Embed Size (px)
Citation preview

Pathologic Anatomy of the Pancreas inJuvenile Diabetes Mellitus
Willy Gepts, M.D., Brussels, Belgium
SUMMARY
1. Quantitative study of insular tissue has revealed thatthe number of B cells is greatlyacute juvenile diabetes from the time of clinical onset oftKeTctisease. The number of these cells is as a*niTe"less than10 per cent of normal. Such B cells as are still present showthe cytological signs of marked activity.
2. The normal or supranormal insular activity that isusually found in juvenile diabetics in this stage of thedisease cannot therefore be due to the presence of a nor-mal insular tissue, but is produced by a small number ofhyperactive B cells.
3. On the basis of histological findings (presence ofislets of large size, signs of new islet formation), it maybe assumed that during the preclinical phase of juvenilediabetes, an extrapancreatic factor has exerted a strongstimulant action on the insular tissue. In the long run thismust lead to exhaustion of the islet-forming capacity onthe pancreatic parenchyma and to a decrease in the num-ber of the B cells. By the time the disease becomes clinicallymanifest only the latter stage of this process can be ob-served and the majority of islets consist of A cells or ofatrophic tissue devoid of B cells.
4. Peri- and intra-iiisttlax inflammatory infiltrates havebeen found in 68 per cent of those patients with juvenilediabetes who died soon after the clinical onset of theirdisease. In other words, and contrary to the generally heldview, this lesion is not uncommon. It is specific for diabetesand has never been observed in the rhmmir mnrft
^r.—in patients with chronic juvenile diabetes, the B cellsare completely absent, except in occasional cases. The isletsconsist of small, atrophic cells.
6. A valid assessment of the functional capacity of in-sular tissue can only be achieved if as much use as pos-sible is made of quantitative technics and of cytologicalexamination. DIABETES J4:619-33. October 1965.
Clinical, biological and histological findings have ledto the classical view that juvenile diabetes results froman absolute deficiency of insulin secretion, due to severeinadequacy of the insular tissue.
Nevertheless, recent investigations1*2 have revealed
From the Department of Pathology of the University ofBrussels, Brugmann University Hospital, and the FondationMedicale Reine Elisabeth, Belgium.
that the serum of recent onset juvenile diabetics showsan insulin-like activity that is normal or even higherthan normal. Furthermore, Maclean and Ogilvie3 re-ported that the pancreas of juvenile diabetics who diesoon after the clinical onset of their disease containslarge islets and that in such patients both the relativeand total mass of insular tissue are often only slightlyless than normal.
Such observations are of obvious interests They leadone to consider that the inadequacy of the insular tis-sue, which one is often inclined to regard as congenital,may not in fact be primary in nature, but only the latestage of a progressive deterioration under the influenceof an extrapancreatic diabetogenic factor.
In view of this new aspect of the physiopathology ofjuvenile diabetes, we have resumed the study of the pan-creas of the young diabetic patient. Most of the workpreviously done in this field was performed prior to thedevelopment of modern technics for the demonstrationof the various types of insular cells, and at a time whenour knowledge of the physiopathology of the diseasewas as yet rudimentary.
In collecting the material to be used in this study, weattempted to include as many cases as possible of juve-nile diabetic patients who had died soon after the clinicalonset of their disease.
MATERIAL AND METHODS
The material for our study consisted of fifty-four pan-creases from young diabetic patients in whom the onsetof the disease had occurred prior to the age of thirty-one.Of these patients, twenty-two had died less than sixmonths after the onset of the first symptoms of diabetes(in most cases: weight loss, polydipsia and polyuria).In the remaining cases, the disease had been knownfrom one to thirty-seven years. Most of these cases havebeen kindly provided by the Departments of Pathologyof the principal hospitals of Boston and Philadelphia.Others, including twenty-six pancreases from nondiabeticpatients serving as control material, came from theDepartments of Pathology of the two University hos-
OCTOBER, 1965 619

PATHOLOGIC ANATOMY OF THE PANCREAS IN JUVENILE DIABETES MELLITUS
pitals at Brussels. The origin of the cases, the age andsex of the patients, and the duration of the diabetesare shown in tables 1-3.
Because of the diverse origins of this pancreatic ma-terial, it is understandable that the quantity availablefor study and the methods of fixation were variable. Inall but one case (Case 18) paraffin blocks were pro-vided. Their number varied from one to five. In manycases routinely stained sections or pieces of wet tissuewere also available. The fixative that had been used was:formalin (25 cases), Zenker (18 cases), Romeis (7cases), Bouin (4 cases).
For Case 18, six Gomori stained sections of fairlywell preserved pancreatic fragments were available. Inall the other cases we stained the sections with hemalumerythrosin saffron and with the chromium hematoxylinphloxine method of Gomori. In those cases in which asatisfactory differential staining could not be obtainedin newly made sections from paraffin blocks or from wettissue, restaining of decolorized routine sections was
tried. Decolorization was achieved by oxidation with apermanganate-sulfuric acid mixture, which representsthe first step in the classical Gomori chromium hema-toxylin method. This procedure yielded satisfactory re-sults in two cases only (cases 9 and 16). In most of theacute and several of the chronic and control cases wealso performed Dominici's method (toluidine blueerythrosine orange) or the methyl green pyronine meth-od, with or without previous digestion in a 0.1 per centsolution of ribonuclease (120 min. at 370 C ) .
In forty cases (twenty-two acute, eighteen chronic),the proportion of islet tissue in the pancreatic paren-chyma and the size of the islets were assessed. Fourteencases (26 per cent) (cases forty-one to fifty-four) wererejected from this part of the study because of un-satisfactory definition of the outlines of the islets. Todetermine the proportion of islet tissue and the size ofthe islets the sections were scanned systematically undera Leitz Panphot and all the islets encountered weredrawn at a magnification of 250 X. The contours of
TABLE 1
Cases of acute juvenile diabetes
Case OriginH
123456789
10111213141516171819202122
B.G. 55/145E.C.H. 53/9N.D.H. 43475Ch.H.Ph. 1928S.P. 57/130Ch.H.B. 60/184C.H. 61/43Ch.H.Ph. 56/85M.G.H. • 9677-M.GJL 10938N.D.H. 197176M.G.H. 9381M.G.H. 14089M.G.H. 11301tM.G.H. 8275StM.H. 56/103U.P.H. 59/200Ph.G.H. 60/397U.P.H. 55/99S.P. 56/237N.H. 48/91B.H. 58/112
Age
11 mos.11 mos.11 mos.
1 yr. 3 mos.2 yrs.
2 yrs. 10 mos.3 yrs.
3 yrs. 6 mos.6 yrs.
9 yrs. 6 mos.13 yrs.15 yrs.15 yrs.15 yrs.15 yrs.15 yrs.15 yrs.16 yrs.17 yrs.21 yrs.22 yrs.30 yrs.
SexFMMMFMFMMMFFFFFMFMMFMM
Knownduration of
diabetes(days)
33
1490
960304515
4146090213016
180411
1490
Weightof
pancreas(gm.)
87.5—15—2520252040—4980
—50—50756055
Numberof islets
per cm2 ofpancreatic
tissue76
17612478
1328872613837363658
(125)8156596236415456
Per centof islettissuein the
pancreas0.330.890.880.600.830.350.230.510.520.510.460.490.33
(1.71)0.920.800.850.460.600.440.470.48
Numberof B cellsper cm2 ofpancreatic
tissue172286— t— i
115563
0— t '199 i
1,919378— %
296(554)509175— %
524807267598242
*N.D.H.: New England Deaconess Hospital, Boston.Ch.H.Ph.: Children's Hospital, Philadelphia.S.P.: Hopital Universitaire St. Pierre, Brussels.Ch.H.B.: Children's Hospital, Boston.C.H.: Carney Hospital, Boston.M.G.H.: Massachusetts General Hospital, Boston.N.H.: Newton-Wellesley Hospital, Mass.B.H.: Hopital Universitaire Brugmann, Brussels.
tSevere chronic pancreatitis.^Evaluation of the number of B cells proved impossible in these cases.
