Embed Size (px)
Citation preview

QUALITY REPORT
PART A – Patient Experience
1
Complaints and Patient Advice and Liaison Report
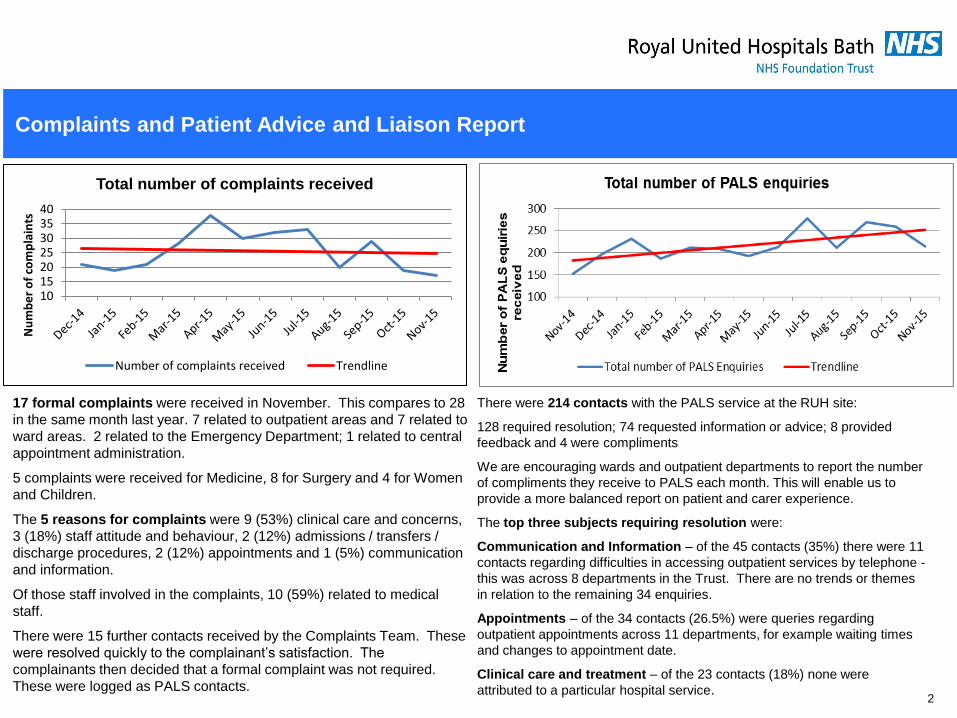
17 formal complaints were received in November. This compares to 28
in the same month last year. 7 related to outpatient areas and 7 related to
ward areas. 2 related to the Emergency Department; 1 related to central
appointment administration.
5 complaints were received for Medicine, 8 for Surgery and 4 for Women
and Children.
The 5 reasons for complaints were 9 (53%) clinical care and concerns,
3 (18%) staff attitude and behaviour, 2 (12%) admissions / transfers /
discharge procedures, 2 (12%) appointments and 1 (5%) communication
and information.
Of those staff involved in the complaints, 10 (59%) related to medical
staff.
There were 15 further contacts received by the Complaints Team. These
were resolved quickly to the complainant’s satisfaction. The
complainants then decided that a formal complaint was not required.
These were logged as PALS contacts. 2
10152025303540
Nu
mb
er
of
com
pla
ints
Total number of complaints received
Number of complaints received Trendline
There were 214 contacts with the PALS service at the RUH site:
128 required resolution; 74 requested information or advice; 8 provided
feedback and 4 were compliments
We are encouraging wards and outpatient departments to report the number
of compliments they receive to PALS each month. This will enable us to
provide a more balanced report on patient and carer experience.
The top three subjects requiring resolution were:
Communication and Information – of the 45 contacts (35%) there were 11
contacts regarding difficulties in accessing outpatient services by telephone -
this was across 8 departments in the Trust. There are no trends or themes
in relation to the remaining 34 enquiries.
Appointments – of the 34 contacts (26.5%) were queries regarding
outpatient appointments across 11 departments, for example waiting times
and changes to appointment date.
