Embed Size (px)
Citation preview
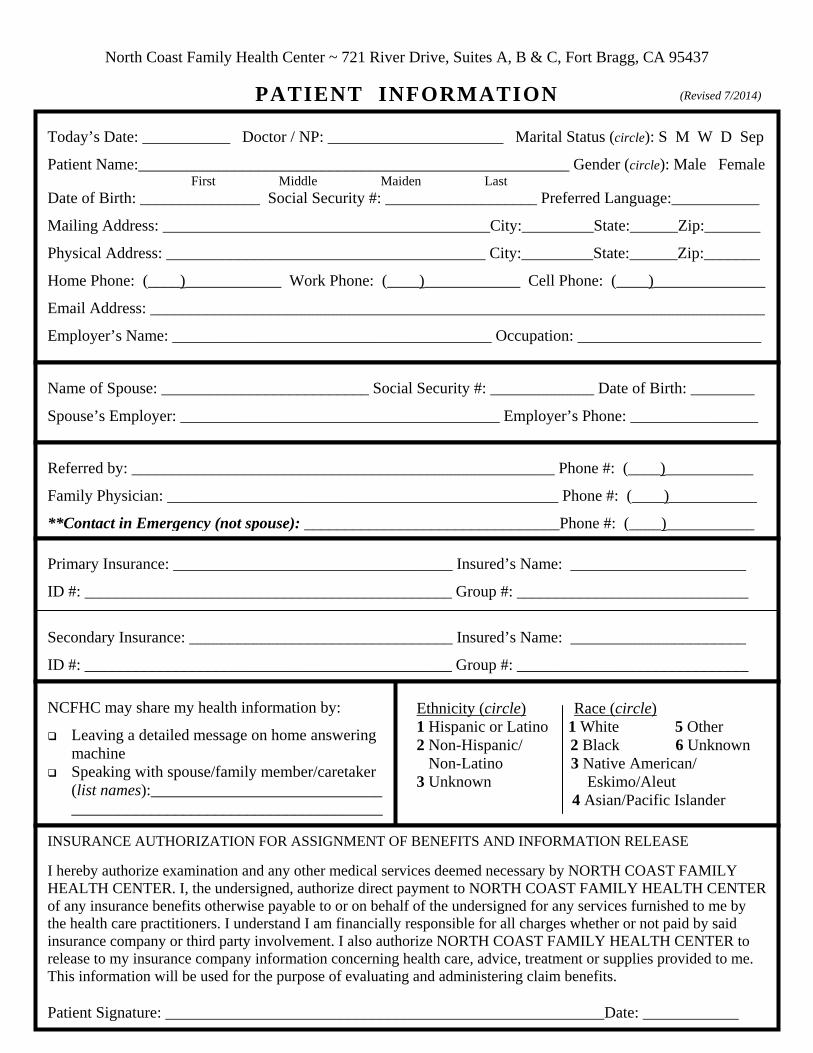
North Coast Family Health Center ~ 721 River Drive, Suites A, B & C, Fort Bragg, CA 95437
PATIENT INFORMATION
Today’s Date: ___________ Doctor / NP: ______________________ Marital Status (circle): S M W D Sep
Patient Name:______________________________________________________ Gender (circle): Male Female First Middle Maiden Last
Date of Birth: _______________ Social Security #: ___________________ Preferred Language:___________
Mailing Address: _________________________________________City:_________State:______Zip:_______
Physical Address: ________________________________________ City:_________State:______Zip:_______
Home Phone: (____)____________ Work Phone: (____)____________ Cell Phone: (____)______________
Email Address: _____________________________________________________________________________
Employer’s Name: ________________________________________ Occupation: _______________________
Name of Spouse: __________________________ Social Security #: _____________ Date of Birth: ________
Spouse’s Employer: ________________________________________ Employer’s Phone: ________________
Referred by: _____________________________________________________ Phone #: (____)___________
Family Physician: _________________________________________________ Phone #: (____)___________
**Contact in Emergency (not spouse): ________________________________Phone #: (____)___________
Primary Insurance: ___________________________________ Insured’s Name: ______________________
ID #: ______________________________________________ Group #: _____________________________
Secondary Insurance: _________________________________ Insured’s Name: ______________________
ID #: ______________________________________________ Group #: _____________________________
NCFHC may share my health information by:
Leaving a detailed message on home answering machine Speaking with spouse/family member/caretaker
(list names):____________________________________________________________________
INSURANCE AUTHORIZATION FOR ASSIGNMENT OF BENEFITS AND INFORMATION RELEASE
I hereby authorize examination and any other medical services deemed necessary by NORTH COAST FAMILY HEALTH CENTER. I, the undersigned, authorize direct payment to NORTH COAST FAMILY HEALTH CENTER of any insurance benefits otherwise payable to or on behalf of the undersigned for any services furnished to me by the health care practitioners. I understand I am financially responsible for all charges whether or not paid by said insurance company or third party involvement. I also authorize NORTH COAST FAMILY HEALTH CENTER to release to my insurance company information concerning health care, advice, treatment or supplies provided to me. This information will be used for the purpose of evaluating and administering claim benefits.