Ph.G.H.: Philadelphia General Hospital, Philadelphia.U.P.H.: University of Pennsylvania Hospital, Philadel-
phia.B.G.: Bowman Gray School of Medicine, Winston-
Salem, N.C.E.C.H.: Elliot Community Hospital, Keene, N.H.St.M.H.: St. Mary's Hospital, Montreal, Canada.
6 2 0 DIABETES, VOL. 14, NO. IO

WILLY GEPTS, M.D.
TABLE 2
Cases of chronic juvenile diabetes
Case232425262728293031323334353637383940
Origin*M.G.H. 10765M.G.H. 10922N.D.H. 179.232N.D.H. 190.581N.D.H. 184.720N.D.H. 132.966B.H.59/292N.D.H. 197.521N.D.H. 206.426N.D.H. 183.253N.D.H. 174.414N.D.H. 203.499S.P. 57/424F.H. 50/86B.H.62/228N.D.H. 207.546S.P. 57/135N.D.H. 152.680
Age131523242425303131313132333437394347
SexFFFMFFFMMMMMFFMFMF
Knownduration of
diabetes(yrs.)
72
181420192614172323126
2217372318
Weightof
pancreas(gm.)
55
3533
1203560244090
100706816608580
Numberof islets
per cm2 ofpancreatic
tissue302528195632291968454511261034
45755
Per centof islettissuein the
pancreas0.190.250.160.200.410.230.260.141.240.880.360.100.170.060.360.040.65 -0.41
Numberof B cellsper cm2 ofpancreatic
tissue0
— t— t— t
- j -00
7174.
2850
107000
^ 01,825
*See table 1.fAn evaluation of the number of B cells proved impossible in these cases.
TABLE 3Nondiabetic controls
Numberof isletsper cm2
of pancreatictissue
587246264172295205
6 mos. 1586 mos. 105
2771521546491507855
1221831?41334869935359
202121
Per centof islettissue inpancreas
3.092.191.261.06 -1.461.221.570.642.000.950.673.461.481.020.690.551.730.992.040.520.510.720.660.612.692.04
Numberof B cellsper cm2
of pancreatictissue8,5767,4845,448
4-
4,2885,1546,6923,7365,5444,7184,576
13,060— t2,3781,248
9873,1041,9402,8441,400
9502,1141,0381,0582,9002,688
Case Origin*
123456789
1011121314151617181920212223242526
S.P. 60/479S.P. 58/131S.P. 60/81
• B.H. 60/25S.P. 59/30S.P. 59/437S.P. 58/269B.H. 59/154B.H. 62/93S.P. 60/82S.P. 59/130S.P. 60/182S.P. 53/52B.H. 62/196B.H. 61/249B.H. 61/261B.H. 61/444B.H. 61/509B.H. 61/505B.H. 61/189B.H. 61/489B.H. 60/346B.H. 61/18B.H. 61/83B.H. 61/129B.H. 62/295
Age9 mos.
10 mos.1 yr.2 yrs.2 yrs.3 yrs.4 yrs.,4 yrs.5 yrs.9 yrs.
10 yrs.11 yrs.13 yrs.13 yrs.16 yrs.19 yrs.20 yrs.24 yrs.25 yrs.25 yrs.29 yrs.33 yrs.36 yrs.38 yrs.38 yrs.41 yrs.
* See table 1.f An evaluation of the number of B cells proved impossible in these cases.
OCTOBER, 1965 621

PATHOLOGIC ANATOMY OF THE PANCREAS IN JUVENILE DIABETES MELLITUS
the section were drawn at magnification of 9 X, withdeduction of the larger lacunae and the principal fibrouscords. The area of each islet and that of the section weremeasured with the aid of a planimeter.
The total area of insular tissue visible in the sectionswas calculated by adding up the area of the individualislets. The percentage of insular tissue in the pancreaticparenchyma was calculated with the aid of the formula:s X 100 (s: total area of the islets, S: area of the sec-
Stion). From the number of islets present in the sections,the number per one square centimeter of pancreatic tis-sue was calculated.
Because, in juvenile diabetics, a considerable propor-tion of islets are composed of small cells which cannotbe distinguished as A cells or undifferentiated cells, dif-ferential cell counts could not be carried out. The Bcells, on the other hand, are clearly recognizable in mostof the acute cases and in a small number of chroniccases. We therefore limited ourselves to counting thenumber of B cells in the sections, and we have calculatedthe number of B cells present in one square centimeterof pancreatic tissue. From this part of the study twenty-five cases (46 per cent) were rejected because the cyto-logical preservation or the staining of the B cells provedunsatisfactory.
In view of the variability of the sample material, thecrudeness of the quantitative methods employed, andthe asymmetric distribution of the values, a statisticalanalysis appeared unwarranted and has therefore notbeen undertaken. In the cases which appeared unsuitablefor quantitative estimation of the islet tissue or assess-ment of the number of B cells, only the qualitativechanges w£f"e recorded.
RESULTS
A. Quantitative observations1. Weight of the pancreas. The weight of the pan-
creas was known in fifteen of the twenty-two acutecases (table 1, figure 1). The weight never deviated sig-nificantly from the normal figures, as listed in the studiesof Rossle,4 of Nakamura5 and of Vartiainen.6 In chroniccases, however, the weight of the pancreas was highlyvariable (table 2) , and in a considerable proportion ofsuch cases it was lower than normal (figure 1). Thisweight did not correlate with the age at onset of thediabetes (figure 2) , the duration of the disease (figure3) or the severity of the pancreatic fibrosis.
2. Number of islets. In both the acute and chroniccases, the number of islets per square centimeter of pan-
E"C7t
Pan
crea
s
"o
jht
Wei
c
120
110.
«Q
9a
80.
70.
6a
sa
<0L
30.
20.
ia
c
/
>
#
ifo Vs
• Acute juvenile diabeticse Chronic juvenile diabetics•Non diabetic patients
o
O 0
O O 0 O0 O
o
• o
^ ^ °o
f^ • O O 0
/>-• 0
o °oo
O 0 O Oo
o
o
o
& is io & to A ioNormal weight of the pancreas accordingto the data of Nakamura
Rossle — — — —
Age (years}
FIG. I. Weight of the pancreas in acute and chronic juvenilediabetics, and in nondiabetics.
>-—»
en1/1COCDl_O
cCOQ .
O+-*JCen0)
120f
11010090.80706050403020
10
0 2 A 6 8 10 12 14 16 18 20 22 2U 26 28 30
Age at onset of diabetes (years)
FIG. 2. Relationship of weight of pancreas to age at onset ofdiabetes (in chronic juvenile diabetics).
creatic tissue was, as a rule, smaller than that of thecontrol cases of corresponding age (tables 1-3, figure4) . This numerical decrease was proportionally morepronounced in very young children belonging to theacute group, and in the chronic cases.
3. Size of the islets. As a rule, the islets of mediumand of large size were proportionally more numerous inthose young diabetics who had died after a brief periodof disease than in the nondiabetic controls of cor-responding age. This difference is less striking in the
6 2 2 DIABETES, VOL. 14, NO. IO

WILLY GEPTS, M.D.
m
• pancr
ec
°en
110
100
90
80
70
60
50
40
30
20
10
• Acute juvenile diabeticso Chronic juvenile diabetics• Non diabetic patients
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
Duration of diabetes ( years )
FIG. 3. Relationship of weight of pancreas to duration of dia-betes (in chronic juvenile diabetics).
?ts
pe
r er
r•
isle
°
Num
ber
700.
600.
soo.
40Q
30Q
20Q
10a
•
l " ••
. •
** *• .
• • •• •
* ; •6 8 *
•
• •
" o ° 3
• Acute Juvenile diabeticso Chronic juvenile diabetics• Non diabetic patients
••
'•£, . • o o° ° O ° 9 r> O
20 40 45 50
Age (years)
PIG. 4. Number of islets per square centimeter of pancreatictissue in acute and chronic juvenile diabetics, and innondiabetics.
diabetic children who had died prior to the age ofthree years since in these children the pancreas oftencontains very small islets. In the cases of chronicjuvenile diabetes, the islets were variable in size; insome of these cases large islets were observed (figure
5).4. Proportion of insular tissue. The proportion of
insular tissue is as a rule smaller in the diabetic patientsthan in the controls (tables 1-3, figure 6). The dif-ference is more marked in the chronic than in theacute cases.
