Embed Size (px)
Citation preview

Part 7: Meeting the Standards Challenges
Healthcare Engineering Consultants
Strategies for the Standards Challenges

Safety Management
Healthcare Engineering Consultants
Issue:
Proactive Risk Assessments for Safety
Tip for Compliance:
Think of risk assessments as simply prioritizing potential problems

Documenting Risk Assessments
Healthcare Engineering Consultants
Risk Assessment:
“Prioritization and management of resources though an assessment of
probability and impact”

Why Perform Risk Assessments?
Not enough time!
Not enough staff!
Not enough money!
Healthcare Engineering Consultants

Calculating Risk Assessments
Risk =
Probability X Impact
Healthcare Engineering Consultants

Global Risk Assessments
What’s a Global Risk Assessment and What is
it’s Purpose?
Healthcare Engineering Consultants

Performing a Global Risk Assessment
Step 1: Identify a “Global” Area to Assess
Step 2: Select a Team of Stakeholders
Step 3: Brainstorm and List the Risk Elements
Step 4: Assign Probability and Impact to the Risk Elements
Step 5: Prioritize the Risk Elements
Step 6: Perform the Specific Risk Assessments
Healthcare Engineering Consultants

Documenting Risk Assessments
Healthcare Engineering Consultants
Global Risk Assessment Form
Department/ Area:_____________________________ Date: _____________ Completed by: _____________________
Risk Element Description Occurrence Probability(1-5)
Occurrence Impact(1-5)
Total Impact Score(Probability X Impact)
Notes: To use this form, list all of the possible risk elements associated with the department or area that may impactpatient or staff safety or result in damage to buildings or equipment. Using all available data sources, including experienceand previous history, insert numerical values for the probability and impact for each element. Calculate the total impactscore for each element, prioritize in descending numerical order and select a “cut-off” limit. For all scores above the “cut-off”, perform the six step risk assessment process.

Example Global Safety Risk Assessment
Healthcare Engineering Consultants
Global Risk Assessment for Safety Management
Risk Element Description Occurrence Probability (1-5) Occurrence Impact (1-5) Total Impact Score(Probability X Impact)
Employee injuries 5 2 10Ergonomic issues 4 2 8Unauthorized staff appliances 4 2 8Unauthorized smoking 5 1 5Egress corridor clutter 4 1 4Unlocked clean supply roomsin inpatient areas
4 1 4
Improper storage 3 1 3General housekeeping 3 1 3Unlocked supply rooms inoutpatient clinics
2 1 2
Improperly stored cylinders 1 1 1
Note 1: This form is used to determine the possible impact to safety that may occur in the hospital resulting from a variety ofdifferent risk elements. Each of the risk elements is prioritized based on the total impact score, starting with the highest scoreobtained. Specific assessments are then performed for each risk element (starting with the highest impact score) to determineactions that may be taken or processes that may be altered to reduce the overall risk to the hospital.
Note 2: The scoring is defined as follows:
Probability Score Description Impact Score Description
1 Very unlikely to ever occur 1 No injury is likely to occur 2 Unlikely to occur in one year 2 Minor injury is likely to occur 3 May occur in one year 3 Moderate injury is likely to occur 4 Likely to occur in one year 4 Serious injury is likely to occur 5 Almost certain to occur within one year 5 Death is likely to occur

Example Global Security Risk Assessment
Healthcare Engineering Consultants
Global Risk Assessment for Security Management
Risk Element Description Occurrence Probability (1-5) Occurrence Impact (1-5) Total Impact Score(Probability X Impact)
Infant abduction 1 3 3Pediatric abduction 1 3 3Assaultive behavior - ED 5 3 15Assaultive behavior – mentalhealth unit
5 3 15
Theft – gift shop 4 1 4Theft – pharmacy 2 2 4Theft of hospital property 5 2 10Theft from patients 5 2 10Auto accidents on hospitalproperty
4 3 12
Trespassing 4 1 4Auto vehicle break-in 4 2 8Weapons brought ontohospital property
4 1 4
Utility systems intentionallyturned off or damaged
2 4 8
Terrorist activity near or onhospital property
1 5 5
Toxic gas introduced intohospital air intakes
2 4 8
Note 1: This form is used to determine the possible impact to security that may occur in the hospital resulting from a variety ofdifferent risk elements. Each of the risk elements is prioritized based on the total impact score, starting with the highest scoreobtained. Specific assessments are then performed for each risk element (starting with the highest impact score) to determineactions that may be taken or processes that may be altered to reduce the overall risk to the hospital.
1

