Embed Size (px)
Citation preview

PASSIVE SMOKING AND BREAST CANCER RISK AMONG NON-SMOKINGCHINESE WOMENMartha J. SHRUBSOLE
1, Yu-Tang GAO2, Qi DAI
1, Xiao-Ou SHU1, Zi-Xian RUAN
2, Fan JIN2 and Wei ZHENG
1*1Department of Internal Medicine and Vanderbilt-Ingram Cancer Center, Vanderbilt University, Nashville, TN, USA2Shanghai Cancer Institute, Shanghai, People’s Republic of China
Our purpose was to evaluate whether passive exposure tocigarette smoke may be related to breast cancer risk. Datafrom the Shanghai Breast Cancer Study, a large population-based study of 1,459 breast cancer cases and 1,556 controlsaged 25–64 years, were analyzed. Respective response rateswere 91.1% and 90.3%. Passive smoking questions were addedto all face-to-face interviews 7 months into the study.Women were asked about exposure to their husbands’smoke at home as well as exposure in the workplace. Anal-yses were restricted to the 1,013 cases and 1,117 controlswith passive tobacco smoke exposure data who had neveractively smoked. Over 60% of controls reported some expo-sure to a husband’s smoke and over 40% reported exposureto passive smoke in the workplace. Overall, there was noapparent association between any passive smoke exposure orexposure to a husband’s smoke and breast cancer risk. Therewas some evidence of an elevated breast cancer risk associ-ated with passive smoking exposure of 5 hr or more per dayin the workplace (OR � 1.6, 95% confidence interval 1.0–2.4;p for trend � 0.02). This association warrants further inves-tigation.© 2004 Wiley-Liss, Inc.
Key words: breast cancer; passive smoking; epidemiology; tobacco
Tobacco smoking has been established as the major risk factorfor a number of cancers in humans, including cancers of the lung,oral cavity, esophagus, larynx and bladder.1 The association ofcigarette smoking and breast cancer has been less well understood.Despite a large body of epidemiologic literature on active smokingand breast cancer and several plausible mechanisms, results havebeen inconsistent and mostly null.2,3 One explanation given forthese inconsistent results is that the referent group of nonsmokingwomen in most of the previous studies may have included asubstantial number who were exposed to environmental or passivesmoke.3 Several epidemiologic studies have evaluated the associ-ation between passive smoking and breast cancer.4–15 Many ofthese studies had small sample sizes, particularly in the exposuregroups. As with the active smoking literature, the results fromthese studies have been mostly null, though a positive associationfor at least one measure has been reported in some studies.3
To investigate the association of passive cigarette smoking andbreast cancer risk, we analyzed data from the large population-based Shanghai Breast Cancer Study (SBCS). The vast majority ofChinese women in Shanghai have never smoked cigarettes, whilethe smoking prevalence is high among adult men, most of whomsmoke at home.16 Smoking is also not restricted in public places,including work settings. This exposure pattern provides a uniqueopportunity to vigorously investigate the hypothesis related topassive smoking.
MATERIAL AND METHODS
Subject selectionThe SBCS was a large population-based case-control study
conducted in Shanghai from August 1996 to March 1998. Allsubjects were permanent residents of urban Shanghai who had noprior history of cancer and were alive at the time of interview.Cases were between the ages of 25 and 64 and identified througha rapid case-ascertainment system supplemented by the popula-tion-based Shanghai Cancer Registry. A total of 1,602 eligiblebreast cancer cases were identified, and in-person interviews were
completed for 1,459 (91.1%) of them. Controls were randomlyselected from female permanent residents in urban Shanghai andfrequency-matched to cases by age (5-year interval) according tothe age distribution of the incident breast cancer cases reported tothe Shanghai Cancer Registry during 1990–1993. The ShanghaiResident Registry, which keeps registry cards for all permanentresidents in urban Shanghai, was used to randomly select controls.For each age-predetermined case, a registry card identifying apotential control in the same 5-year age group was randomlyselected. Only women who lived at the registered address duringthe study period were considered eligible for the study. In-personinterviews were completed for 1,556 (90.3%) of the 1,724 eligiblecontrols
Data collectionAll subjects were interviewed in person by trained interviewers
using a structured questionnaire, which included information ondemography, menstrual and reproductive history, diet, diseasehistory, weight, physical activity and family history of cancer.Questions about passive smoking exposure were added to allin-person interviews after March 1997, 7 months after the com-mencement of the study. Passive smoking data were obtained from1,119 cases (71.9%) and 1,231 controls (71.4%). Passive smokinghistory was collected for 2 exposure sources. First, the subject wasasked whether her husband had ever smoked at home and abouther lifetime exposure to her husband’s smoke by stating thenumber of cigarettes he smoked per day at home and the numberof years she had been exposed to this smoke. Second, the subjectwas asked about the hours she was exposed to the smoke of otherpeople in her workplace(s) over the past 5 years. Subjects werecategorized as exposed to passive smoke if they reported everbeing exposed to smoke from their husbands or in the workplace.
Data analysis and statistical methodsOf the 2,350 subjects who completed the passive smoking
questionnaire, 57 (25 cases, 32 controls) reported a past or currenthistory of personal cigarette smoking. These women were ex-cluded from analyses. Also excluded from analyses were womenwho were not currently married (81 cases, 82 controls). Womenwho had never worked during the 5 years prior to interview wereexcluded from all analyses involving workplace exposure (149cases, 181 controls). Odds ratios (ORs) were used to measure theassociation of breast cancer risk with passive cigarette smoking.Unconditional logistic regression models were used to obtainmaximum likelihood estimates of ORs and their 95% confidence
Grant sponsor: National Cancer Institute; Grant number: RO1CA64277.
