-
8/8/2019 Pathology and Pa Tho Genesis of Arthritis
1/6
Pathology and Pathogenesis of Arthritis
Overview
This module gives an overview of the pathogenesis and pathology
first of osteoarthritis and, secondly, ofrheumatoid arthritis.
Specific Objectives:
Upon completion of this module, the student will be able to:
1. Discuss the pathogenesis of OA, identifying genetic,
mechanical, cellular, metabolic and biochemicalfactors
involved.
2. Describe changes in the joint that occur as OA progresses.3.
Identify factors that may influence the pathogenesis of RA,
including genes, immune complexes,
cytokines and viruses.
4. Describe changes in the joint that occur as RA
progresses.Date of in-class session:
This unit is complementary to the Arthritis sessions and should
be completed prior to the second Arthritis TBL
(January 19). The Approach to Arthritis exercise and
Monoarthritis, and Polyarthritis modules should becompleted prior
to this module, as indicated in the Learning Map.
Estimated preparation time: 60 minutes
Required preparation:
1. Read1. Cecil's Essential Ch 87, pp.779-780. "Osteoarthritis".
Subsection titled Pathology. (see FAQs).2. Cecil's Essential Ch 78,
pp.735-736 "Rheumatoid Arthritis". Subsections titled Pathology
and
Pathophysiology; also see Table 78-1 and Fig. 78-1. (see
FAQs).3. Maksimowicz-McKinnon, K Rheumatoid Arthritis (Cleveland
Medical clinic) - pathophysiology
section.4. PostGraduate Medicine module on OA. Pathogenesis
section. Table 1 and Table 2.
2. Work through this module
Pathogenesis of Osteoarthritis
Osteoarthritis attacks weakened joints. In idiopathic (primary)
OA, hormonal, genetic, metabolic and mechanicalfactors appear to be
implicated but the etiology remains unclear. In secondary OA, all
of these factors one factoris identifiable as the primary cause.
Often in secondary OA, mechanical causes are primary and the
affected
joint(s) has (or have) been exposed to previous trauma involving
repeated and/or excessive loading of thejoint(s). Congenital and
development deformities, neurologic disorder and pre-existing
arthritis may also incite
secondary OA.
Factors that may contribute to the development of osteoarthritis
are explored further below:
Genetic and Hormonal Factors Mechanical Factors Cellular and
Metabolic Factors Biochemical Abnormalities
-
8/8/2019 Pathology and Pa Tho Genesis of Arthritis
2/6
Genetic and Hormonal Factors
As seen in the Osteoarthritis section of the Polyarthritis
module, idiopathic OA is more frequently seen in womenand is
hereditary. Mutations in collagen genes (types II, IX, X) appear to
contribute to the development ofpremature idiopathic OA. Heberden's
nodes are symptomatic of a particular hereditary form of OA thought
to be
associated with a gene that is recessive in males and dominant
in females.
Mechanical Factors
The composition and structure of articular cartilage define its
mechanical properties, making it well-suited toabsorb shock, bear
weight, and defining how much weight is too much. Articular
cartilage is composed of cells(chondrocytes), surrounded by a
matrix and immersed in water. The matrix is 60-80% water, with
collagen,proteoglycan and glycoprotein macromolecules making up the
remainder of its structure. Each chondrocyte cell is
surrounded by matrix and is nourished primarily via synovial
fluid in the joint.
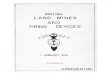
Schematic of articular cartilage structure. Not to scale.
Redrawn from Wroble, 2000.Synovial membrane (SM), articular
cartilage (AC), bonespicules (bo) and bone marrow spaces (m) in a
synovial
joint. University of Ottawa Histology
Like all weight-bearing structures, articular cartilage has a
critical stress (force per unit area) which it cantolerate and
above which, it begins to break down. When the joint is exposed to
stresses above this critical value,
the unit load on the chondrocytes becomes too high and
overburdened chondrocytes begin to die. The death ofchondrocytes
cells weakens the matrix by stopping chondrocyte homeostasis in
those cells; this leads todegradation of the articular
cartilage.
An increased unit load on the chondrocytes may also be the
result of changes in the subchondral bone. In Paget'sdisease, for
example, damage to the coarse cancellous bone ofteh epiphysis may
cause an increase in thestiffness of the subchondral bone. This, in
turn, increases the unit load on the chondrocytes and increases
the
likelihood that articular cartilage will eventually degrade and
OA will develop.
