Embed Size (px)
Citation preview

Patient Management Issues in Menopause
A CME Slide Library From the
Council on Hormone Education

Patient Management Issues in Menopause
Section 1: Appropriate Use of HT
Section 2: Barriers to Appropriate Use of HT
Section 3: Importance of Individualizing HT3a. Characteristics of Estrogens3b. Characteristics of Progestins3c. Use of Low-Dose HT3d. Non-Oral HT Formulations
Section 4: Non-HT Alternatives for Menopausal Symptoms
Section 5: Patient Counseling Strategies
HT = hormone therapy (estrogen [E] alone or combined with a progestin [E+P]).

Section 1:
Appropriate Use of HT
Patient Management Issues in Menopause

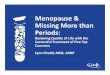
Percentage
Menopause-relatedSymptoms
Osteoporosis, Bone Loss,Fracture Prevention
Doctor Prescribed It,Told Me to Take It
Cardiovascular DiseasePrevention
Other
Depression, Anxiety,Emotional Distress
0 10 20 30 40 50 60
Newton KM, et al. J Womens Health. 1997;6:459-65.
Reasons Women Gave for Initiating or Continuing HT

FDA-Approved Indications for HT
Treatment of moderate-to-severe vasomotor symptoms associated with menopause
Treatment of vulvar and vaginal atrophy
Prevention of postmenopausal osteoporosis
FDA Guidance for Industry. Available at: http://www.fda.gov/cder/guidance/5417dft.pdf. Accessed 1/04.

Women’s Health Initiative (WHI) Updated Results Summary: Breast Cancer
For invasive breast cancer, HR = 1.24 (95% CI, 1.01–1.54; P = .003) after 5 years of E+P
For total breast cancer, HR = 1.24 (95% CI, 1.02–1.50; P < .001) after 5 years of E+P
Exclusion of women with prior HT use (26.1%), HR was nonsignificant at 1.09 (95% CI, 0.86–1.39)
Analysis of breast cancer data showed slightly larger tumors (1.7 cm with E+P use vs 1.5 cm with placebo) and ~10% more regional node positivity
Chlebowski RT, et al. JAMA. 2003;289:3243-53.

WHI Updated Results Summary: CHD, Fracture, Dementia
CHD data failed to show significance with adjudicated overall 5-year results (HR, 1.24; 95% CI, 1.00–1.54)1
In addition to hip fracture reduction, vertebral fracture was significantly reduced in a non-osteoporotic population (HR, 0.60; 95% CI, 0.38–0.95)2
Dementia increased in women who initiated E+P at age 65 years (HR, 2.05; 95% CI, 1.21–3.48; P = .01)3
– Additional 23 cases/10,000 women/year
– No increase in mild cognitive impairment
CHD = coronary heart disease.1Manson JE, et al. N Engl J Med. 2003;349:523-34; 2Cauley JA, et al. JAMA. 2003;290:1729-38; 3Shumaker SA, et al. JAMA. 2003;289:2651-62.

Cancer (after 5 years of E+P)1
– Endometrial: HR = 0.81 (95% CI, 0.48–1.36, NS)
– Ovarian: HR = 1.58 (95% CI, 0.77–3.24, NS)
No significant improvement in health-related QOL found in largely asymptomatic women (average age, 63 years)2
– Small subset of symptomatic women showed improvement in hot flushes, small benefit in sleep
QOL = quality of life; NS = not significant.1Anderson GL, et al. JAMA. 2003;290:1739-48; 2Hays J, et al. N Engl J Med. 2003;348:1839-54.
WHI Updated Results Summary: Gynecologic Cancers, QOL

WHI Updated Results Summary: Stroke
After 5 years, the risk of stroke was 1.8% for E+P, 1.3% for placebo (HR, 1.31; 95% CI, 1.02–1.68)
– Attributable risk of 0.5% is <0.1% per year
– Attributable risk of E+P for stroke increases with age
age 50–59 years is 0.04% per year
age 70–79 years is 0.13% per year
Wassertheil-Smoller S, et al. JAMA. 2003;289:2673-84.

Study ConsiderationsWHI
There were relatively high rates of discontinuation in the conjugated equine estrogens (CEE)/medroxyprogesterone acetate (MPA) group (42%) and crossover to active treatment in the placebo group (10.7%)
WHI did not evaluate symptom relief, and therefore symptom relief was not included in the global index
Results do not necessarily relate to lower dosages of these drugs or other formulations or routes of administration

*aCIs not available; †Only in women 65 years of age at baseline.1Manson JE, et al. N Engl J Med. 2003;349:523-34; 2Chlebowski RT, et al. JAMA. 2003;289:3243-53; 3Shumaker SA, et al. JAMA. 2003;289:2651-62; 4Wassertheil-Smoller S, et al. JAMA. 2003;289:2673-84; 5Writing Group for the WHI Investigators. JAMA. 2002;288:321-33; 6Anderson GL, et al. JAMA. 2003; 290:1739-48; 7Chlebowski RT, et al. N Engl J Med. 2004;350:991-1004; 8Cauley JA, et al. JAMA. 2003;290:1729-38.
WHI: Results With CEE/MPACHD1
Breast Cancer2
Dementia3*†
Stroke4
VTE5
Endometrial Cancer6
Ovarian Cancer6
Colorectal Cancer7
Hip Fracture8
Total Fracture8*
Death5
HR0.5 1.0 5.02.0
95% nCI
95% aCI

EventOverall
HR 95% nCI 95% aCI
Attributable Risk per 10,000
Women/Year
Benefit per 10,000
Women/Year
CHD1 1.24 1.00–1.54 0.97–1.60 6
Breast cancer2 1.24 1.01–1.54 0.97–1.59 8
Dementia3* 2.05 1.21–3.48 — 23
Stroke4 1.31 1.02–1.68 0.93–1.84 7
VTE5 2.11 1.58–2.82 1.26–3.55 18
PE5 2.13 1.39–3.25 0.99–4.56 8
Colorectal cancer6 0.56 0.38–0.81 0.33–0.94 6
Hip fractures7 0.67 0.47–0.96 0.41–1.10 5
Total fractures7 0.76 0.69–0.83 — 47
WHI Results: Overall Relative and Attributable Risk
VTE = venous thromboembolism; PE = pulmonary embolism. *Only in women 65 years of age at baseline.1Manson JE, et al. N Engl J Med. 2003;349:523-34; 2Chlebowski RT, et al. JAMA. 2003;289:3243-53; 3Shumaker SA, et al. JAMA. 2003;289:2651-62; 4Wassertheil-Smoller S, et al. JAMA. 2003;289:2673-84; 5Writing Group for the WHI Investigators. JAMA. 2002;288:321-33; 6Chlebowski RT, et al. N Engl J Med. 2004;350:991-1004; 7Cauley JA, et al. JAMA. 2003;290:1729-38.

WHI Summary
Results from WHI indicate that CEE 0.625 mg/d plus MPA 2.5 mg/d should not be initiated or continued for the primary prevention of CHD
Risks for CVD and breast cancer must be weighed against the benefit for fracture and colon cancer
CVD = cardiovascular disease.Writing Group for the Women's Health Initiative Investigators. JAMA. 2002;288:321-33.

