Embed Size (px)
Citation preview

To Radiate or Not? Is APBI the Right Compromise Solution?
Partial Breast Irradiation for Breast Conserving Therapy
Julia White MDProfessor, Radiation Oncology

Agenda
• Role of radiotherapy in breast conservation – what are the goals of treatment?
• Accelerated partial breast irradiation ( APBI) – rationale, outcome and indications
• Comparison of APBI to Omission of radiotherapy post lumpectomy
• Intraoperative Partial Breast Irradiation ( IPBI).

Breast Conservation with Lumpectomy and Radiotherapy (RT)
• Equivalent long term survival is evident from breast conservation compared to mastectomy from numerous Phase III randomized trials from the U.S. and Europe - now with > 20 years of follow-up.
• Equivalent local regional cancer recurrence now reported from breast conservation compared to mastectomy from analyses that reflect modern treatment era; e.g. complete excision, systemic therapy, etc.
• Breast conservation affords many benefits including faster recovery, lower health costs, intact sensation, among others.
• Increasingly, modern registry and cost analysis support the benefit of breast conservation for early stage invasive breast cancer

Improved Disease Specific Survival with Breast Conservation Therapy vs Mastectomy
SEER 1998-2008: 132,149 patients, BCT 92,671 (70.1%), Mastectomy alone 34,999 (26.5%), and mastectomy with RT 4479 (3.4%).
Agarwal , JAMA surg 2014

Whole Breast Irradiation post-Lumpectomy
50 Gy/25 Fractions42.56 Gy/ 16 Fractions
Total: 60 -66 Gy30-33 Fractions
– WBI method used in:• Randomized control trials
demonstrating equivalency of BCT to MRM
• Early Breast Cancer Trialists Collaborative Group’s meta-analysis
• Registry Analyses
10 -16 Gy5-8 Fractions

Alternatives to WBI Post-Lumpectomy: Subject of Clinical Investigation for Decades!
Randomized Trials Accrued Prior to 1990

Goals of Post-lumpectomy RadiotherapyInvasive breast cancer:
• Maximize local control• Equivalence to mastectomy• Prevent Distant Metastases• Optimize breast cancer/ overall survival• Maintain sensate and acceptable
cosmetic breast appearance

ACCELERATED PARTIAL BREAST IRRADIATION (APBI)

Scientific Rationale for Radiation Targeted to the Tumor Bed Only
Recurrences (LR) Away From Tumor Bed(‘Elsewhere’ Failures-New Primary cancers):– Much lower frequency after lumpectomy
alone or followed by whole breast RT- LR Roughly 2-3% w/o RT and < 1% with RT *
Major Effect Of Post-Lumpectomy RT:– Reduce risk of recurrence in tumor bed region– LR Roughly 10-25% w/o RT and 3-4% with RT *
Potential Benefits: • Less toxicity• Reduced burden of care• Better utilization of BCT
* Milan 3,OCOGUOBCG

Accelerated Partial Breast Irradiation
30-38 Gy/6-10 treatments
5-8 days
Accelerated PBI Definition: Delivery of hypo fractionated ( i.e.larger doses/fraction)radiation to the high risk breast only (lumpectomy cavity plus 1-2 cm margin) AFTER Lumpectomy using brachytherapy or external beam irradiation techniques
Goals: to achieve local control post-lumpectomy that is equivalent to WBI

20 Years of Clinical Trials in APBI: Where Do We Stand?1997 -2000 RTOG 9517 Multi catheter APBI Phase II/ feasibility 2000-2001 MammoSite APBI Phase II/ feasibility
2002 MammoSite FDA Approval2002-2004 ASBS Registry MammoSite APBI2003-2004 RTOG 0319 3DCRT APBI Phase II/ feasibility
2004 NASBP B39/ RTOG 0413 Phase III opens2006 OCOG 3DCRT RAPID Phase III opens2009 ASTRO Consensus Guidelines2011 OCOG 3DCRT RAPID Phase III closes2013 NSABP B39/ RTOG 0413 Phase III closes2013 OCOG RAPID Reports Cosmetic Interim Analysis2015 Phase III University of Florence Trial reports Cancer Outcomes2016 Phase III ESTRO Clinical Trial reports Cancer Outcomes

