Embed Size (px)
Citation preview

Applying TG-100 Methodology to SRS / SBRT
Jennifer Lynn Johnson, MS, MBASenior Medical Physicist and Director for Safety, Radiation [email protected]
Patient Safety in the Treatment Process
MD Anderson
AAPM Working Group on Prevention of Errors, Chair
Special thanks to:• Team members of the Division at Radiation Oncology• Julian R Perks, et. al.• Laura Masini, et. al.• Kelly Cooper Younge, et. al.• F Yang, et. al.• Ryan P. Manger, et. al.
Disclosures2Patient Safety in the Treatment Process

MD Anderson
Clearly, we want to avoid patient harm.
We typically measure and respond to specific incidents of harm.
Can we do better?
3Patient Safety in the Treatment Process

MD Anderson
Contents
1 RISK
2 SRS / SBRT QA PROGRAM
3 SRS / SBRT PROCESS
4 FAILURE MODES AND EFFECTS ANALYSIS
5 FAULT TREE ANALYSIS
6 SOPS FOR MAJOR STEPS
7 SAFETY CHECKLIST
8 PROGRAM MONITORING
Patient Safety in the Treatment Process 4

MD Anderson
Risk
5Patient Safety in the Treatment Process

MD Anderson
Risk is the likelihood a hazard causes harm to a patient.
What can go wrong?
How likely is it to go wrong?
What are the consequences if it goes wrong?
Defining Risk6Patient Safety in the Treatment Process

MD Anderson
RT is adopting incident learning system (ILS)
• Reactive: identify after the fact, control only for the future
• Difficult to monitor low occurrence incidents
High risk industries identify, control and monitor hazards
Allows active management of the environment
• Manage the hazards that give rise to risk
• Create resilience for unexpected risks
Risk Management7Patient Safety in the Treatment Process

MD Anderson
Prospectively analyze hazards in a process.
For the RT treatment process, AAPM TG-100 uses:
• Process Mapping
• Failure Modes and Effects Analysis
• Fault Tree Analysis
Structured ways to prioritize risk and determine where to focus resources
Risk Assessment8Patient Safety in the Treatment Process

MD Anderson
SRS / SBRT is typically a complete course of radiation therapy (RT) delivered in 1 to 5 sessions (fractions).
SRS / SBRT requires greater precision and accuracy than conventionally fractionated RT => follow strict protocols for quality assurance (QA).
9Patient Safety in the Treatment Process

MD Anderson
ACR–ASTRO Practice Parameter for the Performance of Stereotactic Body Radiation Therapy. Practice guidelines and technical standards. Reston, VA: American College of Radiology; 2014: 1-11.
ACR–ASTRO Practice Parameter for the Performance of Stereotactic Radiosurgery. Practice guidelines and technical standards. Reston, VA: American College of Radiology; 2014: 1-11.
Benedict SH, Yenice KM, Followill D, et al. Stereotactic body radiation therapy: the report of AAPM Task Group 101. Med Phys. 2010;37(8):4078-4101.
Keall PJ, Mageras GS, Balter JM, et al. The management of respiratory motion in radiation oncology report of AAPM Task Group 76. Med Phys. 2006;33(10):3874-3900.
Klein EE, Hanley J, Bayouth J, et al. Task Group 142 report: quality assurance of medical accelerators. Med Phys. 2009;36(9):4197-4212.
Solberg TD, Balter JM, Benedict SH, Fraass BA, Kavanagh B, Miyamoto C, Pawlicki T, Potters L, Yamada Y. Quality and safety considerations in stereotactic radiosurgery and stereotactic body radiation therapy. Prac. Rad. Onc. 2012; Mar 31;2(1):2-9.
Published Guidance for Comprehensive QA10Patient Safety in the Treatment Process

MD Anderson
“Central goal of patient safety is to avoid potential harm rather than compliance with systems and processes.”
11Patient Safety in the Treatment Process
Vincent C, Burnett S, Carthey J. The measurement and monitoring of safety. London: The Health Foundation. 2013 May 24;2013.

