Embed Size (px)
Citation preview

Special Lecture:
Patient Blood Management
EORTC 03-2015 Madrid
Dr. rer. medic. Axel Hofmann, ME
Visiting Professor | Institute of Anaesthesiology
University Hospital Zurich - Switzerland
Adjunct Associate Professor | School of Surgery
Faculty of Medicine Dentistry and Health Sciences
University of Western Australia
Adjunct Professor | Faculty of Health Sciences
Curtin University Western Australia
Bangkok 10-2013

EORTC 03-2015 Madrid

Blood Management
Patient Blood Management
(PBM)
DonorBlood Management
EORTC 03-2015 Madrid
The rationale behind PBM is that optimal clinical outcomes can be achieved when the optimization and preservation of a patient’sown blood takes priority over the transfusion of donor blood
GGombotz, H., Hofmann Patient Blood Management – A Concept to Improve Patient Safety and Outcome in A.Gombotz, H., Zacharowski, K.,
Spahn, D. Patient Blood Management, 2nd Edition, 2015 Georg Thieme Verlag KG

EORTC 03-2015 Madrid
BleedingAnaemiaand ID
Two Conditions of Clinical Significance

EORTC 03-2015 Madrid
Highest prevalence of all
diseases worldwide, caused by• absolute iron deficiency (50% of
all causes)
• functional iron deficiency
• severe hemorrhage
• chemotherapy (CIA) and/or
radiation
• medication
• congenital disorders
• other
BleedingAnaemiaand ID
Two Conditions of Clinical Significance

EORTC 03-2015 Madrid
Highest prevalence of all
diseases worldwide, caused by• absolute iron deficiency (50% of
all causes)
• functional iron deficiency
• severe hemorrhage
• chemotherapy (CIA) and/or
radiation
• medication
• congenital disorders
• other
BleedingAnaemiaand ID
Two Conditions of Clinical Significance
Very high prevalence
caused by• local surgical or vessel interruption
• therapeutic and diagnostic
interventions
• trauma
• anticoagulant drugs
• obstetric complications
• congenital disorders
• other
related

EORTC 03-2015 Madrid
1
Problem
Anemia & ID

Anemia Prevalence in Surgical Populations
EORTC 03-2015 Madrid
Type of surgery Prevalence of
pre-operative anaemia (%)
Elective surgery1 19–75
Cardiac surgery1,6 24-26
Non-cardiac surgery2,7 30-40
Orthopaedic surgery1,3-5 19–38
Colorectal surgery5 70
1. Gombotz H, Rehak PH, Shander A, Hofmann A. Blood use in elective surgery: the Austrian benchmark study. Transfusion 2007;47:1468–80.2. Beattie AS, Karkouti K, Wijeysundera DN, Tait G. Risk associated with pre-operative anemia in noncardiac surgery. Anesthesiology 2009;110:574–81.3. Saleh E, McClelland DBL, Hay A, Semple D, Walsh TS. Prevalence of anaemia before major joint arthroplasty and the potential impact of pre-operative
investigation and correction on peri-operative blood transfusions. Br J Anaesth 2007;99:801–8.4. Carson JL, Duff A, Berlin JA, et al. Peri-operative blood transfusion and post-operative mortality. JAMA 1998;279:199–205.5. Auerbach M, Goodnough LT, Picard D, Maniatis A. The role of intravenous iron in anemia management and transfusion avoidance. Transfusion 2008;48:988–10006. Karkouti, K., D.N. Wijeysundera, and W.S. Beattie, Risk associated with preoperative anemia in cardiac surgery: a multicenter cohort study. Circulation, 2008.
117(4): p. 478-84 7. Musallam, K.M., et al., Preoperative anaemia and postoperative outcomes in non-cardiac surgery: a retrospective cohort study. Lancet, 2011.

Independent
Risk Factor
for
AdverseOutcomes
Anemia
& Iron
Deficiency
EORTC 03-2015 Madrid

Independent
Risk Factor
for
AdverseOutcomes
Anemia
& Iron
Deficiency
Anaemia independently associated with increased:
• morbidity
• hospital length of stay
• Mortality
• likelihood of transfusion (2-9 fold) Mussallam KM et al. Lancet 2011
Spahn DR. Anesthesiology 2010; 113(2) 1-14
Beattie WS, et al Anesthesiology 2009; 110(3) 574-81
Dunne JR, et al J Surg Res 2002; 102: 237-44
Shander A. Am J Med 2004; 116(7A) 58S-69S
EORTC 03-2015 Madrid

