set out and promote the dissemination of a guide as to indications forcorrectlyrequestingimagingdiagnostictesting.
• Favor the patient’s clinical documentation including information beingrecordedoneachoneoftheprocedureswhicharecarriedoutwithionizingradiation (dose received, activity and route for administration of radiologydrugs, description of the technique employed and distribution of doses inradiationtherapyandbrachytherapy).
• Periodicallyconductareviewtomakecertainthattheequipmentisinproperworking order so as to guarantee the least amount of ionizing radiationpossible in the diagnostic procedures, aswell as optimized distributions inradiationtherapy.
• Makecertainthattheincidentsrelatedtoradiationtherapyarereportedandproperlymanaged(attheveryleast,atthedepartmentallevel).
� Strategic line of action 3: Risk management andreportingandlearningsystemsThisriskmanagementisfocusedontheidentificationandanalysisofthehealth
care-associatedrisks,aswellascarryingoutplansforactionforpreventingtheserisksand informing the professionals concerning the achievements attained. This riskmanagementprovidessomehighlyusefultoolssuchastheRootCauseAnalysis,whichaffords the possibility of making an in-depth analysis of the patient safety-relatedincidents, especially the sentinel events, and of preventing these incidents fromrecurring.
Themedical services centersmust carry out specific strategies for the propermanagementofhealthcarerisks.
Thereportingsystemsaffordtheopportunityof learningfromtheexperiencesofothersforthepurposeofpreventingerrors.However,thefearandreticencesoftheprofessionals with regard to reporting these errors due to possible penalizingconsequenceshaveabearingonthequalityofthereportingsystemsandtheirbeingusedtothebestadvantage.
96
Generalobjective3.1:Promoteriskmanagementatthemedicalservicescenters
Specificobjectives:
1. Promote the creation of riskmanagement units at healthcare centerswhichwill carry out strategies for the propermanagement of health care-relatedrisks.
Recommendations:
• Setup(atthe individualcenterormanagement level) functionalhealthcareriskmanagementunitsorsimilarunitswhichassumetheseduties.
• Promote different methods for identifying safety-related risks (analysis ofcomplaints and suggestions, safety rounds, review of medical records,sessionsforlearningfrommistakesmade,epidemiologicalstudies,etc.).
• Promote the training of all of the professionals in themanagement of risksandintheuseoftheriskassessmenttoolsapplicabletotheirindividualfield.
• Carry out specific risk management actions, including taking a proactiveattitudeandtheuseofamethodologywhichwillmakeitpossibletoidentifyproblems, analyze their causes and carry out actionswhichwill prevent orreducetheirbeingrepeated.
• Makein-depth,systematizedanalysesofthesentineleventsidentifiedwhichsorequire.
Generalobjective3.2:Promotetheimplementationanddevelopmentofsystemsforreportinghealthcare-relatedincidentsforpurposesoflearning
Specificobjectives:
1. Promote the implementation and development, at healthcare centers, ofsystems for reporting health care-related incidents focused on lessonlearningandproblemsolvingatlocallevel.
2. Promote strategies being carried out for further enhancing and providingincentivesforincidentsbeingreportedatthemedicalservicescenters.
3. Fosteragile,timelyfeedbackfromtheinformationtotheprofessionalswhohave taken part in reporting incidents, as well as to the rest of theorganization.
4. Foster periodic publication of information related to the safety incidentsidentifiedintheNHS.
97
5. Promote the protection of the professionals taking part in the reportingsystemsfordisciplinaryorlegalproceedings.
Recommendations:
• Set up a system for reporting health care-related incidents at the medicalservicescentersorunitswhichdonotalreadyhavesuchasystem inplace,which will be voluntary, confidential and non-punitive and which willencouragelearning.
• Facilitatethosecenterswhichdohavethissysteminplacewiththeuseandsustainabilitythereofforthepurposeoffurtherenhancingthesafetyofthehealthcareprovided.
• Carryouttrainingactionsforalloftheprofessionalsfortheproperreportingofhealthcare-relatedincidents.
• Carry out actionswith themanagers and professionalswhichwill favor thereporting,analysisandmanagementof incidents related to thehealthcareprovided.
• Facilitatethereportingofincidentsbypatients/caregivers.
• Provide theclinicalprofessionalswith timely informationas to the incidentsidentifiedandtheactionstakenfortheirprevention.
• Furnish theclinicalprofessionalswith the informationon themost frequentsafety-related incidents in the NHS and the recommendations for theirprevention
• Promotefurtherexpansiononthefittingrulesandregulationsfocusingontheprotectionofthosereportingincidents.
98
� Strategic line of action 4: Patient and caregiverparticipationfortheirsafetyManyreticencesstillasyetexistbothonthepartofthemanagersandonthe
part of the professionalswhich are hindering patients being actively involved in thedecision-making process and citizen participation at the group level in health care-relateddecision-making.Thisparticipation isbasedontherightwhich individuals,ascitizens, have for taking part in the decisions affecting them and their freedom ofchoicewithinthehealthsystem.
Therearealsoculturalreticencesonthepartofthepatientspropertoadoptadifferentprofileandroleinthehealthcaredeliveryprocess.
Despite the above, it is indeed true that the role of patients is changing andthat this requires a major cultural change in the professional-patient relationshipbasedontheshareddecision-makingprocess.
Generalobjective4.1:Promotetheparticipationofthepatientsandtheircaregiversinpatientsafety
Specificobjectives:
1. Promote the patient/caregiver being furnished with complete, readilycomprehensible information concerning their care delivery process and therisks entailed, facilitating a shared decision-making process with theprofessional/teamprovidingthepatient’scare.
2. Promote the training of the patients/caregivers concerning the patient’sdisorder,thecarerequiredandtherisksentailedinthehealthcareprovidedandtheirprevention.
3. Promotetheactiveinvolvementofthepatients/caregiversinpatientsafety-relatedaspectsintheircontactswiththehealthsystem.
Recommendations:
• · Have patient receiving plan in place including clear, complete,comprehensible information on their rights and obligations, the healthservicesinwhichthecarewillbeprovided,therisksentailedinthecaretobeprovidedandthepatient’sinvolvementinthedecision-makingprocess.
99
• Foster specific training programs for patients/caregivers for the purpose ofachievingtheiractiveinvolvementinthedecision-makingandcare-providingprocesses.
• Carryoutactionsforstimulatingtheparticipationofthepatients/caregiversinpatient safety-related activities (joint patient and professional committees,patients’council,etc.).
• Allow and promote the presence of a companion for the patient, providedthatthisbepossible,inallofthehealthcaresettings,especiallyinthecaseofpediatricpatientsorthosepatientswhosecognitiveabilitiesarediminished.
• Assure the correct procedure in obtaining the informed consent of thepatients, above all in invasive procedures, as well as in the process ofrecording living wills, promoting practices which will help the patient toexecutealivingwillinaninformedmanner.
• Prepareguidelinesastohowtoprovidepatientswithcarequalityandpatientsafety-relatedinformation,fosteringthetransparencyoftheinformation.
• Carryouttrainingactionsforprofessionalsontechniquesforcommunicatingwiththepatients.

100
� Strategiclineofaction5:ResearchintopatientsafetyThe fields of research into patient safety should include aspects for further
enhancing the knowledge concerning: the magnitude and the characteristics of theclinical risk, the comprehension of the factors contributing to patient safety-relatedincidentsoccurring, the impactwhich theadverseeventshaveon thehealth systemand the identification of cost-effective, feasible, sustainable solutions for achievingsaferhealthcare.
General objective 5.1: Promote the further enhancement of the knowledge in thepreventoftheharmassociatedwithhealthcare
Specificobjectives:
1. Promote specific linesof research inpatient safetyatnationalandRegionallevel.
2. FosterthedisseminationofthefindingsofthepatientsafetyresearchtotheentireNHSandtothecitizenry.
Recommendations:
• Promoteresearchstudiesbeingcarriedoutwhichwillmakeitpossibleto:
o Quantify themagnitude and the characteristics of the clinical risk and therisktrends.
o Furtherenhancethecomprehensionofthefactorswhichcontributetotheoccurrenceofthepatientsafety-relatedincidents.
o Evaluate the economic impact which adverse events have on the healthsystem.
o Evaluate the impact, effectiveness and sustainability of the practices,proceduresandsolutionsimplementedforthepurposeoffurtherenhancingpatientsafety.
• Promote the identification and dissemination of cost-effective, feasible,sustainablesolutionsforachievingsaferhealthcareandpreventingincidentsharmfultothepatients.
• Favor the dissemination of the findings of the research studies conductedconcerningpatientsafety.

101
� Strategiclineofaction6:InternationalparticipationSpain has been taking active part in the activities carried out by the World
HealthOrganization’sPatientSafetyProgramsincetheProgramfirstbegan,aswellasinpatientsafety-orientedactionswiththePan-AmericanHealthOrganization.SpainisamemberofthetechnicalgroupsintheOrganizationforEconomicDevelopmentandCooperation,andintheEuropeanCommission..
Generalobjective6.1:Promoteinternationalcollaborationinpatientsafety
Specificobjectives:
1. Foster collaboration with the World Health Organization’s and the PanAmericanHealthOrganization’spatientsafetyProgram.
2. Promote Spanish participation in international forums related to patientsafety.
Recommendations:
• MaintainandbolsterthecollaborationwiththeWorldHealthOrganization’sandthePanAmericanHealthOrganization’sPatientSafetyProgram.
• Maintain and bolster the collaboration with the Member States and theEuropean Commission in working groups and joint actions within theframework of the EuropeanUnion’s care quality andpatient safety-relatedactions.
• Collaborate with other international organizations which carry our relevantactionsregardingpatientsafety.
102
3.EVALUATION
Fortheevaluationofthisstrategy,severalindicatorsandcriteriaarebeingagreedwiththe Health Regions and will be included in a separate document currently in theprocess,titled“Evaluationofthe2015-2020NationalHealthSystemSafetyStrategy”.

103
104
4.GLOSSARY
• Accreditation.Formalrecognitionoftheindependenceandtechnicalcapacityof a conformanceevaluationagency for carryingout itswork inaccordancewithinternationally-recognizedrequirements207.
• Adverseevent:Anincidentwhichcausesharmtothepatient213.
• HealthRegion.Territorialentitywhich,withintheconstitutionalbodyoflawoftheKingdomofSpain,isendowedwithlegislativeautonomyandexecutiveauthorities, as well as the power of administering themselves bymeans oftheirownrepresentatives211.
• Qualityofcare.Thedegreetowhichthehealthservicesfortheindividualsorthe population increase the possibility of achieving the desired results andare, at the same time, consistent with current scientific knowledge. Thehealthsystemmustseetofurtherenhancingthefollowingareasofthehealthcare provided: effectiveness, efficiency, accessibility, acceptability (patient-centeredcare),equityandsafety209.
• Error. This refers to the fact of not carrying out a planned action or ofemploying an incorrect plan. Errors can be either errors of commission, ifsomething is done wrong, or errors of omission, if the correct thing is notdone213.
• Safe patient identification.A procedure affording the possibility ofmakingcertainofthepatient’sidentifyduringthecare-providingprocessonthebasisoftheidentificationofdetailswhichpertainsolelytothepatientinquestionandcannotbesharedbyotherpatients195.
• Handhygiene.Ageneraltermforreferringtotheremovalofmicrooganismsbywayofdisinfectingagentssuchasalcoholorsoapandwater86.
• Harmless incident. An incident which the patient experiences but whichcausesnoappreciableharm213.
• Healthcare-associatedinfection.Aninfectionacquiredasaresultofahealthcareinterventioninanyhealthcaresetting(hospital,outpatientcaresetting,living facilities, etc.) and which was not present or being incubated at thepointintimeatwhichthecarewasprovided104.