MD Anderson
SRS / SBRT Process
12Patient Safety in the Treatment Process

MD Anderson
Visual illustration of the steps in a process
What is accomplished
How steps are related
Process steps may be subdivided into sub-processes, and so on.
Process Mapping13Patient Safety in the Treatment Process

MD Anderson
Imaging
Treatment Planning
Dose Delivery
Generic SRS / SBRT ProcedurePatient Safety in the Treatment Process 14
Adapted from Ford, E. C., et al. "Consensus recommendations for incident learning database structures in radiation oncology." Medical physics 39.12 (2012): 7272-7290.

MD Anderson
Delivering modern external beam radiation therapy is not so simple.
15Patient Safety in the Treatment Process

MD Anderson 16Patient Safety in the Treatment Process
MDACC Radiation Oncology Process - EBRT
Adapted from Ford, E. C., et al. "Consensus recommendations for incident learning database structures in radiation oncology." Medical physics 39.12 (2012): 7272-7290.

MD Anderson
Failure Modes and Effects Analysis
Fault Tree Analysis
17Patient Safety in the Treatment Process

MD Anderson
Vocabulary:
• Failure mode: how a part or process can fail
• Cause: a deficiency that results in a failure mode; source of variation
• Effect: impact on a person if the failure mode is not prevented or corrected
A multidisciplinary team (experts) generate actual and potential risks (without QC)
Especially useful for high-risk processes
Structured approach that links failure modes to an effect
Failure Modes and Effects Analysis (FMEA)18Patient Safety in the Treatment Process

MD Anderson
Steps:
• Identify ways a sub-process (or product) can fail, both known & potential
• Determine each failure mode’s causes & effects • Assign a number to most severe (S)
effect
• Determine likelihood each failure mode’s occurrence (O) & detection (D)
Failure Modes and Effects Analysis (FMEA)19Patient Safety in the Treatment Process
Huq MS, Fraass BA, Dunscombe PB, Gibbons JP, Ibbott GS, Mundt AJ, Mutic S, Palta JR, Rath F, Thomadsen BR, Williamson JF. The report of Task Group 100 of the AAPM: Application of risk analysis methods to radiation therapy quality management. Medical Physics. 2016 Jul 1;43(7):4209-62
• Calculate risk priority number (RPN) = O x S x D

MD Anderson
Rank the RPN values (highest to lowest)
Pick the 3 failure modes with the highest RPN values and highest S values
• RPN ≥ 100
• S ≥ 7
Propose process changes that would decrease the probability of occurrence, O
Propose QC that would decrease the probability of un-detectability, D
Failure Modes and Effects Analysis (FMEA)20Patient Safety in the Treatment Process
Huq MS, Fraass BA, Dunscombe PB, Gibbons JP, Ibbott GS, Mundt AJ, Mutic S, Palta JR, Rath F, Thomadsen BR, Williamson JF. The report of Task Group 100 of the AAPM: Application of risk analysis methods to radiation therapy quality management. Medical Physics. 2016 Jul 1;43(7):4209-62

MD Anderson
Completing FMEAMDACC Exercise (2013)
21Patient Safety in the Treatment Process
Asked a multidisciplinary team to complete a survey
• For each of the sub-process steps
• Did not ask specific causesEstimating Failure Mode ScoresIn columns 2-4 of Table 1, use Table A (provided separately) to fill in your best estimate the following scores:O = Occurrence. The likelihood the failure would occur. (1-10)D = Detectability. The likelihood the failure would go undetected. (1-10)S = Severity. The severity of the consequences of the failure. (1-10)Again, imagine the worst case scenario. Consider each failure independently
• Team reviewed results together and agreed in general the RPN rankings
• Purpose for ILS action scale

MD Anderson
Completing FMEATreatment Planning – O, D, S
22Patient Safety in the Treatment Process

MD Anderson
Completing FMEAMDACC Exercise (2013) Calculating RPN
23Patient Safety in the Treatment Process

MD Anderson
Completing FMEAMDACC Exercise (2013) Ranking RPN
24Patient Safety in the Treatment Process

