Embed Size (px)
Citation preview

Review
Path toward Precision Oncology: Review ofTargeted Therapy Studies and Tools to Aid inDefining "Actionability" of a Molecular Lesion andPatient Management SupportYoung Kwang Chae1,2, Alan P. Pan2, Andrew A. Davis2, Sandip P. Patel3,Benedito A. Carneiro1,2, Razelle Kurzrock3, and Francis J. Giles1,2
Abstract
Precision medicine trials and targeted therapies haveshifted to the forefront of oncology. Although targeted ther-apies have shown initial promise, implementation across thebroad landscape of oncology has many challenges. Theselimitations include an incomplete understanding of the func-tional significance of variant alleles as well as the need forclinical research and practice models that are more patient-centered and account for the complexity of individual patienttumors. Furthermore, successful implementation of targetedtherapies will also be predicated on efforts to standardizethe framework for patient management support. Here, we
review current implementations of targeted therapies in pre-cision oncology and discuss how "actionability" is defined formolecular targets in cancer therapeutics. We also commenton the growing need for bioinformatics tools and data plat-forms to complement advances in precision oncology. Final-ly, we discuss current frameworks for integrating precisiononcology into patient management and propose an integratedmodel that combines features of molecular tumor boardsand decision support systems. Mol Cancer Ther; 16(12); 2645–55.�2017 AACR.
See related article by Pili�e et al., p. 2641
IntroductionWith the evolving landscape of medical oncology, focus has
shifted away from nonspecific cytotoxic treatment strategiestoward therapeutic paradigms more characteristic of precisionmedicine, whereby therapy is delivered to patients on the basis ofunique patient clinical and molecular features. When applyingprecision medicine, the goal is to tailor diagnosis and treatmentto each patient's individual biologic profile, while minimizingexposure to unnecessary or ineffective therapies. Technologicaladvances in accessibility of patient and tumor genomics haveimproved understanding of tumor biology and led to enhance-ments in the ability to identify and target major molecular driversof cancer. These developments have shifted precision oncology tothe forefront of cancer treatment strategies.
Despite early successes of targeted cancer therapies, complex-ities in therapeutic development and application have beenrevealed, in many cases due to considerable genomic heteroge-
neity among tumor histology subtypes. Some of these complex-ities will need to be addressed by customized combinationtherapy or bymoving targeted therapeutics fromend-stage diseaseto earlier stages,when thediseasehas evolved to a lesser extent (1).Although significant advances in targeted therapeutics have beenobserved in some areas in medical oncology—notably in late-stage melanoma (2) and non–small cell lung cancer (3)—thereare many areas that have not experienced similar progress, at leastin part due to the paucity of biomarker-driven trials (4–6).
Limitations also exist with respect to clinical trial design, avail-ability of biomarker data, and challenges in understanding howto use existing, yet un-annotated data in clinical practice. Theseobstacles have limited the application of targeted therapies andhighlight the need for validated bioinformatics tools and dataplatforms that can help guide clinicians in patient management.
Here, we review the implementation of precision oncologytrials to study targeted therapies.We also discuss considerations indescribing the "actionability" of amolecular target, with respect tothe biomarker–response association. Lastly, we comment onimportant topics relevant to the development of a standardizedframework for integrating precision oncology trials and targetedtherapies into patient management.
Clinical development pathway of targeted therapiesTargets of precision therapeuticsmay include aberrant products
of altered genes, cell surface molecules differentially expressed incancer, andmolecules that regulate immune cell activity. Supportfor targeted therapies in oncology has been driven by severalfactors. First, the advent of next-generation sequencing (NGS) andthe emergence of increasingly cost- and time-efficient genomicprofiling methods have advanced our capability to develop novel
1Developmental Therapeutics Program, Division of Hematology Oncology,Northwestern University Feinberg School of Medicine, Chicago, Illinois. 2Depart-ment of Medicine, Northwestern University Feinberg School of Medicine, Chi-cago, Illinois. 3Center for Personalized Cancer Therapy, Moores Cancer Center atthe University of California San Diego, La Jolla, California.
Y.K. Chae and A.P. Pan contributed equally to this article.
Corresponding Author: Young Kwang Chae, Northwestern University FeinbergSchool of Medicine, 645 North Michigan Avenue, Suite 1006, Chicago, IL 60611.Phone: 312-926-4248; Fax: 312-695-0370; E-mail:[email protected]
doi: 10.1158/1535-7163.MCT-17-0597
�2017 American Association for Cancer Research.
MolecularCancerTherapeutics
www.aacrjournals.org 2645
on September 20, 2020. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

clinical trial designs (7–9), and current turnaround times of threeto four weeks (half of which is generally attributed to specimencollection) have made tumor molecular profiling clinically fea-sible in patient management (10).
Second, improved understanding of the molecular pathologyof disease has aided in the capacity to develop therapeuticstargeting oncogenic drivers. Initial efforts using matched ther-apeutic agents were driven by the perspective that molecularalterations were specific to tumor location and histopathology,and early clinical development of targeted therapies oftenfollowed that of standard-of-care cytotoxic chemotherapies.However, lack of evidence supporting this approach led to trialdesigns that match specific molecular alterations to therapeuticagents, independent of tumor cell origin (11–14). These con-siderations contributed to the birth of precision oncology trials.Nonetheless, adaptations have been necessary to address lim-itations of classical trial designs. These challenges includetechnical and practical concerns hindering patient selectionand biomarker discovery (11).
Precision oncology trialsSeveral factors provided the impetus for precision oncology
trials. First, while traditional cytotoxic chemotherapy targetscommon, generic disease mechanisms shared among tumors,tumor heterogeneity beyond random variation has been repeat-edly demonstrated (11). Second, the use of a biomarker approachto tailor treatments to subsets of patients with the same tumortype became more common, particularly in programs that aimedto show a significant therapeutic effect in unselected patientswhere the prevalence of the biomarker was low (11). This createdchallenges in advancing a drug's development, especially if ther-apeutic effects were detectable in only a small patient population.As a result, early phase trials now feature selected patient popula-tions tominimize the inclusion of patients unlikely to respond tonovel treatments.
The evolution of the clinical drug development pathway hasresulted in flexible trial designs, including "umbrella" and "bas-ket" trials (5, 11, 15, 16). "Umbrella" trials, such as BATTLE-2(NCT01248247), Lung-MAP (NCT02154490), and I-SPY(NCT01042379), assign patients with particular tumor histolo-gies to treatment regimens specifically developed to target thetumor's oncogenic molecular pathway. The Leukemia & Lympho-ma Society's (LLS) Beat AMLCore Study is particularly unique as itwill be the first-ever precision oncology trial for a blood cancer(NCT02927106). Newly diagnosed acute myeloid leukemia(AML) patients will be assigned to receive investigational thera-pies targeting particular hematologic malignancies based ongenomic profiling.
Alternative approaches to "umbrella" trials are "basket" and"hybrid" trials. "Basket" trials, such as CUSTOM (NCT01306045)and SHIVA (NCT01771458) treat patients with specific agentstargeting aberrant molecular pathways, independent of tumororigin. In this way, therapeutic agents may be considered effectiveacross tumor types. Lastly, "hybrid" trials incorporate aspects ofboth "umbrella" and "basket" trials into one protocol and featuresubtrials that target different molecular drivers within the samehistology or the samemolecular driver across different histologies(16). Several of these trials have been published, and trials such asUCSD PREDICT and the MD Anderson Phase I initiative dem-onstrate that approximately 25% to 30% of patients can bematched to therapy when larger NGS panels are used, as well as
improved outcomes inmatched versus unmatched patients, albe-it in a nonrandomized setting (13, 14, 17).
