Embed Size (px)
Citation preview
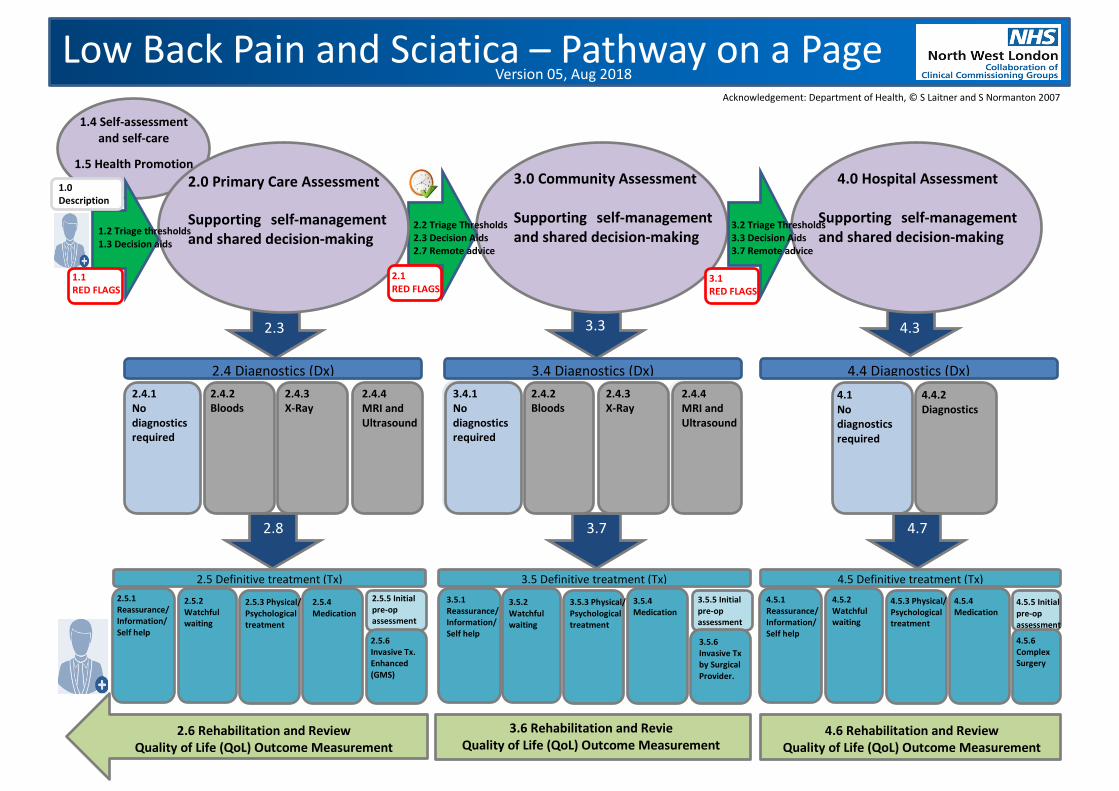
Low Back Pain and Sciatica – Pathway on a Page
2.4 Diagnostics (Dx) 4.4 Diagnostics (Dx) 3.4 Diagnostics (Dx)
2.0 Primary Care Assessment Supporting self-management and shared decision-making
3.0 Community Assessment Supporting self-management and shared decision-making
4.0 Hospital Assessment Supporting self-management and shared decision-making
2.5 Definitive treatment (Tx) 3.5 Definitive treatment (Tx) 4.5 Definitive treatment (Tx)
1.4 Self-assessment and self-care
1.5 Health Promotion
2.5.1 Reassurance/ Information/ Self help
2.5.2 Watchful waiting
2.5.3 Physical/ Psychological treatment
2.5.4 Medication
2.5.5 Initial pre-op assessment 2.5.6 Invasive Tx. Enhanced (GMS)
1.0 Description
2.8
2.3 3.3 4.3
4.7 3.7
1.2 Triage thresholds 1.3 Decision aids
2.2 Triage Thresholds 2.3 Decision Aids 2.7 Remote advice
3.2 Triage Thresholds 3.3 Decision Aids 3.7 Remote advice
Version 05, Aug 2018
2.4.1 No diagnostics required
2.4.2 Bloods
2.4.3 X-Ray
2.4.4 MRI and Ultrasound
4.1 No diagnostics required
4.4.2 Diagnostics
3.5.1 Reassurance/ Information/ Self help
4.5.1 Reassurance/ Information/ Self help
4.5.2 Watchful waiting
3.5.2 Watchful waiting
4.5.3 Physical/ Psychological treatment
3.5.3 Physical/ Psychological treatment
4.5.4 Medication
3.5.4 Medication 4.5.5 Initial
pre-op assessment
3.5.5 Initial pre-op assessment
4.5.6 Complex Surgery
3.5.6 Invasive Tx by Surgical Provider.
1.1 RED FLAGS
2.1 RED FLAGS 3.1
RED FLAGS
2.6 Rehabilitation and Review Quality of Life (QoL) Outcome Measurement
3.6 Rehabilitation and Revie Quality of Life (QoL) Outcome Measurement
4.6 Rehabilitation and Review Quality of Life (QoL) Outcome Measurement
3.4.1 No diagnostics required
2.4.2 Bloods
2.4.3 X-Ray
2.4.4 MRI and Ultrasound
Acknowledgement: Department of Health, © S Laitner and S Normanton 2007

1. 4 Supporting Self-management • Provide training for healthcare professionals and reception staff
including signposting patients to advice to support self-management • Links to national websites via practice and Trust websites e.g.:
NHS Choices MSk Pages NHS Choices Back Pain and NHS Choices Back Pain Tool NHS Choices Sciatica and NHS Choices Sciatica Exercises The Pain Toolkit
• Links to local services via practice and Trust websites e.g.: healthyealing.com careplace.org.uk oneyouealing.org Ealing Community & Voluntary Service LNWH Trust MSk Exercises
2.0 Primary Care Assessment • Clinically exclude serious underlying pathology (for example
cancer, infection, trauma or inflammatory disease such as spondyloarthritis – esp. if age <45). If reasonable suspicion of serious underlying pathology, investigate and refer as clinically appropriate (see below)
• Think about alternative diagnoses when examining or reviewing people with low back pain, particularly if they develop new or changed symptoms
• Consider using risk stratification (for example, the STarT Back risk assessment tool) at first point of contact with a healthcare professional for each new episode of low back pain ± sciatica, to inform shared decision-making about stratified management. (https://www.keele.ac.uk/media/keeleuniversity/group/startback/Keele_STarT_Back9_item-7.pdf)
• Based on risk stratification, consider: - simpler and less intensive support for people likely to
improve quickly and have a good outcome (for example, reassurance, advice to keep active and guidance on self-management)