MD Anderson
Completing FMEAMDACC Exercise (2013) RPN vs. S
25Patient Safety in the Treatment Process
Divisional RPN Physics RPN

MD Anderson
Completing FMEAMDACC Exercise (2013) RPN ≥ 100
26Patient Safety in the Treatment Process

MD Anderson
Completing FMEAMDACC Exercise (2013) S ≥ 7
27Patient Safety in the Treatment Process

MD Anderson
Propose process changes to decrease likelihood of occurrence (O).
Propose quality control to decrease likelihood of un-detectability (D).
28Patient Safety in the Treatment Process
Huq MS, Fraass BA, Dunscombe PB, Gibbons JP, Ibbott GS, Mundt AJ, Mutic S, Palta JR, Rath F, Thomadsen BR, Williamson JF. The report of Task Group 100 of the AAPM: Application of risk analysis methods to radiation therapy quality management. Medical Physics. 2016 Jul 1;43(7):4209-62

MD Anderson
Evaluate the propagation of failures
• Gives visual representation of propagation of a failure in the process
• Helps identify intervention strategies to mitigate the FMEA identified risks
Fault Tree Analysis (FTA)29Patient Safety in the Treatment Process
Huq MS, Fraass BA, Dunscombe PB, Gibbons JP, Ibbott GS, Mundt AJ, Mutic S, Palta JR, Rath F, Thomadsen BR, Williamson JF. The report of Task Group 100 of the AAPM: Application of risk analysis methods to radiation therapy quality management. Medical Physics. 2016 Jul 1;43(7):4209-62

MD Anderson
Fault Tree Analysis (FTA)30Patient Safety in the Treatment Process
Steps
• Define the undesired event
• Understand the system
• Construct the fault tree
• Evaluate the fault tree
• Control the identified hazards
Huq MS, Fraass BA, Dunscombe PB, Gibbons JP, Ibbott GS, Mundt AJ, Mutic S, Palta JR, Rath F, Thomadsen BR, Williamson JF. The report of Task Group 100 of the AAPM: Application of risk analysis methods to radiation therapy quality management. Medical Physics. 2016 Jul 1;43(7):4209-62

MD Anderson
Fault Tree Analysis (FTA)31Patient Safety in the Treatment Process
Events in a fault tree are associated with statistical probabilities
• AND gate probability of output:• P(A and B) = P(A∩B) = P(A) P(B)
• OR gate probability of output:• P(A or B) = P(AUB) = P(A) + P(B) -
P(A∩B)
Huq MS, Fraass BA, Dunscombe PB, Gibbons JP, Ibbott GS, Mundt AJ, Mutic S, Palta JR, Rath F, Thomadsen BR, Williamson JF. The report of Task Group 100 of the AAPM: Application of risk analysis methods to radiation therapy quality management. Medical Physics. 2016 Jul 1;43(7):4209-62

MD Anderson
Utilization of Process Maps, FMEA, and FTA enable development of your Quality Management program.
32Patient Safety in the Treatment Process

MD Anderson
Comprehensive QA ProgramMDACC Exercise (2013) – Improvements in Progress
36Patient Safety in the Treatment Process
Immobilization and Simulation Devices
Treatment Planning System
Treatment Delivery Unit
Ancillary Systems for Imaging and Motion Management
Patient-specific Treatment Delivery Parameter Validation
Other – RO Treatment Planning
Other – Treatment Delivery
QMP, RO present
Committee review required prior release
QMP peer review QA
Improved engineering notifications
Improved SRS / SBRT treatment checklist
RTT time out process & checklist
Dosimetry checklist
RO Peer review

MD Anderson
Experience39Patient Safety in the Treatment Process
Perks, J. R., Stanic, S., Stern, R. L., Henk, B., Nelson, M. S., Harse, R. D., ... & Chen, A. M. (2012). Failure mode and effect analysis for delivery of lung stereotactic body radiation therapy. International Journal of Radiation Oncology* Biology* Physics, 83(4), 1324-1329.