Interpretation of the WHI Data
Majority of women initiate HT to alleviate menopausal symptoms1 – 75% of HT users initiate therapy within 5 years of
menopause– In a 1999 national survey (n = 9400; age 40
years), 24% used HT, 3% E+P for 5 years, 10% used ET for 5 years2
Results should not be extrapolated to symptomatic early menopausal or prematurely menopausal women using HT for symptom relief3
– Average age at screening, 63 years– Only 4% of WHI participants had moderate to
severe vasomotor symptoms1Writing Group for the Women's Health Initiative Investigators. JAMA. 2002;288:321-33; 2Brett KM, Ruben CA. Am J Obstet Gynecol. 2003;102:1240-9. 3North American Menopause Society. Menopause. 2003;10:497-506.

Post-WHI Survey
1000 high-compliance Kaiser Permanente patients were mailed a letter explaining the WHI study findings and recommendations about continuing HT
– 670 women agreed to complete an interview 94.5% considered stopping HT
– 56% of women attempted to discontinue HT
– 44% chose to continue therapy; of those women 25.7% for relief of vasomotor symptoms 19.2% for osteoporosis 47.2% for other reasons (ie, mood swings,
vaginal dryness, urinary incontinence, and depression)
Ettinger B, et al. Obstet Gynecol. 2003;102:1225-32.

American College of Obstetricians and Gynecologists (ACOG). Statement on the Estrogen Plus Progestin Trial of the Women’s Health Initiative. July 9, 2002. Available at: http://www.acog.org/from_home/publications/press_releases/nr07-09-02.cfm. Accessed 8/19/02.
Statement on HT From ACOG
Women who have been taking HT for a number of years should not panic, but discuss their individual situation with their physician
With respect to women’s short-term use of HT for relief of menopausal symptoms, it may be reasonable for women to continue use for this purpose because the benefits are likely to outweigh the risks
For short-term use of HT for relief of menopausal symptoms, ACOG continues to recommend that this be a personal, individualized decision, made after consultations between a woman and her physician—taking into account a woman’s individual benefits and risks from such use

2003 NAMS Position Statement on HT
Primary indication for systemic HT is the treatment of moderate-to-severe menopausal symptoms
Local estrogen recommended for moderate-to-severe vulvar and vaginal atrophy
Primary indication for progestogen – Endometrial protection
HT should not be used for 1° or 2° prevention of CHD or stroke
WHI results cannot be extrapolated to– Symptomatic perimenopausal women– Premature menopause
HT should be used at the lowest effective dose for the shortest duration needed
North American Menopause Society (NAMS). Menopause. 2003;10:497-506.

Indications for Extended Use of HT
After informed discussion and under ongoing supervision
– For the woman for whom, in her opinion, benefits of symptom relief outweigh risks, notably after failing an attempt to withdraw from HT
– For women with moderate-to-severe menopausal symptoms who are at high risk for osteoporotic fracture
– For prevention of osteoporosis in a high-risk woman when alternate therapies are not appropriate for that woman
North American Menopause Society. Menopause. 2003;10:497-506.

National Institutes of Health (NIH). National Heart, Lung, and Blood Institute. New Facts About: Estrogen/Progestin Hormone Therapy. Available at: http://www.nhlbi.nih.gov/health/women/pht_facts.htm. Accessed 8/19/02.
Summary of NIH Recommendations
While short-term use was not studied in the WHI, women taking HT for relief of menopausal symptoms may reap more benefits than risks
Women should keep up with their regular schedule of mammograms and breast self-examinations
HT should not be continued or started to prevent heart disease; women should consult their doctor about other methods of CVD prevention
For osteoporosis prevention, women should consult their doctor and weigh the benefits against their personal risks; alternate treatments are available to prevent osteoporosis and fractures

Section 2:
Barriers to Appropriate
Use of HT
Patient Management Issues in Menopause

Barriers to Appropriate Use of HT
Concerns about the long-term safety of HT
HT-related vaginal bleeding
Inadequate counseling on the risks and benefits

Women’s Perceptions of Their Greatest Health Problems
Adapted from Mosca L, et al. Arch Fam Med. 2000;9:506-15.
Breast Cancer
Cancer
Other Problems
Cardiovascular Disease
Don’t Know/ No Answer
34%34%
27%27%
16%16%
7%7%
16%

Causes of Death Among Women*
*Percentage of total deaths in 1999 among women aged 65 years and older.Anderson RN. Natl Vital Stat Rep. 2001;49:1-13.
Heart Disease
Other Cancers
Other
Diabetes
Chronic LowerRespiratory
Disease
Cerebrovascular Disease
Breast Cancer 34%
10%10%
6%6%
3%3%
15%15%
28%
4%4%

Absolute Risk of Breast Cancer in the General Population
Each 50-year-old woman has approximately a 2.8% chance of developing breast cancer by age 60 years
This translates to an absolute risk of 2.8 per 100 women
All Women Aged 50 Years in the General Population—Risk for Breast Cancer by Age 60 Years
American Cancer Society. Breast Cancer Facts and Figures 2001–2002. Available at: http://www.cancer.org/downloads/STT/BrCaFF2001.pdf.
In 100 women, 2.8 are at riskIn 100 women, 2.8 are at risk

Absolute Risk of Breast Cancer After 5 Years of HT
WHI results indicate a hazard risk for breast cancer of 1.24 (P < .001) after 5 years of HT use (a 24% increase in risk)
This translates into an absolute risk of 3.5 per 100 users
Risk of Breast Cancer by Age 60 Years After 5 Years of HT Use
(Assuming a 24% Increase in Risk)
3.5 of 100 women who are HT users are at risk 3.5 of 100 women who are HT users are at risk (<1 additional woman over baseline risk)(<1 additional woman over baseline risk)
3.5 of 100 women who are HT users are at risk 3.5 of 100 women who are HT users are at risk (<1 additional woman over baseline risk)(<1 additional woman over baseline risk)
American Cancer Society. Breast Cancer Facts and Figures 2001–2002. Available at: http://www.cancer.org/downloads/STT/BrCaFF2001.pdf; Chlebowski RT, et al. JAMA. 2003;289:3243-53.