Clinical care and treatment – of the 23 contacts (18%) none were
attributed to a particular hospital service.

Nursing Quality Indicators Triangulation Chart - Exception Report (November data)
5
Areas of focus - The full Triangulation Report is in Appendix A. Two
wards have flagged this month:
Respiratory ward
This ward has flagged for the second consecutive month with day and night
staffing Registered Nurse (RN) fill rate <90% due to RN vacancies,
however HCA hours were increased to cover, particularly at night.
Quality matrices to note are:
• Pressure ulcer x 1 Grade 2 (x 1 Grade 2 last month)
• Staff sickness RN 17.3% HCA 9.1% (12.2% and 10.8% last mth)
• Appraisal rates RN 50% HCA 77.8% (61.5% and 66.7% last mth)
• FFT score improved to 82 and 1 negative PALs
(63 and negative PALS x 2 last month)
Action being taken
Long term sickness is being managed and staff are starting to return to
work. Staff are deployed from other wards to cover and the ward has been
allocated EU nurses which commence in January 2016.
Cardiac ward
This ward has flagged for the first time due to <90% RN fill rate on both day
and night shifts although increased HCA hours at night to cover. The ward
has RN vacancies and high RN sickness.
Quality matrices to note are:
• FFT score 75, formal complaint x 1
• Staff sickness RN 11.3%
• Appraisal rates RN 63.6% and HCA 54.5%
Action being taken
Long term sickness is being managed.
Recruitment is active and 6 RNs recruited although not in post.
Agency nurses are being block booked
Staff are deployed from other wards to cover as required.
HCA hours have been increased to cover, particularly at night.
The Directorate has placed Cardiac nurse staffing on the Risk Register with
these mitigating plans.
Note:
These 3 wards flagged the previous month, however their quality
matrices have improved this month.
Medical Assessment Unit (MAU)
RN vacancies are still high (around 15.0wte) however staff have
been deployed from other areas to cover.
ACE and Combe ward (OPU)
Both of these wards patient quality matrices have improved, however
it is important to note that both these wards were closed for 2 weeks
in November due to Norovirus.
Ward quality matrices to overall:
Nursing quality matrices have improved this month however it is
important to note that up to 7 wards were closed due to Norovirus in
this month starting from 11th November onwards.
• Complaints and negative PALs (wards only) have gone down
slightly this month
• Clostridium difficile x 4 cases (7 cases last month)
• Grade 2 Pressure Ulcers x 2 (5 last month)
• Nurse staffing Datix reports reduced this month from 29 ( 41 last
month)
• The number of Falls are fairly consistent with last month, but note
the change of interpretation/definition regarding moderate harms
to major harms this month to comply with NPSA guidance.
Recruitment update
• RN vacancies are around 80wte and recruitment remains very
active with new starters in the pipeline and EU nurses starting
Jan/Feb 2016.
• Trainee Assistant Practitioner applications exceeded expected
numbers (48) with interviews being held 22nd and 23rd December
for 15 posts on the wards. 3

QUALITY REPORT
4
PART B – Patient Safety and Quality Improvement
6 Patient Safety
Priorities
Deteriorating Patient including National Early Warning Score (NEWS)
Sepsis Acute Kidney Injury (AKI)
Venous Thromboembolism (VTE) Falls, Clostridium difficile
10 Executive sponsored projects of must-do’s
informed by business unit priorities, CQUIN or as a response to stakeholders
15 Divisional Safety Priorities
Pressure ulcers, Discharge, Ward and outpatient accreditation, Medicines
management, Critical Care, Diabetes, Dementia, Maternity (still birth and
breastfeeding), Urgent Care (Ambulatory Care), Peri-operative
Medicine
Reducing length of stay
Medical ambulatory care
Stroke sentinel audit
performance
Venous Thromboembolism
(VTE)
Nursing vacancies
Surgery
Reducing length of stay
Surgical ambulatory care
(ESAC)
Critical Care
Integration with RNHRD
specialties
Improving patient information
Women and Children
Increased consultant obstetric cover - labour
ward
Gynaecology emergency pathway
Acute paediatric flow
Reducing neonatal readmissions to maternity
Reducing full term admissions to NICU

Patient Safety - Acute Kidney Injury (AKI)
Background
Acute Kidney Injury has been established nationally as an area for improvement
with National drivers such as National ‘Think Kidneys’ campaign, NICE guidelines,
National patient safety alert in June 2014, National CQUIN 2015/6.
