Embed Size (px)
Citation preview

I atttologtc Anatomy o[ the C rrhottc " " u "l, " Ltver tvtth Portal, t rtenston
I) A N I E I ~ II ( )T I I. M. IL
A (?(t?~Sl:bEi~ABl;i~ VO]tH~te Of experiHieliia[ alt(i c] i l l iea , i evi(lel:i¢~2 iud;icates ihat the vei~ous hyperte~lsio~ of cirrhosis is. caused
by obsti'uctio~t of the efferent veins, aml that its t ransfere~ee i~go th~ portal veii~, lead~ ul t imately to the elhfieal expressi(ms of portal hypertensioI~, The additio~ml concept that abnormal arteriovettons shm~ts co~tribnt- to the portal hYl>rtension also asst:lmes prior obstYuetio~ of effareL~t wxir~s. ~ '~
There is disagreement as to the cause of this obstruetiom At p:tese~tt, the rege~erat ing .pare~ehymai l~.odules ra ther than the fibrous septa are gem-rally e~msidered the essential factor. This opbHoll was expressed early b~ the century by Kretz aud Mil~ae, and by oilier a:uthors later.::, ~o...o~a ] lowever, there e , m t i n u e I;o be published eommems at t r ibut ing ihe dis tort ioa add obstruciion of ~he efferent vei~s to th- 5brous sepia, a' ~'~, ~=' Li,,bowit.z revh-ws the literature, thor(m~hly h~ his book. a++
i t was thoue*ht that some elarifieatbm el! tiffs point might result from a comparat ive anatomical study of eases of cirrhosis with a~d without portal hyperb*nsiom ]I: was also hoped that a useful clinical t-el won.hi be gai,md if there eouht l:,~, derived a morpbo- lo>'ie formula for the cirrhotic liver, which would be sufficiei~tly characterist ic to be equab,d with tD" existe~eo, of portal hyper- t(msiom
NATERIALS AND METIIODS
Cases r~,eords of cilwhosis at. ["hi.versify Ho:q~itat we>, e,,llected and separated i,~to two ~Tollps, Olte i l l which there was associated portal hyperte~sion mid o~~e i~ which there was m~t+ There were 23 cas,,s i~i which dh:eet proof of the existe~ee of p~rtaI hyper- ter~sio~ had be(m fur~ished by mmmme~rie reeordb~gs of the portal
From the New York t;~iver~ity----t~elh~vue M,~dieaI Oq3ter a~~d ghe lh~iversi~y Hospital, N~w York, N Y.
The interest, a~,d criticism of Dr, Manriee Riel~ter, Di~'ee~or, Deparf:me~t, of Patbol0~y U~ive:rsi~y Hospital, New York, N~ No, is gratef~atlv ae],;,rmwledgedo
The pho~omie~ograpIe~ were take~ by Sant~ Speneev. B~P,A.