• • I
FIG.
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 J6 38 40 42 44 46 48 SOAge at death(years)
5. Median (P50) of islet areas in acute and chronicjuvenile diabetics, and in nondiabetics.
• Acute juvenile diabetics° Chronic juvenile diabetics• Non diabetic patients
t .
0 5 10 15 20 25 30 35 40 45 50
Age at death (years)
FIG. 6. Percentage of islet tissue in the pancreas of acute andchronic juvenile diabetics, and in nondiabetics.
5. Number of B cells per square centimeter of pan-creatic tissue. The cytological preservation and thequality of the preparations were sufficient to allow evalu-ation of the number of B cells in seventeen of thetwenty-two acute cases and in thirteen of the thirty-twochronic cases. In sixteen of the seventeen acute cases,B cells were found. Their numbers, which were alwaysdistinctly lower than in the controls of the correspond-ing ages, were nevertheless considerably higher thanthose in most of the chronic juvenile diabetics (tables1-3, figure 7). In the latter category, not a single Bcell could be found in nine of the thirteen cases evalu-ated. In the remaining four, they were present in smallnumber in two cases, in moderate numbers in one case,and in relatively large numbers in the fourth case.
OCTOBER, 1965 623

PATHOLOGIC ANATOMY OF THE PANCREAS IN JUVENILE DIABETES MELLITUS
log)
a.
i/i
itic
panc
rej
u
fcOlo
*
u
2
1
1 .
•
• •
•
• •
•
a
• • • ••
• • m m
• • 8
o
• Acute juvenile diabeticso Chronic juvenile diabetics• Non diabetic patients
aoo.O..Q.O..OO
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 SO
5 Age at death (years)
FIG. 7. Number of B cells (log. 10) per square centimeter ofpancreatic tissue.
B. Qualitative observationsAppearance of the islets of Langerhans in the pancreas
of young diabetic patients. The islets found in the pan-creas of patients with acute or chronic juvenile diabetescan be classified into three groups, according to thecytological features of the cells of which they are com-posed:
i. Islets of type I. These islets are highly variable insize, mostly small, but sometimes very large. Some havea compact structure (figure 8); others, more numerous,consist of thin cords arranged in a fibrous stroma(figure 9) or separated by capillaries of varying diam-eter (figure 10). The cells forming these islets aresmall in size; the nucleus is small, with dense chromatin;
FIG. 9. Islet of Langerhans of type I in a juvenile diabetic(Case I I , N.D.H. 197.176). The islet is composed ofnarrow cords of small cells in a fibrous stroma.Gomori's chromium hematoxylin-phloxine. X 150.
the cytoplasm is not abundant, and shows no granula-tions; it may stain red with phloxine (A cells ?).These islets often have irregular outlines; continuitybetween the cords of insular cells and acinous tissue isfrequently observed (figure io) .
PIG. 8. Islet of Langerhans of type I, in a juvenile diabetic(Case 18, Ph.G.H. 60/397). The islet has a compactstructure and is composed of small cells, which stainred with phloxine (A cells). Gomori's chromium hema-toxylin-phloxine. X 150.
FIG. 10. Islet of Langerhans of type I, in a juvenile diabetic(Case 5, S.P. 57-130). The islet is composed of thincords of small cells, separated by capillaries. Gomori'schromium hematoxylin-phloxine. X 500.
2. Islets of type II. These islets are also variable insize, but tend to be large. They have a more regularform than those of type I and are as a rule better de-fined (figure n ) . Some of these islets show a centralcavity (figure 12); we feel that such islets have beenformed by a proliferation of cells from duct epithelium,of which flattened remnants are still visible along partof the contour (figure 13). Islets of type II consist to aconsiderable extent of large cells arranged in cordsseparated by capillaries. The nucleus of these cells is
624 DIABETES, VOL. 14, NO. IO

WILLY GEPTS, M.D.
FIG. II Islet of Langerhans of type II, in a juvenile dia-betic (Case 6, Ch.H.B. 60/184). The islet is com-posed of large cells, with a clear cytoplasm. Thenuclei are slightly irregular. Lymphocytic infiltration(arrows). Gomori's chromium hematoxylin-phloxine.X 150.
FIG. 12. Islet of Langerhans of type II, in a juvenile diabetic(Case 6, Ch.H.B. 60/184). Newly formed islet, de-veloped around a dilated duct. Slight lymphocyticinfiltration at the edge of the islet (arrow). Lympho-cytes and histiocytes in the lumen of the duct. Go-mori's chromium hematoxylin-phloxine. X 150.
FIG. 13. Stronger magnification (X 450). of the same islet asin figure 12, showing the flattened epithelium (arrow)lining the dilated duct in the center of the islet. Alsonote the hypertrophy and the irregularity of thenucleus of some of the newly formed islet cells
FIG. 14. Islet of Langerhans of type II, in a juvenile diabetic(Case 22, B H. 58/1121 "Komrhen11 (arrows) in thecytoplasm of hypertrophic B cells. Dominici's toluidineblue-erythrosine-orange. X 450.
large, usually round. The cytoplasm is abundant, oftencompletely free of granules or hydropic (figure 18);sometimes a few scattered granulations of B type canbe found. Many of these cells contain irregular cor-puscles (figure 14) with vague outlines, which staingray with hematoxylin, blue with toluidine blue, andred with pyronin. These corpuscles have previouslybeen described in the cytoplasm of insular cells byWeichselbaum7 who called them "Kornchen." It shouldbe stressed, however, that they are not secretion granules.Their affinity for toluidine blue or pyronin disappears,or is greatly lessened if the sections are subjected inadvance to digestion with ribonuclease;8 accordingly,
they probably contain a significant quantity of ribo-nucleic acids. We regard these cells as hypertrophic andstrongly hyperactive B cells. The islets of type II alsocontain a variable proportion of typical A cells, whichstain well with phloxine; often they have a hypertrophicappearance, but they contain no "Kornchen."
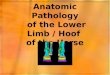
3. Islets of type 111. These as a rule resemble normalLangerhans islets, particularly if only routine stainingmethods are employed. They consist, in variable propor-tions, of typical A ceils and of B cells that are slightlyhypertrophic and more or less degranulated (figure 15)."Kornchen" were on no occasion observed in islets ofthis type.
OCTOBER, 1965 625
PATHOLOGIC ANATOMY OF THE PANCREAS IN JUVENILE DIABETES MELLITUS
FIG. 15. Islet of Langerhans of type III, in a juvenile diabetic(Case 35, S.P. 57/424). The islet is composed of darkstaining A cells, and partly degranulated B cells.Gomori's chromium hematoxylin-phloxine. X 450.