- more complex and intensive support for people at higher risk of a poor outcome (for example, exercise programmes with or without manual therapy or using a psychological approach)
• The BMJ Visual Summary on managing low back pain and sciatica provides an overview of the NICE guidelines, from the perspective of a patient presenting in primary care (BMJ Infographic)
3.0 Community Care Assessment • Refer urgently to secondary care if there is a reasonable clinical suspicion of serious underlying pathology • Assess for risk of poor functional outcome as this will guide the intensity of support that may be needed
4.0 Secondary Care Assessment • Pre-requisites: Patients should have been clinically triaged, images and reports available,
referred into a clinic that is run by a member of staff that is capable of doing the surgery. • Assess for risk of poor functional outcome as this will guide the intensity of physical and
psychological support that may be needed
1.5 Health Promotion and Primary Prevention • Stopping smoking • Adequate calcium intake in diet • Maintain general cardiovascular fitness, strength and balance
CMO Physical activity guidelines • Reducing and maintaining weight loss if overweight • Advice to modify high-risk environments in sports and workplaces • Adopt a life course approach to prevention of musculoskeletal disorders,
see ‘Focus on Musculoskeletal Health’ Ealing JSNA 2017 and full version of MSk JSNA
2.5 Primary Care Management • Low Back Pain: Consider a short course of non-steroidal anti-inflammatory drugs
(NSAIDs) with gastro-protection, or a weak opioid where an NSAID is ineffective or poorly tolerated, and do not offer paracetamol alone for low back pain
• Sciatica: Consider a short course of non-steroidal anti-inflammatory drugs (NSAIDs) with gastro-protection, medium to high-dose tricyclic antidepressants, gabapentinoids; and explain to patients that there is a lack of evidence to support the prescription of any particular pain medication, and that these drugs can have side effects (BMJ 2017)
• Review analgesia, continue only recommended drugs that are helpful and minimise harm; paracetamol, opioids, antidepressants and gabapentinoids are not recommended for chronic low back pain without sciatica
• Back pain is a recurrent condition. Ask the following three questions to guide shared decision-making - What treatments have you had for this condition before? - How much improvement did you have with the treatments? - How long did the improvements last?
3.5 Community Care Management • Consider exercises such as stretching, strengthening, aerobic, yoga, or Tai Chi in a group setting for all patients
with low back pain and sciatica as the main component of non-invasive treatment • Manual therapy and psychological approaches should be recommended only alongside an exercise programme • Acupuncture or electrotherapies should not be recommended • Consider imaging for people with low back pain ± sciatica only if the result is likely to change management, or as
part of shared care arrangements with secondary care providers • Consider a combined physical and psychological programme incorporating a cognitive behavioural approach
(preferably in a group context that takes into account a person’s specific needs and capabilities) for people with persistent low back pain or sciatica: - When they have substantial psychosocial obstacles to recovery (for example, avoiding normal activities based
on inappropriate beliefs about their condition) - When previous treatments have not been effective.