105
• Health care-related harm. The harm which results from the plans ormeasures adopted during the process of providing health care or which isassociatedwiththesame213.
• High-riskmedications.Thosewhichhaveaverygreatprobabilityof causingsevereharmorevendeathwhenanerrorismadeinthecourseoftheiruse.This definition does not indicate that the errors associated with thesemedicationsaremorefrequent,butratherthatintheeventanerrorisindeedmade,theconsequencesforthepatientsareusuallymoresevere216.
• Medication error. An unintentional error in the process of prescribing,dispensingoradministeringamedicineunder thecontrolof thehealthcareprofessionalorofthecitizenwhotakesthemedicine214.
• Medication Reconciliation. A formal process consisting of obtaining acomplete, accurate list of the patient’s medication prior to admission tohospitalandcomparingittothemedicationprescribedforthatsamepatientat hospital admission, in the transfers and at discharge from hospital. Thediscrepanciesfoundmustbeappropriatelyrecordedandreportedtothenexthealthproviderandtothepatientl210.
• NationalHealthSystem.CoordinatedsetofthehealthservicesoftheCentralGovernment Administration and the health services of the Health Regionswhich integratesallof thehealthcarebenefitsand functionswhich,by law,aretheresponsibilityofthepublicpowers220.
• Nosocomialinfection.Aninfectionacquiredduringahospitalstaywhichwasnotpresentorintheincubationstageatthepointintimeatwhichthepatientwasinitiallyadmittedtohospital215.
• Patient participation. The process allowing the patients, their caregivers ortheperson towhom theydevolve their power to takepart in thedecisionsrelatedtotheirhealthconditionandinthepreventionofhealthcare-relatedharm, thus contributing to the organization’s learning by way of theirexperienceaspatients.
The term “public participation” is understood as the extension by way ofwhich thepatientsorcaregivers, throughtheir representativeorganizations,contributetoshapingthehealthsystembymeansoftheiractiveinvolvement

106
in the process of designing the health policies, the preparation of healthstrategiesandthegovernanceoftheinstitutions.64.
• Patientsafety.Reductionoftheriskofunnecessaryharmassociatedwiththeprocess of providing health care up to an acceptableminimum, taking intoaccount thecurrentknowledgeat thepoint in time, theavailable resourcesandthecontextinwhichthecareisprovided213.
• Reportingandlearningsystem.Asystemrequiringthecollectionofdataandanalysisconcerningallaspectsrelatedtotheprocessofprovidingcareforthepatient inwhich therehasbeenanunanticipatedcircumstancewhich couldhavecausedorhascausedthepatientunnecessaryharm,forthepurposeofpreventingitsreoccurrencebywayoflearning65.
• Patient safety-related incident.Aneventorcircumstancewhichhascausedorcouldhavecausedapatientunnecessaryharm213.
• Patient.Apersonwho requireshealth careand isplacedunder the careofprofessionals for maintaining and/or restoring his/her health or bringingsymptomsundercontrol217.
• Procedure.Structuredmethodfordoingsomethingorperformingatask218.
• Riskmanagement.Clinical,administrativeand industrialactivitieswhich theorganizationsemploywithaviewtoidentifying,evaluatingandreducingtheriskofharmtothepatients,thepersonnelandthevisitorsinadditiontotheriskoflossesfortheorganization213.
• Risk.Likelihoodofanincidentoccurring213.
• Safepractices.Interventions,strategiesorapproachesaimedatpreventingormitigating the unnecessary harm associated with the process of providingpatientswithhealthcareandfurtherenhancingtheirsafety86.
• Safesurgery.Setofrulestobefollowedduringthesurgicalprocedureforthepurpose of guaranteeing the patient’s safety in the prevention of adverseevents related to: surgical site infection, wrong site/wrong patient/wrongprocedure, the surgical equipment, the anesthesia and the use of themedicines45.
• Safety culture. An organization’s safety culture is the result of the values,attitudes, perceptions, skills and patterns of behavior of individuals and

107
groups which determine the commitment as well and the style and abilitythereof,withregardtothehealthoftheorganizationandthemanagementofsafety212.
• Sentinelevent.Anunanticipatedincidentinwhichdeathorseverephysicalormental harm or the risk of the same being caused occurs. Severe harmspecificallyincludesthelossofalimborafunction.Thephrase“ortheriskofthe same being caused” encompasses all variations of the process therepetition of which would entail a major probability of a severe adverseoutcome.Theseeventsareknownas“sentinel”eventsbecausetheyalerttotheneedofanimmediateattentionandresponse213.
• Specialized Care Activity Register-MinimumBasic Data Set (RAE-CMBD inSpanish):RoyalDecree69/2015ofFebruary6governingtheSpecializedCareActivityRegister(RAEinSpanish),basedonthecurrentMinimumBasicDataSet(MBDS).Thisincludesthestandardizedrecordingofanumberofvariablesrelatedtothepatientandtothecare-providingepisodeinquestion,includingthe diagnoses and the procedures. This register encompasses bothhospitalizationaswellasthehomecarehospitalization,medicaldayhospital,outpatient surgery, especially complex outpatient procedures and hospitalemergenciescare-providingmodalities219.

108

109
5.ABBREVIATIONS&ACRONYMS
AEMPS:SpanishMedicinesandMedicalProductsAgency
AHRQ:AgencyforHealthCareResearchandQuality
PC:PrimaryCare
CRB:Catheter-RelatedBacteremia
BURDEN:BurdenofResistanceandDiseaseinEuropeanNations
PCC:PrimaryCareCenter
ACs:HealthRegions
CHAFEA: European Commission and Consumers, Health, Agriculture and FoodExecutiveAgency
CISEM-AP:Reportingharmlesssafetyincidentsandmedicationerrorsinprimarycare
CISP:PopulationHealthResearchCenter.MBDS:MinimumBasicDataSet
MedRecon:MedicationReconciliation
AE:AdverseEvent
EARCAS:AdverseEventsatSocialservicesmedicalservicescentersandLivingfacilities
SYREC:SafetyandRiskintheCriticalPatient
EARS-Net:AntimicrobialResistanceInteractiveDatabase
ECDC:EuropeanCenterforDiseasePreventionandControl
ENEAS:NationalStudyonHospitalization-RelatedAdverseEvents
APEAS:StudyonAdverseEventsinPrimaryCare
EVADUR:AdverseEventsinEmergencyCare
FHC:Systemsforreportingandrecordingadverseevents
HELICS:HospitalinEuropeLinkforInfectionControlthroughSurveillance
HH:HandHygiene
HAIs:Infectionacquiredasaresultofahealthcareinterventioninanyhealthcaresetting(hospital,outpatientcare,livingfacilities,etc.)whichhadnotbecomeevidentorhadbeenincubatingatthepointintimeatwhichthecareisprovided(ECDC).
PATIden:PatientIdentification
110
IMPLEMENT:ImplementingStrategicBundlesforInfectionPrevention&Management
INGESA:NationalHealthcareManagementInstituteforCeutaandMelilla
CPI:ConsumerPriceIndex
IPSE:ImprovingPatientSafetyinEurope
UTI:UrinaryTractInfection
JC:JointCommission
SSC:Safesurgerychecklist
HRM:High-RiskMedications
MOSPS:MedicalOfficeSurveyOnPatientSafetyCulture
MRSA:Methicillin-ResistantStaphylococcusAureus
MSSSI:MinistryofHealth,SocialServicesandEquality
NQF:NationalQualityForum
VAP:Ventilator-AssociatedPneumonia
OECD:OrganizationforEconomicCooperationandDevelopment
WHO:WorldHealthOrganization
PaSQ:Jointactionforpatientsafetyandcarequality
ABP:Alcohol-BasedProduct
PROA:ProgramforOptimizationoftheUseofAntibioticsinHospitals
PROHIBIT:PreventionofHospitalInfectionsbyInterventionandTraining
AMR:AntimicrobialResistance
SEEIUC:SpanishSocietyforIntensiveCareNursingandCoronaryUnits
SEMICYUC: Spanish Society for Intensive Care Medicine, Critical Care and CoronaryCareUnits
SGIS:Safety-RelatedIncidentManagementSystem
SINASP:PatientSafety-RelatedReportingandLearningSystem
SINEA:IncidentandAdverseEventReportingSystem
SISNOT:HarmlessIncidentReportingSystem
SNASP:PatientSafety-RelatedReportingandLearningSystem
IncidentRS:IncidentReportingSystemforLearning
111
NHS:NationalHealthSystem
TPSC:PatientSafetyManagementPlatform
ICU:IntensiveCareUnit
FRMU:FunctionalRiskManagementUnit
PUs:Pressureulcers
SMU:SafeMedicationUse

112
6.LISTINGOFTABLESTable1.MainENEASStudydata..........................................................................................26
Table2.Spanishstudiesonthefrequencyofadverseeventsindifferenthealthcare-providingsettings.......................................................................................................29
Table3.Top-priorityrecommendationsforfurtherenhancingpatientsafetyinprimarycare.............................................................................................................................34
Table4.AreasforworkingonpatientsafetyproposedbytheCounciloftheEuropeanUnion..........................................................................................................................38
Table5.Safepracticesrecommendedbydifferentinternationalorganizations.................42
Table6.EuropeanUnionandECDCinitiativesforcombattingHAIsandRAMs...................47
Table7.Actionscarriedoutbydifferentorganizationforfacilitatingpatientparticipationfortheirsafety............................................................................................................52
Table8Frequencyoftheadverseeventsduetomedicationsinthemulticenterstudiesconductsatthenationallevel....................................................................................57
Table9.FindingsofstudiesconductedinSpainonmedicationerrorsandadverseeventsrelatedtomedications...............................................................................................58
Table10.Top-prioritysafepracticesrelatedtomedicationssuggestedbydifferentorganizationsanddegreetowhichimplementedinSpainaccordingtothestudiesconductedin2007(n=105hospitals)and2011(n=165hospitals)withthe“Self-AssessmentQuestionnaireonSafetyintheSystemforUseofMedicationsinHospitals”...................................................................................................................60
Table11.Patientsafetystrategyindicatorsforthe2010-2013timeframe........................76
Table12.Spain’sNHSHandHygieneprogramindicators....................................................78
Table13.PatientsafetycriteriaevaluatedintheauditoftheNHSteachinghospitals.......81
Table14.Resultsofthepatientsafetycriteriaevaluatedin2012intheauditsoftheNHSteachinghospitals.......................................................................................................82