EORTC 03-2015 Madrid
2
Problem
Blood Loss & Bleeding

Independent
Risk Factor
for
AdverseOutcomes
Blood Loss
&
Bleeding
EORTC 03-2015 Madrid

Independent
Risk Factor
for
AdverseOutcomes
Blood Loss
&
Bleeding
Bleeding associated with increased
• Morbidity
• ICU and hospital length of stay
• Mortality
• Elective & emergency surgery ~0.1%
• Subgroups:
• Vascular 5–8%
• Up to 20% with severe bleeding
• Major organ damage 30–40%
Causes
• On average 75 – 90% local surgical interruption or vessel
interruption
• 10–25% acquired or congenital coagulopathy
Shander A. Surgery 2007
Vivacqua et al Ann Thorac Surg 2011
Christensen et al J Thorac Cardiovasc Surg 2009
Spence et al Am J Surg 1990
Stokes, M.E., et al BMC Health Serv Res, 2011
Ye, X., et al BMC Health Serv Res, 2013
Alstrom, U., et al Br J Anaesth, 2012
EORTC 03-2015 Madrid

Independent
Risk Factor
for
AdverseOutcomes
Blood Loss
&
Bleeding
EORTC 03-2015 Madrid
Anemia
& Iron
Deficiency

EORTC 03-2015 Madrid
For decades RED BLOOD CELL TRANSFUSION
was considered theoptimal treatment for anemia and bleeding
How to Fix Anemia and Bleeding?

EORTC 03-2015 Madrid
How to Fix Anemia and Bleeding?
STOP and evaluateoutcome data!

EORTC 03-2015 Madrid
Blood transfusion was the most common procedureperformed during hospitalizations in 2011 (12 percentof stays with a procedure); the rate of hospitalizationswith blood transfusion more than doubled since 1997.
http://www.hcup-us.ahrq.gov/reports/statbriefs/sb165.pdf

EORTC 03-2015 Madrid
3
Problem
Transfusion andOutcome

Independent
Risk Factor
for
AdverseOutcomes
Transfusion
Large observational studies show RBC txn is
independently associated in a dose-
dependent relationship with
•Morbidity
•ALOS
•Mortality
Shaw et al. Transfusion 2014
Parsons J et al. Crit Care 2013
Horvath K et al. Ann Thorac Surg 2013
Linder et al. BJU Int 2013
Al-Refaie et al Surgery 2012
Ferraris V et al. Arch Surg 2012
Paone G et al. J Thorac Cardiovasc Surg 2012
Bhaskar B et al. Ann Thorac Surg 2012
Stone GW et al. Am Heart J 2012
Xenos et al. Thromb Res 2012
Ferraris et al. Ann Thorac Surg 2011
Glance L et al. Anesthesiol 2011
Ranucci M et al. J Thorac Cardiovas Surg 2011
Haijar LA et al. JAMA 2010
Beattie et al. Anesthesiology 2009
Bernard et al. J Am Coll Surg 2009
Bursi et al. Eur J Vasc Endovasc Surg 2009
Chaiwat O et al. Anesthesiology 2009
Karkouti et al. Circulation 2009
Gauvin et al Transfusion 2008
Scott BH et al. Ann Card Anaesth 2008
Salim A et al. J Am Coll Surg 2008
Ho et al. Spine 2007
Kulier A, et al. Circulation 2007
Murphy GJ, et al. Circulation 2007
Bernard AC, et al J Am Coll Surg 2008
Banbury MK et al. J Am Coll Surg 2006
Jagoditsch et al. Dis Colon Rectum 2006
Koch et al. Ann Thorac Surg 2006
Koch et al. Crit Care Med 2006
Rogers et al. Am Heart J 2006
Surgenor SD, et al Circulation 2006
Taylor RW et al. Crit Care Med 2006
Leal-Noval et al. Anesthesiology 2003
Malone DL et al. J Trauma 2003
Chelemer et al. Ann Thorac Surg 2002
Dunne et al. J Surg Res 2002
Chang et al. Vox Sang 2000
Vignali et al. Vox Sang 1996 EORTC 03-2015 Madrid