APBI Success Supported by Important Trends in Breast Cancer Clinical Investigation
1. Technology development• Single Entry Devices for Brachytherapy• Integration of advanced technology for external beam RT (3DCRT,
IMRT, etc)2. Re- evaluation of Breast Cancer Radiobiology
• Safety of larger dose/ treatment (fraction) for Breast RT• Linear Quadratic Equation allows calculation of different schemes to
deliver biologically effective dose3. Breast Cancer Heterogeneity better understood
• Intrinsic Subtypes have different local regional recurrence after BCT

Advantages DisadvantagesIrregularly shaped
cavitiesInvasive Procedure
Skin and chestwall sparing
Technically complicated
Durable results demonstrated
Restricted access
50%
80%
100%
120%
140%
200%
Advantages DisadvantagesSimplified approach
Invasive Procedure
Improved technology access
Potential CavityMisfit
Surgeonacceptance
Availability Limited
Multicatheter (MCT) APBI Single Entry Device (SED) APBIBrachytherapy

APBI Single Entry Brachytherapy: Next Generation are Multi-Channel
Contura SenoRxSAVI Ciana medical
Advantages: • dosimetric coverage • sparing of skin and
chestwall

External Beam APBI
Advantages DisadvantagesNon Invasive Variable Target
DefinitionLinear Accelerators
UbiquitousInter- and Intra-
fraction error
• 3DCRT• IMRT
Linear accelerator delivery

APBI Success Supported by Important Trends in Breast Cancer Clinical Investigation
1. Technology development• Single Entry Devices for Brachytherapy• Integration of advanced technology for external beam RT (3DCRT,
IMRT, etc)2. Re- evaluation of Breast Cancer Radiobiology
• Safety of larger dose/ treatment (fraction) for Breast RT• Linear Quadratic Equation allows calculation of different schemes to
deliver biologically effective dose3. Breast Cancer Heterogeneity better understood
• Intrinsic Subtypes have different local regional recurrence after BCT

Reduced Local Recurrence after Lumpectomy and WBI in Luminal Subtype by IHC
• 1434 BCT patients with 7 year median F/U
Local Recurrence:Lum A 0.8%Lum B 2.3%Lum HER 7.4%HER 2 10.8%TNBC 6.7%
Arvold, et al JCO 2011

Phase II Multi-institution Trials That Established APBI Efficacy Post-lumpectomy for BCT
Clinical Trial nAPBI Type
DoseTarget
DefinitionPopulation (%) Median
F/u% IBR
T1 N0 ER+
RTOG 9517 99MCT
Brachy34 Gy,
10F, BID
C/PTV:2cm radial
1cm Ant/post88 81 74 12.2 yrs 6.2
MammoSiteIndustry
43SED
Brachy34 Gy,
10F, BIDC/PTV: 1 cm expansion 100 100 - 5.5 yrs 0
RTOG 0319 52 3DCRT38.5 Gy, 10 F, BID
CTV: 1.5 cmPTV: 1.0 cm 94 92 83 8 yrs 7.7
Austrian 274MCT
Brachy32Gy8 F
C/PTV: Variable 92 100 100 5.3 yrs 2.9

Three Randomized Trials Comparing APBI to WBI Post Lumpectomy Have Reported Outcomes
• TTrial Years APBI method Dose Eligibility
U. Florence1 2005-2013 IMRT 30 Gy/ 5 F/ QOD Age > 40 yrsTsz < 2.5 cm
NIO Budapst2 1998 - 2004 MCT BrachyHDR
36.4 Gy/ 5.2 Gy x 7 high-dose-rate (HDR)
pN0,G1-2 Tsize < 2.0 cm
GEC-ESTRO3 2004 - 2009 MCT BrachyHDR
32 Gy/ 4 Gy x 8/ BID30 Gy/ 4.3 Gy x 7/ BID
Age > 40Tsz < 3 cmpN0, pN1mi
1 Livi et al. Eur J Ca 20152Polgar et al. Rad & Onc, 20133Strnad et al. Lancet Oncol 2016