Patient Signature: _______________________________________________________Date: ____________
Ethnicity (circle) Race (circle) 1 Hispanic or Latino 1 White 5 Other 2 Non-Hispanic/ 2 Black 6 Unknown Non-Latino 3 Native American/ 3 Unknown Eskimo/Aleut
4 Asian/Pacific Islander
(Revised 7/2014)
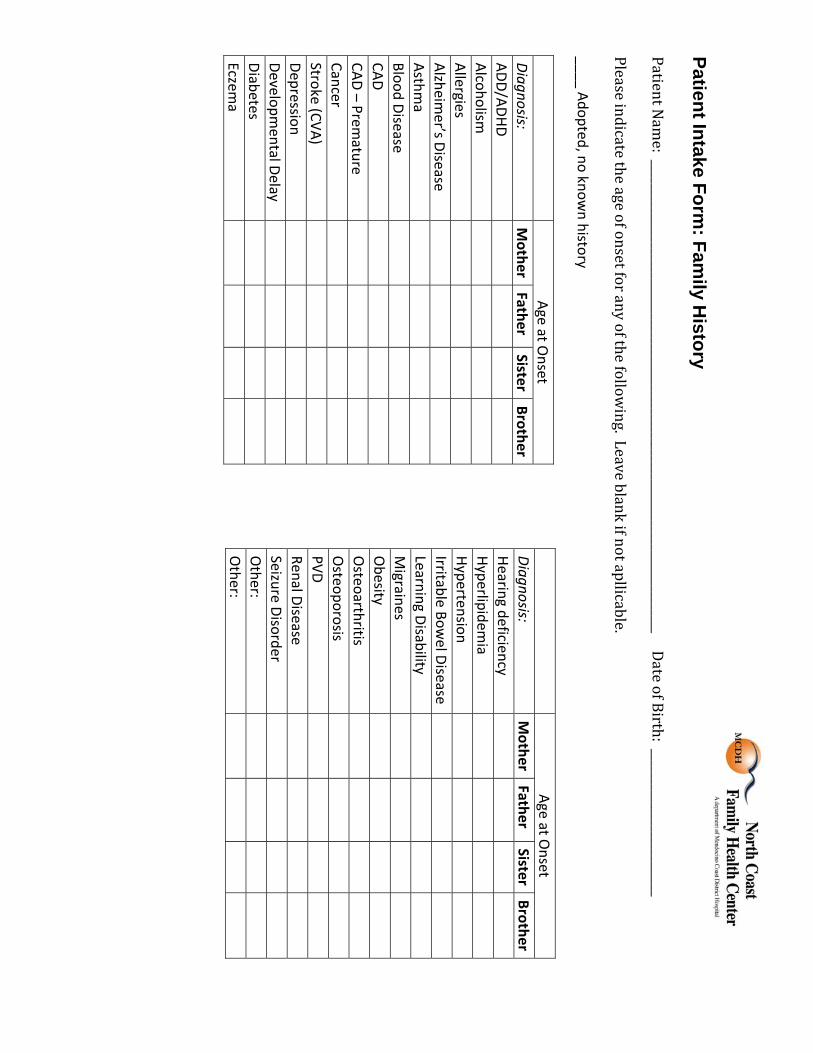
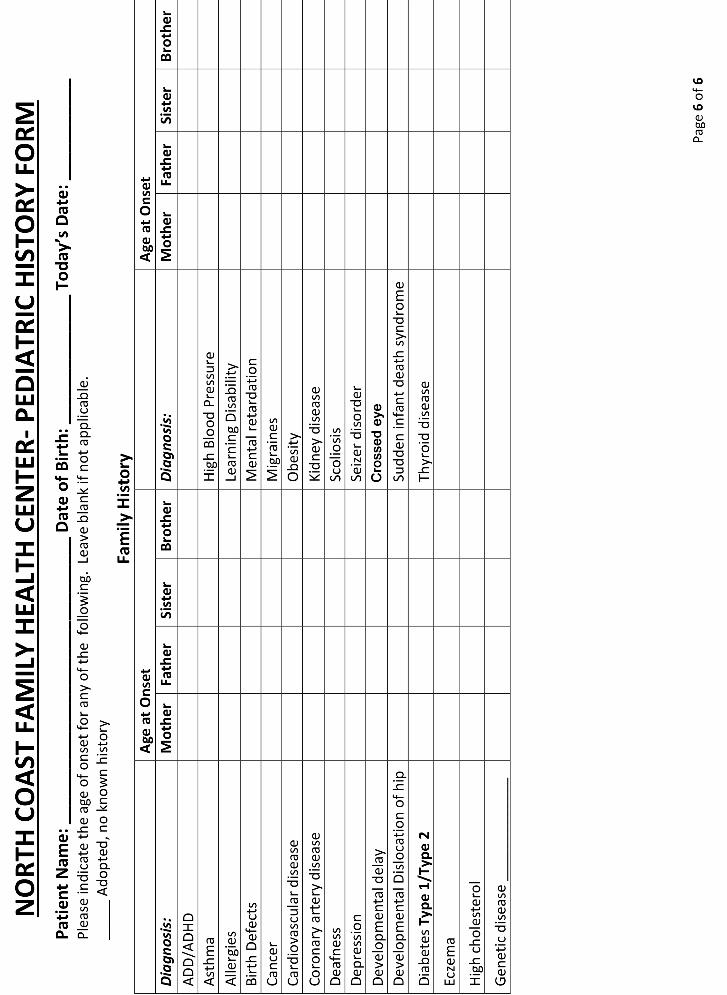
Patient Intake Form: Fam
ily History
PatientN
ame:________________________________________________________________________________DateofBirth:_________________________
Pleaseindicatetheageofonsetforanyofthefollowing.Leaveblankifnotapllicable.