NEW SfiRiES vot.~ < ~0. 9~ ~ 72t

Roth
p r e s s u r - made d n v i u / l apa ro tomy . Since there were pract ical ly no instmiees of lifts proeod.ure b e h ~ ca r r i ed out hi the abs .nee of por ta l }lyperh~nsi,::m. and since tlw total number of Illallol~te{;ri.. eallv p r o w m cases wa~ small, it was n e c e s s a r y to ~xpand the s h l d ) to in¢.lud, c a s . s i ti utfich the. p resence or absv~ico of por ta l }ty[.~>. tensior~ was hMb>e t ly do te rmhled bv th~ prese lwe or absel/ee of [{:-~. s eq u~:la e. t h e s e b e i ~ / esoph a gea ] v a riees a n~ t col:~/esI ]ve s pl {~i~ o.~ me /a /y , sbt,a'ly or i~:~ eoulbinaiion~ Since i:hes~ wer~ e~msid~red p r o o f o:f the ~xisttmce of por ta l hyl>u' tenshm, it ~as a s sumed for l:ht ~ 1)llr;i}os~s of this s t udy tha t wh-u ana tomica l dissectio~Jl i!aibd t,~ reveal them por ta l hyperi;e~isio~i was at~o absent,i. ])mmmstra{h~< their in:'esem.*e or abs.nee required m~ero[>y :mat(~rial, and thi,4 was fm 'u i sh -d by the m,m'opsy tih,s of lh i ive r s i ty [{ospi ta l ' s ih~ partrnmtt of I'at}mtogy~
All eas~s imlexed an c i r rhos is w.re examir~ed. C:.:s.s wvro m! jee|;ed whc~ review of {ht~ {is:~uo s~c.tbms rai~.~d doubt as t~, the val idi ty of the diagm:mis of e i r rhos i< whe~ th- n - c r o p s y p r . t o c o l s "WQF{.' i[tCOtt(JA]SiV!~ it'l t ' o g a / ' t | t o tip,'. 1)t'~*s(lit,:{ o r ~l!}s(<tl(~(? of't~s()llhil- ~'eaI var ices and~of sp[eltoi~tog'aly, w}toll there was a.scites a~d n . i thm ~ of the |;w{~ afor~m~er~tiom~d :stigmata of por ta l hyperte~> aion. and wheu ihm'e was ~iad eq ua~ c confirmation, of the pa t .ne j ' of tho p . r t a l v~hu In cermet.don wh:h the las t point , all cases wt~re r<ieete~l ,,vhe~ t h e r - wer~ mali~'mmt or ~xudaiiv{> :i,it]ammatory processe.~ iuwdvi~g t ee l iver or r~,gion of ihe por ta l vein, because impor t an t bra~eh<~s of this w~ss-I nlix'ht haw. l~een oceh:Id-d by [}]FOItQbON{S o r (!()I[tpl~f~SgiO![l,
Thai: on] 3 elm lrtit~rost~olde secthm of l iver t~xisIed for a ~'iv{ul (-as(, wa~ llot eollsiderod eanse f~)l" re jec t iom prov ided the m~orops y • rtq:}orl imticated un i fo rm and d i f fuse involw-ment of th(' l iver by the chwhotie proe .as , W h o l t l 'ltoF( ~ {ha l l o l t0 seetio,~ were availabh~ IIi a c}ts(? i[ w i t s F{?~l]]alJy ~h}t~ { h e r e w~:/s (t~{~SO lt~F~Hq~b~Ik~, ani.+~g th<m with r e g a r d to those featl~res which {-atn0 undvr s+wu++ tsiuy in this work.
iii {1t~ KFOI![} O{! surKieal eaa~s~ lnos{ < ~,.* ~ ' ,J:~{<tIlt{ /1~ ()I){~liIi(H:l }}5' opeu biopsy of th- ]iw~r provt}d adequa t e fo r s tudy, but when oMy l~.eedle bh:q)sv had be~*n p e r f o r m e d the mate r i a l wa~ rejocb~d as i n s ufiie.i ent.
l"nder these res l r i c tbms , there r ema iued for s t udy 75 n~erop~ied canes of c i r rhos is in which por ta l h y p e r t - n s h m was man i f e s t ed by prove~ . s o p h a / ~ a ] var iees am:t/or e~m~*~tive ..pt .u m~ .~dI , 2;-~ ~ur,,.
AMERICAN JOURNAL OF 722 o~G~snv~ mSEAS~S

Cirrhotic Liver and Por|a! Hypertensi.**
g'ieal cases prove~, by portal veb~ maintain'try to be associated with portal hypertension, 34 necropsied cases with ncithe:v esophageal variees nor congestive sple~mmegaly, a~d ore.: surgical case with i~ormal portal vei~, ma~omotric re~,ordings and m> clinical s t igmata of p~wml hyt:~erte~.~siom Some of the necropsied eases had umier-. gone shuui of)eratio~is dmq~,g life but were I:mt inch~ded among the ~o sur~'ica] cas{?8.