Nonetheless, limitations do exist with flexible trial designs. Themajority of trials feature monotherapies, yet treatment strategiesincorporating drug combinations have provided benefit topatients with multiple genomic aberrations or advanced cancers(10). Approval of targeted drug combinations remains a challengebecause of the potential for overlapping drug toxicities. Further-more, the SHIVA trial notably concluded that off-label use ofmolecularly guided targeted therapies did not show improvementin progression-free survival over conventional therapies (18).However, features of the trial, including choice of inappropriatelymatched therapies, use of monotherapies ineffective in advancedcancers, and assignment of targeted treatments not based onmolecular profiling, have been criticized (19, 20). Lessons learnedfrom the trial have been important considerations in the design oflater trials, and consequently, support for precision therapyremains encouraging.
Here, we briefly discuss representative "hybrid" and "basket"trials led by different government initiatives, pharmaceuticalcompanies, and scientific organizations, including the NationalCancer Institute's Molecular Analysis for Therapy Choice (NCI-MATCH) trial (21), the Signature Program (ref. 22; Novartis), theMyPathway trial (ref. 23;Genentech), and theAmerican Society ofClinical Oncology (ASCO)-led Targeted Agent and Profiling Uti-lization Registry (TAPUR) study (ref. 24; Table 1).
NCI-MATCH. NCI-MATCH is an ongoing trial that analyzespatient tumors for actionable mutations for which targeted treat-ments are available (NCT02465060; ref. 25).NCI-MATCHenrollspatients with advanced solid tumors and lymphomas who are nolonger responding or never responded to standard treatment andevaluates whether treatment based on the molecular profile ofdisease, independent of tumor origin, provides clinical benefit(26). Prior to enrollment, NCI-MATCH provides a pretreatmentbiopsy to screen for eligibility in one of the treatment arms.Furthermore, if a patient does not match with the initial biopsyand a potential treatment match later becomes available, thepatient may require rebiopsy to evaluate eligibility. Although thisprovides a great opportunity for biomarker exploration, it islimiting for patients with tumors not amenable to rebiopsy. Sinceopeningwith 10 treatment arms, NCI-MATCHhas now expandedto 30 treatment arms.
Signature program. The Signature Program includes exploratorysignal-finding studies, with primary endpoints assessing theclinical benefit rate of molecularly guided targeted therapies(27). A key feature of the Signature Program is expedited protocoldelivery, whereby physicians may request to receive a protocol ifa patient is determined to have an actionable mutation in anytissue type.
To date, five Signature trials are active (NCT02160041,NCT02186821, NCT02187783, NCT01885195, andNCT01833169), with the remaining either completed or closeddue to low enrollment. Preliminary data for 106 patients withCDK4/6 pathway aberrations and treated with ribociclib showedclinical benefit (complete/partial response or stable disease) in 19patients at week 16, with preliminary antitumor activity addi-tionally observed in 4 patients (28, 29). Further assessment of thecorrelation between clinical benefit and genomic mutation pro-filing is ongoing.
Chae et al.
Mol Cancer Ther; 16(12) December 2017 Molecular Cancer Therapeutics2646
on September 20, 2020. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

Table
1.Rep
resentativebiomarker-based
precisiononcology"basket"
and"hyb
rid"trials
Program
Design
Maligna
ncytype
Stud
yarms
Molecu
lartargets
Drug
Sponsor
Referen
ce
NCI-MATCH
Pha
seII
Adva
nced
solid
tumors
30EGFR-activatingmutation
Afatinib
NCIan
dECOG-A
CRIN
NCT024
650
60
þLy
mpho
ma
HER2-activating
mutation
Afatinib
METam
plifi
cation
Crizo
tinib
METexon14
deletion
Crizo
tinib
EGFRT79
0M
orrare
activating
mutation
AZD929
1ALK
tran
slocation
Crizo
tinib
ROS1tran
slocationorinve
rsion
Crizo
tinib
BRAFV600E/R
/K/D
mutation
Dab
rafenib/trametinib
PIK3C
Amutationoram
plifi
cation
Taselisib
HER2am
plifi
cation
Trastuzum
ab/pertuzu
mab
mTORmutation
TAK-228
TSC1orTSC2mutation
TAK-228
PTENmutationordeletionorPTENexpression
GSK26
3677
1PTENloss
GSK26
3677
1HER2am
plifi
cation
Ado-trastuzum
abem
tansine
BRAFfusionorBRAFno
n-V600mutation
Trametinib
NF1mutation
Trametinib
GNAQ/G
NA11mutation
Trametinib
SMO/PTCH1mutation
Vismodeg
ibNF2inactivating
mutation
Defactinib
cKIT
exon9/11/13/14mutation
Sun
itinib
FGFRpathw
ayab
errations
AZD454
7DDR2mutation
Dasatinib
AKT1mutation
AZD53
63
NRASmutation
Binim
etinib
CCND1,2
,3am
plifi
cation
Palbociclib
CDK4orCDK6am
plifi
cation
Palbociclib
dMMRdefi
cien
cyNivolumab
NTRKfusions
Larotectinib
BRCA1orBRCA2mutation
AZD1775
Signa
ture
Pha
seII
Advanced
solid
tumors
þhe
matological
8PI3CAmutation,
amplifi
cation;
PTENmutation,
loss;
PIK3R
1mutation
Bup
arlisib
Nova
rtis
NCT01833
169
maligna
ncies
FGFR1/2/3,
FLT
3,c-KIT
mutationoram
plification;
PDGFRa/
b,VEGFR1/2,
RET,T
rkA(N
TRK1),C
SF-1R
Dovitinib
NCT0183172
6
RAS,R
AF,M
EK1/MEK2,
NF1mutation
Binim
etinib
NCT01885195
BRAFV600activating
mutation
Encorafenib
NCT01981187
CDK4/6
mutationoram
plifi
cation,
cyclin
D1/D3
amplifi
cation,
orp16
mutation/loss
Ribociclib
NCT021877
83
FGFRmutation,
amplifi
cation,orfusion;
Translocationof
FGFR1/2/3/4;Ligan
dam
plifi
cation
BGJ398
NCT02160041
ALK
/ROS1mutation,
amplifi
cation,
tran
slocation,
or
rearrang
emen
tCeritinib
NCT02186821
PTCH1,SMO
activa
ting
mutation
Sonideg
ibNCT020
026
89
MyP
athw
ayPha
seII
Adva
nced
solid
tumors
4HER2ove
rexp
ression,
amplifi
cation,
oractivating
mutation
Trastuzum
ab/pertuzu
mab
Gen
entech
NCT020
91141
EGFRmutation
Erlotinib
BRAF-activatingmutation
Vem
urafen
ib/cobim
etinib
Hed
geh
ogpathw
aymutation
Vismodeg
ib
(Continue
donthefollowingpag
e)
Path Toward Precision Oncology
www.aacrjournals.org Mol Cancer Ther; 16(12) December 2017 2647
on September 20, 2020. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

MyPathway. MyPathway evaluates treatment regimens foradvanced cancers in patients with specific molecular alterationsrelated to HER2-overexpression, -amplification, or -activatingmutations, epidermal growth factor receptor (EGFR)-activatingmutation, BRAF-activating mutations, and potentially actionableHedgehog pathway mutations (NCT02091141; ref. 23).