____ Adopted, no known history
Age at O
nset Diagnosis:
Mother
Father Sister
BrotherADD/ADHD Alcoholism
Allergies
Alzheimer’s Disease
Asthma
Blood Disease
CAD
CAD – Premature
Cancer
Stroke (CVA)
Depression
Developm
ental Delay
Diabetes
Eczema
Age at O
nset Diagnosis:
Mother
Father Sister
BrotherHearing deficiency Hyperlipidem
ia Hypertension
Irritable Bowel Disease
Learning Disability
Migraines
Obesity
Osteoarthritis
Osteoporosis
PVD
Renal Disease
Seizure Disorder
Other:
Other:
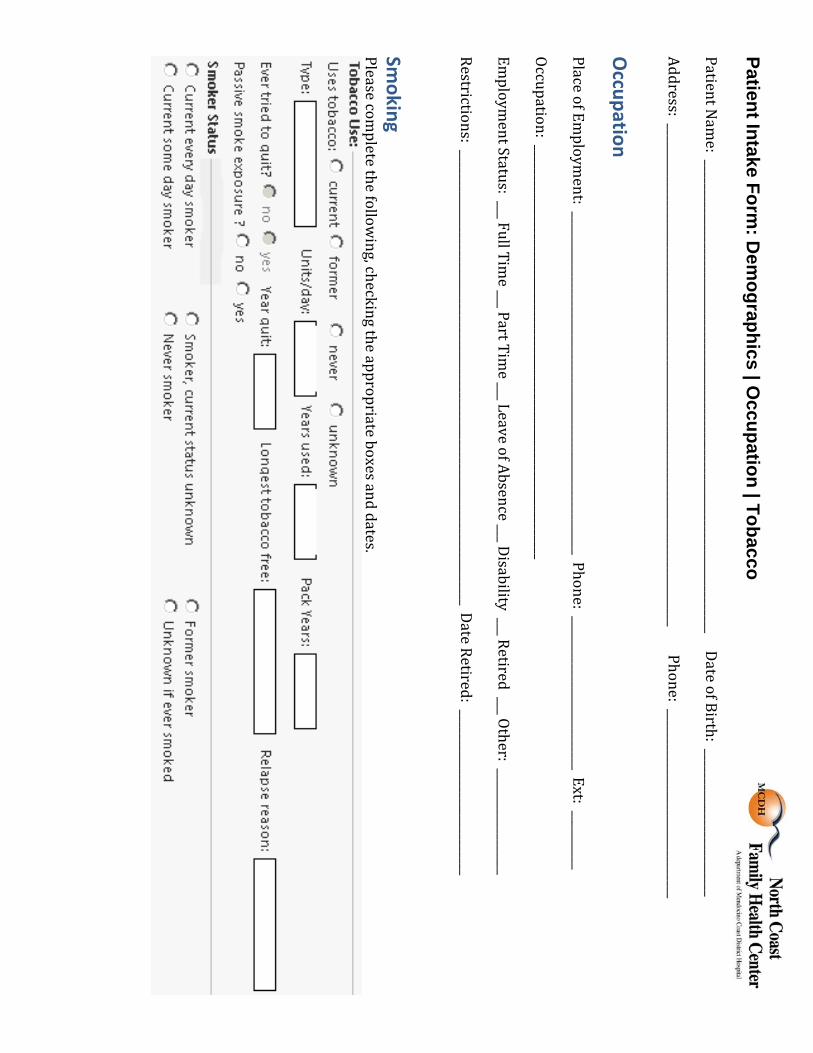
Patient Intake Form: D
emographics | O
ccupation | Tobacco
PatientNam
e:________________________________________________________________________________DateofBirth:_________________________
Address:_____________________________________________________________________________________Phone:________________________________
Occupation
PlaceofEmploym
ent:__________________________________________________________Phone:__________________________Ext:__________
Occupation:______________________________________________________________________
Employm
entStatus:___FullTime___PartTim
e___LeaveofAbsence___Disability___Retired___Other:__________________
Restrictions:_____________________________________________________________________________DateRetired:____________________________
Smoking
Pleasecompletethefollow
ing,checkingtheappropriateboxesanddates.