• Consider referral for spinal injections (or community provision where commissioned) for acute sciatica in accordance with the NW London Low Back Pain policy (2017). (Note that injections for acute sciatica need to be offered within 3 months of referral to be clinically and cost-effective)
• Consider referral for other invasive treatments in accordance with NICE guidance (NG59, 2016) and the NW London Low Back Pain policy (2017), if the person is willing to consider these options.
• Radiofrequency denervation is effective for (some) people with severe localised low back pain arising from structures innervated by the medial branch nerves, where other non-surgical treatments have not worked for them. Consider referral for assessment for radiofrequency denervation for people with chronic low back pain in accordance with NICE guideline CG59 (2016) and the NW London LBP Policy (2017). (Review the old notes first)
• Review if a specialist has considered if other procedures covered by NICE Interventional Procedures guidance are appropriate and cost-effective for use within the NHS for this person. (Review the old notes first)
4.5 Secondary Care Management • Offer treatments in accordance with NICE guideline CG59 (2016) and the NW
London LBP Policy (2017) (see below) • Consider if other procedures covered by NICE Interventional Procedures
guidance are appropriate and cost-effective for use within the NHS for this person. (Review the old notes first)
• Consider referral to community clinics for management (see above) only where a specific treatment recommend above has not been tried, or there has been a clinically meaningful and lasting effect (beyond the end of treatment) for previous recurrences
• Review analgesia, continue only recommended drugs that are helpful and minimise harm; paracetamol, opioids, antidepressants and gabapentinoids are not recommended for chronic low back pain without sciatica.
• Consider the risks and benefits of pursuing investigations and continuing treatments where these are of limited benefit. Instead, patients could return to primary care management, with pain clinic support where needed (BMJ 2017)
2.4 Primary Care Diagnostics • Do not routinely offer imaging in a non-specialist setting for people with low back pain ±
sciatica • Explain to people with low back pain ± sciatica that if they are being referred for
specialist opinion, they may not need imaging • Consider imaging in specialist settings of care (for example, a musculoskeletal interface
clinic or hospital) for people with low back pain ± sciatica only if the result is likely to change management
• Imaging from primary care may be indicated for exclusion of osteoporotic fractures (plain lateral X-ray) as management can be continued in primary care
• Consider other diagnostics (imaging, blood tests) where there is a high suspicion of serious underlying pathology and it is not clinically appropriate to refer the patient and the result is likely to change management
5.1 Triage † • Referrals should be clinically triaged within 48 hours • Clinical triage should be performed by therapists and specialists
with knowledge of management of low back pain • Triage staff should have ready access to a wider
multidisciplinary team including, for instance, spinal orthopaedic or neurosurgeon, pain physician, psychologist, rheumatologist, podiatrist, etc.
• Triage staff should have local knowledge and understanding about which clinics to refer to if all referral thresholds have been met
• Triage staff should feedback to GPs referrals that are not accepted and advise what alternative treatment options have been recommended
† See Referral Criteria for full description of inclusions and exclusions for referral to each service
5.2 Transformation Opportunities • Rates of MRI scanning in different settings of care, including
repeat scans rates • Medicines management for chronic pain • Referrals meeting referral thresholds and guidance (audit or
triage) • Waiting times for community and secondary care • Re-referral rates for same condition • Rates of offering advice to support self-management • Providing comprehensive discharge plans • Providing feedback on the quality and appropriateness of
referrals • Invasive treatment (surgery, RFD, epidurals, etc.) conversion
rates from community clinics • Reducing inappropriate referrals from primary care
5.3 Local and National Guidance • Offer treatments in accordance with NICE guideline CG59 (2016)
and the NW London CCG Commissioning Policies NICE NG59 2016 NWL LBP & Sciatica Policy v4.1 2017 NWL Acupuncture Policy v4.1 2017 NWL Radio Frequency Denervation Policy v4.1 2017
• Follow local triage arrangements and referral advice, particularly on thresholds for referral and which service to refer
• Follow the NW London policy on consultant to consultant (C2C, Internally Generated Demand) referrals where: Conditions that are unrelated to the presenting problems and do not require an urgent referral; Incidental findings; Conditions that can be dealt with by the Primary Care Team without recourse to secondary care. NWL C2C IGD Policy 2014
• NHS England Elective Care Transformation Programme https://www.england.nhs.uk/wp-content/uploads/2017/11/msk-orthopaedic-elective-care-handbook-v2.pdf
Patient Symptom LBP ± Sciatica
Patient
3.4 Community Care Diagnostics • Explain to people with low back pain ± sciatica that if they are being referred for specialist opinion, they may
not need imaging • Consider imaging in specialist settings of care (for example, a musculoskeletal interface clinic or hospital) for