The iypes of cirrhosis and ih,,ir tmmerical distri!:mtiol~, arc given h, Table 1. ]~l this report ~.llt cas~,s of Laemlec 's and el! p~,st,~ec.rodc cirrhosis ave tabulated under the si~igle heading of portal ch.-rhosis.
Si~.lce the regem~rative ~lodub was to be dw central figure o.t" this work, it was considered esseatial to formulate a rigid deih,i... don for it: which, would enable us to maintah , a em~siste~t base ]i~te f m comparison am] to avoid the evvor of treath~g isolated feel of pare~mhymaI cells as proIiferating, expansile structures. The vequiremems as developed t'or this study: were thai. the ,mdute be clearly discret% completely e~lcirch~d by emmecdw, tissue, spheroi- daI i~. shape wit}, its outermost layer of cells molded Io conform to such a~ ot/tli~te, a~d, finally, that the efferent veit~ be mara'inally si tuated or completely excluded from i.he focus of parenchymal cells. I t was felt that these cri teria could olfly be met by a truty regem,rat ive nodule,
A~ atteml:k was made to compare the ratio of proliferati.ng to resti~g cells iI~ the livers associated with portal hyperte~}sio~ and those without portat hypertenshm, i t was thought that this might provide a~other expressi{m of esse~tialfy lhe same phe~mmenon ms does the regenerat ive ~mdule. This was carried out hy counting m~.d classifying the cells which felI at random m~der th.e cross~ hairs of a gr id inset % the mi.c.roscope ocular providi~}g 25 pellets in each field. [;sing ge~eratly accepted cr i ter ia of hepatic paren- eh.ymal ee]I prol iferat ive activity, ~mclear enlargement, multinue- leadom a~d cytopfasm.ie basophilia were sought for a**d the ratio of such co]Is to res t ing cells was determi~md from cell. cmmts made of 100 fields in each sectiom No correlat ion l~etwee~~ this ratio and ihe existe~,ce or absenee of portal hyperte~sion emerged from a piloi group of cases, and this Iir~e of i ,westigation was {herefore discontkmed.
The degree of fibrosis wa~ est imated by examination of the routinely stained (hematoxylin rosin) settling.s, This method has
NEW S~RIES voL ~, NO ,~ ~ 9 723

i~ ~
~I
~ ~
'~ ~ ~ ~
i~
ib~
i~
!~i!~
h~ ~
i ~%
~!i
~ i~
~i~i
~ ~I~
,~ ~
i~ ~
ii~
b~'~
i~i~
!~
" ~i~
i~
~ ~
~
~t~
i~
~,~!
~.~
~...-
I..~.
.- ..
..
.
~.~...~..~ ii
~.i~
.. ~.
..~
'~
~"~
fi~...~
l~..~
,, ~-
.-~~
ti~
..~..~
,,~,
~...~
~ c
~
~ill.
..~.~
..~ ~
.--~.
~ .....
. ti~
..~i~.
.~..~
~ ~
..
~.i/~
...~.
. i~
....~
..~...
~..
..I~
~
....
~
~
~ ~
.q~
y ~
~!~
t~
~ ~i~
i~ ~
~ ~
~ 17
17
{!
~ i
ll '~
i~ t
li ~
~ ~
i~
~
~ ~
~ ~i!
