Embed Size (px)
Citation preview

Pathology in Endodontics
Bobby M. Collins, DDS, MS
College of Diplomates8th Annual Board Review CourseSaturday, February 17, 2018San Antonio, TX

References:
• Oral and Maxillofacial Pathology, 4th Ed. Neville, Damm, Allen, and Chi
• Oral Pathology: Clinical Pathologic Correlations, 7th Ed. Regezi, Sciubba, Jordan
• Oral and Maxillofacial Surgery Clinics of North America: Pediatric Oral and Maxillofacial Pathology, February 2016. Kolokythas, Miloro
• Cohen’s Pathways of the Pulp, 11th Ed. Hargreaves, Berman. Chapter 15

Domed masses on the gingiva
• Reactive processes, very common, F>M
• The 4 Ps
– Pyogenic granuloma
– Peripheral fibroma
– Peripheral ossifying fibroma
– Peripheral giant cell granuloma

Ulcers and Erosions
• Aphthous stomatitis
– Painful, round, ovoid ulcer, tan pseudomembrane coat, fiery red halo occurs on loose, non-keratinized mucosa
• Herpes simplex lesions (labialis, oralis)
– Painful, but not like aphthae, jagged erosions that follow collapse of preceding vesicle
– Merge and fuse to form larger erosion
– Recurrences occur on keratinized mucosa

Bone
• Response to trauma, irritation, inflammation– Osteolytic (Radiolucent) – more ominous– Osteoblastic (Radiopaque)– Diagnostic caveat – make sure you see the entire extent
of the lesion radiographically• All margins of the lesion, assess adjacent anatomy, teeth
• Some reactive processes, fibro-osseous lesions, neoplasms produce osseous matrix– There are varying degrees of lytic and blastic activity
over the maturation of the lesions

Voroscopes co. uk

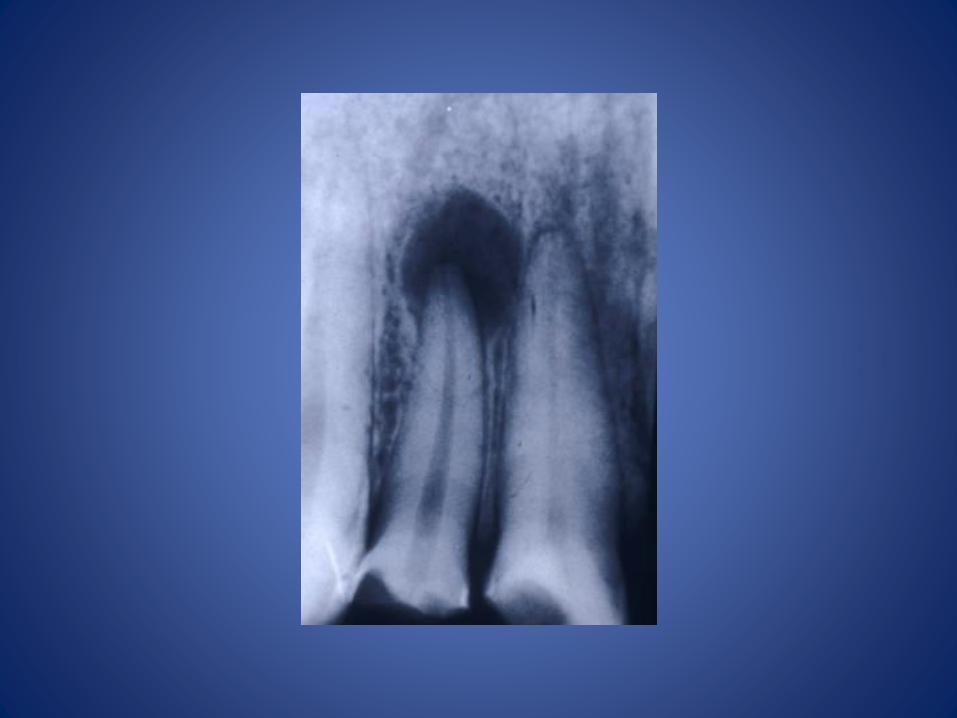
Periapical Lesions
• ~90% of all periapical lesions result from periapical periodontitis
– A radiolucency noted at the apex of a tooth
– Host response to microbial challenge (infection) and necrosis in root canal system
– Histopathologically, lesions are periapical granulomas or periapical cysts, abscesses, scars with variable numbers of acute or chronic inflammatory cells