113
7.LISTINGOFFIGURES
Fig.1.Listofstudiesconducted for thepurposeofascertainingthe incidenceofadverseeventsinhospitals......................................................................................................24
Fig.2.IncidentreportingsystemsdevelopedinSpain’sNHSandtheircharacteristics…….70
Fig.3.SafepracticesrecommendedinthepatientsafetystrategywhichareimplementedinspecializedcareintheNHS(includingthe17HealthRegionsandINGESA)...........73
Fig.4.Safepracticesrecommended inthepatientsafetystrategywhichare implementedin specialized care in the NHS (including the 17 Health Regions andINGESA)………………………………………………………………………………………………………………….74
Fig.5.Results of the evaluation of the patient safety indicators for the 2010-2013 timeframe..........................................................................................................................77
Fig.6.ResultsoftheevaluationoftheNHSHandHygieneindicators.................................79
Fig. 7. Evolution of the consumption of alcohol-based product in theNHS for the 2009-2013period................................................................................................................79

114
8.BIBLIOGRAPHY
1LeyGeneraldeSanidad.Ley14/1986de25deAbril.BoletínOficialdelEstado,nº102,(25-4-1986).2 Oficina de Planificación Sanitaria y Calidad. Desarrollo de la Estrategia Nacional en Seguridad delPaciente2005-2011. [Internet]Madrid:MinisteriodeSanidadyPolíticaSocial;AgenciadeCalidaddelSistema Nacional de Salud. Diciembre de 2011. [Acceso 19 febrero 2015] Disponible en:http://www.seguridaddelpaciente.es/resources/documentos/estrategia_sp_sns_2005_2011.pdf3AgenciadeCalidaddelSistemaNacionaldeSalud.PlandeCalidadparaelSistemaNacionaldeSalud2006.[Internet]Madrid:MinisteriodeSanidadyConsumo;AgenciadeCalidaddelSistemaNacionaldeSalud; 2006. [Acceso 19 febrero 2015]. Disponible en:http://www.msssi.gob.es/organizacion/sns/planCalidadSNS/pncalidad.htm)4KohnLT,CorriganJM,Donaldson.MSInstituteofMedicine.Toerrishuman:buildingasaferhealthsystem.Washington,DC:NationalAcademyPress;19995 World Health Organization. Patient Safety. World Alliance for Patient Safety. PatientSafety.[Internet].TheLaunchoftheWorldAllianceforPatientSafety,WashingtonDC,USA—27October2004[Accedido20febrero2015].Disponibleen:http://www.who.int/patientsafety/worldalliance/en/6 Council of Europe. Committee of Ministers. Recommendation Rec (2006)7 of the Committee ofMinisters to member states on management of patient safety and prevention of adverse events inhealthcare.[Internet]Brussels:CouncilofEurope;2006[acceso1deoctubrede2013].Disponibleen:https://wcd.coe.int/ViewDoc.jsp?id=10054397EuropeanComission.RecomendacionesdelConsejosobrelaseguridaddelospacientes,enparticularlaprevencióny luchacontra las infeccionesrelacionadascon laasistenciasanitaria.DiariodelConsejode laUniónEuropea9de juniode2009 (2009/C151/01). [Internet].Brussels: EuropeanCommission;2011. [Acceso 19 febrero 2015] Disponible en:http://ec.europa.eu/health/patientsafety/docs/council2009es.pdf8BrennanTA,LeapeLL,LairdNM,HerbetL,LocalioAR,LawthersAGetal.Incidenceofadverseeventsandnegligence inhospitalizedpatients: resultsof theHarvardMedicalPracticeStudy I.NEngl JMed1991;324:370-3769BrennanTA,LeapeLL,LairdNM,HerbetL,LocalioAR,LawthersAGetal.Incidenceofadverseeventsandnegligence inhospitalizedpatients: resultsof theHarvardMedicalPracticeStudy II.NEngl JMed1991;324:377-38410WilsonRM,RuncimanWB,GibberdRW,HarrisonBT,NewbyL,HamiltonJD.TheQualityinAustralianHealthCareStudy.MedJAust1995;163(9):458-711 Davis P, Lay-Yee R, Schug S, Briant R, Scott A, Johnson S, et al. Adverse events regional feasibilitystudy:indicativefindings.NZMedJ.2001;114(1131):203-512VincentC,NealeG,WoloshynowychM.AdverseeventsinBritishhospitals:preliminaryretrospectiverecordreview.BMJ2001;322:517-51913 Schiøler T, Lipczak H, Pedersen BL, Mogensen TS, Bech KB, Stockmarr A, Svenning AR, Frølich A.Incidence of adverse events in hospitals. A retrospective study of medical records. Ugeskr Laeger.2001;163(39):5370-8

115
14ForsterAJ,AsmisTR,ClarkHD,AlSaiedG,CodeCC,CaugheySCetal.OttawaHospitalPatientSafetyStudy:incidenceandtimingofadverseeventsinpatientsadmittedtoaCanadianteachinghospital.CanMedAssoc.J2004;170(8):1235-15 Estudio nacional sobre los efectos adversos ligados a la hospitalización: ENEAS 2005. [Internet]Madrid: 2006. Ministerio de Sanidad y Consumo. [Accedido 19 febrero 2015] Disponible en:http://www.seguridaddelpaciente.es/resources/contenidos/castellano/2006/ENEAS.pdf16 Michel P, Quenon Jl, Djihoud A, Tricaud-Vialle S, de Sarasqueta AM. French national survey ofinpatientadverseeventsprospectivelyassessedwithwardstaff.QualSafHealthCare2007;16:369–377.doi:10.1136/qshc.2005.01696417ZegersM,deBruijneMC,WagnerC,HoonhoutLH,WaaijmanR,SmitsM,etal.AdverseeventsandpotentiallypreventabledeathsinDutchhospitals:resultsofaretrospectivepatientrecordreviewstudy.QualSafHealthCare.2009;18(4):297-302.doi:10.1136/qshc.2007.02592418 Soop M, Fryksmark U, Köster M, et al. The incidence of adverse events in Swedish hospitals: aretrospectivemedicalrecordreviewstudy.IntJQualHealthCare.2009Aug;21(4):285–291.19 Mendes W, Martins M, Rozenfeld S, Travassos C. The assessment of adverse events in Brazilianhospitals.IntJQualHealthCare2009;21(4):279-284.20 Letaief M1, El Mhamdi S, El-Asady R, et al. Adverse events in a Tunisian hospital: results of aretrospectivecohortstudy.IntJQualHealthCare.2010Oct;22(5):380-521deVriesEN,RamrattanMA,SmorenburgSM,GoumaDJ,BoermeesterMA.Theincidenceandnatureof in-hospital adverse events: a systematic review. Qual Saf Health Care. 2008;17(3):216-23. PMID:1851962922FosterAJ,MurffHJ,PetersonJF,GandhiTK,BatesDW.Theincidenceandseverityofadverseeventsaffectingpatientsafterdischargefromhospital.AnnInterMed.2003;138(3):161-16723 ClassenDC,ResarR,Griffin F, Federico F, Frankel T, KimmelN,Whittington JC, FrankelA, SegerA,James BC. Global trigger tool' shows that adverse events in hospitalsmay be ten times greater thanpreviouslymeasured.HealthAff(Millwood).2011Apr;30(4):581-924WorldHealthOrganizationEurope.AbriefsynopsisonPatientsafety.[Internet]WHORegionalOfficefor Europe. Copenhagen, 2010. [Accedido 20 febrero 2015] Disponible en: http://www.euro.who.int/data/assets/pdffile/0015/111507/E93833.pdf25 OECD. Health policies and data. [Internet].OECD. Health care quality indicators-Patient Safety.[Accedido 19 febrero 2015]. Disponible en: http://www.oecd.org/els/health-systems/hcqi-patient-safety.htm
26Estudio-APEAS.Estudiosobrelaseguridaddelospacientesenatenciónprimariadesalud.[Internet].Madrid: Agencia de Calidad del Sistema Nacional de Salud; Informes, Estudios e Investigación 2008.[Accedido 20 febrero 2015] Disponible en:http://www.seguridaddelpaciente.es/resources/contenidos/castellano/2008/APEAS.pdf27Eventosadversosenresidenciasycentrosasistencialessociosanitarios.[Internet].Madrid:AgenciadeCalidad del Sistema Nacional de Salud; Informes, Estudios e Investigación 2011. [Accedido 1 febrero2015]Disponibleen:http://www.seguridaddelpaciente.es/resources/documentos/earcas.pdf28SYREC.Incidentesyeventosadversosenmedicinaintensiva.Seguridadyriesgoenelenfermocrítico2007. Informe Mayo 2009. [Internet]. Madrid: Agencia de Calidad del Sistema Nacional de Salud;