people with low back pain ± sciatica only if the result is likely to change management
4.4 Secondary Care Diagnostics • Explain to people with low back pain ± sciatica that if they are being referred for
specialist opinion, they may not need imaging • Consider imaging in specialist settings of care (for example, a musculoskeletal interface
clinic or hospital) for people with low back pain ± sciatica only if the result is likely to change management
Pathway on a Page Low Back Pain & Sciatica v05, Aug 2018 [email protected]
2.2 Primary and Community Referral Thresholds, and Triage • Check previous clinic and discharge letters as they may give suggestions for further management, the conditions for re-referral and the most appropriate service. • Consider if any treatments have had a significant meaningful clinical benefit on pain or function, lasting well beyond the end of the treatment. (As a guide, for non-invasive treatments, this means at least a 30% improvement in pain
or function, lasting at least 3-6 months beyond the end of treatment. A greater and more sustained improvement would be needed for invasive treatments in view of their higher clinical risks and costs.) • Seek and treat any co-morbid mental health problems, including depression • Follow the NICE pathway for diagnosis of suspected spondyloarthritis (NICE NG65, 2017 infographic), and refer to community or hospital rheumatologist if threshold reached • Consider referral for exercise-based therapies if person has progressed slowly with initial GP management for low back pain (As a guide, consider a threshold for referral of less than 70% recovery after 2wks) • Consider referral to a community or hospital-based service for combined physical and psychological treatments if risk stratification (see above) suggests a high risk of poor functional outcome • Consider referral to a community or hospital-based service for patients with chronic low back pain with or without sciatica, who cannot be managed in primary care. • Consider referral to a community or hospital-based service (including pain clinics) for patients with acute sciatica (of less than 3 months duration), where there is a poor response to analgesics and neuropathic agents, and only if the
patient is willing to consider a spinal steroid injection or surgery. (Note that injections for acute sciatica need to be offered within 3 months of referral to be clinically and cost-effective) • Implement a quality-assured triage system in accordance with NHS England advice (see box 5.3) for all back pain and sciatica referrals from primary care where there is no clinical suspicion of serious underlying pathology. Referrals
should be triaged by specialists (e.g. ESP Physios) with access to the wider MDT to support decision-making. • Adequate information should be provided on referral forms to ensure patients have been offered appropriate advice to support self-management before referral, and to support triage.
2.1 Emergency Referrals • Refer urgently to secondary care if there is a reasonable clinical suspicion of serious underlying pathology: community clinics are not commissioned to investigate cauda equina syndrome and other severe and rapidly progressive
neurological disease, metastatic disease, serious trauma, structural deformities, or infection • Cauda equina syndrome: Emergency Referral: local hospital orthopaedics (or neurosurgery if available). Local hospital will transfer to regional neurosurgery unit as appropriate. • Serious spinal pathology is suspected: referral within 1 week: oncology, infectious diseases, etc. • Progressive neurological deficit, e.g. weakness, anaesthesia: referral within 1 week: local hospital orthopaedics (or neurosurgery if available)
2.3, 3.3, 4.3 Supporting self-management and shared-decision-making at all stages of the pathway Provide following advice to support self-management
• Benign nature of the condition (if serious underlying pathology not suspected on referral) • Good probability of rapid improvement (depends on waiting time before assessed) • Importance of early return to work or normal activities
• No recommendation about bed rest – use clinical judgement (n.b. risk of harm) • Value of engaging in exercise • Signpost to information on the nature of low back pain and sciatica
• Signpost to advice on general exercise (aerobic, yoga, or Tai Chi) and specific exercises (low back stretching and strengthening exercises)
• Incorporate shared decision-making principles and tools
2.6, 3.6, 4.6 Rehabilitation, Supporting Self-Management, Discharge Planning Ensure patients are discharged with a management plan that includes:
• Diagnosis (use positive, non-threatening language) • Prognosis • Advice to support self-management
• Management options that can be offered in primary care • Medication advice, with second and third line options (if within scope of community service) • Whether a combined physical and psychological programme would be beneficial
• The conditions under which the patient should be re-referred (i.e. what new symptoms would warrant re-referral for the same condition)

Low Back Pain and Sciatica 3
1.1 Emergency Referrals to Hospital See ‘Referral Criteria and Triage Specification’
1.2 Referral Thresholds, and Triage to Primary Care See ‘Referral Criteria and Triage Specification’
1.3 Supporting self-management and shared-decision-making (SDM) at all stages of the pathway See ‘Referral Criteria and Triage Specification’
1.4 Supporting self-management • See slide from self-management group in ‘Referral Criteria and Triage Specification’ • Provide training for healthcare professionals and reception staff including signposting patients to