Radiolucencies
• Consider
– Anatomical location
• Sinus, foramina, nutrient canal, Stafne bone cavity
– Association with:
• Teeth, and structures listed above
– Patient age (developing teeth, odontomas, ameloblastic fibroma)
– Trabecular pattern
• Coarse, open, linear, “ladder rung”

Periapical Radiolucencies
• Inflammation (PA granuloma, PA cyst)
• Mental foramen– Mandibular premolar region
• Periapical Cemento-osseous dysplasia– Mandibular anterior teeth
• Focal cemento-osseous dysplasia– Mandibular premolar region
• Florid cemento-osseous dysplasia– Multiquadrant

PCOD


Focal Cemento-osseous Dysplasia

Florid Cemento-osseous Dysplasia

Periapical Radiolucencies cont.
• Developing tooth
• Periapical scar (prior endo or surg at apex)
• Incisive canal cyst
• Stafne bone cyst
• Traumatic (simple) bone cyst
• Lateral periodontal cyst
• Pneumatization of the alveolar ridge
• Neoplasia

“One person’s (tooth’s) floor is another’s ceiling”Dental follicle in tooth embedded in fibrous dysplasia

Pneumatization

TBC

38 yo M
• RCT #9 many years ago
• Clinical exam in AEGD clinic Dec. 2017
– Facial swelling #9, tender to palpation
– Rx Amoxicillin 500 mg, and scheduled for apicoectomy
• Jan 2018, apicoectomy with soft tissue submission
• Rx Clindamycin 150 mg

Brain CheckWhat’s this?

73 yo F
• Clinical Description: Radiolucency left body of mandible associated with teeth #19 and #20. Endodontic testing equivocal in tooth #20. Tooth #19 had RCT performed previously. Aspiration of 2 cm x 1.5 cm lucent area several weeks ago yielded serosanguinous fluid.



58 yo F
• Clinical Description: 1cm x 2cm area of mixed radiolucency/radiopacity of the right mandible in a patient with florid cemento-osseous dysplasia. The patient has a history of an intra-oral draining fistula along the alveolar crest.
• Clinical Impression: Sequestration of bone secondary to florid cemento-osseous dysplasia.
• Procedure: Hard tissue excisional biopsy.


31 yo F
• MH significant for Sickle Cell Anemia
• Crisis 2 x in last year
• Port a cath in right upper chest due to scarring in antecubital fossa.
– No AB premed per patient






WHO Histological Typing of Odontogenic
Tumours
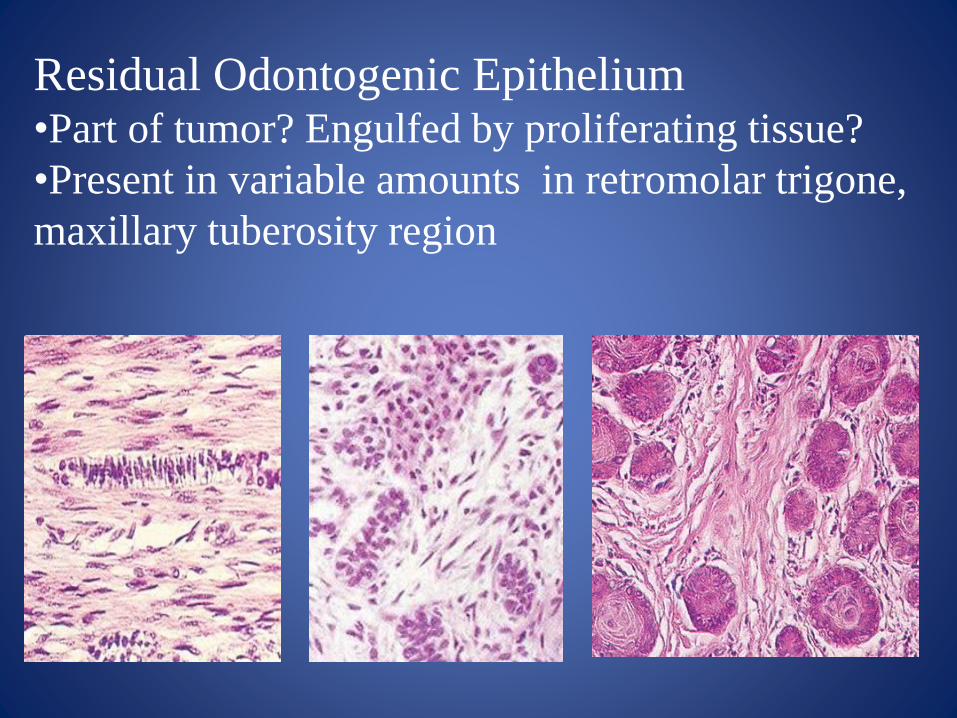
Residual Odontogenic Epithelium•Part of tumor? Engulfed by proliferating tissue?
•Present in variable amounts in retromolar trigone,
maxillary tuberosity region