Nonsignificant.Chlebowski RT, et al. JAMA. 2003;289:3243-53.
WHI: Risk of Invasive Breast Cancer in Women With and Without Prior HT Use
Prior HT Use
None
<5 Years
5 Years
Overall
% of Population
74.0
14.8
11.2
100
Hazard Ratio (95% CI)
0.1 0.5 1.0 4.02.0 6.0

Addressing Patients’ Breast Health Concerns
The WHI reported a small, increased risk of invasive breast cancer with an average of 5.6 years of E+P use
Most observational studies do not show an increased risk of breast cancer with HT use; some suggest a small increased risk with long-term HT use
Risk estimates from prospective, randomized trials and observational studies are similar
In the WHI, breast cancers in women assigned to E+P were somewhat larger and more likely to involve regional lymph nodes; other studies show that HT users have less aggressive, smaller tumors

Addressing Patients’ Breast Health Concerns continued
Positive family history of breast cancer is not a contraindication for HT
In observational studies, breast cancer survival rates are better in HT users
– Million Women Study reported greater risk of fatal breast cancer among HT users, however breast cancer survival rates were equivalent among HT users and nonusers
In breast cancer survivors, HT use has not been shown to worsen mortality or recurrence

HT-Related Breakthrough Bleeding All available continuous-combined E+P regimens are
associated with breakthrough bleeding– Less breakthrough bleeding with lower doses
Definitions and indices used to report bleeding patterns vary
– Most postmenopausal women will experience amenorrhea within 1 year of initiating therapy
– Women who are postmenopausal >3 years may experience less bleeding than recently menopausal women
Managing patient expectations about breakthrough bleeding is critical
Archer DF, Pickar JH. Climacteric. 2002;5:45-69; Archer DF, et al. Fertil Steril. 2001;75:1080-7; Archer DF, Pickar JH. Obstet Gynecol. 2000;96:899-905; Lerner S. Menopause. 1995;2:175-80.

Cumulative Amenorrhea Rates: CEE/MPAfor EE Population (n = 1555)
75.5
86.182.1
88.996.0
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10 11 12 13
Cycle
Pat
ien
ts (
%)
EE = Efficacy-evaluable population included women who recorded taking study medicationand completed all 13 cycles without missing data on bleeding.Archer DF, et al. Fertil Steril. 2001;75:1080-7.
0.45/2.50.625/2.5
0.45/1.50.3/1.5
Placebo
72.8
51.846.2
41.8
27.9
Women's HOPE Study

Patient Concerns Regarding Weight and HT
Changes Commonly Observed at Menopause
Weight gain
Increased central adiposity
HT Is Associated With
Lower body weight and BMI compared with nonusers
Less visceral adipose tissue
Similar weight increase to that observed with placebo
Espeland MA, et al. J Clin Endocrinol Metab. 1997;82:1549-56; Matthews KA, et al. Int J Obes Relat Metab Disord. 2001;25:863-73; Sites CK, et al. Metabolism. 2001;50:835-40.

0.0
0.5
1.0
1.5
2.0
2.5
Placebo CEE0.625 mg
CEE/MPA (con)0.625 mg/2.5 mg
CEE/MPA (cyc)0.625 mg/10 mg
CEE/MP (cyc)0.625 mg/200 µg
*P = .006 vs all active therapy groups; no differences were observed between E-only and E+P groups.Con = continuous regimen; cyc = cyclic regimen (progestin first 12 days of each cycle).Espeland MA, et al. J Clin Endocrinol Metab. 1997;82:1549-56.
Postmenopausal Estrogen/Progestin Intervention (PEPI) TrialW
eig
ht
Ch
ang
e (
kg) **
Body Weight Changes After 3 Years of Treatment

0
1
2
3
Placebon = 218
Treatment Groups
Mea
n C
han
ge
Fro
m B
asel
ine
(kg
)
0.625/2.5n = 241
0.45/1.5n = 228
0.625 mgn = 212
0.45 mgn = 231
0.3 mgn = 235
CEE CEE/MPA
Utian WH, Pickar JH. Obstet Gynecol. 2002;99(suppl):57S.
Mean Change in Weight After 13 CyclesWomen's HOPE Study
0.45/2.5n = 232
0.3/1.5n = 213

Section 3:
Importance of
Individualizing HT
Patient Management Issues in Menopause

Individualizing Patient Management With HT
Type of estrogen/progestin
Dose of estrogen/progestin
Type of regimen (cyclic vs continuous)
Metabolic profiles of hormone combinations
Flexibility of treatment
Experience with therapy
Patient satisfaction with therapy

Section 3a:
Characteristics of Estrogens
Patient Management Issues in Menopause

SteroidsSteroids
Native Native Synthetic Synthetic
Chemically synthesized Chemically synthesized from a natural material from a natural material such as soy, Mexican yamsuch as soy, Mexican yam 1717-estradiol (E-estradiol (E22)) EstroneEstrone Estrone sulfateEstrone sulfate Synthetic conjugated Synthetic conjugated estrogensestrogens Esterified estrogensEsterified estrogens EstriolEstriol
NaturalNaturalFound in NatureFound in Nature
SyntheticSyntheticLaboratory SynthesizedLaboratory Synthesized
Natural SourceNatural Source
No chemical No chemical modificationsmodifications CEECEE
Ethinyl estradiol (EE)Ethinyl estradiol (EE) DiethylstilbestrolDiethylstilbestrol
Classifications of Estrogens: Natural Versus Synthetic

Section 3b:
Characteristics of Progestins
Patient Management Issues in Menopause

Classification of ProgestinsSteroidsSteroids
NaturalNaturalFound in NatureFound in Nature
SyntheticSyntheticLaboratory SynthesizedLaboratory Synthesized
Pregnane DerivativesPregnane Derivatives• MPAMPA• Megestrol acetateMegestrol acetate• Cyproterone Cyproterone
acetateacetate• Chlormadinone Chlormadinone
acetateacetate• MedrogestoneMedrogestone• DydrogesteroneDydrogesterone
Structurally Related Structurally Related to Progesteroneto Progesterone
Structurally Related Structurally Related to Testosteroneto Testosterone
19-Norpregnane 19-Norpregnane DerivativesDerivatives
• Nomegestrol Nomegestrol acetateacetate
• DemegestoneDemegestone• TrimegestoneTrimegestone• PromegestonePromegestone• NesteroneNesterone
NonethinylatedNonethinylated• DienogestDienogest• DrospirenoneDrospirenone
EthinylatedEthinylated• NorethindroneNorethindrone• NorethynodrelNorethynodrel• LynestrenolLynestrenol• Norethindrone Norethindrone
acetate (NETA)acetate (NETA)• TiboloneTibolone• Ethynodiol acetateEthynodiol acetate• LevonorgestrelLevonorgestrel• DesogestrelDesogestrel• NorgestimateNorgestimate• GestodeneGestodene
Stanczyk FZ. Rev Endocr Metab Disord. 2002;3:211-24.
Native Native Synthetic Synthetic• ProgesteroneProgesterone

Percent Change From Baseline After 12 Months of Therapy*
Metabolic Effects of Oral E+P Regimens
*Data shown are from 4 different controlled clinical trials; †All doses are in mg/d.Lobo RA, et al. Fertil Steril. 2001;76:13-24; Activella™ (estradiol/norethindrone acetate tablets). Physician Package Insert; femhrt® (norethindrone acetate/ethinyl estradiol tablets). Product Information; Ortho-Prefest™ (estradiol/norgestimate) tablets. U.S. draft labeling physician package insert.
Regimen†
Total Cholesterol LDL-C HDL-C Triglycerides
CEE/MPA 0.625/2.5 –2.2 –9.3 11.2 32.8
CEE/MPA 0.45/1.5 –2.6 –6.7 9.7 24.8
EE/NETA 0.05/1 –7.0 –7.5 –6.7 12.1
E2/NETA 1/0.5 –10.5 –10.8 –12.4 2.2
E2/Norgestimate 1/0.09 –1.9 1.2 9.7 9.4

Endometrial Response to Sequential Versus Continuous E+P
Open-label, prospective study, 1312 women taking sequential E+P (with 10 days of progestin) and 921 not using any HT were given continuous E+P for 9 months
At baseline, sequential E+P was associated with complex hyperplasia (5.3%) and atypical hyperplasia (0.7%)
Continuous-combined E+P
– Was not associated with an increased risk of hyperplasia
– Converted the endometrium to normal in those with complex hyperplasia arising during sequential E+P
Sequential therapy was associated with a higher risk of endometrial hyperplasia than continuous therapy
Sturdee DW, et al. Br J Obstet Gynaecol. 2000;107:1392-400.