advice to support self-management • Links to national websites via practice and Trust websites e.g.:
NHS Choices MSk Pages NHS Choices Back Pain and NHS Choices Back Pain Tool NHS Choices Sciatica and NHS Choices Sciatica Exercises The Pain Toolkit
• Links to local services via practice and Trust websites e.g.: healthyealing.com careplace.org.uk oneyouealing.org Ealing Community & Voluntary Service LNWH Trust MSk Exercises
1.5 Health Promotion and Primary Prevention • Stopping smoking • Adequate calcium intake in diet • Maintain general cardiovascular fitness, strength and balance
CMO Physical activity guidelines • Reducing and maintaining weight loss if overweight • Advice to modify high-risk environments in sports and workplaces • Adopt a life course approach to prevention of musculoskeletal disorders,
see ‘Focus on Musculoskeletal Health’ Ealing JSNA 2017 and full version of MSk JSNA • See http://www.ealingccg.nhs.uk/media/136195/EALING-JSNA-Focus-On-Musculoskeletal-Health-
Dec17.pdf
2.0 Primary Care Assessment • Clinically exclude serious underlying pathology (for example cancer, infection, trauma or
inflammatory disease such as spondyloarthritis – esp. if age <45). If reasonable suspicion of serious underlying pathology, investigate and refer as clinically appropriate (see below)
• Think about alternative diagnoses when examining or reviewing people with low back pain, particularly if they develop new or changed symptoms
• Consider using risk stratification (for example, the STarT Back risk assessment tool) at first point of contact with a healthcare professional for each new episode of low back pain ± sciatica, to inform shared decision-making about stratified management. (https://www.keele.ac.uk/media/keeleuniversity/group/startback/Keele_STarT_Back9_item-7.pdf)

Low Back Pain and Sciatica 4
• Based on risk stratification, consider: - simpler and less intensive support for people likely to improve quickly and have a good outcome
(for example, reassurance, advice to keep active and guidance on self-management) - more complex and intensive support for people at higher risk of a poor outcome (for example,
exercise programmes with or without manual therapy or using a psychological approach) • The BMJ Visual Summary on managing low back pain and sciatica provides an overview of the NICE
guidelines, from the perspective of a patient presenting in primary care (BMJ Infographic)
2.1 Primary Care Emergency Referrals to Hospital See ‘Referral Criteria and Triage Specification’
• Refer urgently to secondary care if there is a reasonable clinical suspicion of serious underlying pathology: community clinics are not commissioned to investigate cauda equina syndrome and other severe and rapidly progressive neurological disease, metastatic disease, serious trauma, structural deformities, or infection
• Cauda equina syndrome: Emergency Referral: local hospital orthopaedics (or neurosurgery if available). Local hospital will transfer to regional neurosurgery unit as appropriate.
• Serious spinal pathology is suspected: referral within 1 week: oncology, infectious diseases, etc. • Progressive neurological deficit, e.g. weakness, anaesthesia: referral within 1 week: local hospital
orthopaedics (or neurosurgery if available)
2.2 Primary Care Referral Thresholds, and Triage to Community and Hospital See ‘Referral Criteria and Triage Specification’
• Check previous clinic and discharge letters as they may give suggestions for further management, the conditions for re-referral and the most appropriate service.
• Consider if any treatments have had a significant meaningful clinical benefit on pain or function, lasting well beyond the end of the treatment. (As a guide, for non-invasive treatments, this means at least a 30% improvement in pain or function, lasting at least 3-6 months beyond the end of treatment. A greater and more sustained improvement would be needed for invasive treatments in view of their higher clinical risks and costs.)
• Seek and treat any co-morbid mental health problems, including depression • Follow the NICE pathway for diagnosis of suspected spondyloarthritis (NICE NG65, 2017
infographic), and refer to community or hospital rheumatologist if threshold reached • Consider referral for exercise-based therapies if person has progressed slowly with initial GP
management for low back pain (As a guide, consider a threshold for referral of less than 70% recovery after 2wks)
• Consider referral to a community or hospital-based service for combined physical and psychological treatments if risk stratification (see above) suggests a high risk of poor functional outcome
• Consider referral to a community or hospital-based service for patients with chronic low back pain with or without sciatica, who cannot be managed in primary care.
• Consider referral to a community or hospital-based service (including pain clinics) for patients with acute sciatica (of less than 3 months duration), where there is a poor response to analgesics and neuropathic agents, and only if the patient is willing to consider a spinal steroid injection or surgery. (Note that injections for acute sciatica need to be offered within 3 months of referral to be clinically and cost-effective)
• Implement a quality-assured triage system in accordance with NHS England advice (see box 5.3) for all back pain and sciatica referrals from primary care where there is no clinical suspicion of serious underlying pathology. Referrals should be triaged by specialists (e.g. ESP Physios) with access to the wider MDT to support decision-making.