*Correspondence to: 6103 Medical Center East, Vanderbilt UniversityMedical Center, Nashville, TN 37232-8300, USA. Fax: �615-936-1269.E-mail: [email protected]
Received 13 June 2003; Revised 29 December 2003; Accepted 22January 2004
DOI 10.1002/ijc.20168Publishedonline15March2004 inWiley InterScience (www.interscience.
wiley.com).
Int. J. Cancer: 110, 605–609 (2004)© 2004 Wiley-Liss, Inc.
Publication of the International Union Against Cancer

intervals (CIs) after adjusting for potential confounders. Risk fac-tors identified previously as having an independent associationwith breast cancer in this population were controlled in all models.These included breast cancer in a first-degree relative, history offibroadenoma, age at menarche, age at first live birth, age atmenopause, body mass index (BMI), physical activity and meno-pausal status. Models also controlled for age, education and house-hold income. Age was included as a continuous variable through-out data analyses, and categorical variables were treated asindicator variables in the model. Tests for trend were performed byentering categorical variables as continuous parameters in themodels. All statistical tests were based on 2-sided probabilitiesusing SAS version 8.2 (SAS Institute, Cary, NC).
RESULTS
A comparison of cases and controls on demographic and estab-lished breast cancer risk factors is presented in Table I. Cases wereslightly older than controls and of somewhat higher educationalattainment. Cases were more likely to have a family history ofbreast cancer, a personal history of breast fibroadenoma, a largerBMI, an earlier age at menarche and a later age at menopause.Cases were less likely to be physically active. The distribution ofthese demographic and risk factors and their association withbreast cancer risk observed in subjects included in the presentanalysis were virtually identical to those found in all participantsof the SBCS.17
The case-control distribution and ORs for passive smoke expo-sure sources are shown in Table II for all subjects, stratified bymenopausal status. Of all subjects, 59.6% of cases and 62.6% ofcontrols reported ever having been exposed to their husbands’cigarette smoke, with an adjusted OR of 1.0 (95% CI 0.8–1.2).There was also no association of husband’s smoke and breastcancer risk observed among pre- and postmenopausal women.Among women who had worked in the past 5 years, 52.9% ofcases and 49.5% of controls reported ever having been exposed topassive smoke in the workplace, with an adjusted OR of 1.1 (95%CI 0.9–1.4). Similar results were observed when analyses were
stratified by menopausal status. When subjects were categorizedaccording to source(s) of passive smoke exposure, 16.9% of con-trols were exposed only in the workplace, 30.9% of controls wereexposed only to a husband’s smoke and 32.6% reported bothexposures. The association of breast cancer risk with passivesmoke exposure was examined. No association was observedeither in the total sample or by menopausal status.
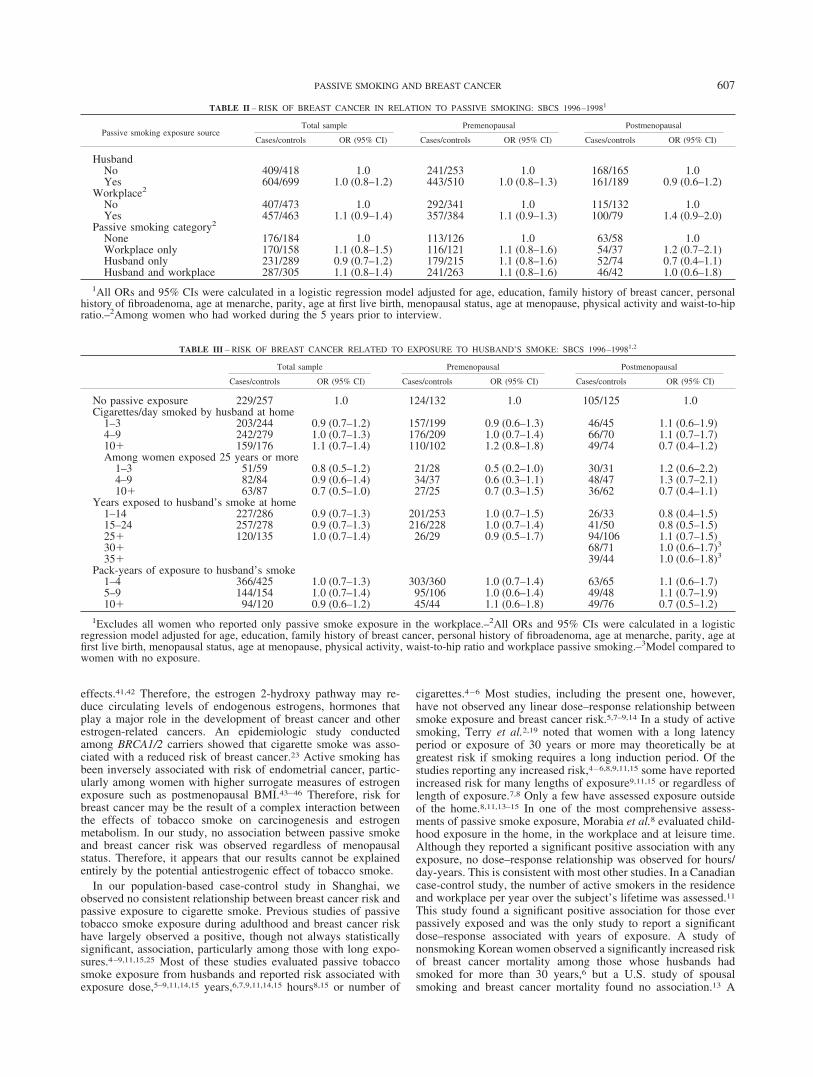
Exposure to a husband’s cigarette smoke is examined in detail inTable III. Women who reported being exposed to passive smokeonly at work were excluded from analyses. Results are presentedfor the total sample and stratified by menopausal status. Therewere no significant or consistent differences in ORs by the amountor duration of exposure either in the total sample or within meno-pausal status. To examine intensity of exposure among womenwith long-term exposure, analyses are presented for women ex-posed for �25 years compared to women with no exposure. Again,no significant association was observed.