Cellular and Metabolic Factors
In hemochromatosis, excessive iron absorption may contribute to
joint pain and the development of OA. In
ochronosis, pigment may be deposited in articular cartilage,
contributing to the development of OA in the joint.
Biochemical Abnormalities
Changes in composition of articular cartilage contribute to the
development of OA. As healthy articular cartilageages, its water
content decreases. In osteoarthirtic cartilage, water content
increases, contributing to the
tendency for this cartilage to swell more than normal. Collagen
fibres become thicker than normal and morewater binds to these
cllagen fibres. Proteoglycan content and aggregation are both
decreased and the length ofglycosaminoglycan chains is
shortened.
These changes are summarized succintly in Table 1 of this
PostGraduate Medicine module on OA.
-
8/8/2019 Pathology and Pa Tho Genesis of Arthritis
3/6
Chondrocytes bearing excessive loads eventually cease to respond
to reparative stimuli, as a result proteinsynthesis by chondrocytes
also decreases. Acid cathepsin attacks protein cores and is
increased in OA cartilage.
Collagenase is found in OA cartilage.
Pathology of Osteoarthritis
As OA progresses, structures in the joint degenerate. First, the
articular cartilage breaks down, exposing thesubchondral bone,
which then becomes damaged. Eventually osteophytes form. These
changes are discussed in
more detial below:
Changes in articular cartilage Changes in subchondral bone
Development of osteophytes
Changes in articular cartilage
Loss of Proteoglycans - Histology of osteoarthritic articular
cartilage indicates a decrease in proteoglycans fromthe surface of
the articular cartilage, evidenced by a decrease in metachromatic
staining.
(IMAGE?)
Chondrocyte Cloning - As chondrocytes in overloaded cartilage
die, empty lacunae are visible under themicroscope. The remainining
viable chondrocytes aggregate into groups in a process termed
chondrocyte cloning.
Fibrillation - The first macroscopic change in the
osteoarthritic joint is the fibrillation of the cartilage.
Multiple, tinysurface cracks develop first in the superficial layer
of the articular cartilage and gradually deepen. Synovial
fluidflows into these cracks and, as deeper layers of cartilage
fibrillate, pieces break off, lodging in the synovium and
leaving the subchondral bone increasingly exposed.
Secondary Synovitis - Fragments of cartilage and bone join to
form osteocartilaginous loose bodies in the jointspace. The
presence of these bodies in the synovium elicits a foreign-body
type inflammatory reaction, causing
the synovium to become hyperemic and hypertrophied.
Changes in subchondral bone
In the region where the articular cartilage is cracked and
fibrillated, the subchondral bone responds by forming
new blood vessels (neovascularization). This process induces
osteoclastic bone resorption and increased activityin adjacent
osteoblasts, resulting in a thickening of the subchondral bone in
the exposed area.
Fibrocartilagenous plugs - As neovascularization continues,
mesenchymal cells invade (the subchondral bone?where?) and form
fibrocartilagenous plugs to replace articular cartilage which has
broken off. These plugs fill the
empty space left by degraded cartilage but are poor substitutes
functionally and wear out quickly.
Eburnation - The subchondral bone becomes exposed such that it
grinds against the opposite joint surface. As thejoint moves, this
grinding burnishes the exposed bone. It becomes eburnated -
polished, shiny and smooth, with
an appearance like ivory.
-
8/8/2019 Pathology and Pa Tho Genesis of Arthritis
4/6
Eburnated osteoarthritic patellae are thick, shiny and
smooth with an appearance like ivory. (PEIR
PathologyLibrary).
Exceptionally large subchondral bone cyst in 70-year oldwith
degenerative arthritis that raised concern for aneoplasm. At
surgery the cyst contained gray, semi-liquid
fluid. The defect was packed with bone chips. (PEIRPathology
Library)
Subchondral bone cysts - These cysts form when synovial fluid
flows into the bone marrow space following acrack in the eburnated
subchondral bone.
Development of osteophytes
In advanced OA, bony spurs called ostephytes develop when
mesenchymal tissue of the synovium modulates intoosteoblasts and
chondroblasts to form a mass of bone and cartilage. Mechanially,
osteophytes serve to increase
the load-bearing area on the joint thus decreasing the load per
unit area (i.e. stress). Osteophytes most oftenappear on the
periphery of the joint.
Osteoarthritic femoral head showing osteophytes, bone
overgrowth, along with evidence of ochronosis and melanin. Note
the pearly greyish appearance of the osteophytes. PEIR Pathology
Library.