Preliminary findings observed objective response in 22 out of118 patients across 9 tumor types, with observed clinical activityin patients with HER2-amplified bladder, biliary, and colorectalcancer, as well as patients with BRAF-mutated lung cancer (30,31). Interim data have demonstrated activity in expanded cohortsofHER2-amplifiedormutatedpatientswith colorectal, urothelial,and biliary cancers, particularly in colorectal cancer, where anoverall response rate and clinical benefit rate of 37.5% and 46.9%was observed, respectively (32–34).
TAPUR. TAPUR supports targeted therapies by providing flexi-bility in tumor and blood sample selection for genomic profiling,as well as less-restrictive eligibility criteria for study enrollment(NCT02693535; refs. 24, 35). This design allows for enrollmentfrom academic and private practice settings, thereby expandingthe potential application of study findings to aid in providinginsights in real clinical practice. The Syapse Precision MedicinePlatform helps guide and automate the study operations work-flow, integrate patient data and clinical outcomes, and supportreview of cases during molecular tumor boards.
Several pharmaceutical companies have agreed to participateand provide study drugs without any patient cost. Currently, theseinclude 17 drugs targeting 15 targeted therapy pathways inadvanced solid tumors and hematological malignancies, includ-ing multiple myeloma and B-cell non-Hodgkin lymphoma.TAPUR also plans to lower the enrollment age from 18 to 12years in order to allow participation to adolescent patients forstudy drugs in which there is a defined adolescent dose.
DiscussionLimitations of targeted therapies and precision oncology trials
Although personalized cancer therapies are evolving intoachievable standards in medical oncology, significant chal-lenges exist. These include insufficient evidence to guide prac-tical biomarker implementation, limited understanding of thefunctional effects of variant alleles, and a lack of consensusregarding the level of evidence required to select patients forpersonalized therapies.
First, treatment strategies for which reliable predictive biomar-kers exist are limited, with evidence of foreseeable clinical benefitfound for only select genomic alterations in a limited number ofcancer types. Consequently, there is often little support for routineclinical implementation of biomarker-targeted therapies. Further-more, trial-based studies on rare biomarkers may have highscreening failure rates during patient selection.
Second, the development of targeted therapies requires strongevidence that genetic alterations within a particular disease havean impact on tumor behavior (36, 37). There are often limiteddata assessing the functional significance of variant alleles andlack of consensus as to what constitutes the minimum level ofevidence necessary to define a variant allele as a potential bio-marker in clinical practice (37). Improving our understanding oftumor biology and establishing these standards are crucial tocontinued progress in precision oncology.Ta
ble
1.Rep
resentativebiomarker-based
precisiononcology"basket"
and"hyb
rid"trials
(Cont'd)
Program
Design
Maligna
ncytype
Stud
yarms
Molecu
lartargets
Drug
Sponsor
Referen
ce
TAPUR
Pha
seII
Adva
nced
solid
tumors
15VEGFRmutation,
amplifi
cation,
ove
rexp
ression
Axitinib
ASCO
NCT026
935
35þ
hematological
Bcr-abl,SRC,L
YN,L
CKmutation
Bosutinib
maligna
ncies
ALK
,ROS1,METmutation
Crizo
tinib
CDKN2A
/p16
loss,C
DK4,C
DK6am
plifi
cation
Palbociclib
CSF1R,P
DGFR,V
EGFRmutation
Sun
itinib
mTOR,T
SCmutation
Tem
sirolim
usEGFRmutation
Erlotinib
ERBB2am
plifi
cation
Trastuzum
ab/pertuzu
mab
BRAFV600Emutation
Vem
urafen
ib/cobim
etinib
PTCH1deletion,
orinactivating
mutation
Vismodeg
ibKRAS,N
RAS,B
RAFwild
-typ
eCetux
imab
Bcr-abl,SRC,K
IT,P
DGFRB,E
PHA2,
FYN,L
CK,Y
ES1
mutation
Dasatinib
RET,V
EGFR1,VEGFR2,
VEGFR3,
KIT,P
DGFRb,
RAF-1,
BRAF,m
utation/am
plifi
cation
Reg
orafenib
BRCA1/BRCA2inactiva
ting
mutation,
ATM
mutationor
deletion
Olaparib
POLE
/POLD
1mutation
Pem
brolizum
ab
Abbreviations:N
CI,Nationa
lCan
cerInstitute;
MATCH,M
olecularAna
lysisforThe
rapyCho
ice;
ECOG-A
CRIN,E
astern
CooperativeOncologyGroup
-American
CollegeofRad
iologyIm
agingNetwork;T
APUR,T
argeted
Agen
tan
dProfilingUtilizationReg
istry;
ASCO,A
merican
SocietyofClinical
Oncology.
Chae et al.
Mol Cancer Ther; 16(12) December 2017 Molecular Cancer Therapeutics2648
on September 20, 2020. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

Level of evidence required to define "Actionability"The application ofNGShas significantly improved the prospect
of utilizing genetic screening as a practical method to identifygenetic variants that may be associated with an increased risk ofdeveloping cancer. The benefit of these advances has been welldocumented in patients with BRCA1/2 mutations, and certaingenetic variants have measurable effects on protein function thatsignificantly increase the risk of developing breast cancer (38–40).The clinical applicability of the BRCA1/2 mutations has beendifficult to replicate with other genetic variants thatmay representpotential molecular targets.
Furthermore, different criteria for treatment selection existwhen considering patients with variants of unknown significance(VUS). As such, the risk of excluding patientswhomay still benefitfrom treatment exists. This variability in defining selection criteria
canbe seen across "umbrella" and "basket" trials. For example, theNCI-MATCH protocol establishes rules of evidence for treatmentselection, while independent models for classifying the "action-ability" of biomarkers have also been proposed (Table 2). NCI-MATCH's criteria, as well as the schemes proposed by Van Allenand colleagues (41), Vidwans and colleagues (42), Meric-Bern-stam and colleagues (36), Sukhai and colleagues (43), and Carrand colleagues (44), provide individual levels of classificationthat describe the strength of evidence associating particular bio-markers with disease response in given tumor types. Overall,similarities exist between these classification schemes, and NCI-MATCH's criteria have demonstrated practicality and applicabil-ity in practice.