0
20
40
60
80
Nu
mb
er o
f P
atie
nts
Wit
h
Po
siti
ve B
iop
sies
*PEPI Trial
*Positive biopsies include simple hyperplasia, complex hyperplasia, atypia, or adenocarcinoma.con = continuous regimen; cyc = cyclic regimen (CEE daily, progestin first 12 days of each cycle).The Writing Group for the PEPI Trial. JAMA. 1996;275:370-5.
n = 119 119 118 120120
Placebo CEE CEE/MPA (con) CEE/MPA (cyc) CEE/MP (cyc)0.625 mg 0.625 mg/2.5 mg 0.625 mg/10 mg 0.625 mg/200 µg
33(2.5%)(2.5%)
7474(62%)(62%)
11(<1%)(<1%)
66(5%)(5%)
66(5%)(5%)
Endometrial Effects After 3 Years of HT

Section 3c:
Use of Low-Dose HT
Patient Management Issues in Menopause

Trend Toward Lower Doses
Accumulating evidence suggests that lower E+P doses may provide similar benefits with reduced side effects
Current guidelines from the FDA, ACOG, NAMS, and SOGC recommend the use of the lowest effective doses of E+P
Grimes DA, Lobo RA. Obstet Gynecol. 2002;100:1344-53.American College of Obstetricians and Gynecologists. ACOG News Release. Available at: http://www.acog.org/from_home/publications/press_releases/nr08-30-02.cfm. Accessed 12/18/02.North American Menopause Society. Amended Report from the NAMS Advisory Panel on Postmenopausal Hormone Therapy. Available at: http://www.menopause.org/news.html#advisory. Accessed 12/18/02.Society of Obstetricians and Gynaecologists of Canada (SOGC). Can Fam Physician. 2004;49:188-91.

Low- and Standard-Dose HT Preparations Available in the US
Oral (mg) Transdermal (mg)
Low-dose estrogen CEE 0.45CEE 0.30Esterified estrogens 0.30E2 0.50
E2 0.0375E2 0.0250
Standard-dose estrogen CEE 0.625Esterified estrogens 0.625Estropipate 0.625E2 1.0
E2 0.05
Low-dose estrogen + low-dose progestin
CEE 0.45/MPA 1.5CEE 0.30/MPA 1.5
Standard-dose estrogen + standard-dose or low-dose progestin
CEE 0.625/MPA 2.5CEE 0.625/MPA 5.0*E2 1.0/NETA 0.5E2 1.0/norgestimate 0.09†
EE 0.005/NETA 1.0
E2 0.05/NETA 0.25E2 0.05/NETA 0.25
*MPA 5.0 mg is used continuously or sequentially with CEE 0.625 mg; †Norgestimate is used intermittently with E2 1.0 mg.

0
25
50
75
1 2 3 4 5 6 7 8 9 10 11 12
Week
Effect of Low Doses of Transdermal Estrogen on Vasomotor Symptoms
Me
an
Ho
t F
lush
Fre
qu
en
cy(n
um
be
r p
er
we
ek)
*P < .05 at weeks 2-11.†P < .05 at week 2; P < .01 at weeks 3-12. n = 324.TS = transdermal system; E2-TS = estradiol 0.02 mg/day provided in one or two 7-day transdermal delivery systems.Speroff L, et al. Obstet Gynecol. 1996;88:587-92.
Placebo-TS
2 Placebo-TSs
E2-TS (0.02 mg/day)*
2 E2-TSs (0.04 mg/day)†

Effect of Various Transdermal Estrogen Doses on Spinal BMD
*P < .05 vs placebo.261 women (mean age, 52 years; mean time since menopause, 32 months) were randomized. Nonhysterectomized women (n = 100) received MPA 2.5 mg/day.McKeever C, et al. Clin Ther. 2000;22:845-57.
*
* **
*
* * *
** *
****
-4-3-2-101234567
0 26 52 78 104
Treatment Duration (week)
Ch
an
ge
in
BM
D
Fro
m B
as
elin
e (
%)
E2 0.1 mg/day
E2 0.05 mg/day
E2 0.0375 mg/day
E2 0.025 mg/day
Placebo

The Women’s Health, Osteoporosis, Progestin, Estrogen
(Women’s HOPE) Study

Women's HOPE Study
Methodology: prospective, randomized, double-blind, placebo-controlled, multicenter trial
Purpose: Investigate efficacy and safety of lower doses of CEE and CEE/MPA
Patients: 2673 healthy, postmenopausal women (40–65 years of age) with an intact uterus
Outcomes: vasomotor symptoms, vaginal atrophy, bleeding profile, endometrial hyperplasia, metabolic profile, and bone mineral density
Design
Utian WH, et al. Fertil Steril. 2001;75:1065-79.

Women's HOPE Study
A double-blind, double-dummy design was used to administer study medication.All groups received a calcium carbonate supplement (600 mg elemental calcium/day).Utian WH, et al. Fertil Steril. 2001;75:1065-79.
8 Treatment Groups
PlaceboCEE 0.625 mg
CEE 0.45 mg
CEE 0.3 mg
CEE 0.625 mg + MPA 2.5 mg
CEE 0.45 mg + MPA 2.5 mg
CEE 0.45 mg + MPA 1.5 mg
CEE 0.3 mg +MPA 1.5 mg

No significant differences between 8 treatment groups were observed. Women were 88% Caucasian, 6% African American, 4% Hispanic, 2% Asian, and <1% Native American, Arabic, or “other.”Utian WH, et al. Fertil Steril. 2001;75:1065-79.
Demographic and Baseline Characteristics
Total (n = 2673) Mean ± SD
Age (years)
Age at menopause (years)
Years since menopause
Weight (kg)
BMI (kg/m2)
53.3 ± 4.9
48.5 ± 4.3
4.7 ± 4.2
65.5 ± 8.7
24.4 ± 2.8
Women's HOPE Study