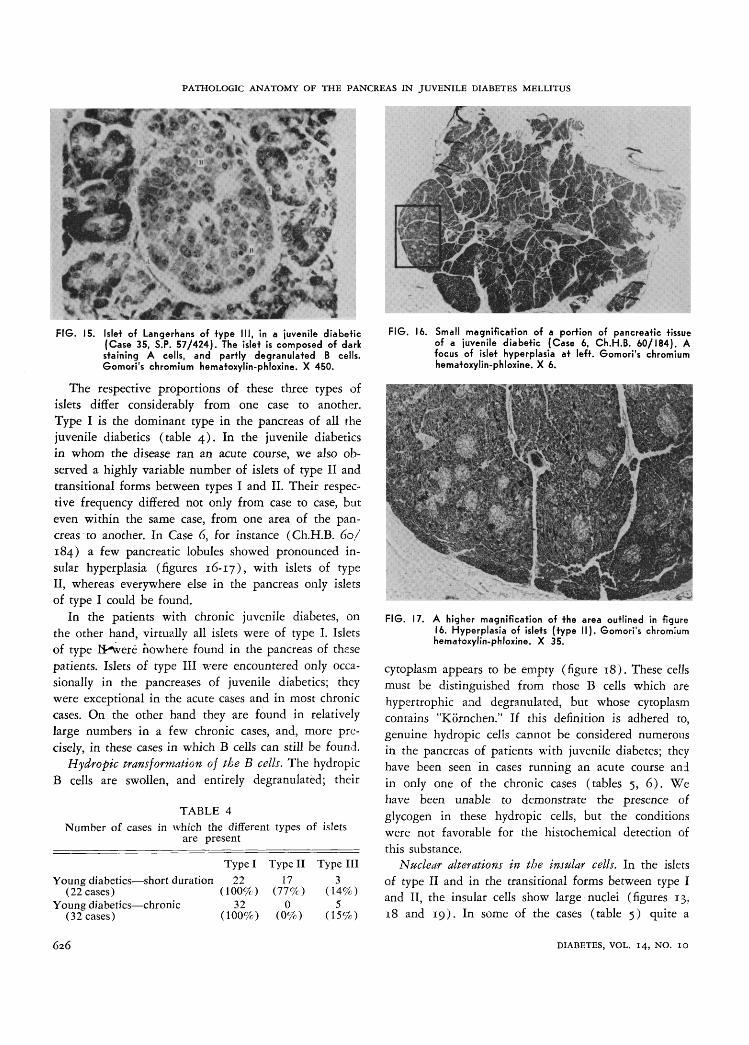
The respective proportions of these three types ofislets differ considerably from one case to another.Type I is the dominant type in the pancreas of all thejuvenile diabetics (table 4) . In the juvenile diabeticsin whom the disease ran an acute course, we also ob-served a highly variable number of islets of type II andtransitional forms between types I and II. Their respec-tive frequency differed not only from case to case, buteven within the same case, from one area of the pan-creas to another. In Case 6, for instance (Ch.H.B. 60/184) a few pancreatic lobules showed pronounced in-sular hyperplasia (figures 16-17), with islets of typeII, whereas everywhere else in the pancreas only isletsof type I could be found.
In the patients with chronic juvenile diabetes, onthe other hand, virtually all islets were of type I. Isletsof type H^were nowhere found in the pancreas of thesepatients. Islets of type III were encountered only occa-sionally in the pancreases of juvenile diabetics; theywere exceptional in the acute cases and in most chroniccases. On the other hand they are found in relativelylarge numbers in a few chronic cases, and, more pre-cisely, in these cases in which B cells can still be found.
Hydropic transformation of the B cells. The hydropicB cells are swollen, and entirely degranulated; their
TABLE 4Number of cases in which the different types of islets
are present
Young diabetics—short duration(22 cases)
Young diabetics—chronic(32 cases)
Type I22
(100%)32
(100%)
Type II17
(77%)0
(0%)
Type III3
(14%)5
(15%)
FIG. 16. Small magnification of a portion of pancreatic tissueof a juvenile diabetic (Case 6, Ch.H.B. 60/184). Afocus of islet hyperplasia at left. Gomori's chromiumhematoxylin-phloxine. X 6.
FIG. 17. A higher magnification of the area outlined in figure16. Hyperplasia of islets (type II). Gomori's chromiumhematoxylin-phloxine. X 35.
cytoplasm appears to be empty (figure 18). These cellsmust be distinguished from those B cells which arehypertrophic and degranulated, but whose cytoplasmcontains "Kornchen." If this definition is adhered to,genuine hydropic cells cannot be considered numerousin the pancreas of patients with juvenile diabetes; theyhave been seen in cases running an acute course andin only one of the chronic cases (tables 5, 6). Wehave been unable to demonstrate the presence ofglycogen in these hydropic cells, but the conditionswere not favorable for the histochemical detection ofthis substance.
Nuclear alterations in the insular cells. In the isletsof type II and in the transitional forms between type Iand II, the insular cells show large nuclei (figures 13.18 and 19). In some of the cases (table 5) quite a
626 DIABETES, VOL. 14, NO. IO

WILLY GEPTS, M.D.
TABLE 5Qualitative changes in the pancreas of acute juvenile diabetics
Case
123456
78
910
111213141516171819202122
Origin*
B.G.55/145E.C.H. 53/9N.D.H. 43475Ch.H.Ph. 1928S.P.57/130Ch.H.B. 60/184
C.H.61/43Ch.H.Ph. 56/85
M.B.H. 9677M.G.H. 10938
N.D.H. 197176M.G.H. 9381M.G.H. 14089M.G.H. 11301M.G.H. 8275St.M.H. 56/103U.P.H. 59/200Ph.G.H. 60/397U.P.H. 55/99S.P.56/237N.H.48/91B.H.58/112
Age(yrs.)
11 mos.11 mos.11 mos.13 mos.2 yrs.2 yrs.,
10 mos.3 yrs.3 yrs.,
6 mos.6 yrs.9 yrs.,
6 mos.13 yrs.15 yrs.15 yrs.15 yrs.15 yrs.15 yrs.15 yrs.16 yrs.17 yrs.21 yrs.22 yrs.30 yrs.
SexFMMMF
MF
MM
MFFFFFMFMMFMM
Knownduration
ofdiabetes(days)
33
1490
9
6030
4515
4146090213016
180411
1490
HydropicB cells
00000
00
00
_|_00
4-4-04-0
4-4-4-4-_j_
4-
NuclearAnomalies
00000
.] |_0
00
0004-
4-4-4-0
_l_4-4-4-
4-604-
ISLET
Mitoses0
_|-000
00
00
0000000000000
TISSUEInflam-matory
infil-tration
_|__| |_
4-+4-0
4-4-
4-4-4-_i_
4-
4-4-4-4-4-4-
004-
4-4-4-4-0
+000
Hyali-nosis
00000
00
00
0000000
4-4-f00000
Fibrosis
4-04-00
00
4-0
0+4-4-0
4-4-4-
+4-4-
4-4-4-4-
EXOCRINE TISSUE
Pancrea-titis
4-004-4-
00
4-4-
4-000
4-4-4-0
. - 0 - ^04-0000
Sclerosisparen-chyma
0004-0
00
04-
0
+00
4-4-4-0
V 0
000000
Sclerosisvessels
00000
00
00
0000000000000
*See table 1.fThe appearance of the hyaline substance is not typical.
.t:T^>T¥V»
FIG. 18. Islet of Langerhans of type II, in a juvenile diabetic(Case 18, Ph.G.H. 60/397). Nuclear hypertrophy, ir-regularity and hyperchromatism. Gomori's chromiumhematoxylin-phloxine. X 450.
few nuclei appear irregular and/or hyperchromatic(figures 18 and 19). Other nuclei have vague contoursand show only slight affinity for hematoxylin (figure19). Pyknotic nuclei and nuclear debris were also ob-served in some of these islets. These nuclear anomalieshave only been observed in acute cases. In chroniccases, the nucleus of the insular cells is small, as arule round, and the chromatin is dense.
FIG. 19. Islet of Langerhans of type II in a juvenile diabetic(Case 17, U.P.H. 59/200). The B cells are swollen,hydropic; their nucleus is large. Note hypertrophic andirregular nucleus. Hemalum erythrosin saffron. X 450.
Mitoses in the insular cells. Although a systematicsearch was made for mitoses in the insular cells, theywere found only in two cells in one of the acute cases(table 5).
Neoformation of islets. In many of the acute casesevidence of new islets formation has been found. Thisneoformation occurs either by proliferation of cells from
OCTOBER, 1965 627
PATHOLOGIC ANATOMY OF THE PANCREAS IN JUVENILE DIABETES MELLITUS
TABLE 6
Qualitative changes in the pancreas of chronic juvenile diabetics
Case24414235234334263044373125454028462747483649395032-33512952385354
Origin*M.G.H. 10922M.G.H. 11212U.P.H. 58/80S.P.57/424M.G.H. 10765B.H. 57/72N.D.H. 203499N.D.H. 190581N.D.H. 199521N.D.H. 198025B.H.62/228N.D.H. 206426N.D.H. 179232N.D.H. 192150N.D.H. 152680N.D.H. 132966N.D.H. 198586N.D.H. 184720N.D.H. 176898N.D.H. 197730F.H.50/86N.D.H. 206428S.P. 57/135N.D.H. 189109N.D.H. 183253N.D.H. 174414N.D.H. 188512B.H.59/292N.D.H. 191917N.D.H. 207546N.D.H. 181450N.D.H. 177827
Age(yrs.)