Proliferating odontogenic epith.
• Squamous odontogenic tumor
–Bland appearing, variably-sized squamous epithelial islands
–Can be bilateral
–Cause vertical bone loss – like periodontal disease
– S.O.T – like change is noted in wall of many odontogenic cysts (DC, OKC, GOC)

Modern Pathology
Regezi
Squamous odontogenic tumor

Anatomic locations of common jaw cystsG- gingival cyst
E- eruption cyst
L- lateral periodontal
R- residual cyst
P- periapical cyst
D- dentigerous cyst
OKC – odontogenic
keratocyst
Contemporary OMP Sapp, Eversole, Wysocki
Periapical Periodontitis
– Radiolucency at apex (root end) of non-viable tooth
– Asymptomatic, unless acutely inflamed
– Tissue reaction to bacterial toxins in root canal system
– Granulation tissue from severed blood supply at apex of tooth
• Intrusion, rotation, avulsion of tooth can compress or shear blood vessels

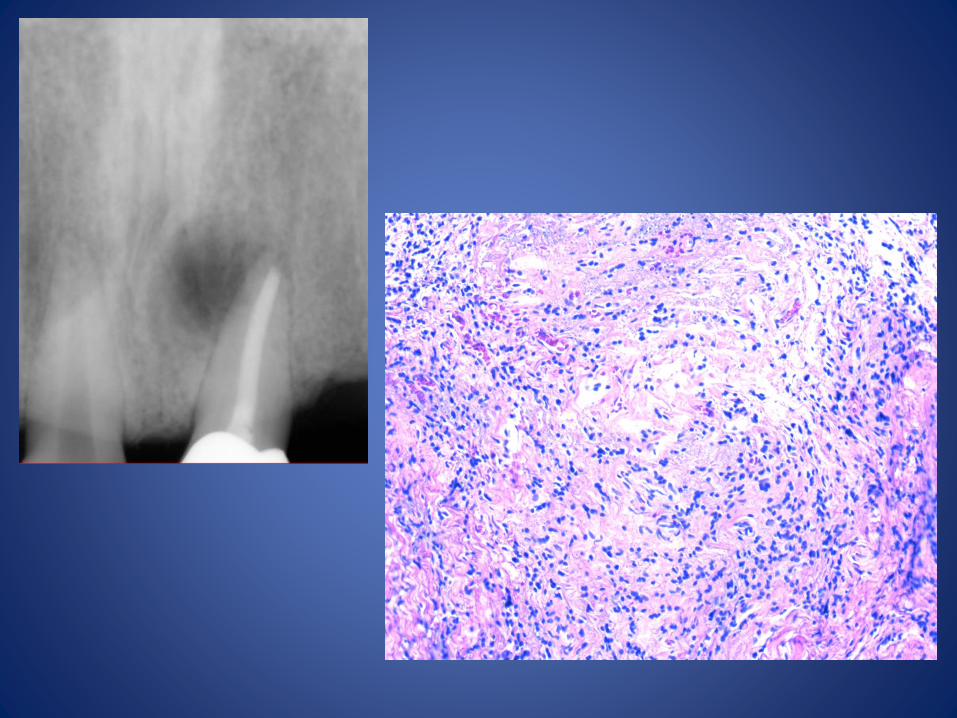
Periapical periodontitis cont.
• Histology: – Granulation tissue, variably dense lymphocytic infiltrate
admixed with PMNs, plasma cells, histiocytes, and rimmed by dense fibrous CT
– Odontogenic epithelial rests may be noted
– When plasma cells abundant, Russell bodies and pyronine bodies are present
– Black, brown, granular foreign material is evidence of root canal therapy
• If eosinophils are noted, think Langerhan cell histiocytosis (S-100, CD-1a, CD-207)