Despite the difficulty in designing trials around patients withVUS, there is utility in including these patients in trials. For
Table 2. Comparison of representative classification schemes assessing the level of evidence for biomarker–response association
Model Classification Institution Reference
Van Allen et al. (2014) Level A Validated association between biomarker and response forthis indication
Dana-Farber Cancer Institute (41)
Level B Limited clinical evidence exists supporting a biomarker–response association in the same tumor type
Level C Clinical evidence exists supporting a biomarker–responseassociation in a different tumor type
Level D Preclinical evidence exists supporting a biomarker–responseassociation
Level E Inferential biomarker–response associationVidwans et al. (2014) Level 1 Drug approved with companion diagnostic UCSD Moores Cancer Center (42)
Level 2 Therapeutic approach outlined in treatment guidelinesLevel 3 Clinical evidence indicating responsiveness to drug class(es)Level 4A Clinical trialswith biomarker aberration as an inclusion criteriaLevel 4B Preclinical evidence indicating responsiveness to
drug class(es)Level 4C Evidence in genetic disease with biomarker aberrationLevel 5 No evidence
NCI-MATCH (2015) Level 1 Demonstrated effectiveness with approved drug NCI and ECOG-ACRIN (26)Level 2A Eligibility criteria in ongoing clinical trialLevel 2B Identified in N of 1 responsesLevel 3 Preclinical inferential data only
Meric-Bernstam et al. (2015) Level 1A Drug has been FDA approved for a specific biomarker in thesame tumor type
MD Anderson Cancer Center (36)
Level 1B Drug has been demonstrated to predict tumor response orprovide clinical benefit in a biomarker-selected cohort of a
study in the same tumor typeLevel 2A Biomarker has been demonstrated to predict tumor response
to drug in a study in the same tumor typeLevel 2B Biomarker has been demonstrated to predict tumor response
to drug in a study in a different tumor typeLevel 3A Scientific rationale exists for a biomarker–response
association, but clinical evidence is limitedLevel 3B Preclinical data
Sukhai et al. (2015) Class 1 Variants can be used for direct patient care Princess Margaret Cancer Centre (43)Class 2 "Actionability" has been demonstrated in a different disease
site/histologyClass 3 "Actionability" has been demonstrated in gene in a particular
disease site/histology; however, "actionability" of specificvariant has not been demonstrated.
Class 4 "Actionability" has been demonstrated in gene in a differentdisease site/histology; however, "actionabillity" of specific
variant in this disease site/histology has not beendemonstrated
Class 5 Variants are of unknown significanceCarr et al. (2016) Tier 1 Highly actionable in exploratory trials AstraZeneca (44)
Tier 2 Potentially actionable in exploratory trialsTier 3 Not currently actionable
Abbreviations: NCI, National Cancer Institute;MATCH,Molecular Analysis for Therapy Choice; ECOG-ACRIN, Eastern CooperativeOncologyGroup-American Collegeof Radiology Imaging Network.
Path Toward Precision Oncology
www.aacrjournals.org Mol Cancer Ther; 16(12) December 2017 2649
on September 20, 2020. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

example, while the TAPUR protocol does not explicitly excludepatients with VUS, these cases are encouraged to be sent toTAPUR's molecular tumor board to discuss whether rationaleexists that the patient may derive clinical benefit from targetedtherapies. Additional focus will be necessary, as the predictivevalue of genetic variants on associated disease risk, such as theexample of BRCA1/2 variants and breast cancer risk, may beinitially unknown without further investigation. Lastly, it isimportant to note the distinction between germline mutations,such as BRCA1/2, and somatic mutations, such as those in EGFR.Although the availability of data differs across the literature forgermline and somatic mutations, ongoing efforts exist to bridgethis gap and expand this area.
Framework for Precision OncologyWhile defining the "actionability" of a molecular target is
subjective, a clearer consensus is necessary for building a frame-work for implementing targeted therapies into clinical practice.This framework includes components such as bioinformaticstools, data repositories, and platforms for patient managementsupport.
Bioinformatics toolsIncreased understanding of themutational landscape of cancer
has been accompanied by difficulties in determining the func-tional relationships between molecular alterations and tumori-genesis. Although independent knowledge of the oncogenicpotential of rare mutations exists for some genetic alterations,there is often insufficient evidence to support therapeuticapproaches that target these alterations (45). As such, there is agrowing need for bioinformatics tools that can shed light onunknown mechanisms of disease associated with specific geneticvariants. Numerous resources have previously been reviewed, andrepresentative tools are included in Table 3.
These tools include independent methods and combinedmethods that integrate the prediction scores of other tools. Themethods differ in their prediction algorithms for annotating andscoring variants, with variance in parameters including sequenceconservation and homology as well as protein structure andfunction. Several tools have been previously reviewed for perfor-mance (46, 47), with respect to relative and predictive utility.While individual tools outperformed others in different factors—all-around performance, prediction rate, sensitivity and specific-ity, etc.—a combined approach using multiple prediction toolsprovided benefits over individual methods, including a moreevenly balanced sensitivity and specificity (46).
The availability of bioinformatics tools has greatly improvedour understanding of the genomic landscape of cancer. None-theless, there is variability in how tools generate predictionmodels. For example, BRAF V600E has been demonstrated as avaluable target for BRAF and MEK tyrosine kinase inhibitors inanticancer treatments (48–50), yet it can be considered VUS byprediction tools under varying parameters. To address this, initia-tives to create repositories and databases for variant-level databased on these bioinformatics tools are prevalent, including thoseby TCGA (NCI and NHGRI), cBioPortal for Cancer Genomics(Memorial Sloan-Kettering Cancer Center), My Cancer Genome(Vanderbilt-Ingram Cancer Center), COSMIC (Wellcome TrustSanger Institute), and ClinVar (NCBI). However, many databasesare limited by the lack of defined data on the functional
significance of variants and a general inability to sufficiently minethe scientific literature for relevant information. Nonetheless,efforts have been promising. For example, My Cancer Genome'sDIRECT database has catalogued 188 primary EGFRmutations inlung cancer and their associated drug responses (51). Althoughthe initial objective was to catalogue relevant somatic mutationsin lung cancer, the goal is to expandDIRECT to include all knownmutations of clinical significance across various cancers. Giventhat VUS are evolving targets, efforts such as these will ultimatelyhelp clinicians better predict the functional significance ofthese variants.
Data sharingComplementing the advancements in precision oncology is the
need to develop platforms for data sharing. Although analytictechnologies have experienced success in different industries,implementation in a clinical setting requires further adaptation.The American Association for Cancer Research's (AACR) ProjectGenomics, Evidence, Neoplasia, Information, Exchange (GENIE;ref. 52) and the Oncology Precision Network (OPeN; ref. 53)—formed by Intermountain Healthcare, Stanford Cancer Institute,Providence St. Joseph Health, and Syapse—are promising effortsthat aim to aggregate and link cancer genomics data and clinicaloutcomes.
The gaps in applyingmutational andmechanistic discoveries toderive clinically meaningful value in patient care underscore theimportance of complementing the implementation of targetedtherapies with efficient data compilation and sharing to helpclinicians make informed decisions. Despite the remainingchasm, the efforts by GENIE and OPeN are promising stepsforward and serve as valuable models in clinical practice.
Patient management supportMolecular tumor boards. Precision oncology practice models cen-tered around molecular tumor boards (MTB) have been valuableimplementations in guiding personalized patient management.Recent experiences with MTBs have provided insight on theireffectiveness in practice. Several experiences are discussed here,including those with the Northwestern OncoSET (Sequence,Evaluate, Treat) program and the University of California SanDiego (UCSD) Moores Cancer Center.
The Northwestern OncoSET program—through collaborationbetween the Robert H. Lurie Comprehensive Cancer Center andNorthwesternMedicine—launched in2015 as a research initiativedesigned to provide patients with personalized cancer treatmentoptions through a combined oncology and genomics approach(54). To support the patient management decision process,OncoSET has established the Lurie Cancer Center's MTB which,similar to existing tumor boards, brings together a multidisci-plinary team that meets weekly to discuss cases and decide uponrecommendations for patient treatment plans, whichmay involvetreatment in a clinical trial or alternative therapies.