116
Informes, Estudios E Investigación 2010. [Accedido 20 febrero 2015] Disponible en:http://www.seguridaddelpaciente.es/es/proyectos/financiacion-estudios/e-epidemiologicos/2008/29TomásS,ChanovasM,RoquetaF,AlcarazJ,ToranzoJyGrupodeTrabajoEVADUR-SEMES.EVADUR:eventosadversosligadosalaasistenciaenlosserviciosdeurgenciasdehospitalesespañoles.[Internet]Emergencias 2010; 22: 415-428. [Accedido 20 febrero 2015] Disponible en:http://www.semes.org/revista_EMERGENCIAS/buscar/titulo/EVADUR%3A+eventos+adversos+ligados+a+la+asistencia+en+los+servicios+de+urgencias+de+hospitales+espa%C3%B1oles/.30 Aranaz JM, Aibar C, Vitaller J, Ruiz-López P, Limón-Ramírez R, Terol-García E and the ENEAS workgroup.IncidenceofadverseeventsrelatedtohealthcareinSpain:resultsoftheSpanishNationalStudyofAdverseEvents.JournalofEpidemiologyandCommunityHealth.2008;62(12):1022-931 Aranaz J. Limon R,Mira J, Aibar-Remón C.Whatmakes hospitalized patientsmore vulnerable andincreasestheirriskofexperiencinganadverseevent?IntJQualityHealthCare.2011:23(6):705-71232Aranaz J,AibarC,Vitaller J,Requena J,TerolE,KelleyE,GeaAandENEASworkgroup. Impactandpreventability of adverse events in Spanish public hospitals: results of the Spanish National Study ofAdverseEvents(ENEAS).InternationalJournalforQualityinHealthCare.2009;21:408-41433 Aibar-Remón C, Aranaz-Andrés JM Vitaller-Burillo J, Agra-Varela Y, Giménez-Júlvez T,Marcos-CalvoMP. Seguridaddel pacienteenatenciónprimariade salud:magnituddel problema. [Internet]RevistaClínicaElectronicaenAtenciónPrimaria,2003-ISSN1887-4215[Accedido20febrero2015]Disponibleenhttp://www.fbjoseplaporte.org/rceap/sumario2.php?idnum=1834Aranaz J,AibarC, LimónR,Mira JJ,Vitaller J,AgraY, TerolE.A studyof theprevalenceofadverseeventsinprimaryhealthcareinSpain.EurJPublicHealth.2012;22(6):921-92535MerinoP,ÁlvarezJ,MartínC,AlonsoA,GutiérrezI.AdverseeventsinSpanishintensivecareunits:theSYRECstudy.IntJQualHealthCare2012;24(2):105-113.doi:10.1093/intqhc/mzr08336 Special Eurobarometer 411. Patient Safety andQuality of Care. [Monografía en Internet]. Brussels:Directorate-General for Health and Consumers. European Commission; 2014. [Accedido 18 febrero2015].Disponibleen:http://ec.europa.eu/publicopinion/archives/ebs/ebs411en.pdf37 Instituto de Información Sanitaria. Barómetro Sanitario 2010 [Publicación en Internet]. Madrid:Ministerio de Sanidad, Política Social e Igualdad, 2010. [Accedido 20 febrero 2015] Disponible en:http://www.mspsi.gob.es/estadEstudios/estadisticas/sisInfSanSNS/informeAnual.htm38MittmannN,KooM,DanemanN,McDOnaldN,BakerM;MatlowAetal. Theeconomicburdenofpatientsafetytargets inacutecare:asystematicreview. [Internet].DrugHealthcPatientSaf.2012;4:141–165. [Accedido 20 febrero 2015][Publicado online 5 octubre 2012] Disponible en:http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3476359/. doi: 10.2147/DHPS.S33288; PMCID:PMC347635939AntoñanzasF.Aproximaciónaloscostesdelanoseguridadenelsistemanacionaldesalud.RevEspSaludPública2013,Vol.87,nº340MinisteriodeSanidadyConsumo.RevisiónBibliográficasobretrabajosdecostesdela“noseguridaddelpaciente”.SerieInformes,EstudioseInvestigación2008.[Internet]Madrid:MinisteriodeSanidadyConsumo; 2008. [Accedido 20 febrero 2015] Disponible en:http://www.seguridaddelpaciente.es/resources/contenidos/castellano/2008/CostesNoSeguridadPacientes.pdf
117
41 Allué N, Chiarello P, Bernal E, Castells X, Giraldo P, Martínez C, et al. Impacto económico de loseventosadversosenloshospitalesespañolesapartirdelConjuntoMínimoBásicodeDatos.[Internet]Barcelona: Gac Sanit 2014 28(1) [Accedido 20 febrero 2015] Disponible en:http://scielo.isciii.es/scielo.php?pid=S0213-91112014000100009&script=sciarttext42ShekellePG,WachterRM,PronovostPJ,SchoellesK,McDonaldKM,DySM,etal.MakingHealthCareSafer II: AnUpdatedCriticalAnalysis of the Evidence for Patient SafetyPractices. [Internet]Rockville,2013. MD:. Agency for Health care Research and Quality. [Internet] [Accedido 20 febrero 2015]Disponible en: http://www.ahrq.gov/research/findings/evidence-based-reports/services/quality/ptsafetyII-full.pdf43AranazJM,AgraY.Laculturadeseguridaddelpaciente:delpasadoalfuturoencuatrotiempos.MedClin(Barc)2010:135(Supl1):1-2.44World HealthOrganization Clean care is Safer care. [Sedeweb]. [Accedido 20 febrero 2015] CleanCareisSaferCarehttp://www.who.int/gpsc/5may/en/index.html45 World Health Organization. Patient Safety. [Sede web]. [Accedido 20 febrero 2015].http://www.who.int/patientsafety/safesurgery/en/index.html46. World Health Organization The evolving threat of antimicrobial resistance - Options for action.[Internet]. [Accedido 20 febrero 2015] Patient safety.http://www.who.int/patientsafety/implementation/amr/publication/en/47WorldHealthOrganizationDraftglobalactionplanonantimicrobialresistance[Internet]..WHO;2015.[Accedido 20 febrero 2015] Drug resistance Disponible en:http://www.who.int/drugresistance/globalactionplan/en/48WorldHealthOrganization Patients for patient safety. [Internet]. Patient safety [Accedido el 10 dejuliode2014]..Disponibleen:http://www.who.int/patientsafety/patientsforpatient/en/index.html49 World Health Organization From information to action. Reporting and learning for patient safety.[Internet]. Patient safety [Accedido 20 febrero 2015] Disponible en:http://www.who.int/patientsafety/implementation/reportingandlearning/en/50CresswellKM,PanesarSS,SalvillaSA,Carson-StevensA,LarizgoitiaI,DonaldsonLJ,etal.onbehalfofthe World Health Organization’s (WHO) Safer Primary Care Expert Working Group. Global ResearchPrioritiestoBetterUnderstandtheBurdenofIatrogenicHarminPrimaryCare:AnInternationalDelphiExercise.[Internet]PLOSMedicine.2013;10(11);e1001554.[Accedido20febrero2015]Disponibleen:http://www.who.int/patientsafety/primary-care-prioirties.pdf51 World Health Organization.. Action on Patient Safety - High 5s WHO. [Internet] Patient safety[Accedido 20 febrero 2015] Disponibleen:http://www.who.int/patientsafety/implementation/solutions/high5s/en/52 World Health Organization. Safer Primary Care [Internet].Patient Safety [Accedido 20 febrero2015Disponibleen:http://www.who.int/patientsafety/saferprimarycare/en/53 Aranaz-Andrés JM,Aibar-RemónC, Limón-Ramírez R, AmarillaA, Restrepo FR,UrrozO et al; IBEASteam. Prevalence of adverse events in the hospitals of five Latin American countries: results of the'IberoamericanStudyofAdverseEvents'(IBEAS).BMJQualSaf.2011Dec;20(12):1043-5154 Estudio IBEAS. Prevalencia de efectos adversos en hospitales de Latinoamérica. [Internet]Madrid:2010. Ministerio de Sanidad y Consumo. [Accedido 19 marzo 2015] Disponible en:http://www.seguridaddelpaciente.es/es/proyectos/financiacion-estudios/e-epidemiologicos/2007/
118
55 Organización Panamericana de la Salud. Sistemas de notificación de incidentes en América Latina.[Internet] Washington, DC: OPS, 2013. Calidad en Atención y Seguridad del Paciente. [Accedido 20febrero 2015] Disponible:http://www.paho.org/hq/index.php?option=com_content&view=category&layout=blog&id=1530&Itemid=1557&lang=es56Montserrat-CapellaD,SuárezM,OrtizL,MiraJJ,DuarteHG,ReveizL;AMBEASGroup.FrequencyofambulatorycareadverseeventsinLatinAmericancountries:theAMBEAS/PAHOcohortstudy.IntJQualHealthCare.2015Feb;27(1):52-9.57OrganizaciónPanamericanadelaSalud.Políticayestrategiaregionalesparalagarantíadelacalidaddelaatenciónsanitaria,incluyendolaseguridaddelpaciente.27.aConferenciaSanitariaPanamericana.59.aSesióndelComitéRegional.ResoluciónCSP27.r10.Washington,D.C,2007.58 Dirección De Empleo, Trabajo y Asuntos Sociales. Comité De Salud. Proyecto De Indicadores DeCalidad De Atención Sanitaria. Patient Safety Data Systems In The OECD: a report of a joint IrishDepartment of Health. [Internet] En: OECD Conference. OCDE DELSA/HEA/HCQ. 2007. [Accedido 20febrero 2015] Disponible en:http://www.msssi.gob.es/organizacion/sns/planCalidadSNS/pdf/excelencia/indicadorescalidadatencionsanitaria.pdf59 OECD. Health at a Glance 2013: OECD Indicators. [Internet] OECD Publishing; 2013 [Accedido 20febrero 2015] Disponible en: http://dx.doi.org/10.1787/health_glance-2013-en.http://www.oecd.org/els/health-systems/Health-at-a-Glance-2013.pdf60 Ministerio de Sanidad y Consumo. Validación de indicadores de calidad utilizados en el contextointernacional: indicadoresdeseguridaddepacienteseindicadoresdehospitalizaciónevitable.Madrid:MinisteriodeSanidadyConsumo;200861 Council of Europe. Committee of Ministers. Recommendation Rec (2006)7 of the Committee ofMinisters to member states on management of patient safety and prevention of adverse events inhealthcare.[Internet]Brussels:CouncilofEurope;2006[acceso1deoctubrede2013].Disponibleen:https://wcd.coe.int/ViewDoc.jsp?id=100543962Consolidatedversionof thetreatyonthe functioningof theEuropeanUnion.Official Journalof theEuropeanUnion,C115/47,9May2008.[Internet][Accedido31enero2015]Disponibleen:http://eur-lex.europa.eu/legal-content/ES/TXT/PDF/?uri=OJ:C:2008:115:FULL&from=EN63 European Commission. DG Health and Consumer Protection. Patient safety – Making it Happen!Luxembourg declaration on patient safety, 5 April 2005. [Internet] [Accedido 20 febrero 2015]Disponibleen:http://ec.europa.eu/health/phoverview/Documents/ev20050405rd01en.pdf64EuropeanCommision.PublicHealth.PatientSafety[Internet][Accedido20febrero2015]Disponible:http://ec.europa.eu/health/patient_safety/policy/index_en.htm65 European Patients Forum. EUNetPaS. 2014. [Internet] [Accedido 20 febrero 2015] Disponible en:http://www.eu-patient.eu/whatwedo/Projects/EUNetPaS/66EuropeanUnionNetworkforPatientSafetyandQualityofCare[sedeWeb]PaSQ;2011[acceso8dediciembrede2013].Disponibleen:http://www.pasq.eu/67EuropeanCommission.ReportFromTheCommissionToTheCouncilonthebasisofMemberStates'reports on the implementation of the Council Recommendation (2009/C 151/01) on patient safety,includingthepreventionandcontrolofhealthcareassociatedinfections.[Internet]Brussels:European