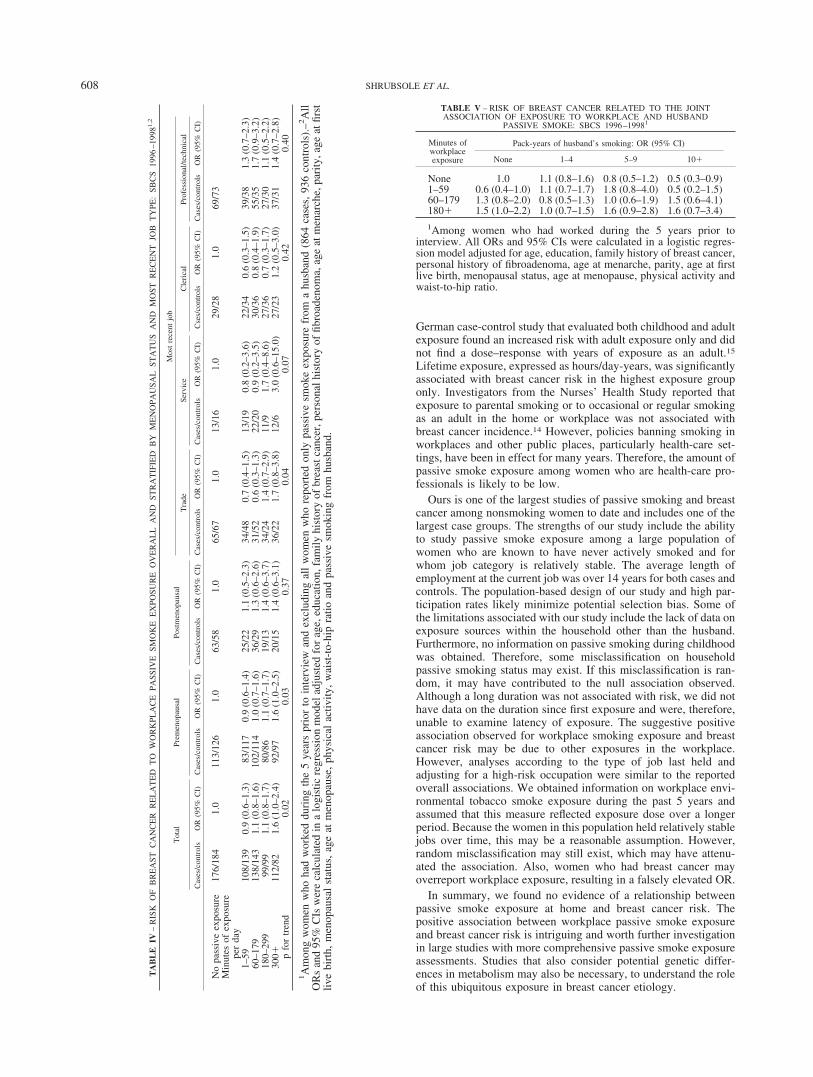
As shown in Table IV, there was some evidence of a slightlyelevated breast cancer risk associated with passive workplaceexposure of 5 hr or more per day (OR � 1.6, 95% CI 1.0–2.4; pfor trend � 0.02) among women who worked during the 5 yearsprior to interview. A similar association was observed amongpremenopausal women, but no significant association was ob-served for postmenopausal women. Women who had not workedin the 5 years prior to interview were excluded from all analysesand were mostly older (median age 59 years) and postmenopausal(�75%). Results are also presented for stratified analyses byoccupation. The association was strongest among those with atrade or service job.
Presented in Table V is the joint association of passive smokeexposure in the workplace and from a husband. Women who hadnot worked in the 5 years prior to interview were excluded fromanalysis. There is some suggestion that workplace passive smokeexposure of 3 hr or more is associated with an increased risk forbreast cancer. However, no clear or consistent relationships wereobserved.