RUH has agreed a local CQUIN target with the CCGs.
Current Status
• The CQUIN report for the second quarter has been submitted and awaiting
response but expecting full achievement as compliant with all targets
• Project Support Manager appointed for 6 months to support the AKI work and
started in November
• Baseline numbers for incidence of AKI at RUH have been established from the
e alert – average 64 patients a week, 250 patient a month
• 2/3 of patients with AKI were triggered from ED majors i.e. were admitted with
AKI (similar to national data)
• Next commonest areas MAU, ICU, respiratory and cardiac wards
• Baseline data from July – September 2015 (709 patients) demonstrates that
65% of these patients had AKI grade 1, 20% grade 2 and 15% grade 3
• CCG representative joined steering group to link with care in the community
Awareness and Training
• Awareness campaign UR INE Trouble has been launched in November with
cascade training of a simple 10 minute teaching tool and launch of U.R.I.N.E.
bundle
• November training target was met of 100 staff since the beginning of November
Bundle compliance
• Details of measures to demonstrate bundle compliance have been established
• Focused work now starting on pilot wards (cardiac and respiratory)
• Baseline measures being collected on these wards in November and December
• Improvement ideas to improve bundle compliance to be tested in January
• Work planned with radiology to standardise process for reducing AKI following
contrast medium for imaging
Next Steps
• Test improvement ideas on cardiac and respiratory wards
• Awaiting IT linking E alert to discharge summary for patients with
AKI. Mandatory information on AKI then included in discharge
summary
• Outcome data from BIU to be obtained
• Developing patient information stickers linking with NBT as regional
renal centre and national resources
5

Patient Safety - Acute Kidney Bundle
6
Patient Safety - Clostridium difficile
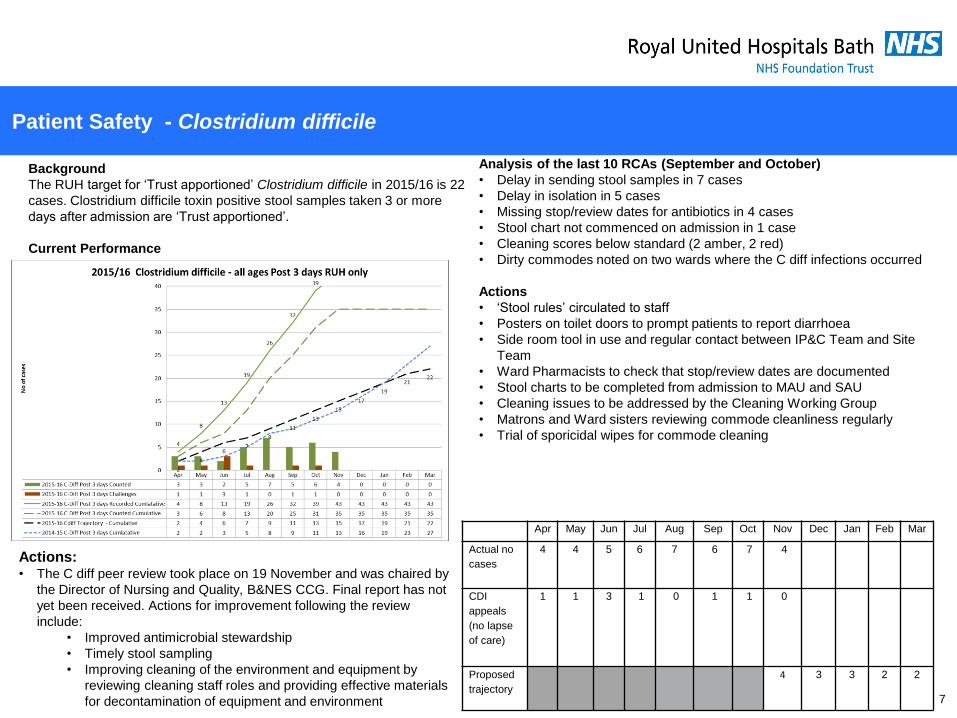
Background
The RUH target for ‘Trust apportioned’ Clostridium difficile in 2015/16 is 22
cases. Clostridium difficile toxin positive stool samples taken 3 or more
days after admission are ‘Trust apportioned’.