Two experiences with MTBs at the Moores Cancer Center havebeen reviewed—one presenting various cancer cases (55) and thesecond presenting breast cancer cases (56). Discussion of pre-sented findings culminated in a consensus on a recommendedcourse of treatment tailored for each patient, with the ultimatetreatment decision left to the discretion of the treating physicians.Published findings from these MTB experiences have been pos-itive. In the first study, among the 34 patients whose cases were
Chae et al.
Mol Cancer Ther; 16(12) December 2017 Molecular Cancer Therapeutics2650
on September 20, 2020. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

Table
3.Rep
resentativepredictiontoolsforclassifyingthefunctiona
lsignificanceofvarian
talleles
Predictiontool
Fun
ction
Fea
ture
SelectionBasis
Fea
turesUsedin
Prediction
Referen
ce
MutationA
ligne
rVariant
hotspotan
alysis
Indep
enden
tProtein
domains
(45)
VEP
Variant
anno
tation
Predictionscoresfrom
SIFTþ
PolyPhe
n-2
Seq
uenceco
nserva
tionþ
protein
phy
sico
chem
istryþ
protein
domains
þseque
nceco
ntext
(63)
SIFT
Variant
anno
tation
Indep
enden
tSeq
uenceco
nserva
tion
(64)
PolyPhe
n-2
Variant
anno
tation
Indep
enden
tSeq
uenceco
nserva
tionþ
protein
phy
sico
chem
istryþ
protein
domains
þseque
nceco
ntext
(65)
MutationA
ssessor
Variant
anno
tation
Indep
enden
tSeq
uenceco
nservation
(66)
Cond
elVariant
anno
tation
Combined
(SIFTþ
PolyPhe
n-2þ
MutationA
ssessor)
Seq
uenceco
nservationþ
protein
phy
sico
chem
istryþ
protein
domains
þseque
nceco
ntext
(67)
CHASM
Variant
anno
tation
Indep
enden
tSeq
uenceco
nserva
tionþ
protein
phy
sico
chem
istryþ
protein
domains
þseque
nceco
ntext
(68)
Can
DrA
Variant
anno
tation
Combined
(SIFTþ
PolyPhe
n-2þ
MutationA
ssessorþ
etc.)
Seq
uenceco
nserva
tionþ
protein
phy
sico
chem
istryþ
protein
domains
þseque
nceco
ntext
(69)
MutPred
Variant
anno
tation
Indep
enden
tSeq
uenceco
nserva
tionþ
protein
phy
sico
chem
istryþ
protein
domains
þseque
nceco
ntext
(70)
SNPs&
GO
Variant
anno
tation
Indep
enden
tSeq
uenceco
nserva
tionþ
protein
phy
sico
chem
istryþ
protein
domains
þseque
nceco
ntext
(71)
PANTHER
Variant
anno
tation
Indep
enden
tSeq
uenceco
nserva
tion
(72)
PhD
-SNP
Variant
anno
tation
Indep
enden
tSeq
uenceco
nserva
tionþ
protein
phy
sico
chem
istryþ
protein
domains
þseque
nceco
ntext
(73)
CAROL
Variant
anno
tation
Combined
(SIFTþ
PolyPhe
n-2)
Seq
uenceco
nserva
tionþ
protein
phy
sico
chem
istryþ
protein
domains
þseque
nceco
ntext
(74)
CoVEC
Variant
anno
tation
Combined
(SIFTþ
PolyPhe
n-2þ
SNPs&
GO
þMutationA
ssessor)
Seq
uenceco
nserva
tionþ
protein
phy
sico
chem
istryþ
protein
domains
þseque
nceco
ntext
(46)
Abbreviations:V
EP,V
arient
EffectPredictor;SIFT,SortingIntolerant
From
Tolerant;PolyPhe
n-2,Polymorphism
Phe
notyping;C
ond
el,C
onsen
susDelteriousne
ss;C
HASM,C
ancer-SpecificHigh-Throug
hput
Ann
otationof
Somatic
Mutations;Can
DrA
,Can
cer-SpecificDrive
rMissenseMutationAnn
otation;
SNPs&
GO;PANTHER,Protein
Ana
lysisThroug
hEvo
lutiona
ryRelationships;CAROL,
Combined
Ann
otationSco
ring
Tool;CoVEC,
Consen
susVariant
EffectClassification.
Path Toward Precision Oncology
www.aacrjournals.org Mol Cancer Ther; 16(12) December 2017 2651
on September 20, 2020. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

presented, 3 of 11 evaluable patients achieved partial responses(55). In the second study, 17 of 43 patients were treated incongruence with the recommendations of the MTB, and 7 of the17 achieved stable disease for at least 6 months or partial remis-sion (56).
Three models developed by oncology pharmacy practi-tioners—at the University of Wisconsin, Indiana University, andMoffit Cancer Center—have also been described (57). Althoughthe models vary, they share commonalities in benefitting from amultidisciplinary approach to precision oncology. Results fromthe MTB within Indiana University's Health Precision GenomicsProgram observed a significant difference in number of patientsreaching favorable progression-free survival between those trea-ted with genomically guided therapy (43.2%) and those treatedwith non–genomically guided therapy (5.3%; ref. 58). Overall,these experiences underscore the importance of expanding oppor-tunities to participate in MTBs in clinical practice.
Decision support system. An alternative platform for bridging thegap between identification of molecular targets and implemen-tation of personalized cancer therapeutics has been developedwithin the Institute for Personalized Cancer Therapy (IPCT) atMD Anderson Cancer Center (36, 59). To aid in clinical decision-
making, the precision oncology decision support (PODS) teamprovides clinicians with relevant information for assessing the"actionability" of variant alleles and identifying availablematched therapies and clinical trials. Although public databasesprovide variant-level information about published drug associa-tions, information about the functionality of molecular altera-tions and relevant clinical trials is often not readily available,leaving clinicians to filter through scientific literature and publicdatabases. Consequently, the PODS platform seeks to streamlinethe treatment decision process by communicating curated infor-mation to clinicians.
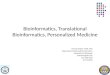
Recent experiences with MTBs and decision support systemshave demonstrated the effectiveness of these platforms as frame-works for supporting personalized patient management. None-theless, opportunities for adaptation exist. Figure 1 compares theworkflow for these approaches. AlthoughMTBs foster knowledgesharing, the responsibility still falls on clinicians to present casesand participate in reaching recommended treatment decisions.Decision support systems provide curated information to clin-icians which, while alleviating the burden on clinicians, offers lessopportunities for multidisciplinary review and discussion. Forboth approaches, there are associated time and resource commit-ments, which limit feasibility. One approach to address this has
Figure 1.
Patient management workflow strategies. Patient management workflow strategies with an (A) independent review model, (B) molecular tumor boardmodel, (C) decision support system model, and (D) integrated model. In A, clinicians filter through scientific literature and public databases to reachtreatment decisions for patients. B and C provide clinicians with support for making informed treatment decisions. In B, clinicians present cases to moleculartumor boards and a recommended course of action is provided. In C, decision support systems provide "curated" information to help clinicians maketreatment decisions. In D, extracted and curated data are reviewed by clinicians and, if necessary, with the support of molecular tumor boards.
Chae et al.
Mol Cancer Ther; 16(12) December 2017 Molecular Cancer Therapeutics2652
on September 20, 2020. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

been the development of virtual decision support tools thatprovide clinicians with the functionality to input patient anddisease features in a portal and view recommended course oftreatments. While this provides flexibility, the limiting factorwould be the availability of pre-prepared decision support.