0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9 10 11 12
Week
Ad
jus
ted
Me
an
Da
ily N
um
be
r*0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9 10 11 12
Week
Ad
jus
ted
Me
an
Da
ily N
um
be
r* 0.6250.450.3
Placebo
0.45/2.50.625/2.5
0.45/1.50.3/1.5
Placebo
*Adjusted for baseline.Mean hot flushes at baseline = 12.3 (range 11.3–13.8). Analyses included women who recorded taking study medication and had at least 7 moderate-to-severe flushes/week or at least 50 flushes per week at baseline.Utian WH, et al. Fertil Steril. 2001;75:1065-79. Used with permission.
Change in Number of Hot Flushes Over 12 Weeks (n = 241)
Women's HOPE Study

0.0
0.5
1.0
1.5
2.0
2.5
1 2 3 4 5 6 7 8 9 10 11 12
Week
Me
an
Se
ve
rity
Hot flush severity: 1 = mild, 2 = moderate, 3 = severe. Mean hot flush severity at baseline = 2.3 (range 2.2–2.4).EE = Efficacy-evaluable population included women who recorded taking study medication and had at least 7 moderate-to-severe flushes/week or at least 50 flushes per week at baseline.Utian WH, et al. Fertil Steril. 2001;75:1065-79. Used with permission.
0.0
0.5
1.0
1.5
2.0
2.5
1 2 3 4 5 6 7 8 9 10 11 12
Week
Me
an
Se
ve
rity
Placebo 0.6250.450.3
0.45/1.5
0.625/2.5Placebo
0.45/2.5
0.3/1.5
Changes in Severity of Hot Flushes Over 12 Weeks (n = 241)
Women's HOPE Study

Women's HOPE StudyImprovement in Vaginal Maturation Index
Compared With Baseline and Placebo*
*P < .05 vs baseline and placebo for all active treatment groups at all time points; †P < .05 vs CEE 0.625Utian WH, et al. Fertil Steril. 2001;75:1065-79.
Su
per
fici
al C
ells
(%
),
Med
ian
Ch
ang
e fr
om
Bas
elin
e
0
5
10
15
20
25Cycle 6
Cycle 13
Treatment Groups
0.625 mg 0.625/2.5 mg
0.45 mg 0.45/2.5 mg
0.45/1.5 mg
0.3 mg 0.3/1.5 mg
PlaceboCEE CEE/MPA
†
† †
Median Change = 0

Cumulative Amenorrhea Rates: CEE/MPAfor EE Population (n = 1555)
75.5
86.182.1
88.996.0
0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10 11 12 13
Cycle
Pat
ien
ts (
%)
EE = Efficacy-evaluable population included women who recorded taking study medicationand completed all 13 cycles without missing data on bleeding.Archer DF, et al. Fertil Steril. 2001;75:1080-7.
0.45/2.50.625/2.5
0.45/1.50.3/1.5
Placebo
72.8
51.846.2
41.8
27.9
Women's HOPE Study

0
20
40
60
80
100
1 2 3 4 5 6 7 8 9 10 11 12 13
Cycle
Pat
ien
ts (
%)
0.45/2.50.625/2.5
0.45/1.50.3/1.5
Placebo
EE = Efficacy-evaluable population included women who recorded taking study medicationand completed all 13 cycles without missing data on bleeding.Archer DF, et al. Fertil Steril. 2001;75:1080-7.
Cumulative No Bleeding Rates: CEE/MPAfor EE Population (n = 1555)
Women's HOPE Study
98.894.593.891.886.3
53.9
64.9
66.7 69.8
89.6

LDL CholesterolWomen's HOPE Study
Mea
n P
erce
nt
Ch
ang
eF
rom
Bas
elin
e
-15
-10
-5
0
5
*†*† *†
*†
*†
*†
*† *†
†
*†
*†
*†*† *†
Cycle 6
Cycle 13
Treatment Groups
0.625 mg 0.625/2.5 mg
0.45 mg 0.45/2.5 mg
0.45/1.5 mg
0.3 mg 0.3/1.5 mg
PlaceboCEE CEE/MPA
*P < .05 vs baseline.†P < .05 vs placebo.Lobo RA, et al. Fertil Steril. 2001;76:13-24.
*

Mea
n C
han
ge
Fro
m B
asel
ine
(%)
0
2
4
6
8
10
12
14
16
18
20
*†‡
*‡
*†
*†
*†
*†
*†
*†‡
*†
*†‡*†
*†
*‡ *‡
Treatment Groups
0.625 mg 0.625/2.5 mg
0.45 mg 0.45/2.5 mg
0.45/1.5 mg
0.3 mg 0.3/1.5 mg
PlaceboCEE CEE/MPA
*P < .05 vs baseline.†P < .05 vs placebo.‡P < .05 vs comparable CEE alone.Lobo RA, et al. Fertil Steril. 2001;76:13-24.
HDL CholesterolWomen's HOPE Study
Cycle 6
Cycle 13

Mea
n C
han
ge
Fro
m B
asel
ine
(%)
0
5
10
15
20
25
30
35
40
45
*†
*†
*†*†
*†
*‡*† *
*
*†
*‡
*†
* *
Treatment Groups
0.625 mg 0.625/2.5 mg
0.45 mg 0.45/2.5 mg
0.45/1.5 mg
0.3 mg 0.3/1.5 mg
PlaceboCEE CEE/MPA
*
*P < .05 vs baseline.†P < .05 vs placebo.‡P < .05 vs comparable CEE alone.Lobo RA, et al. Fertil Steril. 2001;76:13-24.
TriglyceridesWomen's HOPE Study
Cycle 6
Cycle 13

-4
-3
-2
-1
0
1
2
3
4
Baseline 6 mo 12 mo 18 mo 24 mo
CEE 0.625/MPA 2.5 mg/dayCEE 0.45/MPA 2.5 mg/dayCEE 0.45/MPA 1.5 mg/dayCEE 0.3/MPA 1.5 mg/dayPlacebo
-4
-3
-2
-1
0
1
2
3
4
Baseline 6 mo 12 mo 18 mo 24 mo
Me
an
Ch
an
ge
Fro
m B
as
eli
ne
(%
)
CEE 0.625 mg/dayCEE 0.45 mg/day
CEE 0.3 mg/dayPlacebo
CEE CEE/MPA
Intent-to-treat population only.Lindsay R, et al. JAMA. 2002;287:2668-76.
Changes in Spine BMDWomen's HOPE Study

-4
-3
-2
-1
0
1
2
3
4
Baseline 6 mo 12 mo 18 mo 24 mo
Me
an
Ch
an
ge
Fro
m B
as
eli
ne
(%
)
CEE 0.625 mg/dayCEE 0.45 mg/day
CEE 0.3 mg/dayPlacebo
-4
-3
-2
-1
0
1
2
3
4
Baseline 6 mo 12 mo 18 mo 24 mo
CEE 0.625/MPA 2.5 mg/dayCEE 0.45/MPA 2.5 mg/dayCEE 0.45/MPA 1.5 mg/dayCEE 0.3/MPA 1.5 mg/dayPlacebo
Intent-to-treat population only.Lindsay R, et al. JAMA. 2002;287:2668-76.
Changes in Total Hip BMDWomen's HOPE Study
CEE CEE/MPA