Current Performance
Analysis of the last 10 RCAs (September and October)
• Delay in sending stool samples in 7 cases
• Delay in isolation in 5 cases
• Missing stop/review dates for antibiotics in 4 cases
• Stool chart not commenced on admission in 1 case
• Cleaning scores below standard (2 amber, 2 red)
• Dirty commodes noted on two wards where the C diff infections occurred
Actions
• ‘Stool rules’ circulated to staff
• Posters on toilet doors to prompt patients to report diarrhoea
• Side room tool in use and regular contact between IP&C Team and Site
Team
• Ward Pharmacists to check that stop/review dates are documented
• Stool charts to be completed from admission to MAU and SAU
• Cleaning issues to be addressed by the Cleaning Working Group
• Matrons and Ward sisters reviewing commode cleanliness regularly
• Trial of sporicidal wipes for commode cleaning
7
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Actual no
cases
4 4 5 6 7 6 7 4
CDI
appeals
(no lapse
of care)
1 1 3 1 0 1 1 0
Proposed
trajectory
4 3 3 2 2
Actions: • The C diff peer review took place on 19 November and was chaired by
the Director of Nursing and Quality, B&NES CCG. Final report has not
yet been received. Actions for improvement following the review
include:
• Improved antimicrobial stewardship
• Timely stool sampling
• Improving cleaning of the environment and equipment by
reviewing cleaning staff roles and providing effective materials
for decontamination of equipment and environment

Pressure Ulcers
Next steps
Outpatients Accreditation
Outpatient departments are being mapped against KPIs Foundation
level. An observational audit has also been undertaken in each
outpatient area. The findings from the assessment will be presented at
the Outpatient Steering Group in January 2016.
Maternity and Paediatrics Accreditation
KPIs for Foundation level have been agreed with Maternity and
Paediatrics. Assessment to be completed in January 2016.
Ward Accreditation: Bronze level
The KPIs for Bronze level have been agreed. The assessment includes
further indicators including observations of care and unannounced
visits. An observational audit tool has been developed which is currently
being tested. This is an extensive assessment and it will require a team
of staff to undertake the observations of care. It is proposed that the
Bronze level assessment will be undertaken as part of the planning for
the CQC inspection of the Trust. It is anticipated that this will be
completed by February 2016.
Background
The Accreditation Programme has been developed to recognise and
incentivise high standards of care and reduce variation in practice at
ward and department level. It also provides assurance that regulatory
requirements including the Care Quality Commission (CQC)
fundamental standards are being met and identify where any
improvements in practice are required.
Wards and departments are assessed against Key Performance
Indicators (KPI) under the CQC domains (safe, caring, effective,
responsive, well-led) over a period of 6 months. The assessment takes
a tiered approach with wards initially being reviewed against
performance indicators for Foundation level. These are minimum
standards of quality and safety that wards are expected to achieve.
The indicators for Foundation level include information on the number
of incidents, safety briefings and handover, white board rounds, written
complaints, the Friends and Family Test, compliance with Millennium
assessments, compliance with key documentation and infection control
audits, mandatory training and staffing standards.
Current Performance
To date 19 adult wards have achieved accreditation at Foundation
level. There are 4 adult wards that have not yet achieved Foundation
level. The senior sisters of these wards have been given support with
developing an improvement plan and will be reassessed between
December 2015 and March 2016.