MD Anderson
CBCT isocenter misalignment -> vigilent IGRT QA
Automatic setup failure -> frame agreement within 2 mm CBCT
Improper laser marking or transcription error for couch movements -> instituted dry run to test need to translate patient away from iso
Patient movements during treatment -> considering infrared surface tracking
Instituted checklists
Reviewed staffing levels
Experience40Patient Safety in the Treatment Process
Perks, J. R., Stanic, S., Stern, R. L., Henk, B., Nelson, M. S., Harse, R. D., ... & Chen, A. M. (2012). Failure mode and effect analysis for delivery of lung stereotactic body radiation therapy. International Journal of Radiation Oncology* Biology* Physics, 83(4), 1324-1329.

MD Anderson
Experience41Patient Safety in the Treatment Process
Masini, L., Donis, L., Loi, G., Mones, E., Molina, E., Bolchini, C., & Krengli, M. (2014). Application of failure mode and effects analysis to intracranial stereotactic radiation surgery by linear accelerator. Practical radiation oncology, 4(6), 392-397.

MD Anderson
Wrong collimator selection -> instituted bar code reader
Isocenter localization -> utilize infrared surface tracking for independent localization system verification
Target and OAR contours -> contour peer review
RO consults similar patients -> cross-check clinical documentation
Training, roles & responsibilities
Scheduling of treatments
Experience42Patient Safety in the Treatment Process
Masini, L., Donis, L., Loi, G., Mones, E., Molina, E., Bolchini, C., & Krengli, M. (2014). Application of failure mode and effects analysis to intracranial stereotactic radiation surgery by linear accelerator. Practical radiation oncology, 4(6), 392-397.
MD Anderson
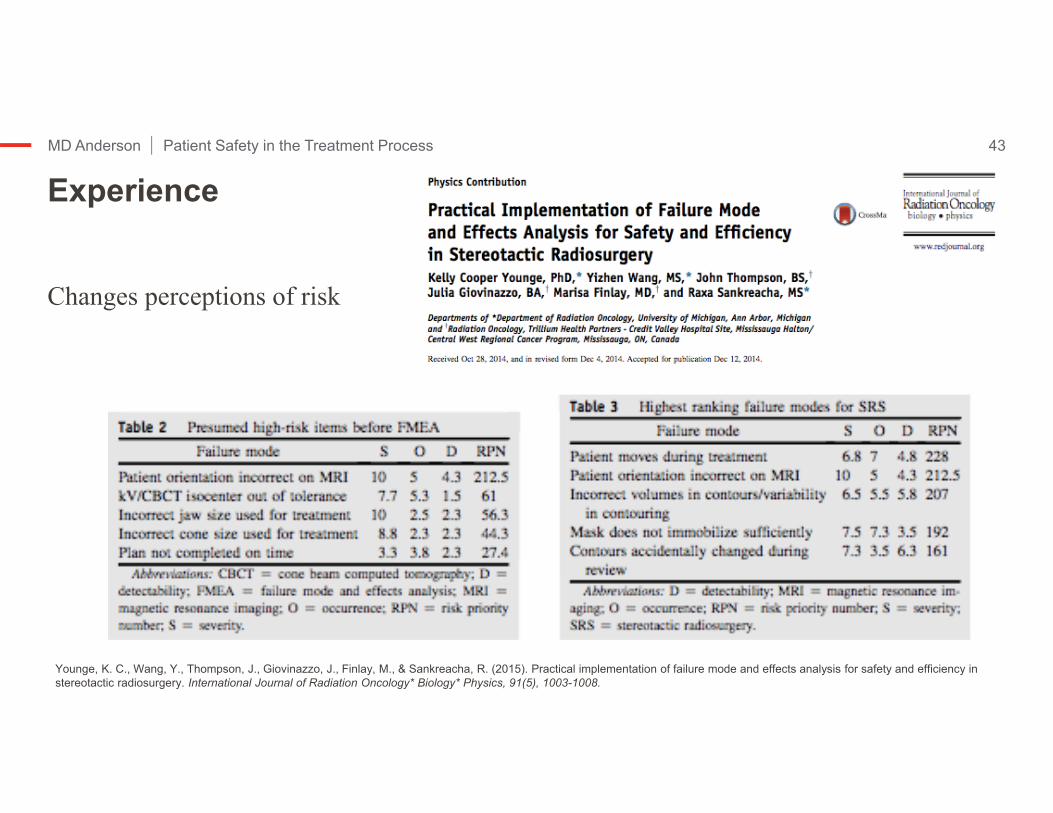
Changes perceptions of risk
Experience43Patient Safety in the Treatment Process
Younge, K. C., Wang, Y., Thompson, J., Giovinazzo, J., Finlay, M., & Sankreacha, R. (2015). Practical implementation of failure mode and effects analysis for safety and efficiency in stereotactic radiosurgery. International Journal of Radiation Oncology* Biology* Physics, 91(5), 1003-1008.