~
~ i~
i~ i~
~
o~
~
z
~0

Cirrhotic Liver and Portal Hypertensiot~
bee~ shown by War ren and Wahl to be fa i r ly reliable, and was con~ s idered adequate for the purpose. ~7
l~'eatures observed f reque~t ly in the c(mrse of this work were a p romine~t t:tilatatiou of small Mood vessels ir~ the pori.at areas; fibrous sel)ta, a im hepatic capsMe. They were cons t rued to be a maMfesfa t ion of i~ereased i~t.rahepatie veuous pressure , a l though it: was nneer tMn whether" they represen ted i~ereased tor tuos i ty of vessels, dilatation, of normal ly (.tosed (:oitalerais, or newly de~ veloped shunts. ;in any event, it seems reaso,mble to it,yoke dis tal obst ruct ion as the mechanism by which such fea[ures wouhi be b rough t about (Figs. 1..3). The pa t t e rn was taken as the two~ (t:imeusi-nal >xp:ressioi~ of i.he d is turbed vascula ture wMch has ot!t(~t been shown~ by perfusi(m, digestion, amt three..dimensional reeox~s*ruei.im~ tech , lcs io b(~ a ~'eaiure of fhe eirt"hotie live~*? '~'
Tahte I g-:iw*s {iris te/a~gi,:~eia~ic fmttern i~ two cob:ram:% (me rep~. re:~mti~v: it a~ ol}served i~l {h~* h~patic pa~e~mhyma~ the, (,thee an observed in the capsule. This (:livi~ion was made b~eause it was
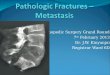
Fig. I ( le/ t) . Rege:lerative ~odnle h~ portal cirrhosis. M{~}dh~g of the peripheral laye~ of pv~re,~ehymal cells, complete discrete~,ess of the m~dole~ a~d absence of an effeeent vein. Cap.~llar a~d parenehyma| telaugiecla~ia. (H & E; reduced ft 'o~ >, 30). Fig. 2 (right). N~d~t|ar cege,tet'atit, n in a case Of postnecrolic. cirrhosis, Portal vei~ pressure 420 ram. water. T~-o adjaeen~ ~mdule.* whose expansile growth i~ limited by contact ~-i~h each other rather than by fibrous septmm (H & E; reduced f r -m >~ 60),
NEW SERIES VOL. 4, NO~ 9, ~9~9 725

Roth
Fig. 3 ( t p# ) . 15:da~lgieclasis il'~ fibr,,~us septt~m ( l l & Er~ r*.~dtieed f ~ m X 6 0 ) . lPlg. 4 (righl) . Tt*langiee~a~is o f e~psuiar eo~(~t'~;ctive f ,[s~e. ( l l & E~ r~'d~]eed fro~t~ ~ 150)~
t b o ~ ' h t that ih~ eap,~,ular ,:~:~d~. mighi r{~pre~en~ di lated cob b~ter~ls ~ff the hepat ic a r t e ry spe~,ifica, lly, a~d t.h,;;r~4ore lmve spe~ eiat sig~ilicanc-; (Fig. 41. To distina~uish with. cer ta in ty small bh,od x, ess~ds from lymphat ics c,r f rom ~paees made by d{ss<dved fat ~:lobules t.~apped h~. fhe s t roma, one mus t find blood cells i~ the
h s absence, 1--~- its pre~euce in mbfima! or equivocal degre(?, 2.~,! ~, and ;i ' - i~s well estahlishod pre~w~c~ h~ moderat~ and marked de~or~,~ r-siw~,tively~
ItESI LTS
NodutariLy was observed i~ more tha~ equivocal or mhdm~d d~.-~ . . . . . , sur~.,qcal case:~ am::l :h~ (:;5 of the 6~ necrol)sh:~d cas~s ~i! por ta l cirrh~sis ass~ciated with porta l h;,'p~rt~,nsion. (Tw~ ~>f th~ three ~ e r o p s i e d cas~s wh.ich w~r- recorded as 1 + actually had bee~ g raded betwe~q~ 1-+, and 2+ but were tabulated in the' lower category, ]n the small aT~mp of e i r rhoses o ther than porta l a c~msisi~,nt dis, t r ibui ion was not appar¢~nt. This may in pa r t be ex~. plaiuod in Lhe case of fa t ty cirrhosis by the fact that large amount:~ of i~tracetlular fat tend to obscure the nodular pa t te rn and feuder it diffic~:flt ~o apply aceurat(!ly ~he cr i ter ia f~r r~%'e~teraiiom Amor~g
AMERICAN JOURNAk O~: 726 D!~EST!¥~ D~S[ASES

Cirrh{}tie Liver and Portal tlyperlensio~
Fi~, 5, Biliary clrrh,,.-i~, Large amount~ of i~traeelh*tar fat lead to in{ti~,ti~tc~t,e,.,, i~ outlit~es of the nothde, eanshl~ dif l ieuhy in its interl}retittic, n. ( | ] & E; eedtleed from / 11.0).