1517313313163224313237312335472535243632343043333131413034394038
Sex
FFFFFMMMMMMMFMFFFFFFFMMFMMMFMFFM
Knownduration
ofdiabetes(years)
2134677
1214141717171818181920202020222323232323252626373025
HydropicB cells
0004-000000000000000000000
+000000
Nuclearanomalies
00000000000000000000000000000000
ISLET
Mitoses
00000000000000000000000000000000
TISSUEInflam-matory
infil-tration
00000000000000000000000000000000
Hyali-nosis
00000000000000000000000000000000
Fibrosis
+0
+++
00
+++0
++++
++4-4-++++00
_J_
6+++++++
4-4-
EXOCRINE PANCREAS
Pancrea-titis
+40
44-0
44-4-4-
00
++
4-4-400-4-0000000000000.0000
Sclerosisparenchyma
04-4-
04-4-
40
4-4-4-++ ++4-
++
4 44-4-4+
+4-4+++++4
44-44-4-44 4++
4-4-++
4-4-4
SclerosisVessels
000400
4-404
4 4+ 4 44 4 +++++++++
+++++++0
+++++++
++++++++
+++++++++++++++
*See table 1.
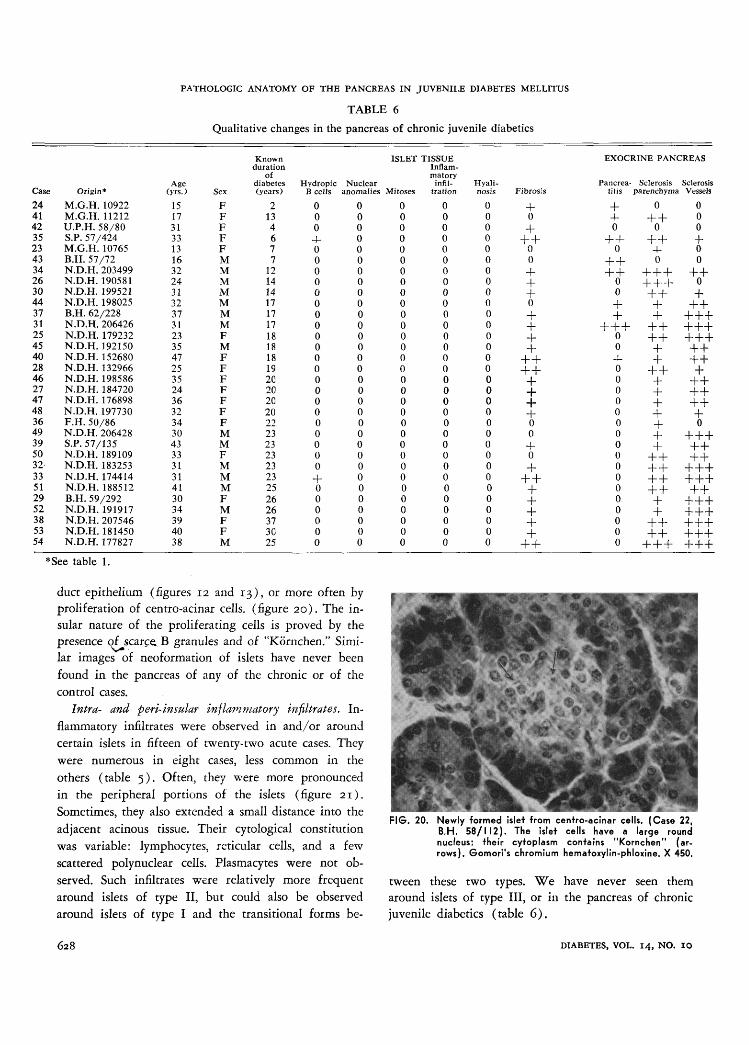
duct epithelium (figures 12 and 13), or more often byproliferation of centro-acinar cells, (figure 20). The in-sular nature of the proliferating cells is proved by thepresence of scarce^ B granules and of "Kornchen." Simi-lar images of neoformation of islets have never beenfound in the pancreas of any of the chronic or of thecontrol cases.
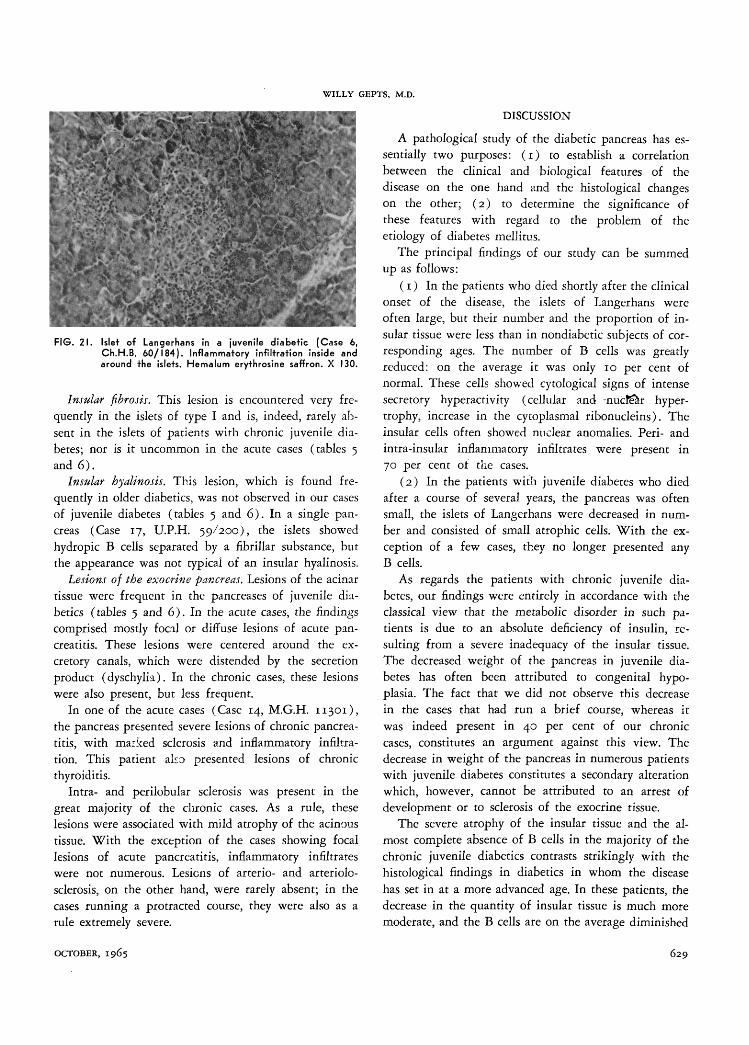
Infra- and peri-insular inflammatory infiltrates. In-flammatory infiltrates were observed in and/or aroundcertain islets in fifteen of twenty-two acute cases. Theywere numerous in eight cases, less common in theothers (table 5). Often, they were more pronouncedin the peripheral portions of the islets (figure 21).Sometimes, they also extended a small distance into theadjacent acinous tissue. Their cytological constitutionwas variable: lymphocytes, reticular cells, and a fewscattered polynuclear cells. Plasmacytes were not ob-served. Such infiltrates were relatively more frequentaround islets of type II, but could also be observedaround islets of type I and the transitional forms be-
FIG. 20. Newly -formed islet from centro-acinar cells. (Case 22,B.H. 58/112). The islet cells have a large roundnucleus; their cytoplasm contains "Kornchen" (ar-rows). Gomori's chromium hematoxylin-phloxine. X 450.
tween these two types. We have never seen themaround islets of type III, or in the pancreas of chronicjuvenile diabetics (table 6).
628 DIABETES, VOL. 14, NO. 10
WILLY GEPTS, M.D.
DISCUSSION
! '! # . X ^ *'<•
FIG. 21. Islet of Langerhans in a juvenile diabetic (Case 6,Ch.H.B. 60/184). Inflammatory infiltration inside andaround the islets. Hemalum erythrosine saffron. X 130.
Insular fibrosis. This lesion is encountered very fre-quently in the islets of type I and is, indeed, rarely ab-sent in the islets of patients with chronic juvenile dia-betes; nor is it uncommon in the acute cases (tables 5and 6).