Independent
Risk Factor
for
AdverseOutcomes
Transfusion
Large observational studies show RBC txn is
independently associated in a dose-
dependent relationship with
•Morbidity
•ALOS
•Mortality
Shaw et al. Transfusion 2014
Parsons J et al. Crit Care 2013
Horvath K et al. Ann Thorac Surg 2013
Linder et al. BJU Int 2013
Al-Refaie et al Surgery 2012
Ferraris V et al. Arch Surg 2012
Paone G et al. J Thorac Cardiovasc Surg 2012
Bhaskar B et al. Ann Thorac Surg 2012
Stone GW et al. Am Heart J 2012
Xenos et al. Thromb Res 2012
Ferraris et al. Ann Thorac Surg 2011
Glance L et al. Anesthesiol 2011
Ranucci M et al. J Thorac Cardiovas Surg 2011
Haijar LA et al. JAMA 2010
Beattie et al. Anesthesiology 2009
Bernard et al. J Am Coll Surg 2009
Bursi et al. Eur J Vasc Endovasc Surg 2009
Chaiwat O et al. Anesthesiology 2009
Karkouti et al. Circulation 2009
Gauvin et al Transfusion 2008
Scott BH et al. Ann Card Anaesth 2008
Salim A et al. J Am Coll Surg 2008
Ho et al. Spine 2007
Kulier A, et al. Circulation 2007
Murphy GJ, et al. Circulation 2007
Bernard AC, et al J Am Coll Surg 2008
Banbury MK et al. J Am Coll Surg 2006
Jagoditsch et al. Dis Colon Rectum 2006
Koch et al. Ann Thorac Surg 2006
Koch et al. Crit Care Med 2006
Rogers et al. Am Heart J 2006
Surgenor SD, et al Circulation 2006
Taylor RW et al. Crit Care Med 2006
Leal-Noval et al. Anesthesiology 2003
Malone DL et al. J Trauma 2003
Chelemer et al. Ann Thorac Surg 2002
Dunne et al. J Surg Res 2002
Chang et al. Vox Sang 2000
Vignali et al. Vox Sang 1996 EORTC 03-2015 Madrid
RCTs and meta-analyses therof show that liberal
transfusion strategies appear to offer no benefit but result
in increased adverse patient outcomes.
Carson et al. Cochrane Review 2012
Salpeter et al. Am J Med 2014

Triad of
Independent
Risk Factors
for
Adverse Outcomes
Anemia
& Iron
Deficiency
Blood Loss
&
Bleeding
Transfusion
Farmer SL., et al. Best Pract Res Clin Anaesthesiol, 2013. 27(1): p. 43-58Gombotz, H., Hofmann Patient Blood Management – A Concept to Improve Patient Safety and Outcome in A.Gombotz, H., Zacharowski,
K., Spahn, D. Patient Blood Management, 2nd Edition, 2015 Georg Thieme Verlag KG.

Triad of
Independent
Risk Factors
for
Adverse Outcomes
Anemia
& Iron
Deficiency
Blood Loss
&
Bleeding
Transfusion
Farmer SL., et al. Best Pract Res Clin Anaesthesiol, 2013. 27(1): p. 43-58Gombotz, H., Hofmann Patient Blood Management – A Concept to Improve Patient Safety and Outcome in A.Gombotz, H., Zacharowski,
K., Spahn, D. Patient Blood Management, 2nd Edition, 2015 Georg Thieme Verlag KG.
Induces or
exacerbates
anemia

Triad of
Independent
Risk Factors
for
Adverse Outcomes
Anemia
& Iron
Deficiency
Blood Loss
&
Bleeding
Transfusion
Farmer SL., et al. Best Pract Res Clin Anaesthesiol, 2013. 27(1): p. 43-58Gombotz, H., Hofmann Patient Blood Management – A Concept to Improve Patient Safety and Outcome in A.Gombotz, H., Zacharowski,
K., Spahn, D. Patient Blood Management, 2nd Edition, 2015 Georg Thieme Verlag KG.
Restellini S, AP&T 2012Hearnshaw SA, et al Aliment Pharmacol Ther 2010Blair SD, et al Br J Surg 1986
Induces or
exacerbates
anemia
Triggers
transfusion
Associated w/ increased
rebleeding

EORTC 03-2015 Madrid

EORTC 03-2015 Madrid

Optimise
red cell
mass
Minimise
blood loss
& bleeding
Harness &
optimise
physio-
logical
reserve of
anaemia
Anemia,
Iron
Deficiency
Blood Loss
&
Bleeding
Transfusion
EORTC 03-2015 Madrid

Optimise
red cell
mass
Minimise
blood loss
& bleeding
Harness &
optimise
physio-
logical
reserve of
anaemia
Blood Loss
&
Bleeding
Transfusion
EORTC 03-2015 Madrid

Optimise
red cell
mass
Minimise
blood loss
& bleeding
Harness &
optimise
physio-
logical
reserve of
anaemia
Transfusion
EORTC 03-2015 Madrid

Optimise
red cell
mass
Minimise
blood loss
& bleeding
Harness &
optimise
physio-
logical
reserve of
anaemia
EORTC 03-2015 Madrid