Nonetheless, data-driven endeavors continue to drive advancesin precision oncology. For example, Watson Genomics fromQuest Diagnostics (60) is a significant pursuit that aims to helpclinicians identify tailored treatments for their patients. TheUniversity of North Carolina's Lineberger Comprehensive CancerCenter has experimentedwithWatson inMTBs (61). Out of 1,000patients, Watson independently identified the same treatmentsrecommended by the MTB in 99% of cases. Furthermore, Watsonidentified new treatment strategies not found by clinicians in 30%of cases and has also been taught to read radiologic scans andmolecular diagnostics to identify abnormalities and potentiallyactionable genetic mutations, highlighting a promising opportu-nity for implementation as part of standard of care.
Future of precision oncology: Integrated patient managementmodel
Limitations exist with using either MTBs or decision supportsystems independently. For example, artificial-intelligence plat-forms can only yield value from published data. In these cases,clinical experience provides crucial insight. To address theseconcerns, we propose an integrated model that combines thestrengths of both approaches, allowing for extracted and curateddata to be reviewed by clinicians and, if necessary, with thesupport of MTBs (Fig. 1). This model provides clinicians withthe advantage of utilizing bioinformatics support and benefittingfrom knowledge sharing among peers, so as to ensure that theinformation used for informed treatment decisions is as error-proof as possible.
ConclusionTargeted therapies are widely regarded as the framework for
future treatment paradigms in the precision oncology era. Withimproved understanding of the molecular pathways that drivetumor biology and the increasing availability of cost- and time-efficient NGS technologies, the reality of such a paradigm shiftcomes into sharper focus. Nonetheless, although success has beendemonstrated in some areas within oncology, the overall treat-ment paradigm remains in its infancy,withmany challenges yet tobe addressed before its potential can be fully realized across thebroad landscape of oncology.
A multitude of considerations has limited the study of bio-marker data and the clinical application of potential moleculartargets (42, 62). Although high-throughput technologies haveallowed sequencing data to be generated quickly and convenient-
ly, the challenge of determining the functional significance ofvariant alleles remains. Because of this, "actionability" of molec-ular targets is often defined differently. Consequently, there is alack of consensus regarding the level of evidence required to selectmolecular targets for clinical application. Addressing these con-siderations is important, as implementation of targeted therapiesnecessitates that the right "actionability" is applied to the rightpatients.
Furthermore, molecular alterations often do not segregate bytumor origin. Patients with metastatic disease usually have mul-tiple genomic alterations, making their tumors both unique andcomplex. These considerations suggest the need for customizedcombinations of therapy, which is a patient-centered paradigmthat departs significantly from current drug-centered models.Finally, genomic testing and matching has been applied almostexclusively in patients with metastatic disease which has been,more often than not, heavily pretreated. Hence, many precisionmedicine studies have high attrition rates due to the patientcondition deteriorating quickly, and, unsurprisingly, resistancerates are high in these patients with complicated tumors who aregenerally treated with matched monotherapy. Moving to earlierstages of the disease, a strategy that was dramatically successful inchronic myelogenous leukemia, warrants investigation in solidtumors as well.
Nonetheless, there is hope that ongoing and future precisionmedicine trials will continue to provide insight regarding thevalue of potential biomarkers and inform the development oftargeted therapies. Additionally, efforts to standardize a frame-work for data sharing are being explored, while support fromdata-driven and artificial-intelligence platforms is expected toshape the future of patient management. Overall, continuedprogress in the study and development of targeted therapiesand immunotherapies to treat cancer is anticipated. However,that success will depend on collaborative efforts to optimize theimplementation of precision oncology, a willingness to changemodels of clinical research to fit the new realities unveiled bygenomics, and establishment of a harmonized, innovativeapproach to patient care.
Disclosure of Potential Conflicts of InterestY.K. Chae is a consultant/advisory board member for Foundation Medicine,
Guardant Health, Biodesix, and Counsyl. R. Kurzrock has ownership interest inCureMatch, Inc., reports receiving a commercial research grant fromGenentech,Merck Serono, Pfizer, Sequenom, Foundation Medicine, and Guardant, hasownership interest (including patents) in Curematch, Inc., and is a consultant/advisory board member for Actuate Therapeutics, Xbiotech, and Roche. Nopotential conflicts of interest were disclosed.
Received July 3, 2017; revised August 4, 2017; accepted August 16, 2017;published online December 4, 2017.
References1. Westin JR, KurzrockR. It's about time: lessons for solid tumors fromchronic
myelogenous leukemia therapy. Mol Cancer Ther 2012;11:2549–55.2. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Cowey CL, Lao CD, et al.
Combined nivolumab and ipilimumab or monotherapy in untreatedmelanoma. N Engl J Med 2015;373:23–34.
3. Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, et al.Nivolumab versus docetaxel in advanced nonsquamous non-small-celllung cancer. N Engl J Med 2015;373:1627–39.
4. Carneiro BA, Costa R, Taxter T, Chandra S, Chae YK, Cristofanilli M, et al.Is personalized medicine here? Oncology (Williston Park) 2016;30:293–303, 307.
5. Hollingsworth SJ. Precision medicine in oncology drug development: apharma perspective. Drug Discov Today 2015;20:1455–63.
6. Heestand GM, Kurzrock R. Molecular landscape of pancreaticcancer: implications for current clinical trials. Oncotarget 2015;6:4553–61.
Path Toward Precision Oncology
www.aacrjournals.org Mol Cancer Ther; 16(12) December 2017 2653
on September 20, 2020. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

7. Tran B, Dancey JE, Kamel-Reid S, McPherson JD, Bedard PL, Brown AM,et al. Cancer genomics: technology, discovery, and translation. J ClinOncol2012;30:647–60.
8. Friedman AA, Letai A, Fisher DE, Flaherty KT. Precisionmedicine for cancerwith next-generation functional diagnostics. Nat Rev Cancer 2015;15:747–56.
9. Blumenthal GM, Mansfield E, Pazdur R. Next-generation sequencing inoncology in the era of precision medicine. JAMA Oncol 2016;2:13–4.
10. Siu LL, Conley BA, Boerner S, LoRusso PM. Next-generation sequencing toguide clinical trials. Clin Cancer Res 2015;21:4536–44.
11. Biankin AV, Piantadosi S, Hollingsworth SJ. Patient-centric trials fortherapeutic development in precision oncology. Nature 2015;526:361–70.
12. VonHoff DD, Stephenson JJ Jr, Rosen P, Loesch DM, BoradMJ, Anthony S,et al. Pilot study using molecular profiling of patients' tumors to findpotential targets and select treatments for their refractory cancers. J ClinOncol 2010;28:4877–83.
13. Tsimberidou AM, Iskander NG, Hong DS, Wheler JJ, Falchook GS, Fu S,et al. Personalized medicine in a phase I clinical trials program: the MDAnderson Cancer Center initiative. Clin Cancer Res 2012;18:6373–83.
14. Wheler JJ, Janku F, Naing A, Li Y, Stephen B, Zinner R, et al. Cancer therapydirected by comprehensive genomic profiling: a single center study. CancerRes 2016;76:3690–701.
15. Kummar S, Williams PM, Lih CJ, Polley EC, Chen AP, Rubinstein LV, et al.Application of molecular profiling in clinical trials for advancedmetastaticcancers. J Natl Cancer Inst 2015;107. pii: djv003.