MD Anderson
Mask fitting -> monitor pre-treatment and post-treatment imaging
Patient orientation on MRI -> additional staff checks
Contours -> additional auto comparison of approved versus final plan
Contours -> mandatory peer review prior to treatment planning
Experience44Patient Safety in the Treatment Process
Younge, K. C., Wang, Y., Thompson, J., Giovinazzo, J., Finlay, M., & Sankreacha, R. (2015). Practical implementation of failure mode and effects analysis for safety and efficiency in stereotactic radiosurgery. International Journal of Radiation Oncology* Biology* Physics, 91(5), 1003-1008.

MD Anderson
Criterion-based FMEA compared with incidents reported in ILS
-> 61% (20/33) identified by FMEA
->39% (13/33) not identified by FMEA ->Significantly lower RPNs
Experience45Patient Safety in the Treatment Process
Yang, F., Cao, N., Young, L., Howard, J., Logan, W., Arbuckle, T., ... & Ford, E. (2015). Validating FMEA output against incident learning data: A study in stereotactic body radiation therapy. Medical physics, 42(6), 2777-2785.

MD Anderson
16 / 91 steps surface imaging
25 / 167 had RPN >100-> 1 related to surface imaging
Use systematic approach to FMEA(e.g., HAZOP or SHERPA)
Experience46Patient Safety in the Treatment Process
Manger, R. P., Paxton, A. B., Pawlicki, T., & Kim, G. Y. (2015). Failure mode and effects analysis and fault tree analysis of surface image guided cranial radiosurgery. Medical physics, 42(5), 2449-2461.

MD Anderson
Experience47Patient Safety in the Treatment Process
Manger, R. P., Paxton, A. B., Pawlicki, T., & Kim, G. Y. (2015). Failure mode and effects analysis and fault tree analysis of surface image guided cranial radiosurgery. Medical physics, 42(5), 2449-2461.
MD Anderson
Experience suggests Standardized Operating Procedures (SOPs) for major steps are critical to patient safety.
48Patient Safety in the Treatment Process

MD Anderson
Safety ChecklistMedical Physics Practice Guideline 4.a
49Patient Safety in the Treatment Process
Role of checklists
Organizational influences on checklists: safety culture
Teamwork is essential
Development & Implementation
Revision
Maintenance
de los Santos LE, Evans S, Ford EC, Gaiser JE, Hayden SE, Huffman KE, Johnson JL, Mechalakos JG, Stern RL, Terezakis S, Thomadsen BR. Medical Physics Practice Guideline 4. a: Development, implementation, use and maintenance of safety checklists. Journal of Applied Clinical Medical Physics. 2015 May 8;16(3).