Insular hyalinosis. This lesion, which is found fre-quently in older diabetics, was not observed in our casesof juvenile diabetes (tables 5 and 6). In a single pan-creas (Case 17, U.P.H. 59/200), the islets showedhydropic B cells separated by a fibrillar substance, butthe appearance was not typical of an insular hyalinosis.
Lesions of the exocrine pancreas. Lesions of the acinartissue were frequent in the pancreases of juvenile dia-betics (tables 5 and 6) . In the acute cases, the findingscomprised mostly focal or diffuse lesions of acute pan-creatitis. These lesions were centered around the ex-cretory canals, which were distended by the secretionproduct (dyschylia). In the chronic cases, these lesionswere also present, but less frequent.
In one of the acute cases (Case 14, M.G.H. 11301),the pancreas presented severe lesions of chronic pancrea-titis, with marked sclerosis and inflammatory infiltra-tion. This patient also presented lesions of chronicthyroiditis.
Intra- and perilobular sclerosis was present in thegreat majority of the chronic cases. As a rule, theselesions were associated with mild atrophy of the acinoustissue. With the exception of the cases showing focallesions of acute pancreatitis, inflammatory infiltrateswere not numerous. Lesions of arterio- and arteriolo-sclerosis, on the other hand, were rarely absent; in thecases running a protracted course, they were also as arule extremely severe.
A pathological study of the diabetic pancreas has es-sentially two purposes: (1) to establish a correlationbetween the clinical and biological features of thedisease on the one hand and the histological changeson the other; (2) to determine the significance ofthese features with regard to the problem of theetiology of diabetes mellitus.
The principal findings of our study can be summedup as follows:
(1) In the patients who died shortly after the clinicalonset of the disease, the islets of Langerhans wereoften large, but their number and the proportion of in-sular tissue were less than in nondiabetic subjects of cor-responding ages. The number of B cells was greatlyreduced: on the average it was only 10 per cent ofnormal. These cells showed cytological signs of intensesecretory hyperactivity (cellular and nucfe&r hyper-trophy, increase in the cytoplasmal ribonucleins). Theinsular cells often showed nuclear anomalies. Peri- andintra-insular inflammatory infiltrates were present in70 per cent of the cases.
(2) In the patients with juvenile diabetes who diedafter a course of several years, the pancreas was oftensmall, the islets of Langerhans were decreased in num-ber and consisted of small atrophic cells. With the ex-ception of a few cases, they no longer presented anyB cells.
As regards the patients with chronic juvenile dia-betes, our findings were entirely in accordance with theclassical view that the metabolic disorder in such pa-tients is due to an absolute deficiency of insulin, re-sulting from a severe inadequacy of the insular tissue.The decreased weight of the pancreas in juvenile dia-betes has often been attributed to congenital hypo-plasia. The fact that we did not observe this decreasein the cases that had run a brief course, whereas itwas indeed present in 40 per cent of our chroniccases, constitutes an argument against this view. Thedecrease in weight of the pancreas in numerous patientswith juvenile diabetes constitutes a secondary alterationwhich, however, cannot be attributed to an arrest ofdevelopment or to sclerosis of the exocrine tissue.
The severe atrophy of the insular tissue and the al-most complete absence of B cells in the majority of thechronic juvenile diabetics contrasts strikingly with thehistological findings in diabetics in whom the diseasehas set in at a more advanced age. In these patients, thedecrease in the quantity of insular tissue is much moremoderate, and the B cells are on the average diminished
OCTOBER, 1965 6 2 9
PATHOLOGIC ANATOMY OF THE PANCREAS IN JUVENILE DIABETES MELLITUS
only to 40 or 50 per cent of normal.9'10 It seems likelythat the few cases of chronic juvenile diabetes in whichpersisting B cells were found constitute transitionalforms between juvenile and adult diabetes.
In the patients with juvenile diabetes in whom thedisease ran a brief, fatal course, the B cells were stillpresent, but were markedly decreased in number. Thisfinding deserves particular emphasis. From biologicalstudies revealing normai or even supranormal insulin-like activity in the blood,1"2 and from the histologicalstudies of Maclean and Ogilvie,3 various authors haveconcluded that the insular tissue must still be normalat this stage of the disease. Our investigation does notconfirm this conclusion. If the cases we have studied arerepresentative for acute juvenile diabetics as a group,they seem to indicate that the supranormal insulin-likeactivity or insulin content of the serum of these diabeticsis produced by B cells which are strongly reduced innumber but markedly hyperactive. The almost completedegranulation, the hypertrophy of the cells and of theirnucleus, constitute classical signs of such hyperactivity.The increase in the cytoplasmic ribonucleins is clearevidence of an enhanced synthesis of protein, probably ofinsulin. We therefore believe that in these patientswith juvenile diabetes, the B cells attempt, by intensehyperactivity, to maintain a satisfactory metabolic equi-librium. Up to the time of clinical onset of the disease,they have succeeded in this attempt for a longer orshorter period. However, this equilibrium grows moreand more precarious. As soon as physiological or patho-logical circumstances lead to an increase in insulin re-quirements (growth, pregnancy, severe infection, etc.),decompensation appears in the form of an acidoticcoma, thisbeing 4:he incident that reveals the existenceof the disease in the majority of young diabetic patients.
Our study shows that exact comprehension of therole of the islets of Langerhans in the physiopathologyof juvenile diabetes can only be achieved by a combina-tion of cytological observations of the islet cells andquantitative estimates of the insular tissue. Neither theamount of islet tissue, nor the size of the islets furnishesan adequate evaluation of their functional value, be-cause a large proportion of the islet cells appear atrophic.On the other hand the demonstration of B cells withcytological signs of hyperactivity in short durationjuvenile diabetics and their absence in the majority ofchronic cases allows a better correlation with the clinicaland biological features of the disease than quantitativestudies only. It could be objected that at least part ofthe islet cells which we have labeled as undifferentiated,
are in fact B cells. We do not believe this to be thecase. However, if these cells should be B cells, it isevident that they are quite abnormal, not only in respectto their morphological appearance but also by theirabsence of stimulation under conditions which havestimulated the other B cells. Our contention that theislet tissue is strikingly abnormal at the clinical onset ofthe disease already, does therefore not appear invali-dated by this objection.
Although we have stressed the importance of theinsular alterations early in the course of juvenile dia-betes, we would definitely not wish to assert that thesealterations are the primary cause of the disease. Thefurther question arises whether the severe quantitativedeficiency of the B cells observed in the juvenile dia-betic patient is congenital or results from slow deteriora-tion of the insular tissue under the influence of anextrinsic factor. From our morphological findings, nodefinite answer to this question can be obtained. On bio-logical grounds it seems improbable that the intensehyperactivity of the B cells serves solely to compensatefor their numerical inferiority; the often supra-normalinsulin-like activity of the blood in cases of acutejuvenile diabetes and of prediabetes1-2 would be difficultto explain if this hypothesis were valid. On the otherhand, the histological features of the insular tissue inthese patients constitute a strong argument in favorof the existence of an extrinsic stimulatory factor. Mac-lean and Ogilvie3 have already described the presence,in patients with acute juvenile diabetes, of largeislets and our study confirms this finding. We have alsoobserved evidence of new islet formation at the ex-pense of centro-acinar and tubular cells; this leads tothe formation of islets consisting largely of hyperactiveB cells (islets of type II). For reasons that are not yetunderstood, the B cells disappear progressively fromthese islets, leaving only the A cells, which undergoatrophy, and a collapsed stroma which undergoes fibro-sis. In this way, the islets of type I are formed, whichconstitute the greater part of the insular population injuvenile diabetics. It seems probable that in the pancreasof acute juvenile diabetics we had the opportunity tocatch the final stages of a process which has been goingfor an indefinite time, perhaps from birth on.
In recent years, a number of factors have beendescribed which might represent agents stimulatinginsular function; among these are physiological an-tagonists of insulin (growth hormone, adreno-corticalhormones), pathological antagonists ("synalbumin an-tagonist" of Vallance-Owen,11 antibodies), disorders of
630 DIABETES, VOL. 14, NO. IO

WILLY GEPTS, M.D.
the mechanism of transport of insulin,12"14 anomalies offatty acid metabolism.15 A discussion of these numerousfactors would be outside the scope of the present paper,which is concerned only with morphological problems.We are of the opinion that none of these factors iscapable of provoking permanent diabetes without severealterations in the insular tissue being present.