Specific Risk Assessments
What’s a Specific Risk Assessment and What is
it’s Purpose?
Healthcare Engineering Consultants

Performing a Specific Risk Assessment
Step 1: Identify Issues and Select a Team
Step 2: Analyze Factors
Step 3: Make a Decision
Step 4: Document the Evaluation and Decision
Step 5: Make the Necessary Changes
Step 6: Monitor and Reassess
Healthcare Engineering Consultants

Specific Risk Assessment Examples
Lock clean supply room doors?
Infant/ pediatric abduction measures
Safe environment for mental health
Medical equipment test tags
Utility system PM intervals
Security “sensitive areas”
Other?
Healthcare Engineering Consultants
Understanding RCA’s and FMEA’s
What’s the Difference Between an FMEA and an RCA?
Are They Both Risk Assessments?
Healthcare Engineering Consultants

Safety Management
Healthcare Engineering Consultants
Issue:
What about recurring operational deficiencies?
Tip for Compliance:
You can’t improve what you can’t measure!
How Do We Solve This Problem?
Steps required to reduce operational deficiencies:
1. Determine how to measure the problem severity
2. Establish a numerical baseline score
3. Explain measurement system to area staff
4. Let staff determine an improvement goal
5. Re-measure scores at unscheduled times
6. Provide numerical feedback to staff
7. Celebrate achievement of goal
8. Continue measurement until the culture changes
Healthcare Engineering Consultants
Solving the Hallway Clutter Problem
Healthcare Engineering Consultants
Step 1: Determine how to measure the problem severity
Solution and Procedure: Assign points to various types of egress corridor deficiencies, based on severity of violation

Solving the Hallway Clutter Problem
Healthcare Engineering Consultants
Point Score Examples
Description of Deficiency Point Score(per occurrence)
Small medical device on wheels (NIBP unit), against wall, charging, not blocking shut-offs
1
Equipment or furniture, not in use, one side of corridor only, not blocking shut-off or fire alarm
3
Large furniture or equipment, on both sides of corridor, not in use, not blocking shut-off/ alarm
5
Large furniture or equipment, in corridor, not in use, blocking emergency shut-off or fire alarm
8
Large furniture or equipment, in corridor, preventing fire or smoke door from closing
10
Solving the Hallway Clutter Problem
Healthcare Engineering Consultants
Step 2a: Establish a numerical baseline score for a specific hospital area (4 West)
Procedure: Use the point values for deficiencies that have been assigned and determine total scores by randomly inspecting the area once per day for at least one week
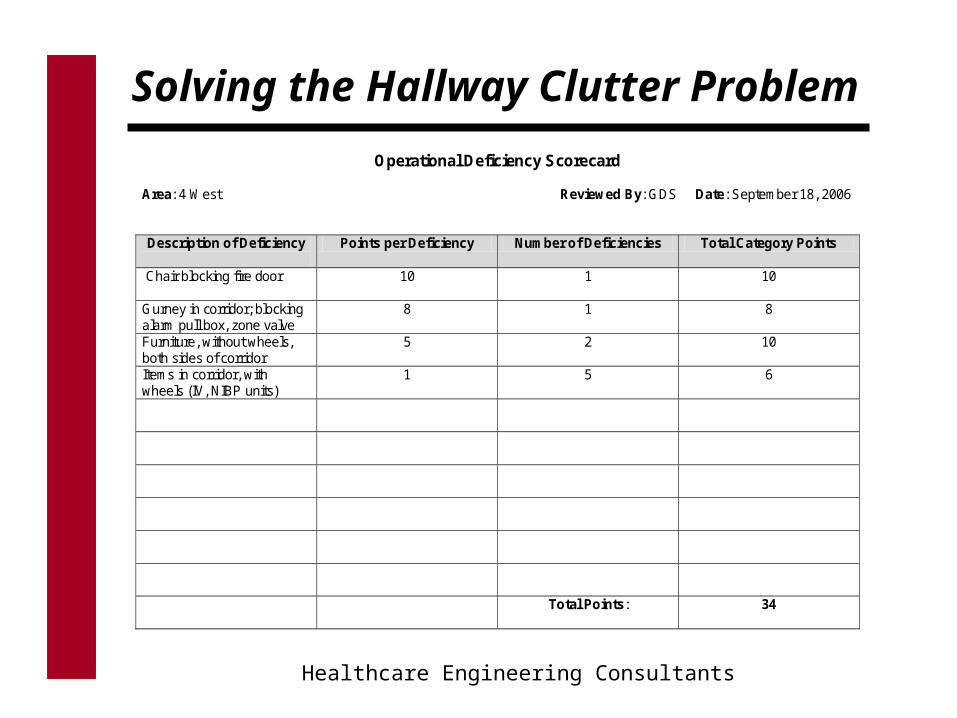
Solving the Hallway Clutter Problem
Healthcare Engineering Consultants
Operational Deficiency Scorecard Area: 4 West Reviewed By: GDS Date: September 18, 2006 Description of Deficiency
Points per Deficiency Number of Deficiencies Total Category Points
Chair blocking fire door
10 1 10
Gurney in corridor; blocking alarm pull box, zone valve
8 1 8
Furniture, without wheels, both sides of corridor
5 2 10
Items in corridor, with wheels (IV, NIBP units)
1 5 6
Total Points: 34