the i-1~l 35 ea~e~ of eirrh~i~ um~oeiu~e~ with po!'ta] hypm'- t{'n.&m lhm'e v,a.- only mie e8~,, whh h i . r - than mh~ima] mMular]ty
fat . the i,mq'pP.t.ati,nt of th*' de,/roe ,ff nodu la r i ty m a y haw, Bem~ in ~ 'rroP. T h e c a ; . e w a s o m ~ o f bil iary chu 'h~ i s ; mi,] at i:h,~ t ime of ;~uv~']eaI repa i r of the b]l]avy traei; 8 man()m~4rie recordin~ -f iho portal w,]n |n'o~ure wa~ 200 Iron. of wa{er. |t: i~ md k~own W}lt'[h(~I " {11{* p a i i e n t }m~[ ,~[}~OtlO]Iif)°'813" {~F {~Nol)}t[gR'~?{I Vf~]'i('{*:'< ~ htJW-, ew:% there were n(, ;~i~'ns of lhese complieatious.
Well ,,staI}iished fll:}ro:48 un.s found in ~ lar~e ]}r.p{}P{:hm . f ( ' a ~ w}th as~oe ia l ed 1}oPl.a} ]~yi~ert{mshm. but was a}~o oh~orved in al}-nt hal f of the ea~e~ f r e . of the eomp]ieathm. It was not u]F u~md i(} find a m a r k e d fihrosis and ]~- uodu la r ] ty (I'~i~ '. {;). Mh~hna{ fi!q'o.~i~ am/ well d -ve loped ] .Muta r i ty occasional ly w-P{, f{:mmt fn case.~ of p{~rtaI hyi}ert{msi(m; they ~ e r e t'om~d in fouP of the 2;~ su r~4ieal (:'ases,
3't]o pat torn of vascu la r {iih~tati{:m closely l}aralieh, d tlmt - f {]}}ros i~ a~t~] WaN ( )o rvo /a I : ed \v]t}t t~ortal hypert:ensi,}]~ i ~. tho n,.er,}p. si{~{t ~r{:)u t} mot-{:4osely iha~i ht {he sur~%al ~z]'{ml}~ The re wer{~ ao 81}prociat}le differen{Be8 ]}eiw,.{m t h { ~ (:}oeurr{me{ • of par{mc}lymal and (,apsalaP t{:4an~h~etasi8.
DISCUSSION
T h - findi,~*s ~eom to suppor~ tho c{:mc,,p{ that the , 'o~onerath'( ~
N~W STORIES VOL, 4, NO° 9, I9S9 727

Roth
Fig, 6, Portal cirrhosis. Abanda~t t lbrosls~ a b s e n c e of m . h ~ l a r r e g e ~ e r a t i o m Portal "t~ressurr 3 0 0 r a m . w a | e r bo~h b e f o r e a~d afler portocaval anastomosts~ ( i t . & E~ ~.-
nodule is wu T closely as:~ciat*,d with th- devetopmeul, of portal h )p - r t ens ion in portal cirrhc~sis, In the able,me of i~odules, portal hypertension was seldom associated. Probably th~,ir eeee~tri(; dewqopme~t and oximnsile gr~}wth act to distort and {~ompr~ss the effere~t vein~. The distorti~m and compression eaI~ ,'recur where there are rmt significant am~mnts of fibrosis; by the ap- proximatio~, o:f >,re ad;}ae,:,nt :nodules, the effereut veh~s, exi:~?uded from the centers of 17}to parenchymal feel, beeom,~ compressed, fn cases of postneerotie cirrhosis ibis is f requently seen, as where t lwre is little fibr(~sis to imp-d{, the eXlmm:ting regeneraliw~ nodule, growth continues m*til the nodule m~,ets am}ther expanding nodule. Tiffs possibly explains the l a rge r size of 'the regenerat ive nod,ties in postrmerotic e i r rDMs than of those in Laermec's cirrhosis.