The Emergency Department have also achieved accreditation at
Foundation level.
Accreditation Programme Update
8

Patient Safety – Falls
Background
Reduction in falls is one of the Trust’s safety priorities. All ward areas,
including the RNHRD site, have an identified ward falls lead, with
evidence of embedding of active falls prevention and management
strategies. The targets for this workstream are a 10% reduction in the
number of repeat falls (the same patient falls more than once) and a 25%
reduction in falls resulting in moderate or severe harm. 05
101520253035
Nu
mb
er
of
falls
Falls resulting in moderate or severe harm (cumulative)
2015 (falls) 2015 (cumulative) 2015 Target
0
2
4
6
8
Nu
mb
er
of
falls p
er
1,0
00 b
ed
days
Falls per 1,000 bed days
Falls per1,000 beddays
HQIP
• The Trust is above the trajectory for moderate or major harms from falls. The
Trust had a rate of 0.16 falls per 1000 bed days resulting in
moderate/major/death. This is below the HQIP benchmark of 0.19
moderate/severe/death per 1000 bed days
• The Patient Safety Steering Group and the Falls Steering Group endorsed a
decision to change the harm level arising from falls with serious injury, in line
with National Guidance. Falls that were classified as resulting in moderate harm
are now major harm. From November this will be reflected in all reporting.
• A Falls Leads study morning is planned for December 2015 to include national
falls audit action plan, and development of falls training matrix
• Achievement of Falls CQUIN for Q2. There continues to be concentrated
support to identified clinical areas to facilitate achievement of Q3. A quarterly
report is produced which details progress to the work plan. The data from the
falls care bundle audit is included to provide ward level data
• Presentation to Innovation Panel planned for December on use of slippers.
Results suggest qualitative and anecdotal benefit. However data does not show
a reduction in falls
9
The Trust is above the trajectory for repeat fallers. There were 17 repeat
falls in November 2015. However, this is within the monthly target of 19.7.
Repeat Falls continue to be a high priority for reduction and are being
addressed through the ward falls leads and individual ward action plans.
050
100150200250300350
Nu
mb
er
of
falls
Repeat Falls 2015
2015 (falls) 2015 (cumulative) 2015 Target
The Healthcare Quality Improvement Partnership (HQIP) proposed a
benchmark of 6.63 falls/1000 bed days in October 2015. This replaces the
previous NPSA benchmark of 5.6 falls/1000 bed days.
Patient Safety – National Falls Audit
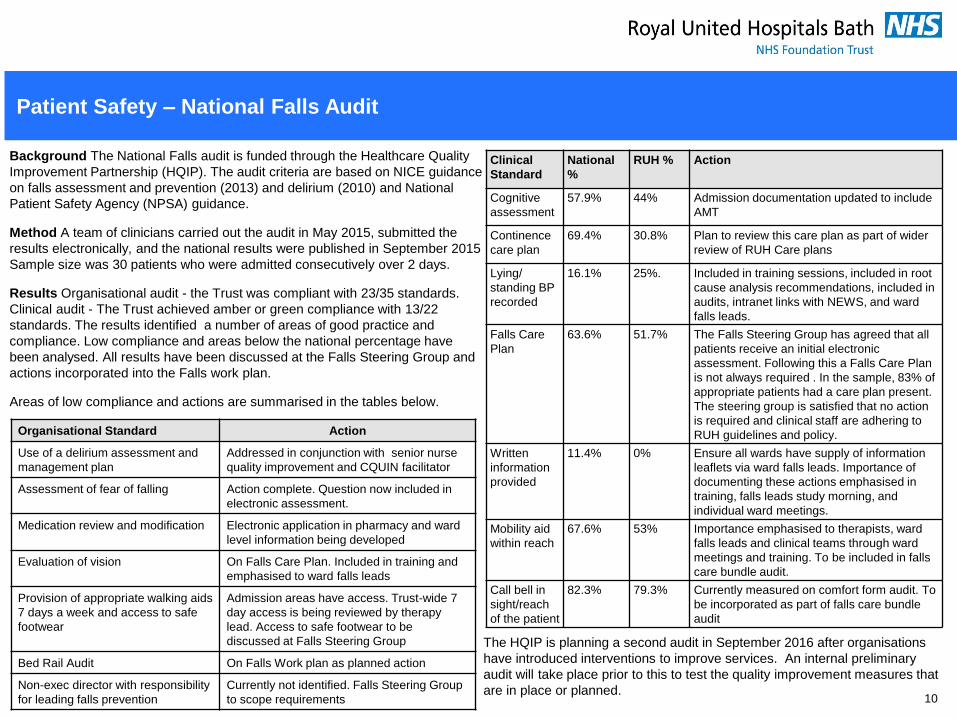
Background The National Falls audit is funded through the Healthcare Quality
Improvement Partnership (HQIP). The audit criteria are based on NICE guidance
on falls assessment and prevention (2013) and delirium (2010) and National
Patient Safety Agency (NPSA) guidance.