119
Commission. 2012. [Accedido 20 febrero 2015] Disponible en:http://ec.europa.eu/health/patientsafety/docs/council2009reporten.pdf68EuropeanCommission.ReportFromTheCommissionToTheCouncilTheCommission’sSecondReportto the Council on the implementation of Council Recommendation 2009/C 151/01 on patient safety,includingthepreventionandcontrolofhealthcareassociatedinfections.[Internet]Brussels:EuropeanCommission. 2014. [Accedido 20 febrero 2015] Disponible en: http://ec.europa.eu/health/patientsafety/docs/ec2ndreportpsimplementationen.pdf69Directiva2011/24/UEdelParlamentoEuropeoydelConsejorelativaalaaplicacióndelosderechosdelospacientesenlaasistenciasanitariatransfronteriza.DiarioOficialdelaUniónEuropea.L88/45.4deAbril 2011 9 demarzo de 2011. [Internet] [Accedido 20 febrero de 2015]. Disponible en: http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2011:088:0045:0065:es:PDF70 Patient Safety and Quality of Care Working Group. European Commission. Key findings andrecommendations on Education and training in Patient Safety across Europe. [Internet] EuropeanCommission 2014. [Accedido 31 enero 2015] Disponible en: http://ec.europa.eu/health/patientsafety/docs/guidelinespsqcwgeducationtrainingen.pdf71Reportingand learningsubgroupof theEuropeanCommissionPSQCWG.EuropeanCommissionKeyfindings and recommendations on Reporting and learning systems for patient safety incidents acrossEurope. [Internet] European Commission. 2014. Disponible en: http://ec.europa.eu/health/patientsafety/docs/guidelinespsqcwgreportinglearningsystemsen.pdf72RealDecreto81/2014,de7defebrero,porelqueseestablecennormasparagarantizarlaasistenciasanitariatransfronteriza,yporelquesemodificaelRealDecreto1718/2010,de17dediciembre,sobrereceta médica y órdenes de dispensación. [Internet] BOE: sábado 8 de febrero de 2014 Sec. I. Pág.10915.Disponibleen:http://www.boe.es/boe/dias/2014/02/08/pdfs/BOE-A-2014-1331.pdf73DiarioOficialdelaUniónEuropea.Decisióndelegadadelacomisiónde10demarzode2014porlaqueseestablecenloscriteriosylascondicionesquelasredeseuropeasdereferenciaylosprestadoresdeasistencia sanitariaquedeseen ingresaren las redeseuropeasde referenciadebencumplir (Textopertinente a efectos del EEE) (2014/286/UE). [Internet] Diario Oficial de la Unión Europea L 147/71[Accedidoel3marzo2015]Disponibleen:http://ec.europa.eu/health/ern/docs/erndelegateddecision20140310es.pdf74DiarioOficialdelaUniónEuropea.Decisióndeejecucióndelacomisiónde10demarzode2014porlaque se fijan los criterios para la creación y evaluación de las redes europeas de referencia y de susmiembros, y se facilita el intercambio de información y conocimientos en materia de creación yevaluacióndetalesredes.(TextopertinenteaefectosdelEEE)(2014/287/UE.[Internet]DiarioOficialdela Unión Europea L 147/79. [Accedido el 3 marzo 2015] Disponible en:http://ec.europa.eu/health/ern/docs/ern_implementingdecision_20140310_es.pdf75 Diario Oficial de la Unión Europea. Conclusiones del Consejo sobre seguridad de los pacientes ycalidad asistencial, en particular la prevención y la lucha contra las infecciones relacionadas con laasistencia sanitaria y la resistencia bacteriana (2014/C 438/05) [Internet] Diario Oficial de la UniónEuropea C 438/7 [Accedido el 3 marzo 2015] Disponible en: http://eur-lex.europa.eu/legal-content/ES/TXT/?uri=uriserv:OJ.C_.2014.438.01.0007.01.SPA76 Flin R, Mearns K, O’Connor P and Bryden R. Measuring safety climate: identifying the commonfeatures.[Internet]SafetyScience,Vol34(1-3),Feb2000,177-192.
120
77 Improving patient and worker safety. Oppotunities for sinergy, collaboration and innovation.[Internet] Joint Comission, 2012. [Accedido 25 enero 2015] Disponible en:http://www.jointcommission.org/assets/1/18/tjc-improvingpatientandworkersafety-monograph.pdf78El-JardaliF,etal.Predictorsandoutcomesofpatientsafetycultureinhospitals.BMCHealthServRes.2011;24;11-4579CartheyJ,ClarkeJ.ImplementingHumanfactorsinhealthcare;[Internet]PatientSafetyFirst.HowtoGuide 2015. [Accedido 20 febrero 2015] Disponible enhttp://www.patientsafetyfirst.nhs.uk/Content.aspx?path=/interventions/humanfactors/80 Cathpole K. Spreading human factors expertise in health care: untangling the knots in people andsystems.QualityandSafetyinHealthCare2013;0:1–5.doi:10.1136/bmjqs-2013-00203681 Human Factors in Patient Safety Review of Topics and Tools. Report for Methods and Measures.[Internet]WorkingGroupofWHOPatientSafety.WHO2009;[Accedido4febrero2015]Disponibleen:http://www.who.int/patientsafety/research/methods measures/human factors/human factorsreview.pdf82GursesAP,OzokAA,PronovostPJ.Timetoacelérateintegrationofhumanfactorsandergonomicsinpatientsafety.BMJQualSaf;2012:21(4):347-51)83 Carayon et al. Systems Engineering Initiative for Patient Safety (SEIPS) model of work system andpatient safety. [Internet] Qual Saf Health Care 2006;15:i50-i58. doi:10.1136/qshc.2005.015842[Accedido23enero2015]Disponibleen:http://qualitysafety.bmj.com/content/15/suppl_1/i50.short84 World Health Organization. Multi-professional Patient Safety Curriculum Guide. [Internet] PatientSafety. World Health Organization; 2011. [Accedido 20 febrero 2015] Disponible en:http://www.who.int/patientsafety/education/curriculum/tools-download/en/#85AgencyforHealthcareResearchandQuality(AHRQ).MakingHealthCareSafer:ACriticalAnalysisofPatientSafetyPractices. [Internet]AHRQ. July,2001 [Accedidoel6demayode2014].Disponibleen:http://archive.ahrq.gov/clinic/tp/ptsaftp.htm86AgencyforHealthcareResearchandQuality(AHRQ).[SedeWeb]U.S.DepartmentofHealth&HumanServices[Accedido20febrero2015]Disponibleen:http://www.ahrq.gov/87 National Quality Forum (NQF). Safe Practices for Better Health care—2010 Update: A ConsensusReport. [Internet] Washington, DC: National Quality Forum; 2010 [Accedido: 20 febrero 2015]Disponible en: https://www.qualityforum.org/Publications/2010/04/Safe_Practices_for_Better_Healthcare_%E2%80%93_2010_Update.aspx88 Joint Commission on Accreditation of Health care Organization. National Patient Safety Goals.[Internet] Joint Commission; 2015. [Accedido 20 febrero 2015] Disponible en:http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals89WorldHealthOrganization.WorldAllianceforPatientSafety.[Internet]PatientSafetySolutions,2007.[Accedido 20 febrero 2015] Disponible enhttp://www.who.int/mediacentre/news/discharges/2007/pr22/en/90 Aspden P, Wolcott JA, Lyle Bootman J, Cronenwett LR, editors. Preventing medication errors.Committee on Identifying and Preventing Medication Errors. Washington, DC: Institute of Medicine.NationalAcademyPress;2007
121
91ExpertGrouponSafeMedicationPractices.CreationofabettermedicationsafetycultureinEurope:Buildingupsafemedicationpractices.Strasbourg:CouncilofEurope;2006.92 European Medicines Agency. Medication-errors workshop. Workshop report. [Internet] EuropeanMedicines Agency London:; 2013. [Accedido 20 febrero 2015] Disponible enhttp://www.ema.europa.eu/ema/index.jsp?curl=pages/newsandevents/events/2012/10/eventdetail_000666.jsp&mid=WC0b01ac058004d5c393 Directiva 2010/84/UE del Parlamento Europeo y del Consejo de 15 de diciembre de 2010, quemodifica,enloquerespectaalafarmacovigilancia, laDirectiva2001/83/CEporlaqueseestableceuncódigo comunitario sobre medicamentos para uso humano. [Internet] [Accedido 20 febrero 2015]Disponibleenhttp://ec.europa.eu/health/files/eudralex/vol-1/dir201084/dir201084es.pdf94 World Health Organization. Report on the Burden of Endemic Health Care-Associated InfectionWorldwide. [Internet] [Accedido20 febrero 2015] World Health Organization; 2011. Disponible en:http://www.who.int/gpsc/countrywork/burdenhcai/en/95WorldHealthOrganization.Theglobalburdenofhealthcare-associatedinfections.Inauguralinfectioncontrol webinar series. World Health Organization; 2010 [Internet] [Accedido 20 febrero 2015]Disponibleen:http://www.who.int/entity/gpsc/5may/media/infectioncontrolwebinar19012010.pdf96 Pittet D, Hugonnet S, Harbarth S, Mourouga P, Sauvan V, Touveneau S, et al. Effectiveness of ahospital-wide programme to improve compliance with hand hygiene. Infection ControlProgramme.