Pathogenesis of Rheumatoid Arthritis
The etiology of RA is unknown. Various factors appear to
influence the pathogenesis of the disease, including
Genetic Factors Humoral Immunity Cellular Immunity Infectious
Agents
Genetic Factors
Patients with RA are found to have certain genetic features,
including an important genetic locus in HLA genes.Increased risk of
RA is associated with the presence of a specific set of HLA-DR
alleles.
These alleles share a pentapeptide sequence of AA's that forms
the rheumatoid pocket on the HLA molecule.
-
8/8/2019 Pathology and Pa Tho Genesis of Arthritis
5/6
Humoral Immunity
The synovium of RA patients shows certain abnormalities. Ig's
are produced in the synovium due to anaccumulation of lymphoctes
and plasma cells. Immune complex deposits are present in the
synovium and
articular cartilage.
Serum levels of certain immunoglobulins (IgM, IgA, IgG) are
increased in RA patients. Rheumatoid factor (RF) isand IgM which is
present in 70%-80% of patients with classic RA. The presence of RF
is associated with moresevere disease, though RF is also found in
some people who do not have RA.
Cellular Immunity
Activated, helper-type T lymphocytes infliltrate the rheumatoid
synovium. These T cells interact withmacrophages directly or
indirectly to produce an excess of pro-inflammatory cytokines, such
as TNF and IL-1.These contribute to inflammation in the synovium
and subsequent joint destruction.
Infectious Agents
Structures resembling viruses have been reported early in the
course of the disease. High incidence of B cells andantibodies to
Ebstein-Barr Virus (EBV) in RA patients suggests EBV may play a
role in inciting RA. EBV is a
polyclonal B-cell activator that stimulates production of
rheumatoid factor.
Pathology of Rheumatoid Arthritis
The joint pain and inflammation in RA the result of synovitis
and synovial pannus within the joint. This eventually
leads to changes in the peri-articular bone and soft tissue in
the area of the joint.
Changes in synovial membrane Changes in peri-articular bone
Changes in soft tissue Synovial fluid
Changes in synovial membrane
Early changes in the synovium include:
edema, lymphocytes, plasma cells, macrophages increased
vascularity exudation fibrin in joint space (formation of rice
bodies)
Hyperplasia and hypertrophy of synovial lining cells causes
these cells to creep over adjacent structures,including articular
cartilage. This creeping synovial lining is called pannus. It fills
the periphery of the joint,
cutting off the articular cartilage from the nourishment of the
surrounding synovial fluid.
Eventually the joint is destroyed and ankylosis occurs, fusing
the fibrous tissues in the joint. This is eventuallyfollowed by
bony ankylosis, where apposing bones acutally fuse in the destroyed
joint.
-
8/8/2019 Pathology and Pa Tho Genesis of Arthritis
6/6
Changes in peri-articular bone
As articular cartilage becomes completely degraded, the bone at
the sides of the joint begins to erode, probably
due to a factor elaborated locally by rheumatoid synovium.
Progressively worsening bone erosion. From the ACR High Impact
Rheumatology slide collection.
Changes in soft tissues
Rheumatoid nodules may form in subcutaneous tissue.
Macroscopically, zones of fibrinoid necrosis can beidentified in
these nodules. Microscopically, zones of necrobiosis are seen,
surrounded by pallisading histiocytes.
Gross view of a rheumatoid nodule on lung tissue. PEIR
Pathology Library.
Rheumatoid nodule under the microscope, in the heart.
PEIR Pathology Library.
Synovial fluid
Aspirated rheumatoid synovial fluid has increased turbidity and
decreased viscosity compared to normal synovialfluid. Inflammation
causes the volume of fluid to increase, with increased content of
both polymorphonuclear
lymphocytes (PMNL's) and proteins.
Review Exercise and Summary
Review what you have been learning about the pathogenesis and
pathology of OA and RA. If you are not sure ofyour answers, follow
the links to go back to the relevant part of the module.
Use the Back button on your browser to return to this page.
Identify factors that are involved in the development of
idiopathic OA. Contrast changes in osteoarthritic articular
cartilage with those seen in cartilage that is aging normally.
Describe the degradation of an osteoarthritic joint, identifying
the chronology in which various
structures are affected.
List factors that are thought to contribute to the development
of RA. Describe the changes in the synovium of a joint affected by
RA.