16. Schmidt KT, Chau CH, Price DK, Figg WD. Precision oncology medicine:the clinical relevance of patient specific biomarkers used to optimize cancertreatment. J Clin Pharmacol 2016;56:1484–99.
17. Schwaederle M, Parker BA, Schwab RB, Daniels GA, Piccioni DE, Kesari S,et al. Precision Oncology: The UC San Diego Moores Cancer CenterPREDICT Experience. Mol Cancer Ther 2016;15:743–52.
18. Le Tourneau C, Delord JP, Goncalves A, Gavoille C, Dubot C, Isambert N,et al. Molecularly targeted therapy based on tumour molecular profilingversus conventional therapy for advanced cancer (SHIVA): a multicentre,open-label, proof-of-concept, randomised, controlled phase 2 trial. LancetOncol 2015;16:1324–34.
19. Saad ED, Paoletti X, Burzykowski T, Buyse M. Precision medicine needsrandomized clinical trials. Nat Rev Clin Oncol 2017;14:317–23.
20. TsimberidouAM, Kurzrock R. Precisionmedicine: lessons learned from theSHIVA trial. Lancet Oncol 2015;16:e579–80.
21. National Cancer Institute. NCI-Molecular Analysis for Therapy Choice(NCI-MATCH) Trial 2016 [Available from: http://www.cancer.gov/about-cancer/treatment/clinical-trials/nci-supported/nci-match.
22. Novartis Pharmaceuticals Corporation. Signature: Bring the Protocol to thePatient 2016 [Available from: http://www.trials.novartis.com/en/clinical-trials/us-oncology/oncology/signature/.
23. ClinicalTrials.gov. A Study Evaluating Herceptin/Perjeta, Tarceva, Zel-boraf/Cotellic, and Erivedge Treatment Targeted Against CertainMutationsin Cancer Patients [Available from: https://clinicaltrials.gov/ct2/show/NCT02091141.
24. American Society of Clinical Oncology. Targeted Agent and ProfilingUtilization Registry Study 2016 [Available from: http://www.tapur.org.
25. ClinicalTrials.gov. NCI-MATCH: Targeted TherapyDirected byGenetic Test-ing in Treating Patients With Advanced Refractory Solid Tumors or Lym-phomas [Available from:https://clinicaltrials.gov/ct2/show/NCT02465060.
26. Conley BA, Doroshow JH. Molecular analysis for therapy choice: NCIMATCH. Semin Oncol 2014;41:297–9.
27. Kang BP, Slosberg E, Snodgrass S, Lebedinsky C, Berry DA, Corless CL, et al.The signature program: bringing the protocol to the patient. Clin Pharma-col Ther 2015;98:124–6.
28. Peguero JA, O'Neil BH, Sohal D, Bauer TM, Subbiah V, Kelly K, et al.Genomicmutation profiling (GMP) and clinical outcome in patients (pts)treated with ribociclib (CDK4/6 inhibitor) in the Signature program.Presented at the ASCO Meeting 2016 Chicago, IL Abstract 25282016.
29. Peguero JA, Knost JA, Bauer TM, Taylor M, Braiteh FS, Eder JP, et al.Successful implementation of a novel trial model: The Signature program.Presented at the ASCO Meeting 2015 Chicago, IL Abstract 106. 2015.
30. Burris HA,HurwitzH, Perez EA, Spigel D, Swanton C,Hainsworth JD, et al.MyPathway: An open-label phase IIa study of trastuzumab/pertuzumab,erlotinib, vemurafenib, and vismodegib in patients who have advancedsolid tumors with mutations or gene expression abnormalities targeted by
these agents. Presented at the ASCO Meeting 2015 Chicago, IL AbstractTPS11111. 2015.
31. Hainsworth JD, Meric-Bernstam F, Swanton C, Hurwitz H, Spigel DR,Sweeney C, et al. Targeted therapy for advanced solid tumors based onmolecular profiles: Early results fromMyPathway, an open-label, phase IIaumbrella basket study. Presented at the ASCO Meeting 2016 Chicago, ILAbstract LBA11511. 2016.
32. Hurwitz H, Raghav KPS, Burris HA, Kurzrock R, Sweeney C, Meric-Bern-stam F, et al. Pertuzumab þ trastuzumab for HER2-amplified/overex-pressed metastatic colorectal cancer (mCRC): Interim data from MyPath-way. Presented at the 2017 Gastrointestinal Cancers Symposium SanFrancisco, CA Abstract 676. 2017.
33. BryceAH, Kurzrock R,Meric-BernstamF,HurwitzH,Hainsworth JD, SpigelDR, et al. Pertuzumab plus trastuzumab for HER2-positive metastaticurothelial cancer (mUC): Preliminary data from MyPathway. Presentedat the 2017 Genitourinary Cancers Symposium Orlando, FL Abstract 348.2017.
34. Javle MM, Hainsworth JD, Swanton C, Burris HA, Kurzrock R, Sweeney C,et al. Pertuzumab þ trastuzumab for HER2-positive metastatic biliarycancer: Preliminary data from MyPathway. Presented at the 2017 Gastro-intestinal Cancers Symposium San Francisco, CA Abstract 402. 2017.
35. ClinicalTrials.gov. TAPUR: Testing the Use of Food and Drug Administra-tion (FDA) Approved Drugs that Target a Specific Abnormality in a TumorGene in People with Advanced Stage Cancer (TAPUR) [Available from:https://clinicaltrials.gov/ct2/show/NCT02693535.
36. Meric-Bernstam F, Johnson A, Holla V, Bailey AM, Brusco L, Chen K, et al. Adecision support framework for genomically informed investigationalcancer therapy. J Natl Cancer Inst 2015;107. pii: djv098.
37. Conley BA. Genomically guided cancer treatments: from "promising" to"clinically useful". J Natl Cancer Inst 2015;107. pii: djv168.
38. Easton DF, Pharoah PD, Antoniou AC, Tischkowitz M, Tavtigian SV,Nathanson KL, et al. Gene-panel sequencing and the prediction ofbreast-cancer risk. N Engl J Med 2015;372:2243–57.
39. Phimister EG. Curating the way to better determinants of genetic risk.N Engl J Med 2015;372:2227–8.
40. Foulkes WD. Inherited susceptibility to common cancers. N Engl J Med2008;359:2143–53.
41. Van Allen EM,Wagle N, Stojanov P, Perrin DL, Cibulskis K, Marlow S, et al.Whole-exome sequencing and clinical interpretation of formalin-fixed,paraffin-embedded tumor samples to guide precision cancermedicine.NatMed 2014;20:682–8.
42. Vidwans SJ, TurskiML, Janku F, Garrido-Laguna I,Munoz J, Schwab R, et al.A framework for genomic biomarker actionability and its use in clinicaldecision making. Oncoscience 2014;1:614–23.
43. Sukhai MA, Craddock KJ, Thomas M, Hansen AR, Zhang T, Siu L, et al.A classification system for clinical relevance of somatic variants identifiedin molecular profiling of cancer. Genet Med 2016;18:128–36.
44. Carr TH,McEwen R, Dougherty B, Johnson JH, Dry JR, Lai Z, et al. Definingactionable mutations for oncology therapeutic development. Nat RevCancer 2016;16:319–29.