[Internet]Lancet.2000;356:1307-12.Erratumin:Lancet2000;356(9248):2196[Accedido20febrero 2015] Disponible en: http://www.ncbi.nlm.nih.gov/pubmed/11073019 PMID: 11073019[PubMed-indexedforMEDLINE]97StoneSPetal.EvaluationofthenationalcleanyourhandsCampaigntoreduceStaphylococcusAureusbacteraemiaandClostridiumdifficileinfectionInhospitals.BMJ2012;344:e300598Kirklandetal.Impactofahospital-widehandhygieneinitiativeonhealthcare-associatedinfections:resultsofaninterruptedtimeseries.BMJQualSaf201399HELICSSurgicalSiteInfectionsStatisticalReport.[Internet].EuropeanCommission/DGSANCO,March2006. [Accedido 20 febrero 2015] Disponible en:http://whqlibdoc.who.int/hq/2009/WHOHSEEPR2009.1eng.pdf100TheIPSEReport2005-2008ImprovingPatientSafety inEurope.[Internet]Projectcommissionedbythe EC/DG SANCO Project n° 790903. 2009. [Accedido 20 febrero 2015]Disponible enhttp://www.ecdc.europa.eu/en/activities/surveillance/HAI/Documents/0811 IPSE TechnicalImplementationReport.pdf101 European Commission Research & Innovation – Health. Burden of Resistance and Disease inEuropean Nations [Internet] [Actualizado 01/03/2012; accedido 20 febrero 2015]https://ec.europa.eu/research/health/infectious-diseases/antimicrobial-drug-resistance/projects/023en.html102 ImplementingStrategicBundles for InfectionPrevention&Management (IMPLEMENT). [Sitioweb][Accedido20febrero2015]Disponibleenhttp://www.eu-implement.info/103 PreventionofHospital Infectionsby Intervention andTraining. PROHIBIT. [Sitioweb] [Accedido20febrero2015]Disponibleen:https://plone.unige.ch/prohibit/104EuropeanCentre forDiseasePreventionandControl (ECDC) [Sitioweb]Accedido20 febrero2015]Disponibleenhttp://www.ecdc.europa.eu/en/Pages/home.aspx
122
105 Transatlantic Taskforce on Antimicrobial Resistance – TATFAR [Sitio web] European Centre forDisease Prevention and Control (ECDC) 2005 – 2015 [Accedido 20 febrero 2015] Disponible en:http://ecdc.europa.eu/en/activities/diseaseprogrammes/TATFAR/Pages/index.aspx106 European Centre for Disease Prevention and Control (ECDC) SURVEILLANCE REPORT. Pointprevalencesurveyofhealthcare-associatedinfectionsandantimicrobialuseinEuropeanlong-termcarefacilities. [Internet] April-May 2013. [Accedido 20 febrero 2015] Disponible en:http://www.ecdc.europa.eu/en/publications/Publications/health care-associated-infections-point-prevalence-survey-long-term-care-facilities-2013.pdf107 European Centre for Disease Prevention and Control. Surveillance [Sitio web] [accedido el 12 deenerode2015]Dsiponibleen:http://www.ecdc.europa.eu/en/activities/surveillance/Pages/index.aspx108WorldHealthOrganization.WHOGuidelinesforSafeSurgery2009.[Internet][accedidoel8deenerode2015]Disponibleen:http://whqlibdoc.who.int/publications/2009/9789241598552eng.pdf109HaynesBet al.A Safe surgery checklist toReduceMorbidity andMortality in aGlobal Population.[Internet] New Eng J Med 360;5 nejm.org, 2009 [Accedido 20 febrero 2015] Disponible en:http://www.who.int/patientsafety/safesurgery/SurgicalSafetyChecklist.pdf110 Arriaga AF, Bader AM,Wong JM, Lipsitz SR, BerryWR, Ziewacz JE et al. Simulation-Based trial ofSurgical-Crisischecklists.NEnglJMed.2013Jan17;368(3):246-53.doi:10.1056/NEJMsa1204720.111MahajanRP.TheWHOSurgicalchecklist.BestPracResClinAnasthesiol2011;25:161-68112VatsA,VincentCA,NagpalK,DaviesRW,DarziA,MoorthyK.PracticalchallengesofintroducingWHOsurgicalchecklist:UKpilotexperience.BMJ2010;340:133–136113Treadwell,JLucasS,TsouA.Systematicreview.Surgicalchecklists:asystematicreviewofimpactsandimplementation.BMJQualSaf2014;23:299-318.doi:10.1136/bmjqs-2012-001797114 Mellin-Olsen J, Staender S, Whitaker DK, Smith AF. Helsinki Declaration for Patient safety inAnaesthesiology. [Internet] Eur J Anaesthesiol. 2010 Jul; 27(7):592-7. doi:10.1097/EJA.0b013e32833b1adf. [Accedido 20 febrero 2015] Disponible en:http://www.ncbi.nlm.nih.gov/pubmed/20520556115 Whitaker DK, Brattebø G, Smith AF, Staender SE. The Helsinki Declaration on patient safety inanaesthesiology:Puttingwords intopractice.BestPractResClinAnaesthesiol. 2011 Jun;25(2):277-90.doi:10.1016/j.bpa.2011.02.001.116MuñozyRamón,J.M;GilsanzRodríguez,FLadeclaracióndeHelsinkisobreseguridaddelpacienteenanestesiología. [Internet] Actual. anestesiol. reanim; 21(3): 1-1[3], jul.-sep. 2011. [Accedido 3 enero2015]Disponibleen:http://saudepublica.bvs.br/pesquisa/resource/pt/ibc-97561117 Cometto C,Gómez P, Dal SassoG, Zárate R, de Bortoli S,Falconí C. Enfermería y Seguridad de losPacientes.WashingtonDC.OrganizaciónPanamericanadelaSalud.2011118GarcíaFernándezFP,PancorboHidalgoPL,SoldevillaÁgredaJJ,BlascoGarcíaC.Escalasdevaloracióndel riesgodedesarrollarúlcerasporpresión.Gerokomos [revistaen Internet]. 2008Sep [citado2015Abr 15] ; 19(3): 136-144.Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1134-928X2008000300005&lng=es.http://dx.doi.org/10.4321/S1134-928X2008000300005119CleopasA,KollyV,BovierPA,GarnerinP,PernegerTV.Acceptabilityof identificationbracelets forhospitalinpatients.QualSafHealthCare.2004;13(5):344–348
123
120JointCommission[Sitioweb]StandardsFAQDetails.TwoPatientIdentifiers-NPSG-Goal1-01.01.01[Actualizado Diciembre 2008; Accedido 20 febrero 2015] Disponible en:http://www.jointcommission.org/standardsinformation/jcfaqdetails.aspx?StandardsFaqId=662&ProgramId=47121WorldHealthOrganization.Draftguidelinesforadverseeventreportingandlearningsystems.Frominformationtoaction.[Internet]WorldHealthOrganization.Geneve;2006[Accedido20febrero2015]Disponibleen:http://www.who.int/patientsafety/events/05/ReportingGuidelines.pdf?ua=1122WorldHealthOrganization.PatientSafety.EUValidationofMinimal InformationModel forPatientSafety Incident Reporting. [Internet] [Accedido 20 febrero 2015] Disponible en:http://www.who.int/patientsafety/implementation/informationmodel/en/123VincentC,CoulterA.Patientsafety:whataboutthepatient?QualSafHealthCare2002;11:76-80124BarachP.etal.Exploringpatientparticipationinreducinghealth-care-relatedsafetyrisks[Internet]WHO, 2013 [Accedido 27 diciembre 2014] Disponible en:http://www.euro.who.int/en/publications/abstracts/exploring-patient-participation-in-reducing-healthcare-related-safety-risks125 EMPATHIE: Avedis Donabedian Foundation. Proyecto EMPATHIE: [Internet] [Accedido 20 febrero2015]Disponibleen:http://www.fadq.org/Investigaci%C3%B3n/tabid/56/Default.aspx126 European Patients Forum. Value+ [Internet] [Accedido 20 febrero 2015]. Disponible en:http://www.eu-patient.eu/whatwedo/projects/valueplus127 The Joint Commission. SpeakUp Initiatives. [Internet]. [Accedido 20 febrero 2015]. Disponible en:http://www.jointcommission.org/speakup.aspx128 National Patient Safety Foundation. Patient safety awareness week. [Internet] [Accedido 1marzo2015]Disponibleen:http://www.npsf.org/?page=awarenessweek129NationalInstituteforHealthandCareExcelencePatientexperienceinadultNHSservices:improvingtheexperienceofcareforpeopleusingadultNHSservices..[Internet][Creadofebrero2012;Accedido20febrero2015].http://www.nice.org.uk/guidance/cg138130 Institute forHealthCare Improvement. InvolvePatients inSafety Initiatives. [Internet] Institute forHeath Improvement. Cambridge, Massachussets [Accedido 20 febrero 2015]http://www.ihi.org/resources/Pages/Changes/InvolvePatientsinSafetyInitiatives.aspx131 Safety Is Personal: Partnering with Patients and Families for the Safest Care. Report of theRoundtable on Consumer Engagement in Patient Safety [Internet] The National Patient SafetyFoundation’s Lucian Leape Institut, 2014 [Accedido 20 febrero 2015] Acceso:http://www.npsf.org/about-us/lucian-leape-institute-at-npsf/lli-reports-and-statements/safety-is-personal-partnering-with-patients-and-families-for-the-safest-care/132AustralianCommissionon Safety andQuality inHealthCare.Opendisclosure. [Internet].ACSQHC;2015. [acceso Accedido el 9 de octubre de 2013]. Disponible en:http://www.safetyandquality.gov.au/our-work/open-disclosure/133 Agra Y, FernándezMM. El paciente, elemento clave en lamejora de la seguridad de los serviciosSanitarios.MedicinaPreventivaVol.XVI,N.º3,3erTrimestre,2010;12-16134 Aibar C. ¿Nos creemos de verdad la necesidad de la participación del paciente? Rev Calid ASist2009;24(5):183-184.