Pickar JH, et al. Fertil Steril. 2003;80:1234-40.
Endometrial Hyperplasia Rates After 1 and 2 Years of Low-Dose E+P
Women's HOPE Study
0
5
10
15
20
25
30
Hy
per
pla
sia
Ra
te (
%)
0.000.000.000.000.000.00
Year 1
Year 2
Treatment Groups
0.625 mg 0.625/2.5 mg
0.45 mg 0.45/2.5 mg
0.45/1.5 mg
0.3 mg 0.3/1.5 mg
PlaceboCEE CEE/MPA

0
2
4
6
8
10
12
14
16
Hy
per
pla
sia
Ra
te A
fter
1
2 M
on
ths
(%
)
n = 1176.P < .001 for all continuous-combined groups vs unopposed E2.Kurman RJ, et al. Obstet Gynecol. 2000;96:373-9.
Endometrial Hyperplasia Rates With Lower Doses of NETA
E2 1 mg E2 1 mg/NETA0.1 mg
E2 1 mg/NETA0.25 mg
E2 1 mg/NETA0.5 mg

Low-Dose HT: Conclusions Research findings demonstrate that lower doses of
estrogen and progestin
– Relieve vasomotor symptoms and prevent vaginal atrophy
– Are associated with a reduced incidence of endometrial bleeding, especially in the early months of therapy
– Provide effective endometrial protection
– Prevent early postmenopausal bone loss Lower-dose regimens provide clinicians and patients
with expanded options for individualizing HT E alone at lower dosages for longer durations may be
associated with increased rates of endometrial hyperplasia

Section 3d:
Non-Oral HT Formulations
Patient Management Issues in Menopause

Non-Oral Estrogen and Progestin Formulations
Estrogen
– Estradiol ring
– Nasal estradiol
– Estradiol gel
– Vaginal estrogen
Progestin
– Levonorgestrel IUD/IUS
– Vaginal progesterone gel
– Trimegestone
– Lotion

Section 4:
Non-HT Alternatives for
Menopausal Symptoms
Patient Management Issues in Menopause

Non-HT Alternatives for Menopausal Health Issues
Lifestyle modifications
Menopausal complaints
– Non-prescription therapies
– Prescription therapies
Osteoporosis therapies
Lipid-lowering drugs
Neurocognitive therapies

1Eisenberg DM, et al. JAMA. 1998;280:1569-75; 2Rafferty AP, et al. Am J Public Health. 2002;92:1598-600.Newton KM, et al. Obstet Gynecol. 2002;100:18-25.
Scope of Alternative Medicine Use in the US
19901 19972 20013
Adults surveyed 1539 2055 3764
Utilization prevalence (%) 33.8 42.1 49.7
Number of visits (millions) 427 629 —
Covered by insurance (%) 36 42 —

n = 886 (ages 45 to 65 years).Reprinted from Newton KM, et al. Use of alternative therapies for menopause symptoms: results of a population-based survey. Obstet Gynecol. 2002;100:18-25, ©2002, with permission from the American College of Obstetricians and Gynecologists.
Proportion of Women Using Alternative Therapies for Any Reason and for
Menopausal Symptoms
0 10 20 30 40 50
Ever Used
Using Now
Used for Menopausal Symptoms
Herbal Remedies
Chiropractic
Massage Therapy
Dietary Soy Products
Acupuncture
Homeopathic Physician Visit
Herbalist Visit
Relaxation or Stress Management

1McTiernan A, et al. JAMA. 2003;290:1331-6; 2Thune I, et al. N Engl J Med. 1997;336:1269-75; 3Li CI, et al. Cancer Epidemiol Biomark Prev. 2003;12:1061-6; 4Huang Z, et al. JAMA. 1997;278:1407-11; 5Morimoto LM, et al. Cancer Causes Control. 2002;13:741-51; 6Reynolds P, et al. J Natl Cancer Inst. 2004;96:29-37.
Lifestyle Choices That Increase Breast Cancer Risk
Lack of exercise1,2
– Recreational exercise 1.25–2.5 hours per week of brisk walking,
RR = 0.82 (95% CI, 0.68–0.97)1
4 hours per week, RR = 0.63 (95% CI, 0.42–0.95)2
Alcohol3
– RR = 1.3 (95% CI, 1.0–1.5; ever-use of alcohol over the past 20 years)
Obesity4,5
– RR = 1.99 for never-users of HT who gained >20 kg (95% CI, 1.43–2.76)4
– RR = 2.52 for BMI >31.1 kg/m2 (95% CI, 1.62–3.93)5
Cigarette smoking6
– HR = 1.32 (95% CI, 1.10–1.57; relative to all never smokers)

0
2
4
6
8
10
12
14
16
Rel
ativ
e R
isk
Magnitude of Various Risk Factors for Breast Cancer
Family History
(2 Members)
HT for 5 Years
ObesityBMI >31.1 kg/m2
Family History
(1 Member)
Age at Menarche (Delayed)
Huang Z, et al. JAMA. 1997;278:1407-11; Thune I, et al. N Engl J Med. 1997;336:1269-75; Longnecker MP, et al. Cancer Epidemiol Biomark Prev. 1995;4:721-5; McTiernan A, et al. JAMA. 2003;290:1331-6.
Lack of Exercise

Non-HT Alternatives for Vasomotor Symptoms
Lifestyle changes (limited effectiveness)
– Cooling body core temperature
– Exercise
– Avoiding hot and spicy foods
– Pace respirations
– Relaxing activities
North American Menopause Society. Menopause. 2004;11:11-33; Kronenberg F, Fugh-Berman A. Ann Intern Med. 2002;137:805-13; Huntley AL, Ernst E. Menopause. 2003;10:465-76.

Non-Prescription Remedies
Some alternative therapies may provide relief of mild vasomotor symptoms for some women
– Phytoestrogens/isoflavones Dietary or supplements (soy-derived) Red clover
– Black cohosh
– Vitamin E – not clinically significant Studies show no effect compared with placebo for
Dong quai Ginseng Evening primrose oil
North American Menopause Society. Menopause. 2004;11:11-33; Kronenberg F, Fugh-Berman A. Ann Intern Med. 2002;137:805-13; Huntley AL, Ernst E. Menopause. 2003;10:465-76.