The mechanism by which the B cells progressivelydisappear from the islets of type I has not yet beenelucidated. We are confronted with an identical prob-lem in the idio- and metahypophyseal diabetes of thedog. In the latter case, the destruction of the B cells hasbeen attributed to a hyperactivity which leads to hy-dropic degeneration and to death of the cells. Thestudies of Lazarus and Volk16>17 have revealed, however,that the glycogen overload which characterizes thehydropic transformation of the B cells, is not associatedwith any alteration in the cellular organelles and that ittherefore cannot be regarded as a degenerative lesion.In dogs treated with growth hormone, on the otherhand, the same authors observed a different type of cel-lular change: the "ballooning degeneration," which isassociated with nuclear pyknosis and with other ultra-microscopic signs of cellular dysfunction. We haveregularly found lesions of "ballooning degeneration" inthe B cells of spontaneously diabetic dogs.18 On theother hand we have been unable to find any correspond-ing changes in human diabetic patients. In a number ofhuman cases, we have observed irregularity and hyper-chromatism of the nuclei of the B cells. The exact sig-nificance of these nuclear changes is difficult to assess.We do not believe that they result from autolysis, be-cause they have not been found outside the islets or inthe islets of the control cases. They may represent aprocess of degeneration. The intense secretory stimula-tion indicated by the abundance of the cytoplasmicribonucleins may in the long run lead to a disorder ofthe regulation of nucleic acid metabolism and to pro-gressive extinction of the strain of B cells.
In connection with the etiology of diabetes, one find-ing deserves particular attention: the frequency of peri-and intra-insular inflammatory infiltrations in juvenilediabetics who had died soon after the clinical onset ofthe disease. Such infiltrates were observed as early asthe beginning of the century by a number of pathol-ogists (see Kraus).19 Warren and Root20 and Stansfieldand Warren21 again called attention to this lesion. Sofar, all authors are in agreement that this finding isspecific for diabetes and that it is only found in youngdiabetic patients in whom the disease has run a rapid
course. LeCompte22 has recently made a study of thislesion and advances the hypothesis that it may not be souncommon as has hitherto appeared. Our findings sup-port this view: we have been able to find such in-filtrates in fifteen of the twenty-two acute cases, i.e., in68 per cent. This high frequency is the more remarkablesince we had only routine material at our disposal, sothat fully detailed examination was possible only in aproportion of the cases.
What significance is to be attached to the inflam-matory infiltrates? In LeCompte's study22 a number ofpossibilities are reviewed: an inflammatory lesion ofviral or microbial origin, an alteration secondary tolesions in the insular cells due to hyperactivity, aninflammatory reaction following the destruction of in-sular cells by an unknown toxic agent, and an immuno-logical reaction.
None of these hypotheses appears to be entirely satis-factory. The possibility of an infectious etiology is sug-gested by the fact that in certain juvenile cases, in-fectious phenomena coincide with the onset of thediabetes.23 The development of diabetes followingmumps has been described.24 Gundersen25 has observedan increased incidence of diabetes during the yearsimmediately following epidemics of mumps in Nor-way. Barboni and Manocchio26 have reported the onsetof diabetes in cows shortly after an epidemic of aph-thous fever; in the islets of the diabetic animals theseauthors observed inflammatory infiltrates. However, inthe great majority of cases of human diabetes, no in-fectious etiology appears to be present.
Inflammatory infiltrates of the islets of Langerhansare usually not observed in idio- or metahypophysealdiabetes, after alloxan, or in other forms of experimentaldiabetes. However, Toreson et al.27 have recently re-ported such infiltrations in rabbits made diabetic byimmunization with beef insulin.
The view that the insular lesions might have an im-munological origin has very recently found support ina number of interesting observations. In rats that havebeen rendered diabetic by intravenous administrationof anti-insulin serum from guinea pigs, Lacy et al.28
found inflammatory infiltrates with eosinophil poly-nuclears and lymphocytes around and within the isletsof Langerhans. Toreson et al.27 recently reported infiltra-tions of the islets and interlobular stroma with mono-nuclear cells in rabbits that have developed a diabeticstate, following immunization against beef insulin. Afterprotracted administration of homologous insulin to cows,Renold et al.29 observed very pronounced and extensive
OCTOBER, 1965 631

PATHOLOGIC ANATOMY OF THE PANCREAS IN JUVENILE DIABETES MELLITUS
lymphocytic infiltrates in the islets. With the aid offluorescence technics, Mancini et al.30 were able todemonstrate antibodies against human insular tissue inthe serum of a young diabetic who had never receivedinsulin. In this connection, it may be worthwhile torecall that one (Case 14, M.G.H. 11301) of the youngdiabetic patients whom we have studied concurrentlypresented lesions of thyroiditis. These observationspointing to a possible immunologic derangement are ofthe greatest interest in view of the high frequency withwhich we have found inflammatory infiltrates in ourrecent onset juvenile diabetics. Further investigation ishowever required before it will be possible to evaluatetheir significance in regard to the etiology and thepathogenesis of human diabetes.
ACKNOWLEDGMENTThis study was supported by grants from the Belgian-
American Educational Foundation and the "Fonds de laRecherche Medicate" of Belgium (Grant 459).
The author gratefully acknowledges his indebtednessto those who aided him in this investigation by placingpancreatic material at his disposal: Dr. B. Castleman(Massachusetts General Hospital, Boston), Dr. H. J.Christian (The Carney Hospital, Boston), Dr. P. Dustin(University of Brussels, Belgium), Dr. Ehrich (Gradu-ate School of Medicine, University of Pennsylvania,Philadelphia), Dr. Enterline (University of Pennsyl-vania Hospital), Dr. D. Kahn (St. Mary's Hospital,Montreal, Canada), Dr. P. M. LeCompte (FaulknerHospital, Boston), Dr. J. D. MacAUister (Elliott Com-munity Hospital, Keene. N.H.), Dr. W. Meissner andDr. M. Legg (New England Deaconess Hospital, Bos-ton), Dr. R. P. Morehead, Bowman Gray School ofMedicine, ^J^inston-Salem), Dr. Vawter (Children'sHospital, Boston), Dr. Yakovac (Children's Hospital,Philadelphia).
I would also like to express my deepest gratitude toDr. P. LeCompte for the hospitality that he and hisdepartment have shown me during my stay and forhis continuous interest in this work. I would also like tothank Dr. F. D. W. Lukens for his guidance during mystay in Philadelphia.
Much appreciation is also expressed for the tech-nical assistance of Mrs. Judith Brandt and Mrs. MagdaCoeck and for the secretarial work of Mrs. Marie-LouiseBaum.
REFERENCES1 Steinke, J., Camerini, R., Marble, A., and Renold, A. E.:
Elevated levels of serum insulin-like activity measured withadipose tissue in early untreated diabetes and prediabetes.Metabolism 10:707-11, 1961.
2 Vallance-Owen, J., and Lilley, M. D.: Insulin antagonism ofthe plasma of obese diabetics and prediabetics. Lancet J:8O6,1961.
3 Maclean, N., and Ogilvie, R. F.: Observations on the pan-creatic tissue of young diabetic subjects. Diabetes 8:83-91,1959-
4 Rossle, R.: Beitrage zur Kenntniss der gesunden und derkranken Bauchspekheldiiise. Beitr. z. pathol. Anat. u. z. allg.Path. Alg. Pathol. 69:163-84, 1921.
5 Nakamura, N.: Untersuchungen iiber das Pankreas beiFo'ten, Neugeborenen, Kindern und im Pubertatsalter. Virch.Arch. 253:286-349, 1924.
6 Vartiainen, I.: Studien iiber den Diabetes Mellitus inFinnland; die Makroskopischen Organveranderungen der Dia-betiker im Lichte des Obduktionsmaterials. Acta Med. Scandi-nav. 7x8:538-74, 1944.
7 Weichselbaum, A.: Uber der Veranderungen des Pankreasbei Diabetes Mellitus. Sitzungsberichte der Kaiserlichen Aka-demie der Wissenschaften 119:73-281, 1910.