Solving the Hallway Clutter Problem
Healthcare Engineering Consultants
Point Score Results of Daily Inspections
Day Mon. Tues. Wed. Thurs. Fri.
Points 34 27 39 42 28
Cum. Average
34 32 33 36 34
This is the baseline number for 4 West

Solving the Hallway Clutter Problem
Healthcare Engineering Consultants
Graphical Results
0
10
20
30
40
50
60
70
Mon Tues Wed Thurs Fri
4 West Daily Data Baseline

Solving the Hallway Clutter Problem
Healthcare Engineering Consultants
Graphical Results
0
10
20
30
40
50
60
70
Mon Tues Wed Thurs Fri
4 West Daily Data New Goal
New goal: 25 pointsDaily Scores

Safety Management
Healthcare Engineering Consultants
Issue:
How to solve the smoking dilemma?
Tips for Compliance: Create a practical policy
Recognize the “citation priority”
Monitor smoking compliance

Smoking Monitoring
Healthcare Engineering Consultants
Summary of Smoking Violations
Location of Smoking Violation Time of Observed Violation Description of Violator
Area directly outside of EmergencyCenter; “B-C” corridor area
All shifts Staff, patients, visitors
Loading dock attached to “B” building First and second shift Staff, vendors
Loading dock attached to “D” building First and second shift Staff, vendors
Second level stairway exterior from “B”building
Second and third shift Staff
Main entrance to “A” building (within 50feet)
First shift Visitors and patients
Summary of Compliance Strategies
New anti-tobacco policy, effective 18 October, 2004 Smoking shelters are on order and will be installed in January, 2005 near the “A” building entrance Current signage will be replaced with universal “No Smoking” signs in January, 2005 New protocols for staff discipline have been implemented with the new policy Additional training for all staff regarding smoking policies has been provided Smoking cessation classes for hospital staff have been implemented; all smokers are encouraged to participate

Security Management
Healthcare Engineering Consultants
Issue: Security Responsibility Appointment
Tips for Compliance:
Letter provided by leadership
Identify security responsibility
Include:
Coordination
Development and implementation
Monitoring

Security Management
Healthcare Engineering Consultants
Issue: Security Risk Assessment
Tips for Compliance:
Include security sensitive areas:
ED, OB/ Gyn, Pharmacy, Infectious waste
Other areas?
Evaluate facility access control
Provide training for staff in sensitive areas