45. Gauthier NP, Reznik E, Gao J, Sumer SO, Schultz N, Sander C, et al.MutationAligner: a resource of recurrent mutation hotspots in proteindomains in cancer. Nucleic Acids Res 2016;44(D1):D986–91.
46. Frousios K, Iliopoulos CS, Schlitt T, SimpsonMA. Predicting the functionalconsequences of non-synonymous DNA sequence variants–evaluation ofbioinformatics tools and development of a consensus strategy. Genomics2013;102:223–8.
47. Bailey AM, Mao Y, Zeng J, Holla V, Johnson A, Brusco L, et al. Implemen-tation of biomarker-driven cancer therapy: existing tools and remaininggaps. Discov Med 2014;17:101–14.
48. Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P, Larkin J, et al.Improved survival with vemurafenib in melanoma with BRAF V600Emutation. N Engl J Med 2011;364:2507–16.
49. Hauschild A, Grob JJ, Demidov LV, Jouary T, Gutzmer R, MillwardM, et al.Dabrafenib in BRAF-mutated metastatic melanoma: a multicentre, open-label, phase 3 randomised controlled trial. Lancet 2012;380:358–65.
50. Flaherty KT, Robert C, Hersey P, Nathan P, Garbe C, Milhem M, et al.Improved survival with MEK inhibition in BRAF-mutated melanoma.N Engl J Med 2012;367:107–14.
51. Yeh P, Chen H, Andrews J, Naser R, Pao W, Horn L. DNA-MutationInventory to Refine and Enhance Cancer Treatment (DIRECT): a catalog
Mol Cancer Ther; 16(12) December 2017 Molecular Cancer Therapeutics2654
Chae et al.
on September 20, 2020. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

of clinically relevant cancer mutations to enable genome-directed antican-cer therapy. Clin Cancer Res 2013;19:1894–901.
52. American Association for Cancer Research. AACR Project GENIE 2016[Available from: http://aacr.org/genie.
53. Syapse. Oncology Precision Network [Available from: http://syapse.com/oncology-precision-network/.
54. Robert H. Lurie Comprehensive Cancer Center. OncoSET (Sequence, Eval-uate, Treat) 2015 [Available from: http://cancer.northwestern.edu/oncoset/.
55. Schwaederle M, Parker BA, Schwab RB, Fanta PT, Boles SG, Daniels GA,et al. Molecular tumor board: the University of California-San\sDiegoMoores Cancer Center experience. Oncologist 2014;19:631–6.
56. Parker BA, Schwaederle M, Scur MD, Boles SG, Helsten T, Subramanian R,et al. Breast cancer experience of the molecular tumor board at theUniversity of California, San Diego Moores Cancer Center. J Oncol Pract2015;11:442–9.
57. Walko C, Kiel PJ, Kolesar J. Precision medicine in oncology: New practicemodels and roles for oncology pharmacists. Am J Health Syst Pharm2016;73:1935–42.
58. Radovich M, Kiel PJ, Nance SM, Niland EE, Parsley ME, FergusonME, et al.Clinical benefit of a precision medicine based approach for guidingtreatment of refractory cancers. Oncotarget 2016;7:56491–500.
59. Johnson A, Zeng J, Bailey AM,Holla V, Litzenburger B, Lara-Guerra H, et al.The right drugs at the right time for the right patient: the MD Andersonprecision oncology decision support platform. Drug Discov Today2015;20:1433–8.
60. IBM Watson Health. IBM Watson for Genomics [Available from: http://www.ibm.com/watson/health/oncology/genomics/.
61. IBM Think. As Seen On 60 Minutes: Watson Accelerates PrecisionOncology [Available from: http://www.ibm.com/blogs/think/2016/10/09/sharpless/.
62. TurskiML, Vidwans SJ, Janku F, Garrido-Laguna I,Munoz J, SchwabR, et al.Genomically driven tumors and actionability across histologies: BRAF-mutant cancers as a paradigm. Mol Cancer Ther 2016;15:533–47.
63. McLaren W, Gil L, Hunt SE, Riat HS, Ritchie GR, Thormann A, et al. Theensembl variant effect predictor. Genome Biol 2016;17:122.
64. Sim NL, Kumar P, Hu J, Henikoff S, Schneider G, Ng PC. SIFT web server:predicting effects of amino acid substitutions on proteins. Nucleic AcidsRes 2012;40(Web Server issue):W452–7.
65. Adzhubei IA, Schmidt S, Peshkin L, Ramensky VE, Gerasimova A, Bork P,et al. A method and server for predicting damaging missense mutations.Nat Methods 2010;7:248–9.
66. Reva B, Antipin Y, Sander C. Predicting the functional impact of proteinmutations: application to cancer genomics. Nucleic Acids Res 2011;39:e118.
67. Gonzalez-Perez A, Lopez-Bigas N. Improving the assessment of the out-come of nonsynonymous SNVs with a consensus deleteriousness score,Condel. Am J Hum Genet 2011;88:440–9.
68. Carter H, Chen S, Isik L, Tyekucheva S, Velculescu VE, Kinzler KW, et al.Cancer-specific high-throughput annotation of somatic mutations:computational prediction of driver missense mutations. Cancer Res2009;69:6660–7.
69. Mao Y, Chen H, Liang H, Meric-Bernstam F, Mills GB, Chen K. CanDrA:cancer-specific driver missense mutation annotation with optimized fea-tures. PLoS One 2013;8:e77945.
70. Li B, Krishnan VG, Mort ME, Xin F, Kamati KK, Cooper DN, et al.Automated inference of molecular mechanisms of disease from aminoacid substitutions. Bioinformatics 2009;25:2744–50.
71. Calabrese R, Capriotti E, Fariselli P, Martelli PL, Casadio R. Functionalannotations improve the predictive score of human disease-related muta-tions in proteins. Hum Mutat 2009;30:1237–44.
72. Mi H, Poudel S, Muruganujan A, Casagrande JT, Thomas PD. PANTHERversion 10: expanded protein families and functions, and analysis tools.Nucleic Acids Res 2016;44(D1):D336–42.
73. Capriotti E, Calabrese R, Casadio R. Predicting the insurgence of humangenetic diseases associated to single point protein mutations with supportvector machines and evolutionary information. Bioinformatics 2006;22:2729–34.
74. Lopes MC, Joyce C, Ritchie GR, John SL, Cunningham F, Asimit J, et al. Acombined functional annotation score for non-synonymous variants.Hum Hered 2012;73:47–51.
www.aacrjournals.org Mol Cancer Ther; 16(12) December 2017 2655
Path Toward Precision Oncology
on September 20, 2020. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from

2017;16:2645-2655. Mol Cancer Ther Young Kwang Chae, Alan P. Pan, Andrew A. Davis, et al. Lesion and Patient Management SupportStudies and Tools to Aid in Defining ''Actionability'' of a Molecular Path toward Precision Oncology: Review of Targeted Therapy
Updated version
http://mct.aacrjournals.org/content/16/12/2645
Access the most recent version of this article at:
Cited articles
http://mct.aacrjournals.org/content/16/12/2645.full#ref-list-1
This article cites 53 articles, 13 of which you can access for free at:
Citing articles
http://mct.aacrjournals.org/content/16/12/2645.full#related-urls
This article has been cited by 3 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mct.aacrjournals.org/content/16/12/2645To request permission to re-use all or part of this article, use this link
on September 20, 2020. © 2017 American Association for Cancer Research. mct.aacrjournals.org Downloaded from