Method A team of clinicians carried out the audit in May 2015, submitted the
results electronically, and the national results were published in September 2015
Sample size was 30 patients who were admitted consecutively over 2 days.
Results Organisational audit - the Trust was compliant with 23/35 standards.
Clinical audit - The Trust achieved amber or green compliance with 13/22
standards. The results identified a number of areas of good practice and
compliance. Low compliance and areas below the national percentage have
been analysed. All results have been discussed at the Falls Steering Group and
actions incorporated into the Falls work plan.
Areas of low compliance and actions are summarised in the tables below.
10
Organisational Standard Action
Use of a delirium assessment and
management plan
Addressed in conjunction with senior nurse
quality improvement and CQUIN facilitator
Assessment of fear of falling Action complete. Question now included in
electronic assessment.
Medication review and modification Electronic application in pharmacy and ward
level information being developed
Evaluation of vision On Falls Care Plan. Included in training and
emphasised to ward falls leads
Provision of appropriate walking aids
7 days a week and access to safe
footwear
Admission areas have access. Trust-wide 7
day access is being reviewed by therapy
lead. Access to safe footwear to be
discussed at Falls Steering Group
Bed Rail Audit On Falls Work plan as planned action
Non-exec director with responsibility
for leading falls prevention
Currently not identified. Falls Steering Group
to scope requirements
Clinical
Standard
National
%
RUH % Action
Cognitive
assessment
57.9% 44% Admission documentation updated to include
AMT
Continence
care plan
69.4% 30.8% Plan to review this care plan as part of wider
review of RUH Care plans
Lying/
standing BP
recorded
16.1% 25%. Included in training sessions, included in root
cause analysis recommendations, included in
audits, intranet links with NEWS, and ward
falls leads.
Falls Care
Plan
63.6% 51.7% The Falls Steering Group has agreed that all
patients receive an initial electronic
assessment. Following this a Falls Care Plan
is not always required . In the sample, 83% of
appropriate patients had a care plan present.
The steering group is satisfied that no action
is required and clinical staff are adhering to
RUH guidelines and policy.
Written
information
provided
11.4% 0% Ensure all wards have supply of information
leaflets via ward falls leads. Importance of
documenting these actions emphasised in
training, falls leads study morning, and
individual ward meetings.
Mobility aid
within reach
67.6% 53% Importance emphasised to therapists, ward
falls leads and clinical teams through ward
meetings and training. To be included in falls
care bundle audit.
Call bell in
sight/reach
of the patient
82.3% 79.3% Currently measured on comfort form audit. To
be incorporated as part of falls care bundle
audit
T
The HQIP is planning a second audit in September 2016 after organisations
have introduced interventions to improve services. An internal preliminary
audit will take place prior to this to test the quality improvement measures that
are in place or planned.