• Adequate information should be provided on referral forms to ensure patients have been offered appropriate advice to support self-management before referral, and to support triage.

Low Back Pain and Sciatica 5
2.3, 3.3, 4.3 Supporting self-management and shared-decision-making (SDM) at all stages of the pathway
• Benign nature of the condition (if serious underlying pathology not suspected on referral) • Good probability of rapid improvement (depends on waiting time before assessed) • Importance of early return to work or normal activities • No recommendation about bed rest – use clinical judgement (n.b. risk of harm) • Value of engaging in exercise • Signpost to information on the nature of low back pain and sciatica • Signpost to advice on general exercise (aerobic, yoga, or Tai Chi) and specific exercises
(low back stretching and strengthening exercises) • Incorporate shared decision-making principles and tools • The following key opportunities have been identified for a SDM approach - Giving GPs better access to up to date meaningful information about risk/benefit, - Allowing patients access to decision making tools to better understand their care and self-
manage where appropriate - Enabling junior doctors to be fully versed on SDM
• NHS RightCare will facilitate a working group to feed into all the MSk pathways, procure the training materials, support integration into primary care clinical systems, and review the points in the pathway where a specific shared-decision intervention should be considered, and support staff to do this.
2.4 Primary Care Diagnostics • Do not routinely offer imaging in a non-specialist setting for people with low back pain ± sciatica • Explain to people with low back pain ± sciatica that if they are being referred for specialist opinion,
they may not need imaging • Consider imaging in specialist settings of care (for example, a musculoskeletal interface clinic or
hospital) for people with low back pain ± sciatica only if the result is likely to change management • Imaging from primary care may be indicated for exclusion of osteoporotic fractures (plain lateral X-
ray) as management can be continued in primary care • Consider other diagnostics (imaging, blood tests) where there is a high suspicion of serious
underlying pathology and it is not clinically appropriate to refer the patient and the result is likely to change management
2.5 Primary Care Management • Low Back Pain: Consider a short course of non-steroidal anti-inflammatory drugs (NSAIDs) with
gastro-protection, or a weak opioid where an NSAID is ineffective or poorly tolerated, and do not offer paracetamol alone for low back pain
• Sciatica: Consider a short course of non-steroidal anti-inflammatory drugs (NSAIDs) with gastro-protection, medium to high-dose tricyclic antidepressants, gabapentinoids; and explain to patients that there is a lack of evidence to support the prescription of any particular pain medication, and that these drugs can have side effects (BMJ 2017)
• Review analgesia, continue only recommended drugs that are helpful and minimise harm; paracetamol, opioids, antidepressants and gabapentinoids are not recommended for chronic low back pain without sciatica
• Back pain is a recurrent condition. Ask the following three questions to guide shared decision-making
- What treatments have you had for this condition before? - How much improvement did you have with the treatments? - How long did the improvements last?
• See slide from medicines management group in ‘Referral Criteria and Triage Specification’ about choice of drugs for back pain and sciatica, and the advice for stopping medication where the harms outweigh benefits.

Low Back Pain and Sciatica 6
2.6, 3.6, 4.6 Rehabilitation, Supporting Self-Management, Discharge Planning Ensure patients are discharged with a management plan that includes:
• Diagnosis (use positive, non-threatening language) • Prognosis • Advice to support self-management • Management options that can be offered in primary care • Medication advice, with second and third line options (if within scope of community service) • Whether a combined physical and psychological programme would be beneficial • The conditions under which the patient should be re-referred (i.e. what new symptoms would
warrant re-referral for the same condition)
3.0 Community Care Assessment • Refer urgently to secondary care if there is a reasonable clinical suspicion of serious underlying
pathology • Assess for risk of poor functional outcome as this will guide the intensity of support that may be
needed
3.1 Community Emergency Referrals to Hospital See ‘Referral Criteria and Triage Specification’
• Refer urgently to secondary care if there is a reasonable clinical suspicion of serious underlying pathology: community clinics are not commissioned to investigate cauda equina syndrome and other severe and rapidly progressive neurological disease, metastatic disease, serious trauma, structural deformities, or infection
• Cauda equina syndrome: Emergency Referral: local hospital orthopaedics (or neurosurgery if available). Local hospital will transfer to regional neurosurgery unit as appropriate.
• Serious spinal pathology is suspected: referral within 1 week: oncology, infectious diseases, etc. • Progressive neurological deficit, e.g. weakness, anaesthesia: referral within 1 week: local hospital
orthopaedics (or neurosurgery if available)
3.2 Community Referral Thresholds, and Triage to Hospital See ‘Referral Criteria and Triage Specification’
• Check previous clinic and discharge letters as they may give suggestions for further management, the conditions for re-referral and the most appropriate service.