Histiocytes,
lymphocytes in delicate
vascularized
fibrous CT

Periapical cyst• Inflammatory cyst associated w/ non-vital tooth
– Most common odontogenic cyst– Carious or traumatic etiology, begins as periapical
granuloma– Inflammation stimulates epithelial rests of Malassez
• Radiograph – Well-defined radiolucency at root apex
• Histology– Luminal SSE, edematous w/ PMN exocytosis– Hyperplastic epithelium has a loop and arcade
architecture– Connective tissue shows lymphoplasmacytic infiltrate,
foamy histiocytes, acicular bodies (cholesterol clefts)• Treatment – endodontic therapy/apicoectomy

Hyperplastic epithelium within inflamed granulation tissue

Rushton bodies:
Non-keratin secretory
product
of odontogenic epithelium
Eosinophilic, curvilinear,
hairpin-like and birefringent
WHO

Brain Check
What’s this?
Odontogenic Keratocyst (OKC) cont.
• Histology– 6-8 cell layer thick, SSE lining, “wavy”, “ruffled”,
“corrugated” parakeratin– Lumen is serum filled or “cheesy” from the shed,
laminated parakeratin– Cuboidal or columnar, hyperchromatic, palisaded basal
layer– Flat epithelial interface with CT, unless inflamed– Satellite or daughter cysts in CT wall in ~ ¼ cases
• Treatment – Enucleation, peripheral ostectomy– Irrigation with Carnoy’s solution (EtOH, Acetic acid)– OKC’s tend to recur
• 30-40% reported in large studies (Brannon, RB)• As high as 60%

Hyperchromatic, columnar
basal layer 6-8 cells thick,
wavy parakeratotic surface

Dentigerous Cyst
• Developmental cyst (separation of follicle from crown)
– Arises during tooth development (2d-3d decade), M>F
– Second most common, 20% of jaw cysts
• Well-corticated lucency around unerupted crown
– Attached at cervical of tooth, third molars most commonly
– Pericoronal lucent appearance mimicked by other cysts/tumors
• 1-2% OKC, 1-2% benign odont tumor, 1% MEC, ameloblastoma, SCCa
– Can fill mandibular body and ramus completely
– Can move tooth bodily, cause root resorption, jaw expansion, and can thin cortex