Security Management
Healthcare Engineering Consultants
Issue: Security “Special Cases”
Tips for Compliance: Consider the following –
Use of firearms or other means of force
Mental health areas
Medication and infectious waste security
Infant/ child abduction prevention and drills
Cell phones with cameras/ privacy issues
Access to unauthorized areas
Security in construction areas

Hazardous Materials and Wastes
Healthcare Engineering Consultants
Issue: MSDS Sheets
Tips for Compliance:
Ensure an accurate inventory
Provide staff training
Consider MSDS options:
Binder with data sheets
1-800 “Fax-on-Demand”
Internet or intranet access

Hazardous Materials and Wastes
Healthcare Engineering Consultants
Issue: Chemical Waste Stream
Tips for Compliance:
Ensure disposal procedures for:
Chemicals
Chemotherapeutics
Radioactive materials
Medical waste and sharps
Waste phamaceuticals
Per applicable laws (OSHA, EPA, NRC, DOT)

Hazardous Materials and Wastes
Healthcare Engineering Consultants
Issue: Compressed Cylinder Storage
Tips for Compliance:
For stored gases <300 cubic feet in smoke compartment:
- Enclosures not required (NFPA 99, section 9.4.3)
For stored gases >300 but <3,000 cubic feet:
- Outdoors: enclosed space with doors or gates (9.4.2.1)
- Indoors: an enclosure with minimum ½ hour protection (9.4.2.3)
For stored gases >3,000 cubic feet:
- Walls, floors, ceilings, doors at least 1-hour rated (5.1.3.3.2)
- Racks, chains or fastenings to secure all cylinders (5.1.3.3.2)
- Continuous powered ventilation within 1 foot of floor (5.1.3.3.3)
Hazardous Materials and Wastes
Healthcare Engineering Consultants
Issue: Compressed Cylinder Storage
Tips for Compliance:
Requirements for stored gas only, not in-use tanks!
In-use gas includes:
- Tanks on code carts
- Tanks on wheelchairs
- Tanks on gurneys
Empty tanks do not count toward the total
Use of fire-rated cabinets can be used on floors

Hazardous Materials and Wastes
Healthcare Engineering Consultants
Issue: Alcohol-Based Hand Rub Units Requirements
Tips for Compliance:
Patient safety goal 7 requires CDC compliance with Category I recommendations, suggests Category II compliance!
When no soiling is present, ABHR units are recommended (Cat I)
ABHR is permitted in a corridor at least 6 feet in width, at least 4 feet apart, and not directly over electrical outlets (6 inches from dispenser)
ABHR dispensers can be used over carpeted surfaces only in sprinklered smoke compartments!
ABHR permissible volumes:
- 10 gallons in dispensers/ 5 gallons in storage per smoke compartment
- Maximum individual dispenser capacity: .3 gallons
- Maximum dispenser size per suite of rooms: .5 gallons

Hazardous Materials and Wastes
Healthcare Engineering Consultants
Issue: Eyewashes and Showers
Tips for Compliance:
Use risk assessment to determine placement
ANSI standards have not been officially adopted by the
Joint Commission
Testing policy is required – specify test intervals
Documentation of test results is required
Differentiate between eyewash station and “first aid”
station, such as mounted bottles

Hazardous Materials and Wastes
Healthcare Engineering Consultants
Issue: Hazardous Vapor Monitoring
Tips for Compliance:
Clinical lab: formaldehyde and xylene
Central supply: ethylene oxide
OR’s: nitrous oxide, methyl-methacrylate
Respiratory: glutaraldehyde
Sleep lab: collodion
Monitor and document per OSHA requirements!
Approved Changes for 2009
EMERGENCY
Healthcare Engineering Consultants
The organization of the standards :
EM.01.01.01: Plans for managing emergencies
EM.02.01.01: Develops an emergency operations plan
EM.02.02.01: Establishes emergency communication strategies
EM.02.02.03: Establishes strategies for managing resources
EM.02.02.05: Establishes strategies for managing safety and security
EM.02.02.07: Defines and manages staff roles and responsibilities
EM.02.02.09: Identifies an alternative means for providing utilities
EM.02.02.11: Identifies strategies for patient management
EM.02.02.13: Privileges to LIP’s
EM.02.02.15: Privileges to volunteer staff
EM.03.01.01: Annual effectiveness review
EM.03.01.03: Regularly tests the emergency operations plan