No Difference in Local Recurrence in 3 Phase III Clinical Trials Comparing
APBI Vs. WBI
nMedian
Follow upAPBI
Method
Local Recurrence
RegionalRecurrence
APBI WBI APBI WBIU. Florence1 520 5 years IMRT 1.5% 1.4% 1.4% 1.9%NIO Budapest2 287 10.2 years MCT 5.5% 4.6% 2.5% 1.7%GEC-ESTRO3 1184 6.6 years MCT 1.4%
(1.9%)*0.92%
(1.67%)*0.49% 0.56%
1 Livi et al. Eur J Ca 20152Polgar et al. Rad & Onc, 2013
*Local + 2nd Primary3Strnad et al. Lancet Oncol 2016

Three APBI Phase III Trials: Similar Low Risk Hormone Sensitive Breast Cancer Populations
Age > 50 yr/ post Menop N0 Median T
sizeGrade
1-2 %ER/PR +
U. Florence1 83 % 86.2 % - # 88.9 % 95.4 %NIO Budapest2 76 % 94 % 1.3 cm 100 % 88.4 %GEC-ESTRO3 80 % 95 %* 1.2 cm 90 % 95 %
*Axillary staging was not performed in DCIS cases 4.5% (53/1185) # Median not given. ~ 95% < 2 cm
1 Livi et al. Eur J Ca 20152Polgar et al. Rad & Onc, 20133Strnad et al. Lancet Oncol 2016

APBI Caution: Adverse Biology
nF/ upmo.
MethodAPBI Factor
LocalRec %
University WI 1 322 60 MCT Histopath 12.7MGH 2 98 71 3DCRT TNBC 33
GER-Aust 3 274 64 MCT ER+ but no endocrine therapy 12
1 Cannon et al., Ann Surg Oncol 20132 Pashtan et al, IJROBP 20123 Ott et al, IJROBP 2011

Adverse Cosmetic Results for 3DCRT APBIOCOG RAPID Early Reporting
WBIABPI-
3DCRT
DifferenceAPBI-WBI(95% CI) p value
Baselinen=1995 17% 19% 2% (2-5%) 0.35
3 yearsn=850 19% 32% 13% (7-19%) < 0.0001
Adverse Cosmetic Outcome ( Fair –Poor)Nurse Assessment at Baseline and 3 years
Olivotto et al, JCO 2013

Improved Cosmetic Results for IMRT APBIUniversity of Florence
Harvard Scale (Excellent, good, fair, poor)Physician Assessment
Livi et al, European J Cancer 2015
Physician-rated Cosmesis WBI % APBI % Overall p valueExcellent 89.6 95.1
Good 9.6 4.9Fair 0.8 0Poor 0 0 0.045

Numerous Additional Phase III Trials Will Build on the Current Findings
Clinical Trial Status Accrual APBI Method
NSABP B-39/ RTOG 0413 Closed 2013 42143-DCRT
SEDMCT
RAPID OCOG Closed 2012 2135 3-DCRT
IMPORT Low MRC Closed 2011 1935 IMRT/3D
IRMA Open to accrual 3302 3DCRT
SHARE Open to accrual 2796 3DCRT
14,382

Suitable Cautionary UnsuitablePatient Factors Age > 60 years 50-59 < 50
BRCA 1-2 no no YesPath Features T-size < 2 cm 2.1-3.0 cm > 3.0 cm
T stage T-1 T-0 – T-2 T 3- T4Margins Negative ( 2 mm) Close (< 2 mm) Positive
LVSI No Limited, focal ExtensiveER Pos. Neg. -
Multicentric Unicentric Unicentric PresentMultifocal Clinically unifocal Clinically unifocal Clinically multifocal
Histo IDC ILC -DCIS, EIC No, No Yes, Yes (< 3 cm) > 3 cm
Nodes N stage pN0 (i+ , -) - pN1, N2-3Nodal Surgery yes yes no
2009 ASTRO Consensus Statement for Treatment with APBI Outside a Clinical Trial
Smith, IJROBP,4:2009