Dentigerous Cyst continued
• Histopathology- can vary if inflamed
– Epithelial hyperplasia, rete peg formation
– Loop and arcade array (can resemble PA cyst)
• Non-inflamed cyst
– 2 - 4 cell layer thickness, luminal cuboidal epithelium (reduced enamel epithelium)
– Mucous, ciliated, sebaceous cells (metaplasia) may be evident
– Discontinuous proliferating epithelium is more pronounced in inflamed cysts, but it is not uncommon
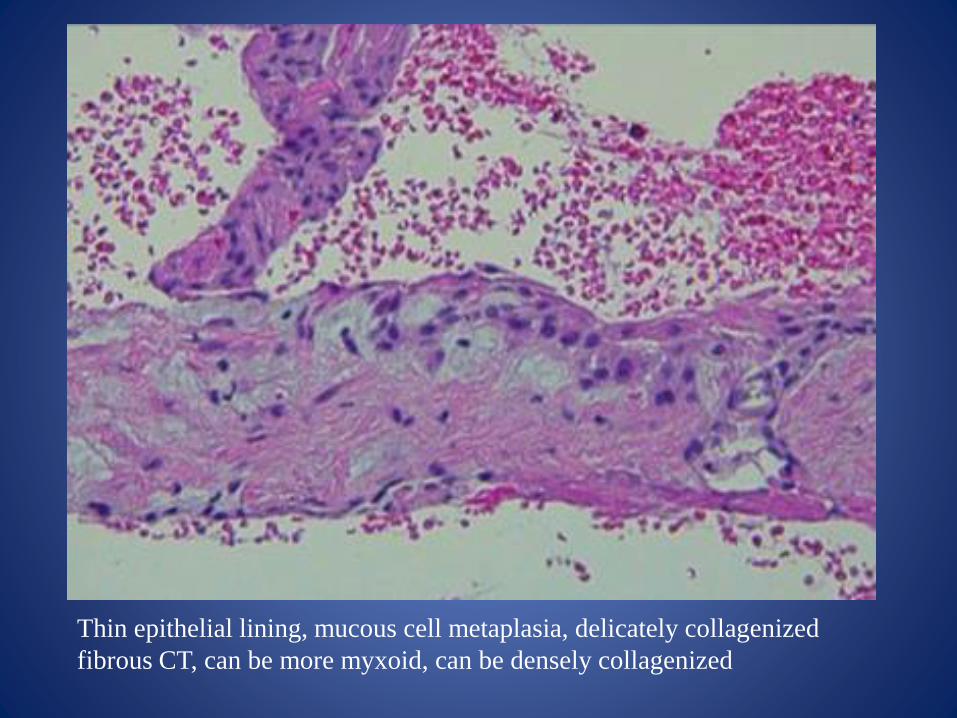
Thin epithelial lining, mucous cell metaplasia, delicately collagenized
fibrous CT, can be more myxoid, can be densely collagenized

Hyperplastic epithelium in inflamed
dentigerous cyst

MCV and USCWell-corticated lucency between the roots
of vital teeth

Lateral Periodontal Cyst cont.
• Histology
– Thin SSE lining with cuboidal cell component, clear cells, focal plaque-like thickening
– Thin, non-inflamed, fibrous connective tissue wall
– Clear cell epithelial rests may be seen in wall
• Treatment
– Enucleation

OSU, USCThin squamous, cuboidal epithelium with focal
plaque-like thickening. Glycogen rich clear cell
change is common

Nasopalatine duct cyst(Incisive canal cyst)
• Midline ant. MX, most common non-odont. cyst• Cystic degeneration of nasopalatine duct
remnants• 4th to 6th decade, palatal swelling, drainage, pain• Radiograph: pear or heart-shaped lucency,
sclerotic border, between mx central incisors• Histo: Epith. varies, (SSE, respiratory, simple
columnar or cuboidal). Moderate-sized nerves, arteries and veins. Cartilage and mucous glands occasionally