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
EM.01.01.01: The organization plans for managing the consequences of emergencies
Medical and clinical staff participate in planning
A Hazard Vulnerability Analysis (HVA) is performed and documented
The hazards are prioritized
Communication of emergency plan with community responders
Mitigation, Preparedness, Response, Recovery
Assets and resources are inventoried and documented (CAP)
Asset and resource inventories are monitored during emergencies (CAP)
The emergency management program is evaluated annually (S,O,P,E)

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Tips for Compliance with EM.01.01.01:
Appoint a physician and administrative representative to actively participate on the emergency management planning committee
Perform and document the Hazard Vulnerability Analysis (HVA) for all geographically separate facilities – review annually!
Be ready to describe the Mitigation, Preparedness, Response and Recovery procedures in the EOP
Ensure that emergency resources are inventoried (PPE, utility and medical supplies and pharmaceuticals) and monitored
Evaluate the emergency management program annually (S,O,P,E) and report the results to the safety committee

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
EM.02.01.01: The organization develops and maintains an Emergency Operations Plan (EOP)
Written EOP includes an “all hazards” command structure
An incident command structure (ICS) is established and is consistent with the community plan
The ICS identifies a reporting structure
Activation of ICS is identified
Activation of ICS phases is identified
The EOP identifies the organization response when community non-support may occur for up to 96 hours (CAP)
Alternative care sites are identified
Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Tips for Compliance with EM.02.01.01
Create a written emergency operations plan (EOP) that describes the incident command structure and process that is in use (HICS 4?) as well as how ICS integrates into the six critical core areas:
1. Emergency communications
2. Resources and assets
3. Safety and security
4. Staff roles and responsibilities
5. Management of utilities
6. Clinical and support activities
The EOP can either describe the ICS and core area integration in detail or reference existing documents

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Incident Commander
Public Info Officer
Liaison Officer
Safety Officer
Med/ Tech Specialist(s)
Operations Section Chief
Planning Section Chief
Logistics Section Chief
Finance/ Admin Section Chief
HICS Organizational Chart

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Tips for Compliance with EM.02.01.01
Create two color-coded timeline charts the indicate how long utilities will be operational and how long consumable supplies will be available in the event of an emergency in which no re-supply is possible
Ensure that decisions are made to determine whether any utility or supply changes will be implemented to extend “green zones”
Create two 96-hour plans that assume the following scenarios:
PLAN A: Supplies are available and are ordered and received
PLAN B: Internal supply shortages or utility failures require partial or
total patient evacuation
PLAN C: Shortages and/ or utilities are not sufficient to continue
normal patient care, although evacuation is not possible

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Critical Utilities and Supplies Timeline
Assume external help is not available
Create timeline for utilities and critical supplies, such as food and medications
Determine time-dependent status:
- Green: Continue all services as usual
- Yellow: Transition to conservation mode
- Red: Discontinue patient treatment, evacuate

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Utility Failure Operational Impact Chart
Hours after utility failure 0 8 16 24 32 40 48 56 64 72 80 88 96 Normal power failure Emergency power failure Water pressure low Entire loss of water pressure Loss of steam generation (winter) Loss of steam generation (summer) Loss of natural gas Loss of propane Chiller failure (winter) Chiller failure (summer) Major air handler failure Failure of sewage system Sump pump failure Loss of bulk oxygen Loss of medical air Loss of bulk nitrous oxide Loss of medical vacuum Computer server failure Telephone switch failure Failure of elevators Pneumatic tube system failure