“Suitable” Group Update 2016ASTRO Consensus Statement for APBI
Selected Factors SuitablePatient Factors: Age > 60 years
Path Features: T-size < 2 cmT stage T-1
Margins Negative ( 2 mm)ER Positive
Nodes: N stage pN0 (i+ , - )
> 50 years
* With Permission – Update of the ASTRO APBI Consensus Statement

IS APBI A “COMPROMISE” IN THE QUESITON OF TO RADIATE OR NOT?
HOW DOES APBI COMPARE TO OMISSION OF POST LUMPECTOMY RADIOTHERAPY?

Rationale for Omission of RT• Early Breast Cancer Trialists meta-analysis in 2011 of 17
randomized trials of RT vs No RT post lumpectomy• Post lumpectomy RT results in 15% reductions in any
recurrence and 3% gains in survival in node negative patients
• However, low risk node negative with low absolute reduction in recurrence did not derive a survival benefit
• This means it’s feasible to identify low risks patient that omission of RT will not threaten survival but will have higher local recurrence that may be acceptable
EBCTCG Lancet 2011; 378: 1707–16

RCT in Hormone Responsive pN0 Breast Cancer Evaluating RT Benefit in Addition to Anti Endocrine Therapy Post-lumpectomy
Clinical Trial nF/Uyrs
Age > 50 y
(%)
T sz <2 cm(%)
ER/PR+
(%)Tam/AI
(%)Grade 1-2 (%)
In-breast recurrence (%)RT No RT
PMH 769 5.6 100 83 80.5 100 68.3 0.6 7.7ABCSG 8a 869 4.48 99 90 100 100 95 0.4 5.1
CALGB 9343 626 12.6 1003 98 97 100 - 1.9 10PRIME 2 1326 5 100 89 90 100 97 1.3 4.1
Low risk features: Older age, pN0, small size, ER/PR+, G1-2, anti endocrine therapy

Elderly Women with Hormone Sensitive Stage 1 Breast Cancer
CALGB 9343 PRIME2
N= 626> 70 yo (median 77 yrs)
12 year follow up
N=1326> 65 yo ( median 70 yrs)
5 year follow up
RT No RT RT No RTLocal regional recurrence 1.9% (6) 10% (32) 1.3%(5) 4.1% (26)
Death From Breast Cancer 4.1% (13) 2.5% (8) 0.6% (4) 1% (8)Death from all causes 52% (166) 52% (168) 6% (40) 7.3% (49)Mastectomy –free rate 98% (-) 96% (-) 99.7% (2) 98% (12)
Hughes et al, JCO, 2013Kunkler et al, Lancet Oncol, 2015 PRIME2: Increase LRR with Estrogen poor tumors w/o RT ~ 9%

Conclusions APBI1. APBI post lumpectomy results in LRR equivalent to WBI in Stage 1
hormone sensitive, HER 2 negative breast cancer 2. Updated ASTRO consensus guidelines for APBI are recommended 3. APBI role remains questionable pending further RCT results in other
breast cancer subtypes and in more advanced stages4. In contrast to APBI, omission of RT post lumpectomy yields higher
local regional recurrences that are unlikely to be associated with excess breast cancer mortality and may be clinically acceptable to patients –trials are pending.
5. Women must be included on decision making for personalizing their breast conservation therapy.