• Consider if any treatments have had a significant meaningful clinical benefit on pain or function, lasting well beyond the end of the treatment. (As a guide, for non-invasive treatments, this means at least a 30% improvement in pain or function, lasting at least 3-6 months beyond the end of treatment. A greater and more sustained improvement would be needed for invasive treatments in view of their higher clinical risks and costs.)
• Seek and treat any co-morbid mental health problems, including depression • Follow the NICE pathway for diagnosis of suspected spondyloarthritis (NICE NG65, 2017
infographic), and refer to community or hospital rheumatologist if threshold reached • Consider referral for exercise-based therapies if person has progressed slowly with initial GP
management for low back pain (As a guide, consider a threshold for referral of less than 70% recovery after 2wks)
• Consider referral to a community or hospital-based service for combined physical and psychological treatments if risk stratification (see above) suggests a high risk of poor functional outcome
• Consider referral to a community or hospital-based service for patients with chronic low back pain with or without sciatica, who cannot be managed in primary care.
Low Back Pain and Sciatica 7
• Consider referral to a community or hospital-based service (including pain clinics) for patients with acute sciatica (of less than 3 months duration), where there is a poor response to analgesics and neuropathic agents, and only if the patient is willing to consider a spinal steroid injection or surgery. (Note that injections for acute sciatica need to be offered within 3 months of referral to be clinically and cost-effective)
• Implement a quality-assured triage system in accordance with NHS England advice (see box 5.3) for all back pain and sciatica referrals from primary care where there is no clinical suspicion of serious underlying pathology. Referrals should be triaged by specialists (e.g. ESP Physios) with access to the wider MDT to support decision-making.
• Adequate information should be provided on referral forms to ensure patients have been offered appropriate advice to support self-management before referral, and to support triage.
3.3 Supporting self-management and shared-decision-making (SDM) at all stages of the pathway See 2.3 above
3.4 Community Care Diagnostics • Explain to people with low back pain ± sciatica that if they are being referred for specialist opinion,
they may not need imaging • Consider imaging in specialist settings of care (for example, a musculoskeletal interface clinic or
hospital) for people with low back pain ± sciatica only if the result is likely to change management
3.5 Community Care Management • Consider exercises such as stretching, strengthening, aerobic, yoga, or Tai Chi in a group setting for
all patients with low back pain and sciatica as the main component of non-invasive treatment • Manual therapy and psychological approaches should be recommended only alongside an exercise
programme • Acupuncture or electrotherapies should not be recommended • Consider imaging for people with low back pain ± sciatica only if the result is likely to change
management, or as part of shared care arrangements with secondary care providers • Consider a combined physical and psychological programme incorporating a cognitive behavioural
approach (preferably in a group context that takes into account a person’s specific needs and capabilities) for people with persistent low back pain or sciatica:
• When they have substantial psychosocial obstacles to recovery (for example, avoiding normal activities based on inappropriate beliefs about their condition)
• When previous treatments have not been effective. • Consider referral for spinal injections (or community provision where commissioned) for acute
sciatica in accordance with the NW London Low Back Pain policy (2017). (Note that injections for acute sciatica need to be offered within 3 months of referral to be clinically and cost-effective)
• Consider referral for other invasive treatments in accordance with NICE guidance (NG59, 2016) and the NW London Low Back Pain policy (2017), if the person is willing to consider these options.
• Radiofrequency denervation is effective for (some) people with severe localised low back pain arising from structures innervated by the medial branch nerves, where other non-surgical treatments have not worked for them. Consider referral for assessment for radiofrequency denervation for people with chronic low back pain in accordance with NICE guideline CG59 (2016) and the NW London LBP Policy (2017). (Review the old notes first)
• Review if a specialist has considered if other procedures covered by NICE Interventional Procedures guidance are appropriate and cost-effective for use within the NHS for this person. (Review the old notes first)

Low Back Pain and Sciatica 8
3.6 Rehabilitation, Supporting Self-Management, Discharge Planning See 2.6 above
4.0 Secondary Care Assessment • Pre-requisites: Patients should have been clinically triaged, images and reports available, referred
into a clinic that is run by a member of staff that is capable of doing the surgery. • Assess for risk of poor functional outcome as this will guide the intensity of physical and
psychological support that may be needed
4.1 Community Emergency Referrals to Hospital See ‘Referral Criteria and Triage Specification’
4.2 Community Referral Thresholds, and Triage to Hospital See ‘Referral Criteria and Triage Specification’
4.3 Supporting self-management and shared-decision-making (SDM) at all stages of the pathway See 2.3 above
4.4 Secondary Care Diagnostics • Explain to people with low back pain ± sciatica that if they are being referred for specialist opinion,
they may not need imaging • Consider imaging in specialist settings of care (for example, a musculoskeletal interface clinic or
hospital) for people with low back pain ± sciatica only if the result is likely to change management
4.5 Secondary Care Management • Offer treatments in accordance with NICE guideline CG59 (2016) and the NW London LBP Policy
(2017) (see below)
• Consider if other procedures covered by NICE Interventional Procedures guidance are appropriate and cost-effective for use within the NHS for this person. (Review the old notes first)
• Consider referral to community clinics for management (see above) only where a specific treatment recommend above has not been tried, or there has been a clinically meaningful and lasting effect (beyond the end of treatment) for previous recurrences
• Review analgesia, continue only recommended drugs that are helpful and minimise harm; paracetamol, opioids, antidepressants and gabapentinoids are not recommended for chronic low back pain without sciatica.