Alternative Non-Prescription Therapies: Concerns
Aggressive marketing generates inquiries and use Side effects and drug interactions are not well known
but clearly occur Lack long-term safety and efficacy data When possible, providers should record use and
amounts Long-term, adequately powered, randomized,
placebo-controlled, clinical trials with defined entry criteria are needed
– FDA efficacy trials require a minimum of 7 to 8 per day or 50 to 60 per week moderate to severe hot flushes

ER = estrogen receptor.Scheiber MD, Rebar RW. Menopause. 1999;6:233-41.
Phytoestrogens
Nonsteroidal plant-derived compounds that bind to ERs
– Some bind weakly to ER– Many bind strongly to ER
Three main classes
– Isoflavones (genistein and daidzein): soybeans, soy products, lentils, chickpeas, red clover
– Lignans (enterodiol and enterolactone): wide variety of fruits, vegetables, and cereals; concentrated in flaxseed
– Coumestans (coumestrol): bean sprouts, fodder crops (alfalfa)

Dietary Phytoestrogens/Isoflavones 11 studies examining soy or isoflavone supplementation Only 3 of 8 studies lasting longer than 6 weeks showed
significant improvement in hot flushes
– Longest study (24 weeks) to date showed no benefit for hot flushes
Published data show only modest effects; most benefits vanish after 6 weeks
Symptoms decreased in all treatment groups, including placebo, by 50%–60%
Comparisons are difficult because of variations in products, dosages, scoring systems, and menopausal status
Red clover (two 3-month, double-blind, small, controlled trials, >3 hot flushes per day)
– No significant effect compared with placeboNorth American Menopause Society. Menopause. 2004;11:11-33; Kronenberg F, Fugh-Berman A. Ann Intern Med. 2002;137:805-13.

Black Cohosh (Cimicifuga racemosa)
NIH-funded, large, randomized, prospective, 2-year trial ongoing
– Preliminary data fails to show binding to ER
– Binding to serotonin receptor noted
4 randomized trials using placebo and/or estrogen treatment arm
– 3 of the 4 trials found black cohosh to be beneficial (only 1 of these 3 used placebo as a control)
– Currently, longest trial is 6 months
Kronenberg F, Fugh-Berman A. Ann Intern Med. 2002;137:805-13.

Design of Trials Evaluating Black Cohosh for Menopausal Symptoms
Huntley AL, Ernst E. Menopause. 2003;10:465-76.1Warnecke G. Medwelt. 1985;36:871-4; 2Stoll W. Therapeutikon. 1987:1-15; 3Lehmann-Willenbrock VE, Reiedel HH. Zentrabl Gynakol. 1988;110:611-8; 4Jacobson JS, et al. J Clin Oncol. 2001;19:2739-45.
Study Design Participants Active Treatment (n) Control (n)
2 week, open-label1
n = 60, with climacteric complaints
40 drops of black cohosh twice daily (4 mg of 27-deoxyacetin) (20)
0.6 mg/d CE (20)2 mg diazepam
daily (20)
12 week, double-blind2
n = 80 , with 3 hot flushes daily
4 tablets daily of black cohosh (4 mg of 27-deoxyacetin) (26)
Low-dose E, 0.625 mg/d (29)
Placebo (20)
24 week, open-label3
n = 60, hysterec-tomized, with 1 ovary & climacteric symptoms (<40 years of age)
4 tablets of black cohosh (4 mg of 27-deoxyacetin) (15)
Estriol 1-mg tablet daily (15)
CE 1.25 mg tablet daily (15)
E+P sequential therapy, 1 tablet daily (15)
60 day, double-blind4
n = 85 breast cancer patients with menopausal symptoms
1 black cohosh tablet twice daily with food (42)
Placebo (43)

KI = Kupperman Index; HAMA = Hamilton Anxiety Scale; NS = not significant.Huntley AL, Ernst E. Menopause. 2003;10:465-76.1Warnecke G. Medwelt. 1985;36:871-4; 2Stoll W. Therapeutikon. 1987:1-15; 3Lehmann-Willenbrock VE, Reiedel HH. Zentrabl Gynakol. 1988;110:611-8; 4Jacobson JS, et al. J Clin Oncol. 2001;19:2739-45.
Results of Trials Evaluating Black Cohosh for Menopausal Symptoms
Reference ResultsWarnecke (1985)1 Black cohosh produced “greatest
improvement” in all measures, but no actual data given
Stoll (1987)2 Black cohosh produced greatest improvement in KI (<15) & HAMA (P < .01) compared with placebo
Lehmann-Willenbrock (1988)3 Improvement in all groups (black cohosh, estriol, CE, and E+P; P < .01) for most treatments at most times; no difference between groups
Jacobson (2001)4 Both black cohosh and placebo groups improved; NS difference between groups

Topical Progesterone Therapies
Wild yam cream contains progesterone precursors (humans lack enzyme to metabolize)
Differential rates with minimal absorption of progesterone-containing creams
3 studies have shown that serum levels of progesterone are insufficient to prevent estrogenic stimulation of the endometrium1-3
Mixed results in randomized, placebo-controlled, hot-flush trials4,5
1Cooper A, et al. Lancet. 1998;351:1255-6; 2Wren BG, et al. Lancet. 1999;354:1447-8; 3Lewis JG, et al. Maturitas. 2002;41:1-6; 4Komesaroff PA, et al. Climacteric. 2001;4:144-50; 5Leonetti HB, et al. Obstet Gynecol. 1999;94:225-8.

Progestins for the Treatment of Vasomotor Symptoms
North American Menopause Society. Menopause. 2004;11:11-33.
Progestin N Dose Efficacy
MPA Oral 27 20 mg/d 25.9%–34.5% in hot flushes
MPA Depot 21 100 mg BID 67%–80% in hot flushes
Depo 71 500 mg + 40 mg megestrol
95% in hot flushes
Megestrol 15 500 mg weekly 69% in hot flushes
Progestin 42 150 mg 85% vs21% placebo

Nonhormonal Prescription Therapies
Antidepressants– SSRI/SNRI therapy– Venlafaxine– Paroxetine– Fluoxetine
Anti-convulsants– Gabapentin
Anti-hypertensives– Clonidine (patch or pill) and methyldopa
Sedatives– Bellergal

0
20
40
60
80
100
Baseline 1 2 3 4
Clinical Trials of Median Hot Flush Score Reduction in Breast Cancer Patients
NOTE: These data are not from head-to-head trials.Loprinzi CL, et al. Lancet Oncol. 2001;2:199-204.
Week
Med
ian
Sco
re
Placebo (n = 347)Soy (n = 66)Clonidine (n = 75)Fluoxetine (n = 20)Vitamin E (n = 57)
Venlafaxine (n = 45)
Megestrol (n = 74)

Nonhormonal Prescription Therapies: Venlafaxine
*Decrease of hot flush score.Schober CE, Ansani NT. Ann Pharmacother. 2003;37:1703-7.1Loprinzi CL, et al. J Clin Oncol. 1998;16:2377-81; 2Loprinzi CL, et al. Lancet. 2000;356:2059-63; 3Barton D, et al. Oncol Nurs Forum. 2002;29:33-40.
Study Design and Duration Population (n)
Venlafaxine Dosage Efficacy Results P-Value
Prospective pilot; 5 weeks1
Women with history of breast cancer or current treatment, and men with androgen deficiency, (28)
12.5 mg bid for 4 weeks
>50% decrease in overall frequency in 54% of patients
<.0002
Double-blind, placebo-controlled; 4 weeks, with open-label 8-week period following2
Women with history of or fear of breast cancer, tamoxifen use, or reluctance to take HT (229)
Placebo, 37.5 mg qd, 75 mg qd, 150 mg qd
From baseline: 27%37%61%61%
.01*
.01*NS
Open-label, continuation phase; 8 weeks3
Women with history of breast cancer or current treatment (102)
37.5 mg qd,75 mg qd,112.5 mg qd,150 mg qd
From baseline: 26%60%60%60%
Not reported

Nonhormonal Prescription Therapies: Fluoxetine
Randomized, double-blind, placebo-controlled, 8-week crossover trial (two 4-week periods) to evaluate the efficacy of fluoxetine (20 mg/day) for vasomotor symptoms
N = 81 women with a history of breast cancer or perceived high risk of breast cancer
– Could be on stable does of tamoxifen or raloxifene
At least 14 hot flushes per week 20% improvement compared with placebo (P = .02)
Loprinzi CL, et al. J Clin Oncol. 2002;20:1578-83.