2nd Pillar
Minimise blood loss
& bleeding
3rd Pillar
Harness & optimise
physiological
reserve of anaemia
• Optimise erythropoiesis
• Be aware of drug interactions that can
increase anaemia
• Vigilant monitoring and management of
post-operative bleeding
• Avoid secondary haemorrhage
• Rapid warming / maintain normothermia
(unless hypothermia specifically
indicated)
• Autologous blood salvage
• Minimise iatrogenic blood loss
• Haemostasis/anticoagulation
management
• Prophylaxis of upper GI haemorrhage
• Avoid/treat infections promptly
• Be aware of adverse effects of medication
• Time surgery with haematological
optimisation
• Optimise cardiac output
• Optimise ventilation and oxygenation
• Identify and manage bleeding risk
• Minimise iatrogenic blood loss
• Procedure planning and rehearsal
• Assess/optimise patient’s physiological
reserve and risk factors
• Compare estimated blood loss with
patient-specific tolerable blood loss
• Formulate patient-specific management
plan using appropriate blood
conservation modalities to minimise
blood loss, optimise red cell mass and
manage anaemia
1st Pillar
Optimise red cell mass
Perioperative multidisciplinary multimodal patient-specific team approach
PR
EO
PIN
TR
AO
PP
OS
TO
P
Hofmann et al. Current Opinions in Anaesthesiology 2012
• Detect anaemia
• Identify underlying disorder(s) causing
anaemia
• Manage disorder(s)
• Refer for further evaluation if necessary
• Treat suboptimal iron stores/iron
deficiency/anaemia of chronic
disease/iron-restricted erythropoiesis
• Treat other haematinic deficiencies
• Note: Anaemia is a contraindication for
elective surgery
• Meticulous haemostasis and surgical
techniques
• Blood-sparing surgical devices
• Anaesthetic blood conserving strategies
• Autologous blood options
• Maintain normothermia
• Pharmacological/haemostatic agents
• Optimise anaemia reserve
• Maximise oxygen delivery
• Minimise oxygen consumption
• Avoid/treat infections promptly
• Restrictive transfusion thresholds
EORTC 03-2015 Madrid

The Rationale of Patient Blood Management
“PBM ... preempts and significantly reduces the resort to transfusions by addressing modifiable risk factorsthat may result in transfusion long before a transfusion may even be considered“
EORTC 03-2015 Madrid
Hofmann A, Shander A, Farmer S. Five Drivers Shifting the Paradigm from Product Focused Transfusion Practice to Patient Blood Management. Oncologist. 2011;16. (suppl3):3-11
BleedingAnaemiaand ID

2008Government of Western Australia
World’s First Statewide PBM Program
EORTC 03-2015 Madrid

“The WA PBMP is the first proposed on a jurisdictionalsystem-wide basis“
EORTC 03-2015 Madrid
Farmer SF et al. Drivers for change: Western Australia Patient Blood Management Program (WA PBMP), World HealthAssembly (WHA) and Advisory Committee on Blood Safety and Availability (ACBSA). Best Pract Res Clin Anaesthesiol
2013;27(1): in press
“… the Government of Western Australia is to be congratu-lated ... to sustainably implement patient blood management. ... they are leading the world in the battle against unnecessary erythrocyte transfusions and their burden—financially and in terms of morbidity and mortality.“
Spahn et al. Patient blood management: the pragmatic solution for the problems with blood transfusions. Anesthesiology, 2008. 109(6): p. 951-3.

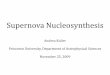
15
20
25
30
35
40
45
50
2006-07 2007-08 2008-09 2009-10 2010-11 2011-12 2012-13 2013-14
Unit
s is
sued
per
1,0
00 p
opula
tion
Financial year
RBC Issuance Comparison between Australia's Five Largest Jusrisdictions2006/07-2013/14
NSW
QLD
SA
VIC
WA
Implementation of WA PBM program
Source: National Blood Authority, 2014
EORTC 03-2015 Madrid

0
1
2
3
4
5
6
7
8
9
10
2006-07 2007-08 2008-09 2009-10 2010-11 2011-12 2012-13 2013-14
Un
its
issu
ed
pe
r 1
,00
0 p
op
ula
tio
n
Financial year
Platelet Issuance Comparison between Australia's Five Largest Jusrisdictions2006/07-2013/14
NSW
QLD
SA
VIC
WA
Source: National Blood Authority, 2014
Implementation of WA PBM program
EORTC 03-2015 Madrid