INTRAOPERATIVE RADIOTHERAPY (IORT) FOR PBI

Definitions
– the delivery of a single high dose (~18-21 Gy) of irradiation directly to the post excision tumor bed during surgery prior to wound closure
Partial Breast Intraoperative Radiotherapy (IORT):

Intraoperative PBI
ADVANTAGES• Very localized dose• Direct visualization of area to treat• Reduce patient burden of care
– Reduce travel for external beam WBI– Spare second procedure for brachytherapy
APBI
DISADVANTAGES• Too localized dose • Final pathology unknown• Patient may receive unnecessary
treatment• Additional O.R time

Electron IORT Breast Cancer• Mobile linear accelerators in O.R.• 6-8 MeV electrons ( 4-15 MeV) • 5 - 8 cm diameter cones for
treatment• ~ 1 – 3 cm depth of breast tissue
ELIOT– Developed European Institute
of Oncology, Milan, Italy– Added lead shield under mobilized breast to protect chestwall

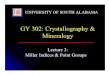
The TARGIT TechniqueCourtesy J.Vaydia 2010
INTRABEAM• A miniature electron generator and accelerator • A point source of 50 kV energy x-rays applicator
20 Gy at Surface
~ 5-7 Gy at depth of 10 mm

Targit: 5 mm
Eliot: 20 mm
Radiotherapy Target Volumes Differ for TARGIT and ELIOT IORT

PBI with Intraoperative Electrons (IOERT): Representative Studies
nF/upMo.’s
AgeMedian
yrsER +
%N-1%
Margins +%
LocalRec (%)
Montpellier(Lemanski)
42 72 72 100 - - 9.2#
Verona(Maluta)
226 46 63 91 22.1 7 0.4# ELIOT(Leonardi) 1822 60 58 89 27 2.9 4.1
# Retrospective analysis # median time to failure 62.4 months

ELIOT PBI: by ASTRO Consensus Guidelines for APBI
5 year rates Suitable Cautionary Unsuitable pn 294 698 812
Ipsilateral in-breast recurrence 1.5 % 4.4 % 8.8 % 0.003Regional nodal failure 1.5 % 1.9 % 1.1 % 0.55
Distant metastases 1.5 % 1.7 % 3.9 % 0.047Cause specific survival 99.1 % 98.7 % 96.5 % 0.025
Leonardi, IJROBP, 2011

ELIOT Phase III Randomized TrialMedian follow-up 5.8 years
5-year event rates WBI50 Gy/25 + boost
ELLIOT21 Gy/1
p
Ipsilateral in- breast recurrence 0.7 % 5.3 % <0.0001
In Quadrant 0.7 % 3.2 % < 0.002Outside quadrant 0 2.1 % < 0.001Regional nodal 0.4 % 1.1 < 0.02
Veronesi et al, Lancet Oncol 14: 2013
• 2000 -2007: randomized 1305 women > 48 years • T size < T1 85%, ER + 90%, N-1 21% • ~5.5% N-2 receive XRT to breast and nodes

TARGIT-A Phase III Randomized TrialMedian follow up: 29 months
• 2000 -2012: randomized 3451 women > 45 years• T size < T1 81.4%, ER + 90%, N-1 17% • ~15% randomized to TARGIT received WBI XRT to
breast and nodes
Vaiyda, Lancet 383, 2014
5-year event rates WBI TARGIT p
In- breast recurrence: ALL 1.3 % 3.3 % <0.042
Immed. IORT ( n=2298) 1.1% 2.1% 0.31Delayed IORT (n=1153) 1.7% 5.4% 0.069
Breast Cancer Mortality 1.9% 2.6% 0.51All Cause Mortality 5.5% 3.9% 0.099

Summary IORT PBIExpanding evidence regarding IORT PBI Will benefit from additional follow up and
analysis to find a population of breast cancer patients best suited for this approach
Recommend if used to focus on ASTRO “suitable” group: > 50, ER +, Node Negative, < 2 cm tumors.
Likely will benefit patients most who have some local control risk but whose risk for distant metastases is inherently low and the intent is its use will maximize breast conservation success.

Comparison of Alternatives to WBI for Hormone Sensitive Stage I Breast Cancer
APBI IORT PBI ObservationEquivalent local control to WBI in Phase III RCT
yes no no
Indication ASTRO Suitable *ASTRO Suitable - Elderly - ER rich
Method- Brachytherapy,- External bean ( 3DCRT, IMRT)
- Electrons- TARGIT (limited F/U) --

QUESTIONS?