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Consumable Supply Operational Impact Chart
Hours after emergency occurs 0 8 16 24 32 40 48 56 64 72 80 88 96 Fuel oil (winter) Fuel oil (summer) Gasoline Propane fuel Natural gas Potable water Non-potable water Oxygen Medical air Nitrous Oxide Nitrogen Nutrition supplies Pharmaceutical supplies IV solutions Pharmaceutical medications General patient supplies Surgical supplies Environmental cleaning supplies Central sterile supplies General office supplies

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
EM.02.02.01: The organization establishes emergency
communications strategies Staff notification procedures are created
Provisions for ongoing staff communication during the emergency
Process to notify external authorities
Communication with patients and their families
Communication with the community and media
Communication with vendors and suppliers (CAP)
Sharing information with other health care providers
Providing information about patients to third-parties (FEMA, CDC, etc.)
Communication with alternative care sites
Establishment of back-up communication systems and technologies

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Tips for Compliance with EM.02.02.01
Create notification charts with phone numbers, email addresses, etc.
Include for staff, external authorities, community, media, vendors
Determine what information will be shared with other health care providers in the area
Ensure that liaisons are established with government agencies
Verify that MOU’s for alternative care sites are updated
Establish and check operation of back-up communication systems, such as the internet, cell phones, two-way radios, emergency land lines, and amateur radio operators

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
EM.02.02.03: The organization establishes strategies for managing
resources and assets during emergencies
Plans for obtaining medications and non-clinical supplies
Replenishing medical supplies and equipment during the emergency
Replenishing pharmaceutical supplies
Replenishing non-medical supplies (food, water, fuel, linens, etc.)
Managing staff and family support activities
Sharing of resources with other health care organizations in and outside of the local community (CAP)
Horizontal, vertical and total evacuation (CAP), including transportation of patients, medications, equipment, staff and medical record information

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Tips for Complying with EM.02.02.03
Plans should be in place to stockpile and reorder critical clinical and non-clinical supplies
Written procedures should describe how the needs of staff and families of staff will be met during an emergency
A plan to share community resources and assets should be in place
A practical patient evacuation plan that includes horizontal and vertical movement within the facility as well as partial or total evacuation outside of the facility is required
Logistics for evacuation should include: 1) transportation; 2) staffing; 3) medications; 4) equipment, and; 5) the medical record

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
EM.02.02.05: The organization establishes strategies for managing
safety and security during emergencies
Internal safety and security measures are established
Role of community security agencies is established with the healthcare organization and means of coordination is identified (CAP)
Processes for handling hazardous materials and waste are developed (CAP)
Plans are developed for radioactive, biological, chemical decontamination
Patients susceptible to wandering are identified (CAP)
Access into and out of the facility are controlled
Movement of staff and patients is controlled within the facility
Traffic accessing the facility is controlled

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Tips for Complying with EM.02.02.05
Security staffing plans during emergencies must be established
Expectations with outside police agencies should be identified
Plans to dispose of infectious and hazardous waste must be created
Procedures to treat contaminated patients must be written (radioactive, biological and chemical)
Methods to lock down the facility to prevent entry must be provided
Methods to minimize staff and patients from leaving the facility must be planned
Plans must be in place to control traffic accessing the facility

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
EM.02.02.07: The organization defines and manages staff roles and responsibilities
Staff roles and responsibilities are defined for the critical areas (communications, resources and assets, safety and security, utilities, clinical activities)
Staff are trained relative to their responsibilities (CAP)
Roles of LIP’s are specifically defined (CAP)
Care providers and command center staff are identified (ID badges, vests, caps, etc.)

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Tips for Complying with EM.02.02.07
Review and update as necessary, the ICS organizational chart and job action sheets (check after each drill)
Ensure that hospital staff have participated in NIMS training
Discuss emergency expectations with the independent physicians who have privileges at the hospital
Select the primary and back-up command center locations
Have a method to identify incident command staff (ID badges, vests, caps, etc.)