DISCUSSION
There have been numerous epidemiologic studies of activesmoking, the most concentrated form of tobacco smoke exposure,and breast cancer risk; results are inconsistent.2,3,15 Some studieshave suggested an increased risk of breast cancer, particularlyamong heavy smokers and those who started at an early age or hada long latent exposure.14,18–21 Other studies have suggested thatcigarette smoking is associated with a decreased risk, particularlyamong those at high risk for breast cancer.22,23 Still other studieshave observed no association between active smoking and breastcancer risk.24,25 The results from passive smoking studies areequally inconsistent. Several known or probable human carcino-gens are present in cigarette smoke, including polycyclic aromatichydrocarbons (PAHs), nitrosamines, heterocyclic amines, aromaticamines and benzene.26 Some of these compounds are mammarycarcinogens in animal models.27 PAH-DNA adducts have beendetected in human breast epithelial cells, and levels of theseadducts in breast tissue have been higher in breast cancer casesthan controls in some epidemiologic studies.28–31 However, itappears that the PAH-DNA adduct level was not always associatedwith smoking status.30 It has been hypothesized that susceptibilityto breast cancer from cigarette smoke may be determined bygenetic differences, e.g., in metabolic genes. However, resultsfrom studies examining some of these polymorphic genes havealso been conflicting.20,32–37 One hypothesis for the inconsistencybetween smoking and breast cancer is the potential antiestrogenicproperties of tobacco smoke.22 Certain compounds identified intobacco smoke, such as PAH, induce the activity of cytochromeP-450-1A2 and other estrogen 2-hydroxylases.38–40 Many in vitroexperiments have shown that 2-hydroxy estrogen metabolites haveno estrogenic effect and even may have certain cancer-inhibitory
TABLE I – COMPARISONS OF CASES AND CONTROLS BY MAJOR BREASTCANCER RISK FACTORS: SBCS 1996–19981
Demographic characteristics Cases(n � 1,013)
Controls(n � 1,117)
Age years, (mean � SD) 47.9 � 8.0 47.2 � 8.8Education (%)
Never 2.3 3.8Elementary 7.1 7.6Middle � high school 76.8 78.0Professional � college 13.9 10.7
Most recent occupation (%)2
Trade worker 35.8 36.8Service worker 11.5 11.7Clerical worker 21.2 21.9Professional and technical 31.6 29.7
Established risk factorsFamily history of breast cancer (%) 4.0 2.0History of fibroadenoma (%) 10.3 5.4Physically active past 10 years (%) 17.3 21.8BMI (kg/m2, mean � SD) 23.5 � 3.4 23.1 � 3.3Age at menarche (years,
mean � SD)14.4 � 1.5 14.6 � 1.7
Age at first live birth(mean � SD)3
27.0 � 4.0 26.5 � 3.7
Number of live births(mean � SD)
1.4 � 0.8 1.4 � 0.8
Age at menopause(years, mean � SD)4
47.8 � 4.6 47.4 � 4.8
1Includes married women with interview data on passive smokingwho had never actively smoked.–2Among women who had workedduring the 5 years prior to interview (864 cases, 936 controls).–3Among women who had live births.–4Among menopausal women.
606 SHRUBSOLE ET AL.
effects.41,42 Therefore, the estrogen 2-hydroxy pathway may re-duce circulating levels of endogenous estrogens, hormones thatplay a major role in the development of breast cancer and otherestrogen-related cancers. An epidemiologic study conductedamong BRCA1/2 carriers showed that cigarette smoke was asso-ciated with a reduced risk of breast cancer.23 Active smoking hasbeen inversely associated with risk of endometrial cancer, partic-ularly among women with higher surrogate measures of estrogenexposure such as postmenopausal BMI.43–46 Therefore, risk forbreast cancer may be the result of a complex interaction betweenthe effects of tobacco smoke on carcinogenesis and estrogenmetabolism. In our study, no association between passive smokeand breast cancer risk was observed regardless of menopausalstatus. Therefore, it appears that our results cannot be explainedentirely by the potential antiestrogenic effect of tobacco smoke.
In our population-based case-control study in Shanghai, weobserved no consistent relationship between breast cancer risk andpassive exposure to cigarette smoke. Previous studies of passivetobacco smoke exposure during adulthood and breast cancer riskhave largely observed a positive, though not always statisticallysignificant, association, particularly among those with long expo-sures.4–9,11,15,25 Most of these studies evaluated passive tobaccosmoke exposure from husbands and reported risk associated withexposure dose,5–9,11,14,15 years,6,7,9,11,14,15 hours8,15 or number of
cigarettes.4–6 Most studies, including the present one, however,have not observed any linear dose–response relationship betweensmoke exposure and breast cancer risk.5,7–9,14 In a study of activesmoking, Terry et al.2,19 noted that women with a long latencyperiod or exposure of 30 years or more may theoretically be atgreatest risk if smoking requires a long induction period. Of thestudies reporting any increased risk,4–6,8,9,11,15 some have reportedincreased risk for many lengths of exposure9,11,15 or regardless oflength of exposure.7,8 Only a few have assessed exposure outsideof the home.8,11,13–15 In one of the most comprehensive assess-ments of passive smoke exposure, Morabia et al.8 evaluated child-hood exposure in the home, in the workplace and at leisure time.Although they reported a significant positive association with anyexposure, no dose–response relationship was observed for hours/day-years. This is consistent with most other studies. In a Canadiancase-control study, the number of active smokers in the residenceand workplace per year over the subject’s lifetime was assessed.11
This study found a significant positive association for those everpassively exposed and was the only study to report a significantdose–response associated with years of exposure. A study ofnonsmoking Korean women observed a significantly increased riskof breast cancer mortality among those whose husbands hadsmoked for more than 30 years,6 but a U.S. study of spousalsmoking and breast cancer mortality found no association.13 A
TABLE II – RISK OF BREAST CANCER IN RELATION TO PASSIVE SMOKING: SBCS 1996–19981
Passive smoking exposure sourceTotal sample Premenopausal Postmenopausal
Cases/controls OR (95% CI) Cases/controls OR (95% CI) Cases/controls OR (95% CI)
HusbandNo 409/418 1.0 241/253 1.0 168/165 1.0Yes 604/699 1.0 (0.8–1.2) 443/510 1.0 (0.8–1.3) 161/189 0.9 (0.6–1.2)
Workplace2
No 407/473 1.0 292/341 1.0 115/132 1.0Yes 457/463 1.1 (0.9–1.4) 357/384 1.1 (0.9–1.3) 100/79 1.4 (0.9–2.0)
Passive smoking category2
None 176/184 1.0 113/126 1.0 63/58 1.0Workplace only 170/158 1.1 (0.8–1.5) 116/121 1.1 (0.8–1.6) 54/37 1.2 (0.7–2.1)Husband only 231/289 0.9 (0.7–1.2) 179/215 1.1 (0.8–1.6) 52/74 0.7 (0.4–1.1)Husband and workplace 287/305 1.1 (0.8–1.4) 241/263 1.1 (0.8–1.6) 46/42 1.0 (0.6–1.8)
1All ORs and 95% CIs were calculated in a logistic regression model adjusted for age, education, family history of breast cancer, personalhistory of fibroadenoma, age at menarche, parity, age at first live birth, menopausal status, age at menopause, physical activity and waist-to-hipratio.–2Among women who had worked during the 5 years prior to interview.