0
1
2
3
4
5
6
7
8
9
10
2006-07 2007-08 2008-09 2009-10 2010-11 2011-12 2012-13 2013-14
Un
its
issu
ed
pe
r 1
,00
0 p
op
ula
tio
n
Financial year
FFP Issuance Comparison between Australia's Five Largest Jusrisdictions2006/07-2013/14
NSW
QLD
SA
VIC
WA
Source: National Blood Authority, 2014
Implementation of WA PBM program
EORTC 03-2015 Madrid

2010Geneva, Switzerland
World Health Assembly
EORTC 03-2015 Madrid

EORTC 03-2015 Madrid
WHA63.12 adoptedby resolution May 21, 2010:
„Bearing in mind that patient blood management means that before surgery every reasonable measure should be taken to optimize the patient’s own blood volume, to minimize the patient’s blood loss and to harness and optimize the patient-specific physiological tolerance of anaemia following WHO’s guide for optimal clinical use (three pillars of patient blood management)“

2011Dubai, UAE
WHO Global Forum on Patient Blood Management
EORTC 03-2015 Madrid

EORTC 03-2015 Madrid

2011Canberra, Australia
National Blood Authority
EORTC 03-2015 Madrid

EORTC 03-2015 Madrid

EORTC 03-2015 Madrid

EORTC 03-2015 Madrid

EORTC 03-2015 Madrid

EORTC 03-2015 Madrid

“The establishment of coordinated patient blood management programs will help organisations to attain accreditation against national standards such as the new Blood and Blood Products Standard developed by the Australian Commission on Safety and Quality in Health Care.”

EORTC 03-2015 Madrid

EORTC 03-2015 Madrid

EORTC 03-2015 Madrid

2014European Commission
PBM Pilot Project
EORTC 03-2015 Madrid

EORTC 03-2015 Madrid

EORTC 03-2015 Madrid

EORTC 03-2015 Madrid
4
PBM
Results

EORTC 03-2015 Madrid

Transfused RBCs per Admissions in the Eight Largest Public Austrian Hospitals (Admissions w/ >0 ALOS)
0,150
0,200
0,250
0,300
0,350
0,400
0,450
0,500
0,550
2004 2005 2006 2007 2008 2009 2010 2011
RB
Cs
pe
r A
dm
issi
on
Year
A
B
C
D
E
F
G
Linz AKH (mit PBMProgramm)
Bekanntgabe der Ergebnisse der österreichischen Benchmark Studie zum Verbrauch von Blutprodukten an öffentlichen Krankenhäusern
Gombotz, H. and A. Hofmann. Patient Blood Management: three pillar strategy to improve outcome through avoidance of allogeneic blood products. Anaesthesist, 2013. 62(7): p. 519-27.
EORTC 03-2015 Madrid
General Hospital Linz w/ PBM Program
Publication of the results of the Austrian Benchmark Study(blood utilization in public hospitals)

Source: National Blood Authority, 2014; Paul Ehrlich Institut, Germany
0
10
20
30
40
50
60
2004-05 2005-06 2006-07 2007-08 2008-09 2009-10 2010-11 2011-12 2012-13 2013-14
Un
its
issu
ed
pe
r 1
.00
0 p
op
ula
tio
n
Year(Australia and WA finacial year 2013-14, Germany calender year 2013)
RBC Issuance Comparison between Germany, Australia and WA 2004-2013
WA
Australia
Germany
EORTC 03-2015 Madrid

Benefits of PBM Programs
EORTC 03-2015 Madrid
reduction up to 43%
reduction of composite morbidity up to 41%,and infection rate up to 80%
reduction up to 68%
reduction by 16-33%Average LOSA
AeadmissionsR
A omplicationsC
ortalityM
A ostsC reduction by 10-24%
Frank 2014; Freedman 2014; Lapar 2013; Kotze 2012; Moskowitz 2010; Reddy 2009; Brevig 2009; Ferraris 2007; Wong 2007; Ghiglione 2007; Freedman
2007; Martinez 2007; DeAnda 2006; Freedman 2005; Pierson 2004; Green 2004; Kourtzis 2004; Morgan 2004; Slappendel 2003; Van der Linden 2001;
Helm 1998
reduction by 10 - 95%ransfusionT
AeoperationR reduction up to 43%

EORTC 03-2015 Madrid
Safety
Mortality & Morbidity ALOS Health Care $$$
Problem:
Solution:
Benefit:

1. Too much unnecessary care
2. Avoidable harm to patients
3. Billions of dollars wasted
4. Perverse incentives in how we pay for care
5. Lack of transparency
EORTC 03-2015 Madrid
All addressed by PBM