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
EM.02.02.09: The organization establishes strategies for managing utilities during emergencies, such as:
Electricity
Potable and non-potable water
Fuel for building operations or transport vehicles (CAP)
Other essential utility needs, such as:
- HVAC equipment
- Medical gas and vacuum systems
- Fire systems
- Sewer

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Tips for Complying with EM.02.02.09
Complete the utility 96-hour timeline chart
Determine which utilities require additional supplies, especially water and fuel
Determine the feasibility of redundant systems or supplies
Examples: Water – on-site well, water tower or nearby lake
Electricity – additional generators installed
Boilers – portable boiler “on a truck”
Medical gas – low pressure external connection, manifold

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
EM.02.02.11: The organization establishes strategies for managing
clinical and support activities during emergencies, including:
Patient scheduling, triage, assessment, treatment admission, transfer, discharge and evacuation
Clinical services for vulnerable patients, such as: pediatric, geriatric, disabled or serious chronic conditions or addictions
Personal hygiene and sanitation
Mental health needs (CAP)
Mortuary services (CAP)
Tracking and documenting patient information (CAP)
Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Tips for Complying with EM.02.02.11
Identify which patients in the hospital are considered “vulnerable”
(neonatal intensive, pediatric, geriatric, dementia, behavioral health)
Plan for patient and staff hygiene and sanitation without water or sewer
Determine mortuary needs in the event of a pandemic
Evaluate back-up methods to track patient information in the event that
the electronic information system fails

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
EM.02.02.13: During disasters, the organization may grant privileges
to licensed independent practitioners
Privileges granted only when EOP has been activated
Medical staff bylaws indicate to who and how to grant privileges, and policies will indicate how performance will be evaluated
Minimum privileging requirements include:
1. Current picture ID and license to practice
2. Must be a member of a recognized disaster response group
3. Proof of government authority to provide services during a disaster
Hospital determines within 72 hours if privileges should continue

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
EM.02.02.15: During disasters, the organization may assign disaster
responsibilities to volunteer practitioners
Hospital assigns responsibilities only when EOP has been activated
Hospital identifies in writing who is eligible and how to assign disaster responsibilities to non-LIP’s
Minimum requirements to assist during disasters include:
1. Current picture ID and license to practice professional specialty
2. Must be a member of a recognized disaster response group
3. Confirmation by hospital staff the individual is qualified
Hospital determines a method to evaluate performance and decide within 72 hours if responsibilities should continue

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
EM.03.01.01: The organization evaluates the effectiveness of its
emergency management planning activities
The Hazard Vulnerability Analysis (HVA) is evaluated annually to determine if revisions are necessary
The Emergency Operations Plan (EOP) is evaluated annually with regard to the Scope, Objectives, Performance and Effectiveness of the program
The hospital conducts an annual review of the inventory process with regard to emergency supplies, and documents the results

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
EM.03.01.03: The organization regularly tests its emergency
operation plan
Twice over 12 months, either as a drill or actual emergency
Once per year in a business occupancy
One “influx of patient” drill per year
One escalation per year to test community “non-support”
One “community-wide” drill per year
Drills are realistic and based on the HVA
A dedicated, trained individual must evaluate the drill

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
EM.03.01.03: The organization regularly tests its emergency
operation plan (continued)
The six critical areas are monitored: 1) Communication; 2) Resource mobilization; 3) Safety and security; 4) Staff roles and responsibilities; 5) Utility systems, and; 6) Patient clinical and support activities
Exercises are critiqued with a multi-disciplinary group, including leadership, physician and support staff and evaluate deficiencies
The operations plan is revised based on the drill findings
Subsequent exercises evaluate the improvements to the EOP
Drill evaluations are reported to the hospital safety committee

Emergency Management
EMERGENCY
Healthcare Engineering Consultants
Tips for Compliance with EM.03.01.03
Two drills per rolling 12-month period should be performed, based on the HVA
At least one drill per 12 months in a business occupancy
At least one “influx” drill for a disaster receiving station
Community-wide and influx drills can be performed concurrently
The community 96-hour “non-support” drill can be a tabletop
Trained staff, including a physician and leadership, must evaluate the drill and must document the six core areas in the evaluation
Infant abduction (EC.2.10) and patient surge (IC.6.10) drills are highly
recommended