Patient Intake Form: D
emographics | O
ccupation | Tobacco PatientN
ame:________________________________________________________________________________DateofBirth:_________________________
Lifestyle

Pag
e 2
of
6
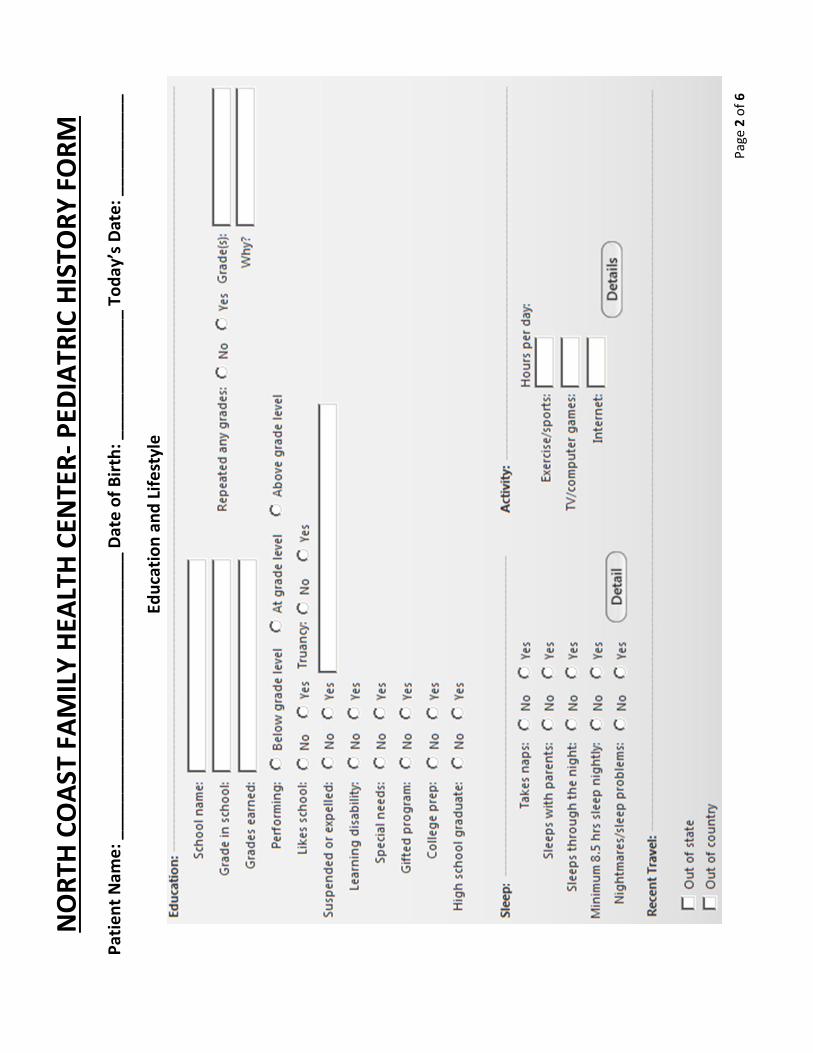
NO
RTH
CO
AST
FA
MIL
Y H
EALT
H C
ENTE
R-
PED
IATR
IC H
ISTO
RY
FO
RM
Pat
ien
t N
ame
: ___
____
____
____
___
____
____
____
_ D
ate
of
Bir
th: _
____
____
____
_ To
day
’s D
ate
: ___
____
____
Edu
cati
on
an
d L
ife
styl
e
Pag
e 3
of
6
NO
RTH
CO
AST
FA
MIL
Y H
EALT
H C
ENTE
R-
PED
IATR
IC H
ISTO
RY
FO
RM
Pat
ien
t N
ame
: ___
____
____
____
___
____
____
____
_ D
ate
of
Bir
th: _
____
____
____
_ To
day
’s D
ate
: ___
____
____
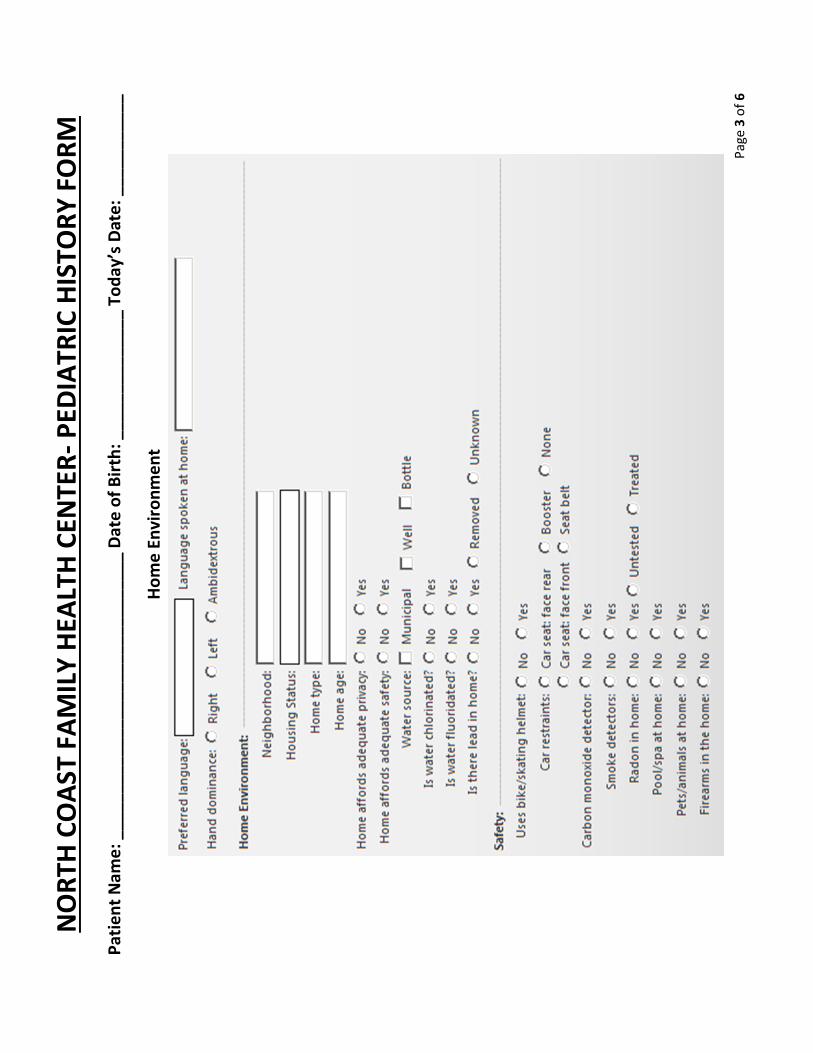
Ho
me
En
viro
nm
en
t

Pag
e 4
of
6
NO
RTH
CO
AST
FA
MIL
Y H
EALT
H C
ENTE
R-
PED
IATR
IC H
ISTO
RY
FO
RM
Pat
ien
t N
ame
: ___
____
____
____
___
____
____
____
_ D
ate
of
Bir
th: _
____
____
____
_ To
day
’s D
ate
: ___
____
____
Re
lati
on
ship
s

Other Information
Other_________________________
Kidney Infection
Ear Infection
Undersized jaw
Frequent acid reflux
Other_________________________
Hurnia repair, stomach
Hurnia repair, groin
Tonsils/Adenoids removed
Inflamation of the airways
Low red blood cells
Seasonal allergies
Crossed eye
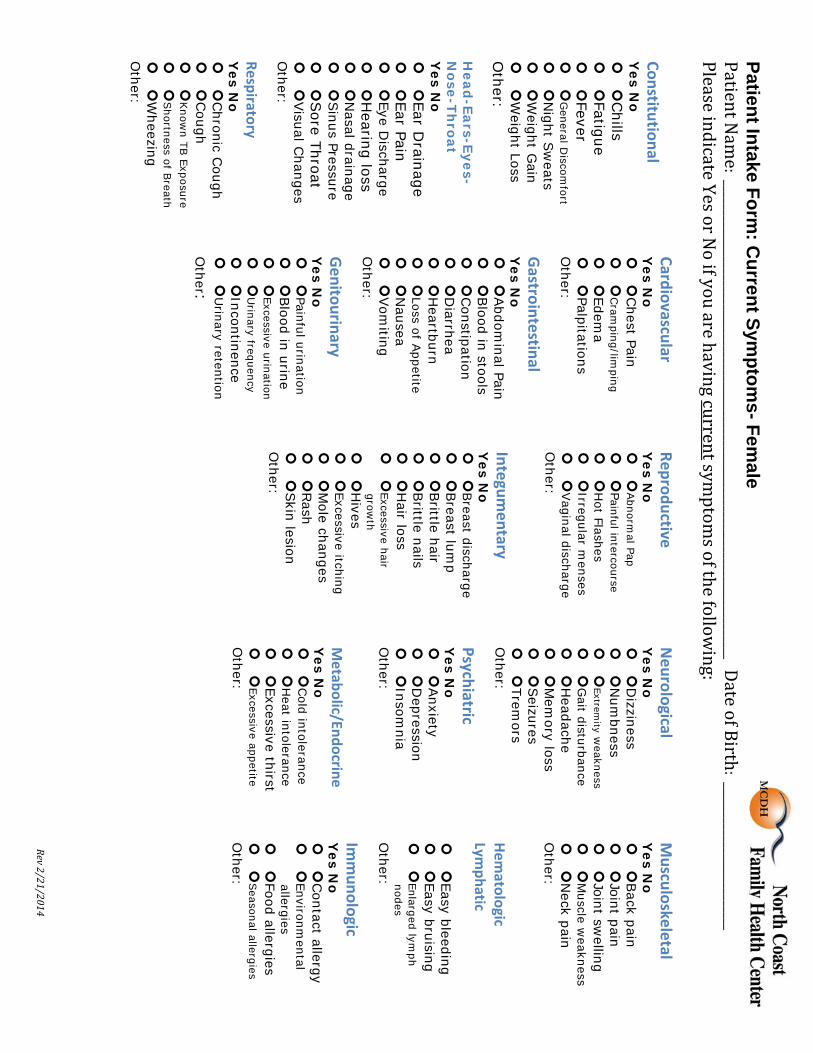
Patient Intake Form: C
urrent Symptom
s- Female
PatientNam
e:_________________________________________________________________________________DateofBirth:_________________________PleaseindicateYesorN
oifyouarehavingcurrentsymptom
softhefollowing:
Constitutional Y
es No
Chills
Fatig ue
Feve r
General D
iscomfort
Night S
weats
Weight G
ain
Weight Loss
Other:
Head
-Ears-Eyes-N
ose-Throat
Yes N
o
Ear Drainage
Ear Pain
Eye Discharge
Hearing loss
Nasal drainage
Sinus Pressure
Sore Throat
Visual C
hangesO
ther:
Respiratory Y
es No
Chronic C
ough
Cough
Know
n TB Exposure
Shortness of B
reath
Wheezing
Other:
Cardiovascular Y
es No
Chest Pain
Cram
ping/limping
Edema
PalpitationsO
ther:
Gastrointestinal
Yes N
o
Abdom
inal Pain
Blood in stools
Constipation
Diarrhea
Heartburn
Loss of Appetite
Nausea
Vom
itingO
ther:
Genitourinary
Yes N
o
Painful urination
Blood in urine
Excessive urination
Urinary frequency
Incontinence
Urinary retention
Other:
Reproductive Y
es No
Abnorm
al Pap
Painful intercourse
Hot Flashes
Irregular menses
Vaginal discharge
Other:
Integumentary
Yes N
o
Breast discharge
Breast lum
p
Brittle hair
Brittle nails
Hair loss
Excessive hairgrow
th
Hives
Excessive itching
Mole changes
Rash
Skin lesion
Other:
Neurological
Yes N
o
Dizziness
Num
bness
Extremity w
eakness
Gait disturbance
Headache
Mem
ory loss
Seizures
Tremors
Other:
Psychiatric Y
es No
Anxiety
Depression
Insomnia
Other:
Metabolic/Endocrine
Yes N
o
Cold intolerance
Heat intolerance
Excessive thirst
Excessive appetiteO
ther:
Musculoskeletal
Yes N
o
Back pain
Joint pain
Joint swelling
Muscle w
eakness
Neck pain
Other:
Hem
atologic Lym
phatic
Easy bleeding
Easy bruising
Enlarged lymph
nodes O
ther:
Immunologic
Yes N
o
Contact allergy
Environmental
allergies
Food allergies
Seasonal allergies
Other:
Rev2/21/2014
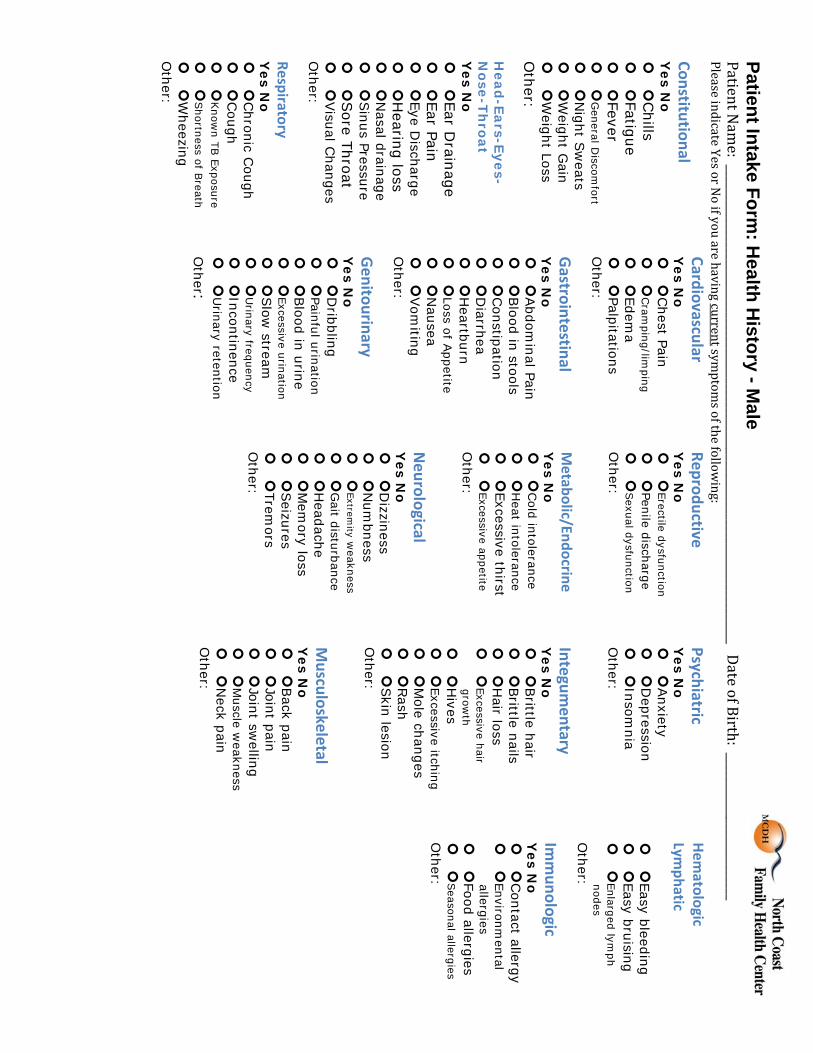