TABLE III – RISK OF BREAST CANCER RELATED TO EXPOSURE TO HUSBAND’S SMOKE: SBCS 1996–19981,2
Total sample Premenopausal Postmenopausal
Cases/controls OR (95% CI) Cases/controls OR (95% CI) Cases/controls OR (95% CI)
No passive exposure 229/257 1.0 124/132 1.0 105/125 1.0Cigarettes/day smoked by husband at home
1–3 203/244 0.9 (0.7–1.2) 157/199 0.9 (0.6–1.3) 46/45 1.1 (0.6–1.9)4–9 242/279 1.0 (0.7–1.3) 176/209 1.0 (0.7–1.4) 66/70 1.1 (0.7–1.7)10� 159/176 1.1 (0.7–1.4) 110/102 1.2 (0.8–1.8) 49/74 0.7 (0.4–1.2)Among women exposed 25 years or more
1–3 51/59 0.8 (0.5–1.2) 21/28 0.5 (0.2–1.0) 30/31 1.2 (0.6–2.2)4–9 82/84 0.9 (0.6–1.4) 34/37 0.6 (0.3–1.1) 48/47 1.3 (0.7–2.1)10� 63/87 0.7 (0.5–1.0) 27/25 0.7 (0.3–1.5) 36/62 0.7 (0.4–1.1)
Years exposed to husband’s smoke at home1–14 227/286 0.9 (0.7–1.3) 201/253 1.0 (0.7–1.5) 26/33 0.8 (0.4–1.5)15–24 257/278 0.9 (0.7–1.3) 216/228 1.0 (0.7–1.4) 41/50 0.8 (0.5–1.5)25� 120/135 1.0 (0.7–1.4) 26/29 0.9 (0.5–1.7) 94/106 1.1 (0.7–1.5)30� 68/71 1.0 (0.6–1.7)3
35� 39/44 1.0 (0.6–1.8)3
Pack-years of exposure to husband’s smoke1–4 366/425 1.0 (0.7–1.3) 303/360 1.0 (0.7–1.4) 63/65 1.1 (0.6–1.7)5–9 144/154 1.0 (0.7–1.4) 95/106 1.0 (0.6–1.4) 49/48 1.1 (0.7–1.9)10� 94/120 0.9 (0.6–1.2) 45/44 1.1 (0.6–1.8) 49/76 0.7 (0.5–1.2)
1Excludes all women who reported only passive smoke exposure in the workplace.–2All ORs and 95% CIs were calculated in a logisticregression model adjusted for age, education, family history of breast cancer, personal history of fibroadenoma, age at menarche, parity, age atfirst live birth, menopausal status, age at menopause, physical activity, waist-to-hip ratio and workplace passive smoking.–3Model compared towomen with no exposure.
607PASSIVE SMOKING AND BREAST CANCER
German case-control study that evaluated both childhood and adultexposure found an increased risk with adult exposure only and didnot find a dose–response with years of exposure as an adult.15
Lifetime exposure, expressed as hours/day-years, was significantlyassociated with breast cancer risk in the highest exposure grouponly. Investigators from the Nurses’ Health Study reported thatexposure to parental smoking or to occasional or regular smokingas an adult in the home or workplace was not associated withbreast cancer incidence.14 However, policies banning smoking inworkplaces and other public places, particularly health-care set-tings, have been in effect for many years. Therefore, the amount ofpassive smoke exposure among women who are health-care pro-fessionals is likely to be low.
Ours is one of the largest studies of passive smoking and breastcancer among nonsmoking women to date and includes one of thelargest case groups. The strengths of our study include the abilityto study passive smoke exposure among a large population ofwomen who are known to have never actively smoked and forwhom job category is relatively stable. The average length ofemployment at the current job was over 14 years for both cases andcontrols. The population-based design of our study and high par-ticipation rates likely minimize potential selection bias. Some ofthe limitations associated with our study include the lack of data onexposure sources within the household other than the husband.Furthermore, no information on passive smoking during childhoodwas obtained. Therefore, some misclassification on householdpassive smoking status may exist. If this misclassification is ran-dom, it may have contributed to the null association observed.Although a long duration was not associated with risk, we did nothave data on the duration since first exposure and were, therefore,unable to examine latency of exposure. The suggestive positiveassociation observed for workplace smoking exposure and breastcancer risk may be due to other exposures in the workplace.However, analyses according to the type of job last held andadjusting for a high-risk occupation were similar to the reportedoverall associations. We obtained information on workplace envi-ronmental tobacco smoke exposure during the past 5 years andassumed that this measure reflected exposure dose over a longerperiod. Because the women in this population held relatively stablejobs over time, this may be a reasonable assumption. However,random misclassification may still exist, which may have attenu-ated the association. Also, women who had breast cancer mayoverreport workplace exposure, resulting in a falsely elevated OR.