124
135TerolE,AgraY,Fernández-MaílloMM,CasalJ,SierraE,BandrésB,GarcíaMJ,delPesoP.TheSpanishNationalHealthSystempatientsafetystrategy,resultsfortheperiod2005-2007.MedClin(Barc).2008Dec;131Suppl3:4-11136Ministerio de Sanidad, Servicios Sociales e Igualdad. Compromiso por la calidad de las sociedadescientíficas de España. [Internet] Ministerio de Sanidad, Servicios Sociales e Igualdad. [Accedido 20febrero2015]Disponibleen:http://www.msssi.gob.es/organizacion/sns/planCalidadSNS/calsscc.htm137WashingtonHealthAlliance.Lesswaste.Lessharm.ChoosingWisely®inWashingtonState.[Internet][Accedido 22 de enero de 2015]. Washington Health Alliance; 2014 Disponible enhttp://wahealthalliance.org/alliance-reports-websites/choosing-wisely/138CollaCH.SwimmingagainsttheCurrent—WhatMightWorktoReduceLow-ValueCare?.NEngl JMed.2014Oct2;371(14):1280-3.doi:10.1056/NEJMp1404503.Ph.D.139MinisteriodeSanidadyConsumo.Análisisde laculturasobreseguridaddelpacienteenelámbitohospitalario del Sistema Nacional de Salud español. [Internet] Madrid: Ministerio de Sanidad yConsumo; 2009. [Accedido 22 febrero 2015] Disponible en:http://www.seguridaddelpaciente.es/es/proyectos/financiacion-estudios/percepcion-opinion/2007/analisis-cultura-seguridad/140MinisteriodeSanidad,ServiciosSocialeseIgualdad.Análisisdelaculturadelaseguridaddelpacientedelosprofesionalesdelaatenciónprimariadelsistemanacionaldesalud.[Internet]Madrid:Ministeriode Sanidad, Servicios Sociales e Igualdad; 2014. [Accedido 22 febrero 2015] Disponible en:http://www.seguridaddelpaciente.es/es/proyectos/financiacion-estudios/percepcion-opinion141 Seguridad del paciente. [Sitio web]. Ministerio de Sanidad, Servicios Sociales e Igualdad. Madrid.[Accedido 28 noviembre 2014]. Disponible enhttp://www.seguridaddelpaciente.es/es/formacion/tutoriales142OteroLópezMJ,AlonsoHernándezP,MaderueloFernández JA,Garrido-CorroB,Dominguez-GilA,Sanchez-RodriguezA.Acontecimientosadversospreveniblescausadospormedicamentosenpacienteshospitalizados.MedClin(Barc).2006;126:81-7143BergaCulleráC,GorgasTornerMQ,AltimirasRuizJ,TusetCreusM,BesalduchMartínM,CapdevilaSunyer M et al. Detección de acontecimientos adversos producidos por medicamentos durante laestanciahospitalaria.FarmHosp.2009;33:312-23.144Pastó-CardonaL,Masuet-AumatellC,Bara-OlivánB,Castro-CelsI,Clopés-EstelaA,Pàez-VivesF,etal.Estudiode la incidenciade loserroresdemedicaciónen losprocesosdeutilizacióndelmedicamento:prescripción, transcripción, validación, preparación, dispensación y administración en el ámbitohospitalario.FarmHosp.2009;33:257-68145 Lacasa C, Ayestarán A y coordinadoras del EMOPEM. Estudio multicéntrico español para laPrevención de Errores deMedicación. Resultados de cuatro años (2007-2011). FarmHosp. 2012; 36:356-67.146 Delgado SánchezO, Nicolás Picó J,Martínez López I, Serrano Fabiá A, Anoz Jiménez L, FernándezCortés F. Errores de conciliación en el ingreso y en el alta hospitalaria en pacientes ancianospolimedicados.Estudioprospectivoaleatorizadomulticéntrico.MedClín(Barc).2009;133:741-9.147Otero LópezMJ,AlonsoHernándezP,MaderueloFernández JA,CerueloBermejo J,Domínguez-GilHurlé A, Sánchez Rodríguez A. Prevalencia y factores asociados a los acontecimientos adversospreveniblespormedicamentosquecausanelingresohospitalario.FarmHosp.2006;30:161-70.
125
148MartínMT,CodinaC,TusetM,CarnéX,NoguéS,RibasJ.Problemasrelacionadosconlamedicacióncomocausadelingresohospitalario.MedClin(Barc)2002;118:205-10.149Ministerio de Sanidad y Consumo. Cuestionario de autoevaluación de la seguridad del sistema deutilizacióndelosmedicamentosenloshospitales.[Internet].Madrid:MinisteriodeSanidadyConsumo;2007. [Accedido 22 febrero 2015]. Disponible en:http://www.msc.es/organizacion/sns/planCalidadSNS/pdf/excelencia/cuestionarioseguridadsistemamedicamentoshospitales.pdf150 InstituteforSafeMedicationPractices.2004 ISMPMedicationSafetySelf-Assessmentforhospitals.[Internet] [Accedido 22 febrero 2015] Disponiblehttp://www.ismp.org/selfassessments/hospital/ismpworkbooksfinal.pdf151MinisteriodeSanidadyConsumo.Estudiodeevaluacióndelaseguridaddelossistemasdeutilizaciónde los medicamentos en los hospitales españoles (2007). [Internet]Madrid:Ministerio de Sanidad yConsumo; 2008. [Accedido 22 febrero 2015] Disponible en:http://www.msc.es/organizacion/sns/planCalidadSNS/docs/evaluacionSeguridadSistemasMedicamentos.pdf152MinisteriodeSanidadyConsumo.Evolucióndelaimplantacióndeprácticassegurasdeutilizacióndemedicamentos en los hospitales españoles (2007-2011). [Internet] Madrid: Ministerio de Sanidad,Servicios Sociales e Igualdad; Informes, estudios e investigación 2012. [Accedido 22 febrero 2015]Disponible en:http://www.msssi.gob.es/organizacion/sns/planCalidadSNS/pdf/EPSMEDICAMENTOSCorregido.pdf153EuropeanCentreforDiseasePreventionandControl.SurveillanceofCommunicableDiseasesintheEuropean Union. A long-term strategy: 2008–2013 [Internet] [accedido el 2 de febrero de 2015].Disponible en: http://www.ecdc.europa.eu/en/aboutus/Key%20Documents/08-13 KD Surveillance ofCD.pdf154 Vaqué J y Grupo de Trabajo EPINE. Resultados del “Estudio de Prevalencia de las InfeccionesNosocomialesenEspaña(EPINEEPPS2012)”enelcontextodel“EuropeanPrevalenceSurveyofHealthcare-associatedInfectionsandAntimicrobialUse(EPPS)”.Versión1.1,19Junio2013.[Internet]SpanishSociety of Medicina Preventiva. [Accedido 20 febrero 2015] Disponible enhttp://hws.vhebron.net/epine/Descargas/Resultados%20EPINE-EPPS%202012%20Resumen%20%28v11%29.pdf155 SEMICYUC: Grupo de trabajo de enfermedades infecciosas. Estudio Nacional de vigilancia de lainfección nosocomial en Servicios de Medicina Intensiva. ENVIN HELICS. Informe 2012. [Internet][Accedido 20 febrero 2015] Disponible en:http://hws.vhebron.net/envin-helics/Help/Informe%20ENVIN-UCI%202012.pdf156 European Centre for Disease Prevention and Control. ECDC surveillance of health care-associatedinfections in intensive care units (ICUs) [Inernet] [accedido el 12 de enero de 2015]. Disponible en:http://www.ecdc.europa.eu/en/activities/surveillance/HAI/aboutHAI-Net/Pages/ICU.aspx157Ministerio de Sanidad, Servicios Sociales e Igualdad. Tolerancia zero en las unidades de cuidadosintensivos. [Internet].MinisteriodeSanidad,ServiciosSocialese Igualdad. [Accedido20 febrero2015]Disponible:http://www.seguridaddelpaciente.es/es/158ProposiciónnodeLeypresentadaporelgrupoParlamentarioPopularenelCongresosobremedidasparalaprevencióndelainfecciónnosocomial.BoletínOficialdelasCortesGenerales,nº181.CongresodelosDiputados,(7deabrilde2009)
126
159PortaldeSaludde laComunidaddeMadridSistemadeVigilanciade InfeccionesRelacionadasconAsistencia Sanitaria VIRAS-Madrid. [Internet] [Creado 13 marzo 2012; Accedido 20 febrero 2015].Disponible en:http://www.madrid.org/cs/Satellite?cid=1142677974680&language=es&pageid=1159444389315&page_name=PortalSalud%2FCMActualidadFA%2FPTSApintarActualidad&vest=1159444389315160 Gencat.cat [Internet]. Vigilancia de las infecciones nosocomiales en los hospitales. [Accedido 20febrero2015]Disponibleen:http://vincat.gencat.cat/es/index.html161 Estrategia Seguridad del Paciente. Osakidtza. 2013-2016. Sistema de Vigilancia y Control de laInfección Nosocomial. INOZ. [Internet] [Accedido 20 febrero 2015] Disponible en:http://www.osakidetza.euskadi.eus/contenidos/informacion/oskpublicaciones/espubli/adjuntos/publica/SeguridadPacienteEs.pdf162 Instituto de Salud Carlos III. Laboratorio de Microbiología [Internet] [Accedido15 febrero 2015].http://www.isciii.es/ISCIII/es/contenidos/fd-servicios-cientifico-tecnicos/laboratorios-referencia2.shtml163EuropeanCentreforDiseasePreventionandControl(ECDC)DatosdelEARS.EuropeanAntimicrobialResistance Surveillance Network (EARS-Net). [Internet] [Accedido 20 febrero 2015]. Disponible en:http://www.ecdc.europa.eu/en/activities/surveillance/EARS-Net/Pages/index.aspx164 European Centre for Disease Prevention and Control. European Surveillance of AntimicrobialConsumption Network (ESAC-Net)[Internet] [accedido el 12 de enero de 2015]. Disponible en:http://www.ecdc.europa.eu/en/activities/surveillance/ESAC-Net/Pages/index.aspx165MinisteriodeSanidad,ServiciosSocialeseIgualdad.ProgramadeHandhygienedelSistemaNacionalde Salud. [Internet] [Accedido 20 febrero 2015]. Disponible en:http://www.seguridaddelpaciente.es/es/proyectos/financiacion-estudios/programa-higiene-manos/166PalomarM,Álvarez-LermaF,RieraA,DíazMT,TorresF,AgraY,LarizgoitiaI,GoeschelCA,PronovostPJ;BacteriemiaZeroWorkingGroup.Impactofanationalmultimodalinterventiontopreventcatheter-relatedbloodstreaminfectionintheICU:theSpanishexperience.CritCareMed.2013Oct;41(10):2364-72167MinisteriodeSanidadServiciosSocialeseIgualdadNotadePrensa[Internet];Madrid.2013-[acceso20dediciembrede2014].Disponibleen:http://www.msssi.gob.es/gabinete/notasPrensa.do?id=2845168Rodríguez-BañoJ,Paño-PardoJR,Álvarez-RochaL,AsensioA,CalboE,CercenadoE,CisnerosJMetal.Programasdeoptimizacióndeusodeantimicrobianos(PROA)enhospitalesespañoles:documentodeconsenso GEIH-SEIMC, SEFH y SEMPSPH. Enf Inf Microb Clin 2012, 30 (1) 22e1-23. doi:10.1016/j.eimc.2011.09.018169MinisteriodeSanidad,ServicioSocialeseIgualdad.Planestratégicoydeacciónparareducirelriesgode selección y diseminación de resistencias a los Antibióticos. [Internet] Agencia Española deMedicamentos y Productos Sanitarios (AEMPS) 2014. [Accedido 20 febrero 2015]. Disponible en:http://www.aemps.gob.es/publicaciones/publica/docs/plan-estrategico-antibioticos.pdf170Aranaz-AndrésJM,Ruiz-LópezP,Aibar-RemónC,Requena-PucheJ,Agra-VarelaY,Limón-RamírezR,Gea-Velázquez MT et al. Sucesos adversos en cirugía general y de aparato digestivo en hospitalesespañoles.CirEsp.2007;82(5):268-77.doi:10.1016/S0009-739X(07)71724-4171MinisteriodeSanidadyPolíticaSocial.BloqueQuirúrgico.Estándaresyrecomendaciones.[Internet].Informes, Estudios e Investigación 2009. Madrid: Ministerio de Sanidad y Política Social. ; 2009.
127