Patient Intake Form: H
ealth History - M
ale PatientN
ame:_________________________________________________________________________________DateofBirth:_________________________
PleaseindicateYesorNoifyouarehavingcurrentsym
ptomsofthefollow
ing:
Constitutional Y
es No
Chills
Fatigue
Fever
General D
iscomfort
Night S
weats
Weight G
ain
Weight Loss
Other:
Head
-Ears-Eyes-N
ose-Throat
Yes N
o
Ear Drainage
Ear Pain
Eye Discharge
Hearing loss
Nasal drainage
Sinus Pressure
Sore Throat
Visual C
hanges O
ther:
Respiratory Y
es No
Chronic C
ough
Cough
Know
n TB Exposure
Shortness of B
reath
Wheezing
Other:
Cardiovascular Y
es No
Chest Pain
Cram
ping/limping
Edema
Palpitations O
ther:
Gastrointestinal
Yes N
o
Abdom
inal Pain
Blood in stools
Constipation
Diarrhea
Heartburn
Loss of Appetite
Nausea
Vom
iting O
ther:
Genitourinary
Yes N
o
Dribbling
Painful urination
Blood in urine
Excessive urination
Slow
stream
Urinary frequency
Incontinence
Urinary retention
Other:
Reproductive Y
es No
Erectile dysfunction
Penile discharge
Sexual dysfunction
Other:
Metabolic/Endocrine
Yes N
o
Cold intolerance
Heat intolerance
Excessive thirst
Excessive appetite O
ther: Neurological
Yes N
o
Dizziness
Num
bness
Extremity w
eakness
Gait disturbance
Headache
Mem
ory loss
Seizures
Tremors
Other:
Psychiatric Y
es No
Anxiety
Depression
Insomnia
Other:
Integumentary
Yes N
o
Brittle hair
Brittle nails
Hair loss
Excessive hair grow
th
Hives
Excessive itching
Mole changes
Rash
Skin lesion
Other:
Musculoskeletal
Yes N
o
Back pain
Joint pain
Joint swelling
Muscle w
eakness