Oral and Maxillofacial Pathology 3rd Ed

Oral and Maxillofacial Pathology 3rd Ed
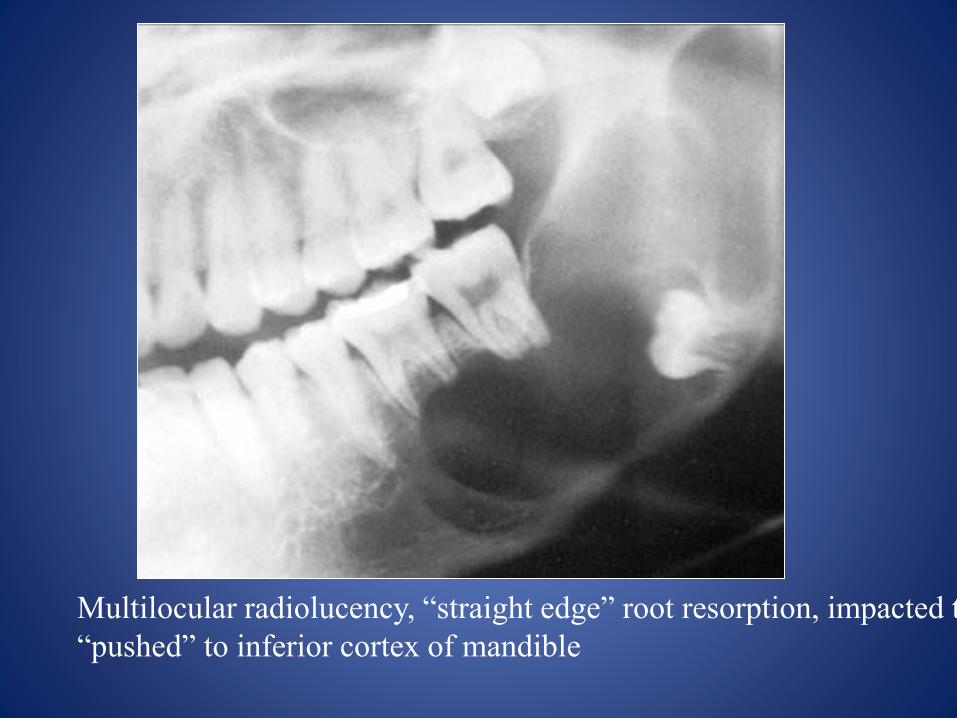
Multilocular radiolucency, “straight edge” root resorption, impacted tooth
“pushed” to inferior cortex of mandible

WHO
Columnar basal cells,
peripheral palisade, centrally,
loose stellate reticulum.
Inductive effect on CT

Ameloblastoma HistopathologyClassic features described by:
Vickers RA, Gorlin RJ. Cancer 1970;26(3):699-710
• Peripheral epithelial cells are tall, columnar and have hyperchromatic nuclei
• The nuclei exhibit reverse polarity, that is they have pulled back from the basement membrane area
• The nuclear polarization leaves a subnuclear vacuole
• Mimics embryologic tooth bud development during enamel matrix production
“There is nothing more deceptive than an obvious fact.”
“When you have eliminated the impossible, whatever remains, must be the truth.”
Arthur Ignatius Conan Doyle

Child with LCH
OMFP Neville

Langerhan Cell Histiocytosis
• Myeloid neoplasm of dendritic antigen presenting cells– Cells commonly found in skin, marrow, lymph
nodes
– Common in pediatric population• Eosinophilic granuloma (solitary, bone involvement)
• Hand-Schuler-Christian Dis (chronic disseminated –involves skin, bone, viscera)
• Letterer – Siwe dis. (infants, multiorgan involvement, hepatosplenomegaly, lymphadenopathy, bone, skin, pancytopenia)

LCH
• Calvarium and mandible commonly affected
• Alveolar bone loss “teeth floating in air” mimics periodontal disease
• BRAF gene mutation
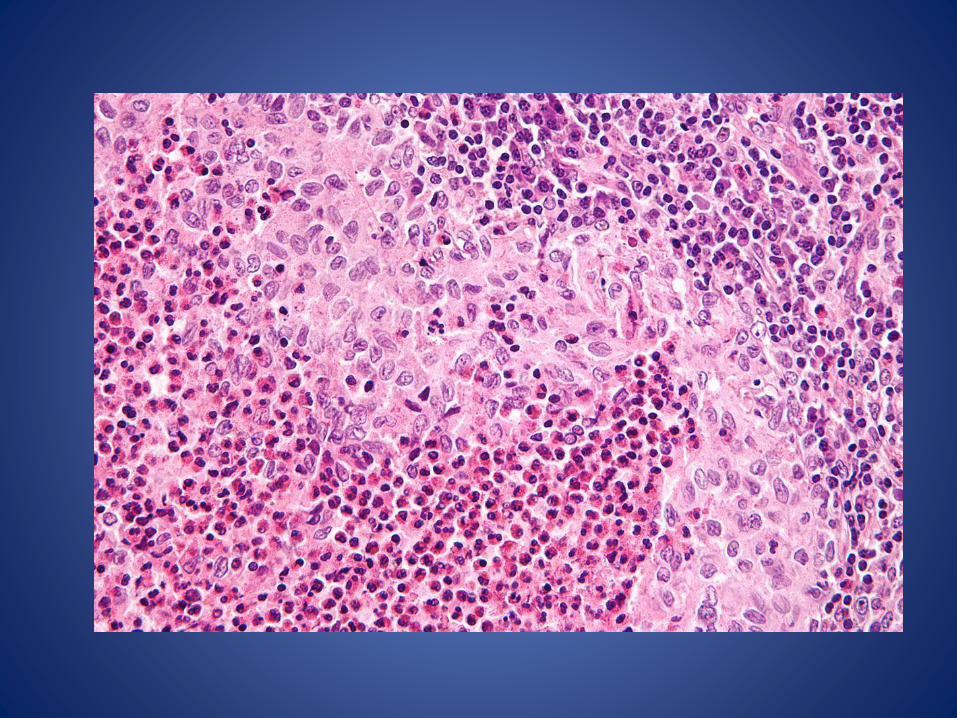
• Histology: LC, eosinophils, lymphocytes, macrophages, multinucleatd giant cells
– LC stain w/ S-100, CD1A, CD207 (Langerin)
– Ultrastructurally LC contain Birbeck granules