In summary, we found no evidence of a relationship betweenpassive smoke exposure at home and breast cancer risk. Thepositive association between workplace passive smoke exposureand breast cancer risk is intriguing and worth further investigationin large studies with more comprehensive passive smoke exposureassessments. Studies that also consider potential genetic differ-ences in metabolism may also be necessary, to understand the roleof this ubiquitous exposure in breast cancer etiology.
TABLE V – RISK OF BREAST CANCER RELATED TO THE JOINTASSOCIATION OF EXPOSURE TO WORKPLACE AND HUSBAND
PASSIVE SMOKE: SBCS 1996–19981
Minutes ofworkplaceexposure
Pack-years of husband’s smoking: OR (95% CI)
None 1–4 5–9 10�
None 1.0 1.1 (0.8–1.6) 0.8 (0.5–1.2) 0.5 (0.3–0.9)1–59 0.6 (0.4–1.0) 1.1 (0.7–1.7) 1.8 (0.8–4.0) 0.5 (0.2–1.5)60–179 1.3 (0.8–2.0) 0.8 (0.5–1.3) 1.0 (0.6–1.9) 1.5 (0.6–4.1)180� 1.5 (1.0–2.2) 1.0 (0.7–1.5) 1.6 (0.9–2.8) 1.6 (0.7–3.4)
1Among women who had worked during the 5 years prior tointerview. All ORs and 95% CIs were calculated in a logistic regres-sion model adjusted for age, education, family history of breast cancer,personal history of fibroadenoma, age at menarche, parity, age at firstlive birth, menopausal status, age at menopause, physical activity andwaist-to-hip ratio.
TA
BL
EIV
–R
ISK
OF
BR
EA
STC
AN
CE
RR
EL
AT
ED
TO
WO
RK
PLA
CE
PASS
IVE
SMO
KE
EX
POSU
RE
OV
ER
AL
LA
ND
STR
AT
IFIE
DB
YM
EN
OPA
USA
LST
AT
US
AN
DM
OST
RE
CE
NT
JOB
TY
PE:
SBC
S19
96–1
9981,
2
Tot
alPr
emen
opau
sal
Post
men
opau
sal
Mos
tre
cent
job
Tra
deSe
rvic
eC
leri
cal
Prof
essi
onal
/tech
nica
l
Cas
es/c
ontr
ols
OR
(95%
CI)
Cas
es/c
ontr
ols
OR
(95%
CI)
Cas
es/c
ontr
ols
OR
(95%
CI)
Cas
es/c
ontr
ols
OR
(95%
CI)
Cas
es/c
ontr
ols
OR
(95%
CI)
Cse
s/co
ntro
lsO
R(9
5%C
I)C
ases
/con
trol
sO
R(9
5%C
I)
No
pass
ive
expo
sure
176/
184
1.0
113/
126
1.0
63/5
81.
065
/67
1.0
13/1
61.
029
/28
1.0
69/7
3M
inut
esof
expo
sure
per
day
1–59
108/
139
0.9
(0.6
–1.3
)83
/117
0.9
(0.6
–1.4
)25
/22
1.1
(0.5
–2.3
)34
/48
0.7
(0.4
–1.5
)13
/19
0.8
(0.2
–3.6
)22
/34
0.6
(0.3
–1.5
)39
/38
1.3
(0.7
–2.3
)60
–179
138/
143
1.1
(0.8
–1.6
)10
2/11
41.
0(0
.7–1
.6)
36/2
91.
3(0
.6–2
.6)
31/5
20.
6(0
.3–1
.3)
22/2
00.
9(0
.2–3
.5)
30/3
60.
8(0
.4–1
.9)
55/3
51.
7(0
.9–3
.2)
180–
299
99/9
91.
1(0
.8–1
.7)
80/8
61.
1(0
.7–1
.7)
19/1
31.
4(0
.6–3
.7)
34/2
41.
4(0
.7–2
.9)
11/9
1.7
(0.4
–8.6
)27
/36
0.7
(0.3
–1.7
)27
/30
1.1
(0.5
–2.2
)30
0�11
2/82
1.6
(1.0
–2.4
)92
/97
1.6
(1.0
–2.5
)20
/15
1.4
(0.6
–3.1
)36
/22
1.7
(0.8
–3.8
)12
/63.
0(0
.6–1
5.0)
27/2
31.
2(0
.5–3
.0)
37/3
11.
4(0
.7–2
.8)
pfo
rtr
end
0.02
0.03
0.37
0.04
0.07
0.42
0.40
1A
mon
gw
omen
who
had
wor
ked
duri
ngth
e5
year
spr
ior
toin
terv
iew
and
excl
udin
gal
lw
omen
who
repo
rted
only
pass
ive
smok
eex
posu
refr
oma
husb
and
(864
case
s,93
6co
ntro
ls).
–2A
llO
Rs
and
95%
CIs
wer
eca
lcul
ated
ina
logi
stic
regr
essi
onm
odel
adju
sted
for
age,
educ
atio
n,fa
mily
hist
ory
ofbr
east
canc
er,p
erso
nalh
isto
ryof
fibro
aden
oma,
age
atm
enar
che,
pari
ty,a
geat
first
live
birt
h,m
enop
ausa
lst
atus
,ag
eat
men
opau
se,
phys
ical
activ
ity,
wai
st-t
o-hi
pra
tioan
dpa
ssiv
esm
okin
gfr
omhu
sban
d.