• Consider the risks and benefits of pursuing investigations and continuing treatments where these are of limited benefit. Instead, patients could return to primary care management, with pain clinic support where needed (BMJ 2017)
4.6 Rehabilitation, Supporting Self-Management, Discharge Planning See 2.6 above
5.1 Triage See ‘Referral Criteria and Triage Specification’
• Referrals should be clinically triaged within 48 hours
Low Back Pain and Sciatica 9
• Clinical triage should be performed by therapists and specialists with knowledge of management of low back pain
• Triage staff should have ready access to a wider multidisciplinary team including, for instance, spinal orthopaedic or neurosurgeon, pain physician, psychologist, rheumatologist, podiatrist, etc.
• Triage staff should have local knowledge and understanding about which clinics to refer to if all referral thresholds have been met
• Triage staff should feedback to GPs referrals that are not accepted and advise what alternative treatment options have been recommended
5.2 Transformation Opportunities • Opportunities - Rates of MRI scanning in different settings of care, including repeat scans rates - Medicines management for chronic pain - Referrals meeting referral thresholds and guidance (audit or triage) - Waiting times for community and secondary care - Re-referral rates for same condition - Rates of offering advice to support self-management - Providing comprehensive discharge plans - Providing feedback on the quality and appropriateness of referrals - Invasive treatment (surgery, RFD, epidurals, etc.) conversion rates from community clinics - Reducing inappropriate referrals from primary care
• Metrics across the pathway - Rates of MRI scanning in different settings of care - (Metrics to support medicines management pathway) - Waiting times to start of definitive treatment - Rates of offering advice and signposting to exercise to support self-management in all settings of
care - Outcome measure for all MSk conditions in all settings of care: MSK-HQ? • Metrics for referrals from primary care and community care - Rates of utilisation of risk stratification or other criteria for interface services - Outliers for referral rates (funnel plots) from pri care to community (by practice) and community
to sec care (by provider across NWL) - Rates of bypassing triage from GP
• Metrics for community care - Invasive treatment (surgery, RFD, epidurals, etc.) conversion rates - New to follow up ratios for community treatment pathways (including hand-offs to other services
e.g. physio to interface or injection clinics) - Rates of referral to, and completion of, group exercise or chronic pain classes - Rates of providing comprehensive discharge plans - Rates of providing feedback on the quality and appropriateness of referrals - Re-referral rates for same condition
• Metrics for secondary care - Invasive treatment (surgery, RFD, epidurals, etc.) conversion rates - New to follow up ratios (stratified by whether or not receiving invasive treatments) - Referral rates to group exercise or chronic pain classes - Absence of procedure codes in SUS data for those items decommissioned as part of NW London
Back Pain Policy - Rates of providing comprehensive discharge plans - Rates of providing feedback on the quality and appropriateness of referrals - Re-referral rates for same condition
Low Back Pain and Sciatica 10
5.3 Local and National Guidance See infographics below
• Offer treatments in accordance with NICE guideline CG59 (2016) and the NW London CCG Commissioning Policies NICE NG59 2016 NWL LBP & Sciatica Policy v4.1 2017 NWL Acupuncture Policy v4.1 2017 NWL Radio Frequency Denervation Policy v4.1 2017
• Follow local triage arrangements and referral advice, particularly on thresholds for referral and which service to refer
• Follow the NW London policy on consultant to consultant (C2C, Internally Generated Demand) referrals where: Conditions that are unrelated to the presenting problems and do not require an urgent referral; Incidental findings; Conditions that can be dealt with by the Primary Care Team without recourse to secondary care. NWL C2C IGD Policy 2014
• NHS England Elective Care Transformation Programme https://www.england.nhs.uk/wp-content/uploads/2017/11/msk-orthopaedic-elective-care-handbook-v2.pdf

Low Back Pain and Sciatica 11

Low Back Pain and Sciatica 12