Neck pain
Other:
Hem
atologic Lym
phatic
Easy bleeding
Easy bruising
Enlarged lymph
nodes O
ther:
Immunologic
Yes N
o
Contact allergy
Environmental
allergies
Food allergies
Seasonal allergies
Other:
Pat
Pati
Plea
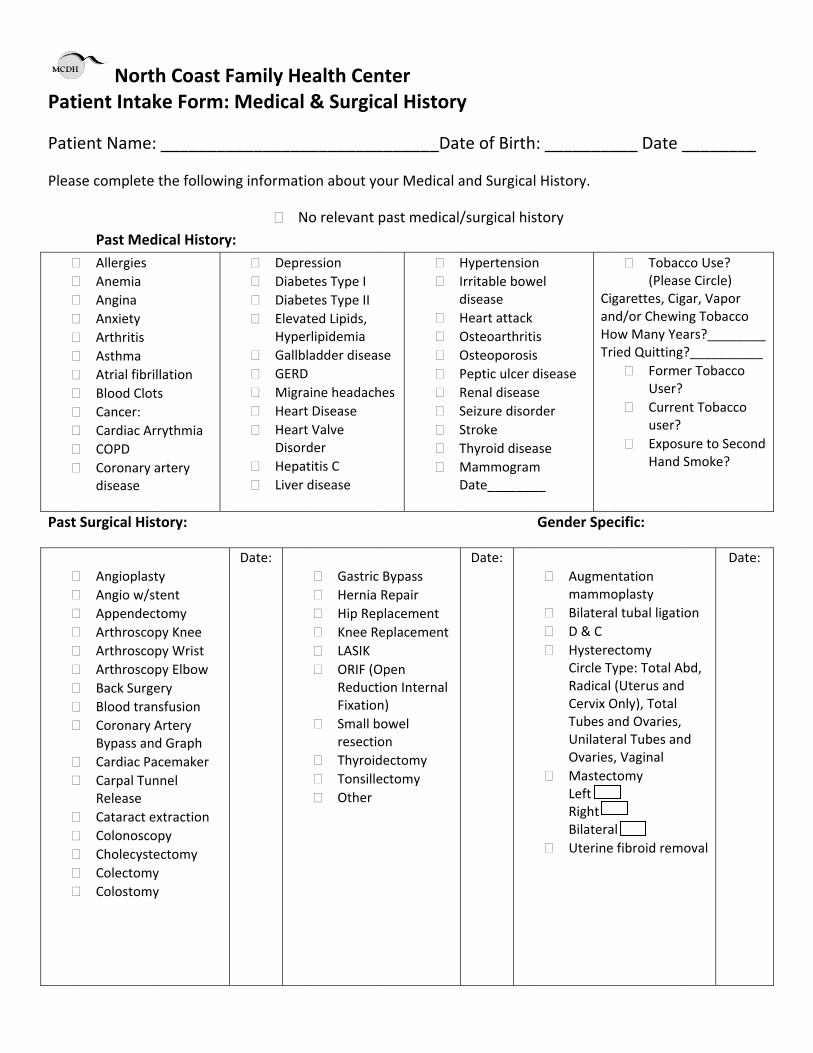
Past
Norttient Inta
ent Name
se complete
Past Med Allergies Anemia Angina Anxiety Arthritis Asthma Atrial fibr Blood Clo Cancer: Cardiac A COPD Coronary
disease
Surgical His
Angioplas Angio w/s Appendec Arthrosco Arthrosco Arthrosco Back Surg Blood tran Coronary
Bypass an Cardiac Pa Carpal Tu
Release Cataract e Colonosco Cholecyst Colectom Colostom
th Coast Fke Form:
: ________
e the followi
dical History
illation ts
rrythmia
artery
story:
sty stent ctomy opy Knee opy Wrist opy Elbow gery nsfusion Artery nd Graph acemaker nnel
extraction opy tectomy y y
Family He Medical
_________
ng informat
Ny:
Depr Diabe Diabe Eleva
Hype Gallb GERD Migra Heart Heart
Disor Hepa Liver
Date:
ealth Cen & Surgic
_________
ion about yo
No relevant p
ession etes Type I etes Type II ated Lipids, erlipidemia bladder diseasD aine headacht Disease t Valve rder atitis C disease
Gastric Hernia Hip Rep Knee Re LASIK ORIF (O
ReductiFixation
Small bresectio
Thyroid Tonsille Other
nter cal Histor
_______Da
our Medical
past medica
se
hes
Bypass Repair placement eplacement
Open ion Internal n) owel on dectomy ectomy
y
ate of Birth
and Surgica
l/surgical his
HypertensioIrritable bowdisease Heart attackOsteoarthritOsteoporosiPeptic ulcer Renal diseasSeizure disorStroke Thyroid diseMammogramDate_______
Date:
h: _______
l History.