608 SHRUBSOLE ET AL.
REFERENCES
1. Kuper H, Boffetta P, Adami HO. Tobacco use and cancer causation:association by tumour type. J Intern Med 2002;252:206–24.
2. Terry PD, Rohan TE. Cigarette smoking and the risk of breast cancerin women: a review of the literature. Cancer Epidemiol BiomarkersPrev 2002;11:953–71.
3. Morabia A. Smoking (active and passive) and breast cancer: epide-miologic evidence up to June 2001. Environ Mol Mutagen 2002;39:89–95.
4. Sandler DP, Everson RB, Wilcox AJ. Passive smoking in adulthoodand cancer risk. Am J Epidemiol 1985;121:37–48.
5. Hirose K, Tajima K, Hamajima N, Inoue M, Takezaki T, Kuroishi T,Yoshida M, Tokudome S. A large-scale, hospital-based case-controlstudy of risk factors of breast cancer according to menopausal status.Jpn J Cancer Res 1995;86:146–54.
6. Jee SH, Ohrr H, Kim IS. Effects of husbands’ smoking on theincidence of lung cancer in Korean women. Int J Epidemiol 1999;28:824–8.
7. Smith SJ, Deacon JM, Chilvers CE. Alcohol, smoking, passive smok-ing and caffeine in relation to breast cancer risk in young women. UKNational Case-Control Study Group. Br J Cancer 1994;70:112–9.
8. Morabia A, Bernstein M, Heritier S, Khatchatrian N. Relation ofbreast cancer with passive and active exposure to tobacco smoke.Am J Epidemiol 1996;143:918–28.
9. Lash TL, Aschengrau A. Active and passive cigarette smoking and theoccurrence of breast cancer. Am J Epidemiol 1999;149:5–12.
10. Marcus PM, Newman B, Millikan RC, Moorman PG, Baird DD,Qaqish B. The associations of adolescent cigarette smoking, alcoholicbeverage consumption, environmental tobacco smoke, and ionizingradiation with subsequent breast cancer risk (United States). CancerCauses Control 2000;11:271–8.
11. Johnson KC, Hu J, Mao Y. Passive and active smoking and breastcancer risk in Canada, 1994–97. Canadian Cancer Registries Epide-miology Research Group. Cancer Causes Control 2000;11:211–21.
12. Delfino RJ, Smith C, West JG, Lin HJ, White E, Liao SY, Gim JS, MaHL, Butler J, Anton-Culver H. Breast cancer, passive and activecigarette smoking and N-acetyltransferase 2 genotype. Pharmacoge-netics 2000;10:461–9.
13. Wartenberg D, Calle EE, Thun MJ, Heath CW Jr, Lally C, WoodruffT. Passive smoking exposure and female breast cancer mortality.J Natl Cancer Inst 2000;92:1666–73.
14. Egan KM, Stampfer MJ, Hunter D, Hankinson S, Rosner BA, HolmesM, Willett WC, Colditz GA. Active and passive smoking in breastcancer: prospective results from the Nurses’ Health Study. Epidemi-ology 2002;13:138–45.
15. Kropp S, Chang-Claude J. Active and passive smoking and risk ofbreast cancer by age 50 years among German women. Am J Epide-miol 2002;156:616–26.
16. Ji BT, Dai Q, Gao YT, Hsing AW, McLaughlin JK, Fraumeni JF Jr,Chow WH. Cigarette and alcohol consumption and the risk of colo-rectal cancer in Shanghai, China. Eur J Cancer Prev 2002;11:237–44.
17. Gao YT, Shu XO, Dai Q, Potter JD, Brinton LA, Wen W, Sellers TA,Kushi LH, Ruan Z, Bostick RM, Jin F, Zheng W. Association ofmenstrual and reproductive factors with breast cancer risk: resultsfrom the Shanghai Breast Cancer Study. Int J Cancer 2000;87:295–300.
18. Band PR, Le ND, Fang R, Deschamps M. Carcinogenic and endocrinedisrupting effects of cigarette smoke and risk of breast cancer. Lancet2002;360:1044–9.
19. Terry PD, Miller AB, Rohan TE. Cigarette smoking and breast cancerrisk: a long latency period? Int J Cancer 2002;100:723–8.
20. Ambrosone CB, Freudenheim JL, Graham S, Marshall JR, Vena JE,Brasure, JR, Michalek AM, Laughlin R, Nemoto T, Gillenwater KA,Shields PG. Cigarette smoking, N-acetyltransferase 2 genetic poly-morphisms, and breast cancer risk. JAMA 1996;276:1494–501.
21. Palmer JR, Rosenberg L, Clarke EA, Stolley PD, Warshauer ME,Zauber AG, Shapiro S. Breast cancer and cigarette smoking: a hy-pothesis. Am J Epidemiol 1991;134:1–13.
22. Baron JA, La Vecchia C, Levi F. The antiestrogenic effect of cigarettesmoking in women. Am J Obstet Gynecol 1990;162:502–14.
23. Brunet JS, Ghadirian P, Rebbeck TR, Lerman C, Garber JE, ToninPN, Abrahamson J, Foulkes WD, Daly M, Wagner-Costalas J, God-win A, Olopade OI, et al. Effect of smoking on breast cancer incarriers of mutant BRCA1 or BRCA2 genes. J Natl Cancer Inst1998;90:761–6.
24. Baron JA, Newcomb PA, Longnecker MP, Mittendorf R, Storer BE,Clapp RW, Bogdan G, Yuen J. Cigarette smoking and breast cancer.Cancer Epidemiol Biomarkers Prev 1996;5:399–403.