Serious Incident (SI) summary
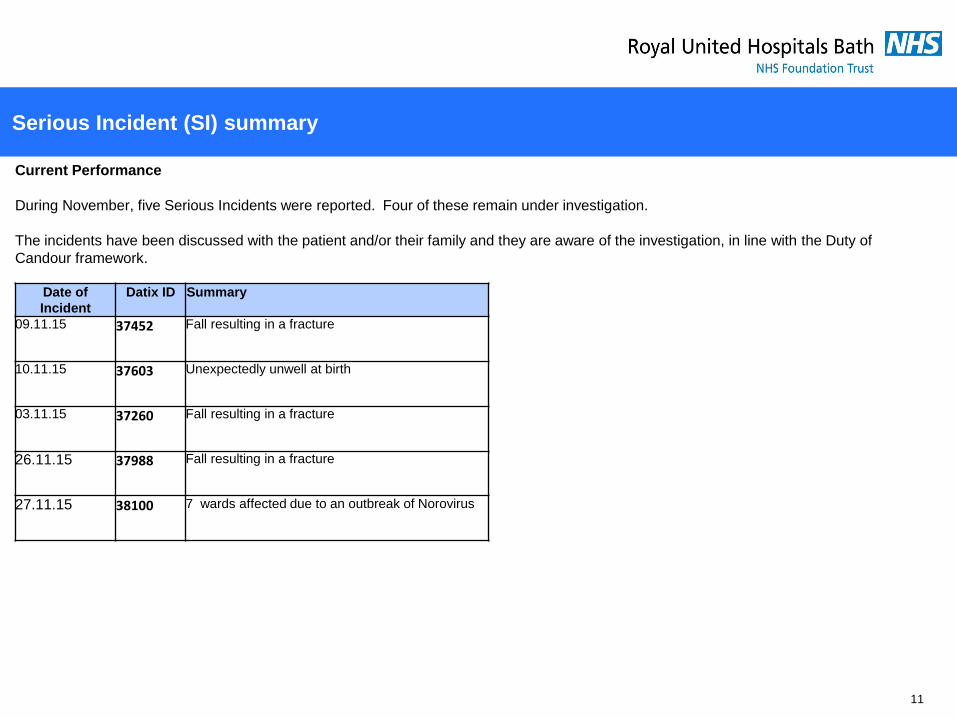
Current Performance
During November, five Serious Incidents were reported. Four of these remain under investigation.
The incidents have been discussed with the patient and/or their family and they are aware of the investigation, in line with the Duty of
Candour framework.
11
Date of
Incident
Datix ID Summary
09.11.15 37452 Fall resulting in a fracture
10.11.15 37603 Unexpectedly unwell at birth
03.11.15 37260 Fall resulting in a fracture
26.11.15 37988 Fall resulting in a fracture
27.11.15 38100 7 wards affected due to an outbreak of Norovirus

Serious Incident reports approved by the November Operational Governance Committee
(OGC)
12
Date of
Incident
Datix
ID
Summary Learning/ Recommendations
28.03.15 30694 Omission of medical alert • Clinical staff need to be aware of how to obtain information on ‘red drugs’, which are drugs not
included on the GP list, because they don’t prescribe them;
• Clinical teams should make the consultant team aware of the admission of any patients.
06.06.15 32730 Patient fall resulting in an injury • To review the use of over-bed tables without brakes in MAU;
• Encourage patients not to use over-bed tables as a means of support;
• Falls risk assessments to be undertaken within the agreed timeframe.
09.06.15 32783 Patient fall resulting in a fracture • To comply with the falls care plan requirement for lying and standing blood pressure
assessments;
• To review the delirium, pathway with the use of the falls care plan;
• To utilise the mental health liaison team for patients with delirium, for a standardised approach
across the Trust.
17.07.15 34053 Patient fall resulting in a fracture • The process for HCA’s undertaking and documenting admission assessments requires review;
• Reinforcement of the falls care bundle within the RNHRD environment.
09.08.15 34768 Collapse following diabetic
ketoacidosis
• For the Diabetes team to provide education to relevant clinical staff on the management of type 1
Diabetes in the elderly;
• To include Diabetes e-learning in the mandatory training matrix.