Two ir~struetive eases may serve to iadieate a ctbfieal usefulness in l}te aforementio~ed ol:~servatim~s.
The first is a ease of I.,aennee's cirrhosis in a 39 year ald ma~ with the presentin.g sig~ of gastrointest inal bleeding. See lqg~ 1. lqsophageal varices were not shown to exist~ and at laparot~m~y portal vein manouwtry gave the equiv~cal pressure of 2t;0 ram, of water. It was therefore decided that probably the patient was rmt
AMI~RIGAN JOURNAL OF 728 DIGESTIVE DIS[ASES

Cirrholie laver and Portal I{ypertcnsion.
Bleeding oe<:anse of portal }o'perten.sion a~~d a shumt~ was not ereate<L Biopsy of the liver ~'ave the pat tern that was consistently ~).o|;ed in cases of portal hyper tension; bad a frozen section b-e,~ ordered at the time of surgery, :it miv'ht have been decided that the patient indeed was s u f f - r i ~ from the eft'eels of lmrtaI hypPrten= siam,
The seeo~d ease is illustrat~,d by Fbx. (L A diagn<Ms of bl~,eding es<)I:)hax'eal varices was established, and at operali<:)u a portal t,r~-s= sure of 300 ram. of water was recorded. After ihe sure'teal forms: riot), of a venous shunt the portal pressure was again measured and fom~d to be uaexpectedly still 300 ram. Biopsy of the live*" s]lowed severe portal cirrhosis lint no true regene:rative no<:lules. I t is pos- sible thai: an extraho[:,ai.ie ohstruetion had beeu elevating lhe p~w+.. tal pressure, or)e si tuated distal to the shm~t.
SUMMARY AND CONCI,USIONS
Comparat ive c]bdc.opal}~ologica/observations indicate tim[ nodu,, lar r-ge~mralion in the cirrhotic liver is almost always associated with portal hyperter)sio*~ when the ext rahetmde port ion of {he pot= tal vein is patent, a~d seldom exists i~ more than m b i m a l degr,~e when portal hyperten~ior~ is not well established,
When one observes appreciable amour~t~ of nodalar i ty and fibrosis, and (to a lesser degree} t ela,tja'iec{asia ia~ s~,cih)ns of! cirrhotic liveS's, it may be surmised that portal hypertension exists. Conversely, ihe absence, of nodular i ty speaks strongly a~ainst lhe exisienee of portal hyl)erte~siom
ComImrative observations lend to emphasize- the eor~eept that nodular regenerat ion is the process in cirrhosis essentially resp(m- sible for the develop**wnt of abnormal t'mrtal pressure, probably hy <tisphehig a)~d em~qwessiug effererf{: veins diff,~sely.
Finally, when the e/inieal diagnosis of portal hypert~m~iou is in doubt, biopsy of the live,' at the tim,. of laparoi;o, uy may !,e of value.
RlgFEItENCES
Am, d'. C1i~t, Path,, 22:717, t95:?, ;~+ POPPER, 1.L, aI~d EC'~A% ]iL }listoge~e~is of hepatic eirrho~;i~ ~et'm'tied by ~he three=
dh}mr~ionrd approae~, d,m+ g. Pet}< S;~ :4~}g, I955. a. Mclx'c, oG A. II. Vascular le*io**s of portal cirrhosis. Ar'ch~ Path~ a:ga, 199K
NEW SgRt[$ ¥OG 4, NO. 9, t gSV 729

i :i7~ 115o°
AMERICAN JOURNAL OF 730 D~GEST~VE DIS~SES