Nonhormonal Prescription Therapies: Paroxetine
165 women, 18 years of age or older Experiencing 2 to 3 hot flushes per day
Stearns V, et al. JAMA. 2003;289:2827-34.
Doses (n)Median Reduction in Hot Flush Composite Score
12.5 mg (51) 62.2% (P = .007)
25 mg (58) 64.6% (P = .03)
Placebo (56) 37.8%

Nonhormonal Prescription Therapies: Gabapentin
12-week, double-blind study
– Dose = 900 mg/d
– 7 hot flushes per day at baseline
– 6-week screening Hot flush composite score decreased 54% vs 31%
for placebo (P = .01) 50% reported at least 1 adverse event (eg,
dizziness, lightheadedness, palpitations, rash, somnolence) vs 27.6% in placebo group; 13.3% withdrew
Guttuso T, Jr, et al. Obstet Gynecol. 2003;101:337-45.

Nonhormonal Prescription Therapies: Clonidine
Randomized, double-blind, placebo-controlled clinical trial1
– 0.1 mg/d oral
– 194 breast cancer patients taking tamoxifen
– Randomized, placebo-controlled
– Hot flush frequency decreased by 38% after 8 weeks vs 24% with placebo
– Side effects: dry mouth, drowsiness, constipation, and dizziness2
1Pandya KJ, et al. Ann Intern Med. 2000;132:788-93.2Goldberg RM, et al. J Clin Oncol. 1994;12:155-8.

Clinical Management of Vasomotor Symptoms
For mild vasomotor symptoms– Encourage lifestyle changes– Non-prescription remedies tested only short term
dietary isoflavones black cohosh vitamin E
– Discuss risk-benefits of HT For moderate to severe vasomotor symptoms
– Systemic HT remains therapeutic standard and only FDA-approved treatment for moderate to severe symptoms
– Progestins effective; however, large doses required Early studies suggest limited efficacy with some SSRIs and
gabapentin; more studies needed, side effects of concern
Adapted from North American Menopause Society. Menopause. 2004;11:11-33.

*All therapies include calcium supplementation; †Treatment time is 2 to 3 years; ‡Dose effect; §Long-term safety (>7 years) is unknown.GI = gastrointestinal.American Association of Clinical Endocrinologists. Endocr Pract. 2001;7:293-312. Osteoporosis Methodology Group and the Osteoporosis Research Advisory Group. Endocrine Rev. 2002;23:496-578.
Current Management of Osteoporosis: A Review
Therapy*
Decreases Vertebral
Fracture RatesDecreases Hip Fracture Rates
Approximate Increases in
BMD (%)†
Most Common Side Effect
HT Yes‡ Yes 5–6 Breakthrough bleeding
Alendronate§ Yes‡ Yes 5–8 Gastric ulceration
Risedronate§ Yes Yes 5–6 Upper GI symptoms
Raloxifene§ Yes No 1–2 Hot flushes
Calcitonin Yes No 1–2 Nasal irritation
PTH Yes No 9 Leg cramps; dizziness

Non-pharmacological treatment calcium: 1500 mg/dayVitamin D: 800 IU/day
Physical activity: >30 min at least 3 times a week
Without fragility fracture With fragility fracture
Vasomotor symptoms
Yes No
HT
Alendronate,risedronate,raloxifene,calcitonin
Calcitonin,etidronate,
HT
1st choice
2nd choice
Osteoporosis Prevention and Treatment
Alendronate, risedronate,
and raloxifene
Adapted from Brown JP, Josse RG. Reprinted from CMAJ 12 Nov 2002:167(suppl): Page S22, by permission of the publisher. © 2002 Canadian Medical Association.
Vasomotor symptoms
Yes No
Calcitonin,etidronate,
HT
Alendronate, risedronate,
and raloxifene
Calcitonin, raloxifene,etidronate
HT ± alendronate or risedronate

Section 5:
Patient Counseling Strategies
Patient Management Issues in Menopause

Counseling Topics for Patients Considering HT
Review the risks and benefits of HT
Discuss the probability of early bleeding while receiving continuous-combined E+P
Review other potential side effects
Provide information about HT and breast health
Emphasize that HT use does not cause weight gain
Obtain informed consent

Counseling Topics for Patients Who Decline or Discontinue HT
Asymptomatic obese women may still require progestational therapy
Urogenital atrophy will develop
Need to increase surveillance for osteoporosis and/or consider alternative osteoporosis regimens
Hot flushes and night sweats may return after discontinuation

Informed Consent Is a Process, Not a Form
Informed Consent Discussions Should Include The diagnosis and the nature of the condition The nature and purpose of the recommended
treatment or procedure, including its risks and potential complications
All reasonable alternative treatments or procedures, including the option of taking no action, and the risks of each option
The relative probability of success for the treatment or procedure
The American College of Obstetricians and Gynecologists. Professional Liability and Risk Management: A Resource for OB-GYNs in Training and in Practice. Washington DC; 2002.

What to Remember When Obtaining Informed Consent
Avoid medical jargon; pay close attention to the patient’s language proficiency
Try to make sure there is true understanding by having information repeated back to you
Allow enough time for questions and answers
Make notations about high-risk issues discussed
The American College of Obstetricians and Gynecologists. Professional Liability and Risk Management: A Resource for OB-GYNs in Training and in Practice. Washington DC; 2002.

Counseling Women About HT
Document reasons for considering HT (eg, use quality-of-life questionnaire)
Review annually indications for HT
Explain benefits of short-term HT use will often outweigh risks
Emphasize that risks attributable to HT in the WHI were low
American College of Obstetricians and Gynecologists. ACOG News Release. Available at: http://www.acog.org/from_home/publications/press_releases/nr07-09-02.cfm. Accessed 8/19/02.Writing Group for the Women’s Health Initiative Investigators. JAMA. 2002;288:321-33.

Counseling on Duration of HT Use
Consider continuing therapy (possibly lower dose) if initial indication was vasomotor symptoms
Excess cardiovascular events occurred in the first 2 years in women (average age, 63 years) in the WHI trial
Breast cancer risk was not increased with <5 years of HT use in the WHI trial
– After 5 years, HT was associated with a slight increased risk (<0.1% per year)
VTE risk continues for duration of therapy (<0.2% per year)
Bone protection is afforded by continuing therapy
Individualized Therapy