8 Lecompte, P. M., and Gepts, W.: Unpublished observa-tions.
9 Maclean, N., and Ogilvie, R. F.: Quantitative estimation ofthe pancreatic islet tissue in diabetic subjects. Diabetes 4:367-76, 1955-
10 Gepts, W.: Contribution a l'etude morphologique desilots de Langerhans au cours du diabete. Ann. Soc. roy. Sc.med. natur. Brux. 70:5-108, 1957.
11 Vallance-Owen, J.: Insulin Antagonists and Inhibitors:Advances in Metabolic Disorders. New York-London, AcademicPress, p. 191-215, 1964.
12 Antoniades, H. V., Bougas, J. A., Camerini-Davalos, R.,and Pyle, H. M.: Insulin regulatory mechanism and diabetesmellitus. Diabetes 13:230-40, 1964.
13 Samaan, N. A., Fraser, R., and Dempster, W. J.: The"typical" and "atypical" forms of serum insulin. Diabetes 12:339-48, 1963.
14 Froesch, E. R.: Insulin im Blut: durch Insulin— •Anti-korper hemmbare und nicht hemmbare Insulin Aktivitat undihre physiologische Bedeutung, in: Fortschritte der Diabetes-forschung. Herausgegeben von K. Oberdisse und K. Jahnke.Stuttgart, Georg Thieme Verlag, 1963.
15Randle, P. J., Garland, P. B., Hales, G. N., and News-holme, C. A.: The glucose fatty acid cycle. Its role in insulinsensitivity and the metabolic disturbances of diabetes mellitus.Lancet 1:785-89, April 1963.
16 Lazarus, S. S., and Volk, B. W.: The Pancreas in Humanand Experimental Diabetes. New York, Grune & Stratton,p. 107, 1962.
1 7 Volk, B. W. , and Lazarus, S. S.: Ultramicroscopic evolu-
tion of B-cell ballooning degeneration in diabetic dogs. Labor.
Invest. 7 2 : 6 9 7 - 7 1 ^ 1963.1 8Gepts, W. , and Toussaint, D . : Unpublished observations.1 9 Kraus, E. J . : Die Pathologischen-Anatomischen Veran-
derungen des Pankreas beim Diabetes Mellitus. In Henke und
Lubarsch: Handbuch der speziellen Pathologischen Anatomie
und Histologie. Berlin, Julius Springer Verlag, p. 672 and
p. 685 , 1922.2 0 Warren , S., and Root, H . F.: The pathology of diabetes,
with special reference to pancreatic regeneration. Amer. J.
Path. 1:415-30, 1925.
632 DIABETES, VOL. r4, NO. IO

WILLY GEPTS, M.D.
2 1 Stansfield, O. H. , and W a r r e n , S.: Inf lammation involving
the islands of Langerhans in diabetes; report on pathologi-
cal findings. N e w Eng. J. Med. 198 :686 -87 , 1928.2 2 Lecompte, P. M . : "Insul i t is" in early juvenile diabetes.
Arch. Path. 6 6 : 4 5 0 - 5 7 , 1958.2 3 J o h n , H . J . : The diabetic child. Etiologic factors. A n n .
Inf. Med. 8 : 1 9 8 - 2 1 3 , 1934.2 4 Barbieri, V . : Gazz. d'osp. 3 0 : 2 7 3 , 1909. Cited by H . J.
John . 2 3
2 5 G u n d e r s e n , E.: Is diabetes of infectious origin? J. Infect.
Dis. 41:197-202, 1927.2(3 Barboni, E., and Manocchio, I.: Alterazioni pancreatiche
in bovini an diabete mellito post-aftoso. Archivio veterinarioitalianio 73:477-89, 1962.
27 Toreson, W. E., Feldman, R., Lee, J. C, and Grodsky,
G. M.: Pathology of diabetes mellitus produced in rabbits bymeans of immunization with beef insulin. Amer. J. Clin. Path.42:531, 1964 (Abstract).
2 8 Lacy, P. E.. W r i g h t , P. H. , and Silverman, J. L.: Eosino-
phi l ic infiltration in the pancreas of rats injected with anti-
insulin serum. Fed. Proc. 2 2 : 6 0 , 1963 .2 9 Renold , A. E., Soeldner, J. S., and Steinke, J . : I m m u n o -
logic studies with homologous and heterologous pancreatic in-
sulin in the cow. Ciba Foundat ion Colloquia. Vol. 15. Aetiol-
ogy of diabetes mell i tus and its complications. Edited by M. P.
Cameron and M. O 'Connor . London, J. R. A. Churchi l l , p .
122, 1964.30Mancini, A. M., Costanzi, G., and Zampa, G. A.: Human
insulin antibodies detected by immunofluorescence techniques.Lancet 1:72.6, March 28, 1964.
Insulin and Enzyme Induction
In addition to its hypoglycemic effect, another demon-strated action of insulin is an enhancement of proteinsynthesis (I. G. Wool, Am. J. Physiol. 199:719, i960;Biochim. Biophys. Acta. 68:28, 1963, and related to this,an increased synthesis of messenger RNA (Wool andA. J. Munro, Proc. Nat. Acad. Sci. ^0:818, 1963). Itis reasonable to assume that this stimulation of proteinsynthesis is a specific and not a general effect of thehormone. In a negative sense, it is also likely that thehypoglycemic effect of insulin is not causally related toprotein synthesis, since hypoglycemia can occur toorapidly following insulin administration to be accountedfor by some mechanism involving protein synthesis.
Another major metabolic disturbance in diabetes isincreased lipolysis from adipose tissue triglycerides lead-ing to elevated levels of plasma free fatty acids (Nutri-tion Reviews 16:135, 1958). The mechanism of thiseffect is obscure, but elevations in free fatty acids canbe demonstrated in animals acutely deficient in insulin(Ibid. 22:334, I964), suggesting that the effect is notsecondary to an effect on protein synthesis. Furthermore,it appears unlikely that a change in plasma lipase canbe invoked in the mechanism (Ibid. 17:191, 1959).
Another well documented defect of fat metabolismin diabetes may, on the other hand, be linked to theinfluence of insulin on protein synthesis. Synthesis ofmonounsaturated fatty acids from acetate and stearate inadipose tissue of diabetic rats is greatly depressed (Nu-trition Reviews 22:252, 1964). Microsomal desaturationof long chain fatty acids almost ceases, and insulin treat-ment in vivo, but not in vitro, restores the desaturationmechanism to normal. In the above review the specula-tion was advanced that the cause of the metabolic block
might be a defect in the level of enzyme .Sfrivities re-quired for the catalysis of these reactions. New experi-ments in this area, discussed below, support this hypoth-esis (A. Gellhorn and W. Benjamin, Science 146:1166, 1964).
Male rats were made diabetic with alloxan, and be-fore experimentation the animals had persistent glycos-uria and blood sugar levels in excess of 300 mg. per100 ml. One group of rats was untreated, another groupwas treated with glucagon free insulin in three dosesduring the twenty-six hours immediately prior to theexperiment, and a third group received actinomycin D,10 to 25 jxg., per 100 gm. body weight, thirty minutesbefore insulin. Additional animals were either normalrats or normal rats treated with actinomycin D. A mea-sure of blood glucose levels showed that actinomycinhad no effect on the blood sugar levels of normal rats,nor did it interfere with the hypoglycemic effect ofexogenously administered insulin in the diabetic rats.
Epididymal fat from these animals was incubated withacetate-1-C-14 to obtain a measure of total fatty acidsynthesis. A rate limiting step in fatty acid synthesisis catalyzed by acetylcarboxylase, a reaction leadingfrom acetyl coenzyme A and carbon dioxide to malonylcoenzyme A. This reaction is known to be depressedin diabetics (O. Wieland, I. Neufeldt, S. Numa,and F. Lynen, Biochem. Z. 336:455, 1963). Gellhornand Benjamin found that adipose tissue in vitro fromnormal rats had a rate of acetate incorporation of 1.40/xmoles per gm. per hour. The rate in diabetic rats was0.24, and this was brought by in vivo insulin to a near
{Continued on page 662)
OCTOBER, 1965 633