story
n wel
is s disease e rder
ase m __
CaHT
Gender Spe
Augmemamm
Bilatera D & C Hystere
Circle TRadicaCervix Tubes aUnilateOvaries
MastecLeft Right Bilatera
Uterine
____ Date _
Tobac(Pleas
igarettes, Cignd/or ChewinHow Many Yearied Quitting?
FormeUser?
Currenuser?
ExposuHand S
ecific:
entation moplasty al tubal ligati
ectomy Type: Total Abl (Uterus andOnly), Total and Ovaries, eral Tubes ands, Vaginal ctomy
al e fibroid remo
________
co Use? e Circle) gar, Vapor ng Tobacco ars?________?__________er Tobacco
nt Tobacco
ure to SecondSmoke?
on
bd,
d
oval
Date:
_ _
d
THE PATIENT PORTAL
DID YOU KNOW?
You can access your medical record through the Patient Portal via your personal computer and Smart Phone?
Click on this icon in the upper right corner at mcdh.org to access your Patient Portal 24/7:
WHAT FEATURES ARE AVAILABLE IN MY PORTAL?
1. Request an appointment
2. Review your latest lab results
3. Request a routine medication refill
4. Communicate with your provider AND they can communicate with you.
5. You can access your portal anytime of the day or night.
6. It’s secure, your patient health information is safe!
If you are interested, ask any NCFHC staff member and we will be glad to assist you in signing up. It’s easy to do!

Patient Intake Form: A
dvanced Directives
PatientN
ame:________________________________________________________________________________DateofBirth:_________________________
Pleasecompletethefollow
inginformationaboutyourAdvanceDirective.IfyoudonothaveanAdvanceDirectivedocum
ent,pleaseindicatenone.





