25. Millikan RC, Pittman GS, Newman B, Tse CK, Selmin O, Rockhill B,Savitz, Moorman PG, Bell DA. Cigarette smoking, N-acetyltrans-ferases 1 and 2, and breast cancer risk. Cancer Epidemiol BiomarkersPrev 1998;7:371–8.
26. National Cancer Institute. Health effects of exposure to environmentaltobacco smoke: the report of the California Environmental ProtectionAgency. Smoking and Tobacco Control Monograph 10. Bethesda:U.S. Department of Health and Human Services, National Institutes ofHealth, National Cancer Institute, 1999.
27. Hollingsworth AB, Lerner MR, Lightfoot SA, Wilkerson KB, HanasJS, McCay PB, Brackett DJ. Prevention of DMBA-induced rat mam-mary carcinomas comparing leuprolide, oophorectomy, and tamox-ifen. Breast Cancer Res Treat 1998;47:63–70.
28. Perera FP, Estabrook A, Hewer A, Channing K, Rundle A, MooneyLA, Whyatt R, Phillips DH. Carcinogen-DNA adducts in humanbreast tissue. Cancer Epidemiol Biomarkers Prev 1995;4:233–8.
29. Petrakis NL. Nipple aspirate fluid in epidemiologic studies of breastdisease. Epidemiol Rev 1993;15:188–95.
30. Li D, Zhang W, Sahin AA, Hittelman WN. DNA adducts in normaltissue adjacent to breast cancer: a review. Cancer Detect Prev 1999;23:454–62.
31. Rundle A, Tang D, Hibshoosh H, Estabrook A, Schnabel F, Cao W,Grumet S, Perera FP. The relationship between genetic damage frompolycyclic aromatic hydrocarbons in breast tissue and breast cancer.Carcinogenesis 2000;21:1281–9.
32. Ishibe N, Hankinson SE, Colditz GA, Spiegelman D, Willett WC,Speizer FE, Kelsey KT, Hunter DJ. Cigarette smoking, cytochromeP450 1A1 polymorphisms, and breast cancer risk in the Nurses’Health Study. Cancer Res 1998;58:667–71.
33. Huang CS, Chern HD, Shen CY, Hsu SM, Chang KJ. Associationbetween N-acetyltransferase 2 (NAT2) genetic polymorphism anddevelopment of breast cancer in postmenopausal Chinese women inTaiwan, an area of great increase in breast cancer incidence. Int JCancer 1999;82:175–9.
34. Basham VM, Pharoah PD, Healey CS, Luben RN, Day NE, EastonDF, Ponder BA, Dunning AM. Polymorphisms in CYP1A1 and smok-ing: no association with breast cancer risk. Carcinogenesis 2001;22:1797–800.
35. Firozi PF, Bondy ML, Sahin AA, Chang P, Lukmanji F, SingletaryES, Hassan MM, Li D. Aromatic DNA adducts and polymorphisms ofCYP1A1, NAT2, and GSTM1 in breast cancer. Carcinogenesis 2002;23:301–6.
36. Hunter DJ, Hankinson SE, Hough H, Gertig DM, Garcia-Closas M,Spiegelman D, Manson JE, Colditz GA, Willett WC, Speizer FE,Kelsey K. A prospective study of NAT2 acetylation genotype, ciga-rette smoking, and risk of breast cancer. Carcinogenesis 1997;18:2127–32.
37. Morabia A, Lash TL. Breast cancer, passive and active cigarettesmoking and N-acetyltransferase 2 genotype. Pharmacogenetics2002;12:85–8.
38. Meek MD, Finch GL. Diluted mainstream cigarette smoke conden-sates activate estrogen receptor and aryl hydrocarbon receptor-medi-ated gene transcription. Environ Res 1999;80:9–17.
39. Cavalieri E, Frenkel K, Liehr JG, Rogan E, Roy D. Estrogens asendogenous genotoxic agents—DNA adducts and mutations. J NatlCancer Inst Monogr 2000;27:75–93.
40. Michnovicz JJ, Bradlow HL. Dietary and pharmacological control ofestradiol metabolism in humans. Ann NY Acad Sci 1990;595:291–9.
41. Zhu BT, Conney AH. Functional role of estrogen metabolism in targetcells: review and perspectives. Carcinogenesis 1998;19:1–27.
42. Jefcoate CR, Liehr JG, Santen RJ, Sutter TR, Yager JD, Yue W,Santner SJ, Tekmal R, Demers L, Pauley R, Naftolin F, Mor G,Berstein L. Tissue-specific synthesis and oxidative metabolism ofestrogens. J Natl Cancer Inst Monogr 2000;27:95–112.
43. Weiderpass E, Baron JA. Cigarette smoking, alcohol consumption,and endometrial cancer risk: a population-based study in Sweden.Cancer Causes Control 2001;12:239–47.
44. Terry PD, Rohan TE, Franceschi S, Weiderpass E. Cigarette smokingand the risk of endometrial cancer. Lancet Oncol 2002;3:470–80.
45. Newcomer LM, Newcomb PA, Trentham-Dietz A, Storer BE. Hor-monal risk factors for endometrial cancer: modification by cigarettesmoking (United States). Cancer Causes Control 2001;12:829–35.
46. Brinton LA, Barrett RJ, Berman ML, Mortel R, Twiggs LB, WilbanksGD. Cigarette smoking and the risk of endometrial cancer. Am JEpidemiol 1993;137:281–91.
609PASSIVE SMOKING AND BREAST CANCER





