Focal Osteoporotic Bone Marrow Defect
• More common in post menopausal females
• Found incidentally, and not until several mm to cm in size
• Not pathologic
• Likely due to aberrant healing following extraction –most are in posterior mandible, edentulous areas
• Marrow response to increased red cell demand
• Well or ill-defined lucency dependent upon series (pano –well, PA- ill defined with thin wispy septation)
• Histopathology: Cellular or fatty bone marrow


Stafne Bone Defect
• Well delineated asymptomatic radiolucency
• Anatomic concavity on lingual cortex of mandible, beneath the inferior alveolar canal– Lucency tends to have dense sclerotic border
– Adults>Children
– Concavity accommodating SMG, SLG, even tail of parotid
– Sometimes depression is empty, sometimes fat or skeletal muscle present

Central Giant Cell Granuloma
• F>M, wide age range, ave 30yrs, 70% mandible• Most are non-aggressive
– Small, few symptoms, no cortical perforation or root resorption
• Some appear locally aggressive– Pain, rapid growth
• Uni or multilocular, well delineated, non-corticated borders
• 5 mm – 10 cm in size, can expand and perforate cortex

CGCG
OMFP Neville


What are these eosinophilic curvilinear structures?

Trabecular pattern in bone
• Trabeculae- thin lines of bone that cross each other in an irregular pattern– Lines are separated by dark spaces – marrow
– White strands- bone, and dark spaces marrow produce a network pattern with normal variations in size and shape
– Pathologic patterns have been described as ground glass, orange peel, granular, permeative, geographic, honeycomb and moth-eaten
• Patterns: open, coarse, linear, wispy


Questions?

• Question 1. A periapical radiolucency persists following conventional endodontic therapy. Apicoectomy with tissue submission is done. Microscopic examination shows filamentous bacterial organisms surrounded by neutrophils. The diagnosis is:
• A. Chronic periodontitis and plaque bacteria
• *B. Periapical periodontitis with Actinomycotic organisms
• C. Periapical scar
• D. Parulis

Question 2. A biopsy of a lucency at the apex of tooth #8 shows a mixed inflammatory infiltrate and granulation tissue (immature capillaries, plump endothelial cells and fibroblasts. The diagnosis is:
• A. Periapical cyst
• B. Eosinophilic granuloma
• C. Granulomatous inflammation
• *D. Periapical periodontitis

• Question 3. A radiolucency is noted midroot at the mesial of tooth #21. The patient is asymptomatic and tooth tests vital. A biopsy reveals a cyst lumen of single layered cuboidal cells with scattered areas of plaque-like thickening and clear cells.
• Your diagnosis is:
• A. Odontogenic keratocyst
• B. Keratocystic odontogenic tumor
• *C. Lateral periodontal cyst
• D. Squamous odontogenic tumor





