[Accedido 20 febrero 2015]. Disponible en:http://www.msssi.gob.es/organizacion/sns/planCalidadSNS/docs/BQ.pdf172 Gómez-Arnau JI, OteroMJ, BartoloméA, Errando L, Arnal D,MorenoAMet al. Etiquetado de losmedicamentosinyectablesqueseadministranenAnestesia.RecomendacionesdelaSpanishSocietyofAnestesiología, Reanimación y Terapéutica del Dolor (SEDAR), Sistema Español de Notificación enSeguridadenAnestesia y Reanimación (SENSAR) e Institutopara elUso Segurode losMedicamentos(ISMP-España).RevEspAnestesiolReanim2011;58:375-383173 Ministerio de Sanidad. Estándares de calidad de cuidados para la seguridad del paciente en loshospitales del SNS Sistema Nacional de Salud. Proyecto SENECA. [Internet]. Madrid: Ministerio deSanidad. 2008:. Informe Técnico 2008. Madrid: Ministerio de Sanidad [Accedido 12 febrero 2015]Disponibleen:http://www.msssi.gob.es/organizacion/sns/planCalidadSNS/docs/SENECA.pdf174 Gallagher TH,Waterman AD, Ebers AG, Fraser VJ, LevinsonW. Patients’ and Physicians’ Attitudesregarding the Disclosure of Medical Errors. [Internet] JAMA. 2003;289(8):1001-1007.doi:10.1001/jama.289.8.1001 [Accedido 20 febrero 2015] Disponible en:http://jama.jamanetwork.com/article.aspx?articleid=196045175WuAW.Medicalerror:thesecondvictim.[Internet]BMJ2000;320:726[Accedido20febrero2015]Disponibleen:http://www.bmj.com/content/320/7237/726176 Aranaz JM, Mira JJ, Guilabert M, Herrero JF, Vitaller J y Grupo de Trabajo Segundas Víctimas.Repercusión de los eventos adversos en los profesionales sanitarios. Estudio sobre las segundasvíctimas.TraumaFundMAPFRE(2013)Vol24nº1:54-60)177ScottS,HirschingerL,CoxK,McCoigM,BrandtJ,HallL.Thenaturalhistoryofrecoveryforthehealthcareprovider“secondvictim”afteradversepatientevents.QualSafHealthCare2009;18:325–30)178 Canadian Patient Safety Institute. Guidelines for informing the media after an adverse event.[Internet] Canadian Patient Safety Institute 2006. [Accedido 20 febrero 2015] Disponible enhttp://www.patientsafetyinstitute.ca/English/news/Documents/CPSI%20Best%20Practice%20Guide.pdf179LeapeLL.Apologyforerrors:whoseresponsability?FrontHealthServManage2012;28:3-12;180PintoA,FaizO,VincentC.managingtheaftereffectsofseriouspatientsafetyincidentsintheNHS:anonlinesurvey.BMJQualSaf2012;21:1001-1008.181 Conway J, Federico F, Stewart K, CampbellM. RespectfulManagement of Serious Clinical AdverseEvents.[Internet]IHIInnovationSerieswhitepaper.Cambridge,Massachusetts:InstituteforHealthcareImprovement; 2010. IHI Innovation Series white paper: . [Accedido 20 febrero 2015] Disponible en:http://www.ihi.org/resources/Pages/IHIWhitePapers/RespectfulManagementSeriousClinicalAEsWhitePaper.aspx182Guía de recomendaciones para la gestión de eventos centinela y eventos adversos graves en loscentrossanitariosdelSistemaPúblicodeSaluddeGalicia [Internet].SantiagodeCompostela:SERGASServicio Gallego de Salud. 2013. [Accedido 20 febrero 2015] Disponible en:https://www.sergas.es/Publicaciones/DetallePublicacion.aspx?IdPaxina=40008&IDCatalogo=2253183Ministerio de Sanidad, Servicios Sociales e Igualdad. SistemadeNotificación yAprendizaje para laSeguridad del Paciente (SINASP) [Internet] [Accedido 20 febrero 2015] Disponible en:https://www.sinasp.es/184MinisteriodeSanidad,ServiciosSocialeseIgualdad.SistemadenotificacióndeincidentesyEAparaelSNS2006-2008.Estudiodeviabilidadjurídicadeunsistemadenotificaciónyregistrodeincidentesy
128
eventos adversos y propuesta de normativa. [Internet] [Accedido 23 abril 2015] Disponible en:http://www.seguridaddelpaciente.es/es/proyectos/financiacion-estudios/sistemas-de-informacion-y-notificacion/sistemas-notificacion-incidentes/2006-2008/
185MinisteriodeSanidad,PolíticaSocialeIgualdad.Laperspectivadelosciudadanosporlaseguridaddel paciente.[Internet] Madrid: Ministerio de Sanidad, Política Social e Igualdad; 2011.[Accedido 2febrero 2015] Disponible en: http://www.seguridaddelpaciente.es/es/proyectos/financiacion-estudios/percepcion-opinion/2007/percepcion-pacientes/186Ministerio de Sanidad, Servicios Sociales e Igualdad. Redde Escuelas de Saludpara la Ciudadanía.[Internet][Accedido2mayo205]Disponibleen:http://www.reddeescuelas.msssi.gob.es187Aibar C, Aranaz JM, García-Montero JI, Mareca R. La investigación sobre seguridad del paciente:necesidadesyperspectivas.MedClin(Barc).2008;131(Supl3):12-7)188Ministerio de Sanidad, Servicios Sociales e Igualdad [Sitioweb]: Biblioteca Seguridad del Paciente.Disponibleen:http://www.seguridaddelpaciente.es/es/biblioteca/189 Aranaz J, Aibar C, GeaMT, LeónMT. Efectos adversos en la asistencia hospitalaria. Una revisióncríticaMedClin(Barc)2004;123(1):21-5.190StelfoxHT,PalmisaniS,ScurlockC,OravEJ,BatesDW.The“ToErrisHuman”reportandthepatientsafetyliterature.Qual.Saf.HealthCare2006;15;174-178191EuropeanUnionNetwork forPatientSafetyandQuality.OverviewofSCP Implementation inPaSQ[Internet] Member States and participating Health Care Organisations [accedido el 2 de febrero de2015].Disponibleen:http://pasq.eu/Wiki/SCP/OverviewofSCPImplementationinPaSQMemberStat.aspx192MinisteriodeSanidad,ServiciosSocialeseIgualdad.Seguridaddelpaciente[SitioWeb]..[Accedidoel3abrilde2015]Disponibleen:www.seguridaddelpaciente.es193VillamañánE,HerreroAlvarez-SalaR.Prescripciónelectrónicaasistidacomonuevatecnologíaparalaseguridaddelpacientehospitalizado.MedClin(Barc).2011;136(9):398–402194 Mueller SK, Sponsler KC, Kripalani S, Schnipper JL. Hospital-Based Medication ReconciliationPractices: A Systematic Review. Arch Intern Med. 2012;172(14):1057-1069.doi:10.1001/archinternmed.2012.2246195Morís de la Tassa J, Fernández de laMota E, Aibar-RemónC, Castan S, Cameo, Ferrer Tarrés JM..IdentificacióninequívocadepacientesingresadosenhospitalesdelSistemaNacionaldeSalud.[Internet]Med Clin Monogr Barcelona. 2008;131(Supl 3):72-8. [Accedido 2 febrero 2015]Disponible en:http://apps.elsevier.es/watermark/ctl servlet? f=10&pident articulo=13132776&pident usuario=0&pcontactid=&pidentrevista=2&ty=147&accion=L&origen=zonadelectura&web=zl.elsevier.es&lan=es&fichero=2v131nSupl.3a13132776pdf001.pdf196 Joint Commission. Sentinel Event Data Root Causes by Event Type 2004 –2014.Comunicación[Internet] [Accedido 20 febrero 2015] Disponible en:http://www.jointcommission.org/assets/1/18/RootCausesbyEventType2004-2014.pdf197GrupodetrabajodelaguíadePrácticaClínicasobreSeguridaddelPaciente.[Internet][Accedido20febrero 2015] Disponible en: http://www.epes.es/anexos/publicacion/guia practica/Guxa PrxcticaSeguridaddelPaciente-2ed.pdf198UnitedNationsScientificCommitteeontheEffectsofAtomicRadiation.UNSCEAR(2008)SourcesandEffectsofIonisingRadiation,Vol1:Sources,AnnexA:MedicalRadiationExposures.[Internet]NewYork:
129
UnitedNations;2010.ReporttotheGeneralAssemblywithScientificAnnexes.[Accedido20febrerode2015]Disponibleen:http://www.unscear.org/docs/reports/2008/09-86753Report2008AnnexB.pdf199 Organización Mundial de la Salud (OMS) 2006. Iniciativa Global de Seguridad Radiológica enEstablecimiento Sanitarios. [Internet] OMS [Accedido 20 febrero 2015] Disponible en:http://www.sepr.es/html/recursos/noticias/OMSyPR.pdf200 Organización Internacional de Energía Atómica (OIEA) 2002 Plan de Acción Internacional para laProtección Radiológica de los Pacientes. [Internet] [Accedido 20 febrero 2015] Disponible enhttps://www.iaea.org/newscenter/focus/radiation-protection201DirectivaEuropea2013/59/EURATOMsobreNormasBásicasdeSeguridadparalaproteccióncontrariesgosderivadosdeexposicionesaradiacionesionizantes.[Internet]DiarioOficialdelaUniónEuropeaL13/1. [Accedido 20 febrero de 2015] Disponible en: http://www.boe.es/doue/2014/013/L00001-00073.pdf202RealDecretoporlosqueseestablecenloscriteriosdecalidadenMedicinaNuclear(RD1841/1997).[Internet] BoletínOficial del Estado num. 303, de 19 de diciembre de 1997. [Accedido 20 febrero de2015]Disponibleen:http://www.boe.es/diarioboe/txt.php?id=BOE-A-1997-27260203 Real Decreto por los que se establecen los criterios de calidad en Radioterapia (RD 1566/1998).[Internet]BoletínOficialdelEstadonum.206,de28deagostode1998.[accedido20febrerode2015]Disponibleen:http://www.boe.es/diarioboe/txt.php?id=BOE-A-1998-20644204RealDecretoporlosqueseestablecenloscriteriosdecalidadenRadiodiagnóstico(RD1976/1999).[Internet] Boletín Oficial del Estado núm. 311 de 29 diciembre 1999. [Accedido 20 febrero de 2015]Disponibleen:http://www.boe.es/boe/dias/1999/12/29/pdfs/A45891-45900.pdf205RealDecretosobreJustificacióndelusode lasradiaciones ionizantespara laprotecciónradiológicade las personas conocasiónde las exposicionesmédicas (RD815/2001). [Internet] BoletínOficial delEstado núm. 168, de 14 de julio de 2001[Accedido 20 febrero de 2015] Disponible en: http:http://www.boe.es/diarioboe/txt.php?id=BOE-A-2001-13626206InternationalAtomic EnergyAgency, the EuropeanCommission, PanAmericanHealthOrganizationandtheWorldHealthOrganization.Proceedingsofaninternationalconference:RadiologicalProtectionof Patients in Diagnostic and Interventional Radiology, Nuclear Medicine and Radiation therapy.[Internet] Málaga: 2001. [Accedido 26 febrero 2015] Disponible en:http://www-pub.iaea.org/mtcd/publications/pdf/pub1113scr/pub1113scr1.pdf207AsociaciónEspañoladeNormalizaciónyCertificaciónAENOR[Internet][Consultada25marzo2015]http://www.aenor.es/aenor/aenor/acreditaciones/acreditaciones.asp.208 Portal Estadístico del Sistema Nacional de Salud. Base de Datos Clínicos de Atención Primaria –BDCAP. [Internet] Ministerio de Sanidad. [Accedido 20 febrero 2015] Disponible:http://www.msssi.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/SIAP/home.htm209WHO.QualityofCare:AprocessformakingstrategicchoicesinHealthsystems,WHO2006.ISBN9241563249210 Rogers G, Alper E, Brunelle D, Federico F, Fenn CA, Leape LL et al. Reconciling medications atadmission:Safepracticerecommendationsand implementationstrategies. JtCommJQualPatientSaf2006;32:37-50211 Constitución Española de 1978. [Internet] [Accedido el 20 febrero 2015] Disponible enhttp://www.lamoncloa.gob.es/documents/constituciones1.pdf
130
212HalliganM,ZecevicA.Safetycultureinhealthcare:areviewofconcepts,dimensions,measuresandprogress.BMJQualSaf2011;20:338–43213WorldHealthOrganization,WorldAlliance for Patient Safety.Marco conceptual de la clasificacióninternacional para la seguridad del paciente. Informe técnico definitivo. [Monografía en Internet].Geneva: World Health Organization, 2009 [citado 10 de febrero de 2015]. Disponible en:http://www.who.int/patientsafety/implementation/taxonomy/es/index.html214RealDecreto577/2013,de26dejulio,porelqueseregulalafarmacovigilanciademedicamentosdeuso humano. [Internet] BOE núm. 179, de 27 de julio de 2013, páginas 55066 a 55092 [Accedido 23marzo2015]Disponibleen:http://www.boe.es/diario_boe/txt.php?id=BOE-A-2013-8191215PujolM,LimónE.Epidemiologíageneralde las infeccionesnosocomiales.SistemasyprogramasdevigilanciaEnfermInfeccMicrobiolClin.2013;31(2):108–113216MinisteriodeSanidadyConsumo.PlandeCalidadparaelSNS.OteroMJ.Prácticasparamejorar laseguridad de los medicamentos de alto riesgo. [Internet] MSC, 2007 [Accedido 23 marzo 2015]Disponible en:http://www.ismp-espana.org/ficheros/Practicas%20para%20mejorar%20la%20seguridad%20de%20los%20medicamentos%20de%20alto%20riesgo..pdf217Ley41/2002,de14denoviembre,básicareguladorade laautonomíadelpacienteydederechosyobligaciones enmateria de información y documentación clínica. [Internet] BOE núm. 274, de 15 denoviembre de 2002, páginas 40126 a 40132. [Accedido el 24 marzo 2015] Disponible en:http://www.boe.es/diario_boe/txt.php?id=BOE-A-2002-22188218. The Free Dictionary..[Internet] Procedimiento [Accedido 15 marzo 2015] Disponible en:http://es.thefreedictionary.com/procedimiento219RealDecreto69/2015,de6defebrero,queregulaelRegistrodeActividaddeatenciónEspecializada.[Internet] BOEnúm.35, de10de febrerode2015, páginas 10789a 10809 (21págs.). [Accedidoel 3marzode2015]Disponibleen:http://www.boe.es/diario_boe/txt.php?id=BOE-A-2015-1235220MinisteriodeSanidadyPolíticaSocial.InstitutodeInformaciónSanitariaSistemaNacionaldeSaluddeEspaña2010 [monografíaen Internet].Madrid:MinisteriodeSanidadyPolíticaSocial, InstitutodeInformación Sanitaria. [Accedido 20 febrero 2015] Disponible en:http://www.msssi.gob.es/organizacion/sns/docs/sns2010/Principal.pdf





