15.08.15 34914 Patient fall resulting in a fracture • To share the report findings with the patient's GP and the CCG, to highlight admission criteria
• To review the criteria for moving staff when balancing staffing levels.
03.09.15 35574 Patient fall resulting in a fracture • To consider the discharge of patients to their pre-admission place of residence, if awaiting long
term plans for alternative accommodation/placement;
• To identify a lead in complex discharges, to ensure that issues that require action are not
overlooked.
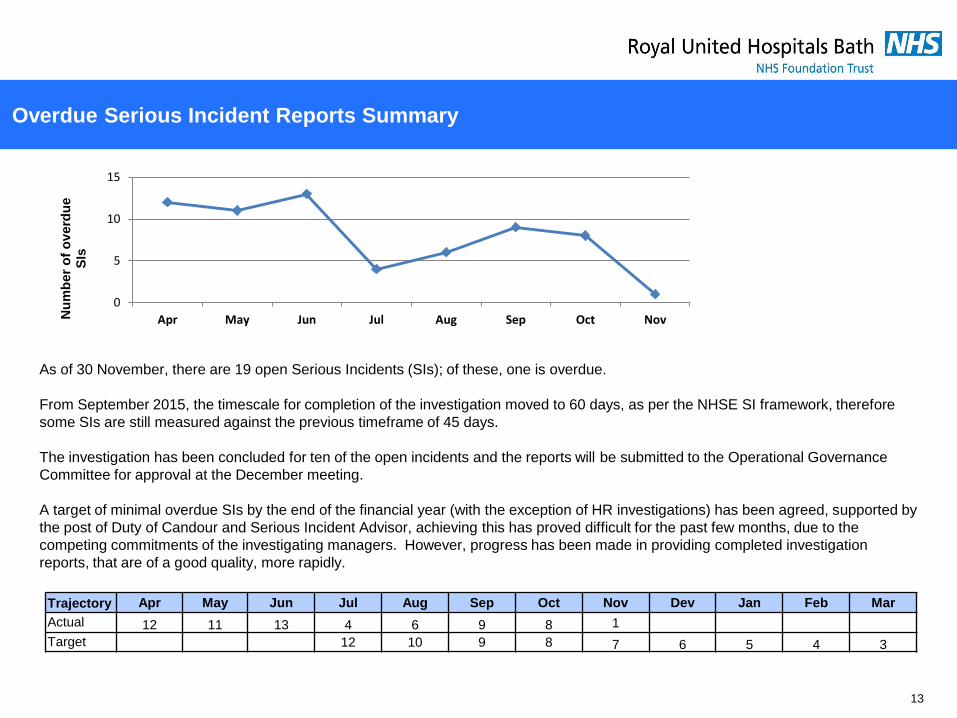
Overdue Serious Incident Reports Summary
13
As of 30 November, there are 19 open Serious Incidents (SIs); of these, one is overdue.
From September 2015, the timescale for completion of the investigation moved to 60 days, as per the NHSE SI framework, therefore
some SIs are still measured against the previous timeframe of 45 days.
The investigation has been concluded for ten of the open incidents and the reports will be submitted to the Operational Governance
Committee for approval at the December meeting.
A target of minimal overdue SIs by the end of the financial year (with the exception of HR investigations) has been agreed, supported by
the post of Duty of Candour and Serious Incident Advisor, achieving this has proved difficult for the past few months, due to the
competing commitments of the investigating managers. However, progress has been made in providing completed investigation
reports, that are of a good quality, more rapidly.
Trajectory Apr May Jun Jul Aug Sep Oct Nov Dev Jan Feb Mar
Actual 12 11 13 4 6 9 8 1
Target 12 10 9 8 7 6 5 4 3
0
5
10
15
Apr May Jun Jul Aug Sep Oct NovNu
mb
er
of
ov
erd
ue
SIs





