Fire Prevention
Healthcare Engineering Consultants
Issue: Fire Drills
Tips for Compliance:
Healthcare and ambulatory:
1 drill per shift per quarter
Business occupancy:
1 drill per shift per year
Drill monitoring as defined in the plan
Evaluate effectiveness annually in written report

Fire Prevention
Healthcare Engineering Consultants
Issue: Interim Life Safety Measures
Tips for Compliance:
A policy must describe the program
Document whether ILSM is or is not required
Determine ILSM applicability for PFI’s!
Document which measures are applicable
Document required inspections
Failure to meet ILSM provisions: CON04!

Medical Equipment Management
Healthcare Engineering Consultants
Issue: Equipment Test Scoring
Tips for Compliance:
100% PM completion for “life support” devices, based on scoring (A)
90% PM completion for “non-life support” devices (C)
Determine test interval by “PM effectiveness” and MTBF data
Test tags with due dates recommended, but not required! What about Ongoing PM vs. initial test only?

Medical Equipment Management
Healthcare Engineering Consultants
Issue: Other Medical Equipment Issues
Tips for Compliance:
Patient-owned equipment
Diagnostic and therapeutic (example: CPAP)
Personal use (iPods, cell phones, blackberries)
Rental devices
Demo, loaner and trial equipment
Radio-frequency interference

Utility Systems Management
Healthcare Engineering Consultants
Issue: Waterborne Pathogens
Tips for Compliance:
Waterborne pathogens policy must include:
1. Patient risk assessment for pathogen
vulnerability
2. Operational description of measures to reduce
waterborne pathogens
3. Remediation procedures if hospital-acquired
waterborne infection is determined

Utility Systems Management
Healthcare Engineering Consultants
Issue: Airborne Pathogens
Tips for Compliance:
An airborne pathogens policy must exist that describes:
Air filter maintenance, room air exchange rate and pressure relationships for operating rooms, delivery rooms, special procedure rooms, patient isolation rooms, clinical laboratories, sterile supply rooms and pharmacies
Note: Refer to AIA document for requirements
Note: “Grandfathering” permitted for air handlers

Utility Systems Management
Healthcare Engineering Consultants
Issue: Utility System Test Scoring
Tips for Compliance:
All devices included in the utility systems management program must be at least initially tested
Expected PM completion rate for “critical life support” and “critical infection control” components based on “A” scoring: 100%
Expected PM completion rate for “critical non-life support” components based on “C” scoring: 90%
“Non-critical” components are not scored

Appropriate Environment
Healthcare Engineering Consultants
Issue: The “General Duty Clause”
Tips for Compliance:
Patient areas are safe, clean, comfortable
Lighting is suitable
Ventilation provides for acceptable temperature
Locks and restraints per regulation
Emergency access for locked spaces

Appropriate Environment
Healthcare Engineering Consultants
Issue: New Construction
Tips for Compliance:
AIA document, 2001 edition (2006 soon?)
Applicable federal, state or local
guidelines
Equivalent design criteria

Appropriate Environment
Healthcare Engineering Consultants
Issue: Pre-Construction Risk Assessment (PCRA)
Tips for Compliance: Include all of the items listed below in the PCRA evaluation
Noise
Vibration
Air quality
Infection control
Emergency procedures
Utility failures
Interim life safety measures

Infection Control Risk Assessment (ICRA)
Healthcare Engineering Consultants
Risk Criteria for Infection Control
Type A Type B Type C Type D
Group 1 (lowest) I II II III
Group 2 (medium) I II III IV
Group 3 (medium high) II III III IV
Group 4 (highest)
III
III IV IV
Construction TypePatient
Risk

Appropriate Environment
Healthcare Engineering Consultants
Issue: Ongoing Monitoring
Tips for Compliance:
• Controls include measures to reduce risk and minimize the impact of the construction activities
• Daily monitoring checklist is recommended
• Consider posting required PCRA permits, such as hot work, ICRA, above-the-ceiling work, etc. on door entrance to construction area