MD Anderson
Use of checklists
Design recommendations
• Content
• Workflow, layout & format
• Physical characteristics (e.g., font, text color, shading)
Safety ChecklistMedical Physics Practice Guideline 4.a
50Patient Safety in the Treatment Process
de los Santos LE, Evans S, Ford EC, Gaiser JE, Hayden SE, Huffman KE, Johnson JL, Mechalakos JG, Stern RL, Terezakis S, Thomadsen BR. Medical Physics Practice Guideline 4. a: Development, implementation, use and maintenance of safety checklists. Journal of Applied Clinical Medical Physics. 2015 May 8;16(3).
MD Anderson
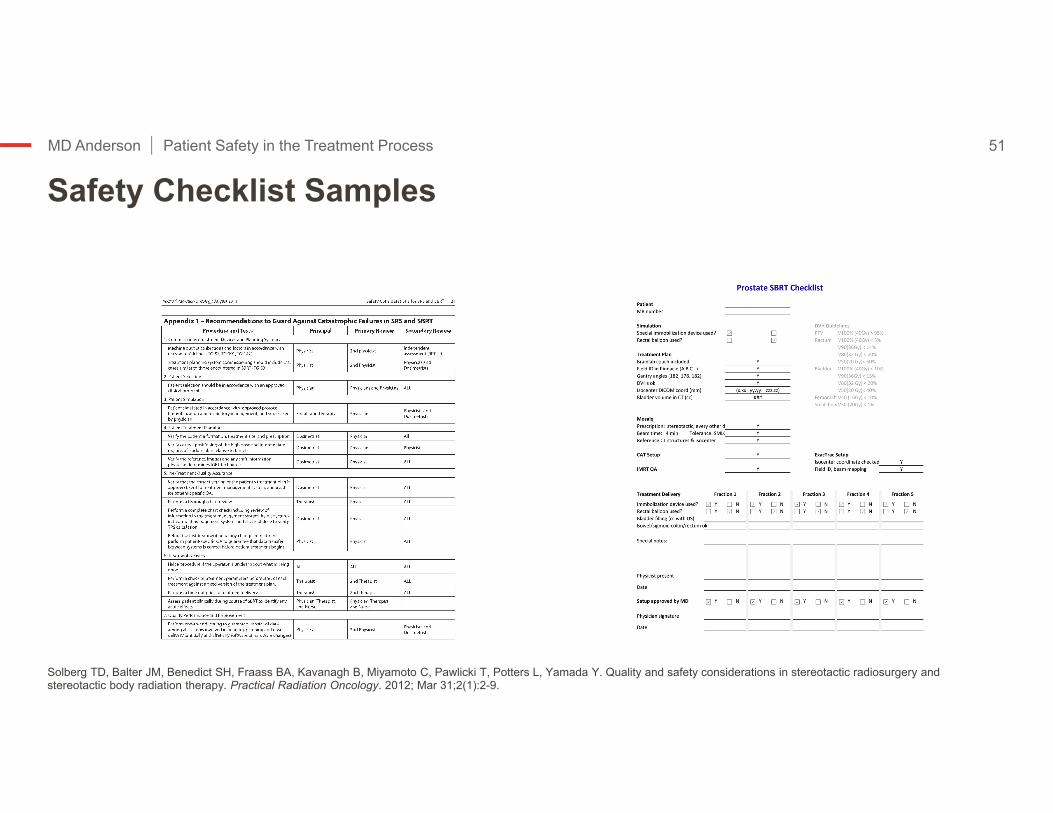
Safety Checklist Samples51Patient Safety in the Treatment Process
Solberg TD, Balter JM, Benedict SH, Fraass BA, Kavanagh B, Miyamoto C, Pawlicki T, Potters L, Yamada Y. Quality and safety considerations in stereotactic radiosurgery and stereotactic body radiation therapy. Practical Radiation Oncology. 2012; Mar 31;2(1):2-9.

MD Anderson
Program Monitoring Patient Safety
Past harm
Reliability
Sensitivity to operations
Anticipation and preparedness
Integration and learning
Vincent, C., Burnett, S., & Carthey, J. (2013). The measurement and monitoring of safety. The Health Foundation
Patient Safety in the Treatment Process 53
MD Anderson
Program Monitoring Patient Safety54Patient Safety in the Treatment Process
Past Harm
• SafetyLink ILS
• Outcomes
Reliability
• Improved standardized protocols and guidelines
Sensitivity to Operations
• Daily Coms
• Team operation huddles
Anticipation and Preparedness
• Checklists
• Safety culture
• Staffing indicators (absence rates)
Integration and Learning
• Walk-rounds
• Patient surveys
• Chart audits, dashboards
• ILS and RCAVincent, C., Burnett, S., & Carthey, J. (2013). The measurement and monitoring of safety. The Health Foundation





























