Embed Size (px)
Citation preview

Part 11: Pediatric Basic Life Support andCardiopulmonary Resuscitation Quality2015 American Heart Association GuidelinesUpdate for Cardiopulmonary Resuscitation andEmergency Cardiovascular Care (Reprint)
Reprint: The American Heart Association requests that this document becited as follows: Atkins DL, Berger S, Duff JP, Gonzales JC, Hunt EA, JoynerBL, Meaney PA, Niles DE, Samson RA, Schexnayder SM. Part 11: pediatricbasic lifesupportandcardiopulmonaryresuscitationquality: 2015AmericanHeart AssociationGuidelinesUpdate forCardiopulmonaryResuscitationandEmergency Cardiovascular Care. Circulation. 2015;132(suppl 2):S519–S525.
Reprinted with permission of the American Heart Association, Inc. Thisarticle has been published in Circulation.
INTRODUCTION
This 2015 American Heart Association (AHA) Guidelines Update forCardiopulmonary Resuscitation (CPR) and Emergency CardiovascularCare (ECC) section on pediatric basic life support (BLS) differs sub-stantially from previous versions of the AHA Guidelines.1 This publica-tion updates the 2010 AHA Guidelines on pediatric BLS for several keyquestions related to pediatric CPR. The Pediatric ILCOR Task Forcereviewed the topics covered in the 2010 International Consensus onCardiopulmonary Resuscitation and Emergency Cardiovascular CareScience With Treatment Recommendations and the 2010 council-specificguidelines for CPR and ECC (including those published by the AHA) andformulated 3 priority questions to address for the 2015 systematicreviews. In the online version of this document, live links are provided sothe reader can connect directly to those systematic reviews on the In-ternational Liaison Committee on Resuscitation (ILCOR) Scientific Evi-dence Evaluation and Review System (SEERS) website. These links areindicated by a superscript combination of letters and numbers (eg, Peds709). We encourage readers to use the links and review the evidence andappendices.
A rigorous systematic review process was undertaken to review therelevant literature to answer those questions, resulting in the 2015International Consensus on CPR and ECC Science With Treatment Rec-ommendations, “Part 6: Pediatric Basic Life Support and Pediatric Ad-vanced Life Support.”2,3 This 2015 Guidelines Update covers only thosetopics reviewed as part of the 2015 systematic review process. Otherrecommendations published in the 2010 AHA Guidelines remain theofficial recommendations of the AHA ECC scientists (see Appendix).When making AHA treatment recommendations, we used the AHA Classof Recommendation and Level of Evidence (LOE) systems. This update
AUTHORS: Dianne L. Atkins, Chair; Stuart Berger;Jonathan P. Duff; John C. Gonzales; Elizabeth A. Hunt;Benny L. Joyner; Peter A. Meaney; Dana E. Niles; Ricardo A.Samson; and Stephen M. Schexnayder
KEY WORDSautomated external defibrillator n cardiopulmonaryresuscitation n pediatrics
www.pediatrics.org/cgi/doi/10.1542/peds.2015-3373E
doi:10.1542/peds.2015-3373E
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
(Circulation. 2015;132[suppl 2]:S519–S525. DOI: 10.1161/CIR.0000000000000265.)
Copyright © 2015 American Heart Association, Inc.
PEDIATRICS Volume 136, Supplement 2, November 2015 S167
SUPPLEMENT ARTICLE
by guest on May 5, 2018http://pediatrics.aappublications.org/Downloaded from

uses the newest AHA Class of Recom-mendation and LOE classification sys-tem, which contains modifications ofthe Class III recommendation and intro-duces LOE B-R (randomized studies) andB-NR (nonrandomized studies) as wellas LOE C-LD (limited data) and LOE C-EO(consensus of expert opinion).
Outcomes from pediatric in-hospitalcardiac arrest (IHCA) have markedly im-proved over the past decade. From 2001to 2009, rates of pediatric IHCA survival tohospital discharge improved from 24%to 39%.4 Recent unpublished 2013 datafrom the AHA’s Get With The Guidelines®-Resuscitation program observed 36%survival to hospital discharge for pediat-ric IHCA (Paul S. Chan, MD, personal com-munication, April 10, 2015). ProlongedCPR is not always futile, with 12%of patients who receive CPR for morethan 35 minutes surviving to dischargeand 60% of those survivors having afavorable neurologic outcome.5
Unlike IHCA, survival from out-of-hospitalcardiacarrest (OHCA) remainspoor.Datafrom 2005 to 2007 from the ResuscitationOutcomesConsortium, a registry of 11USand Canadian emergency medical sys-tems, showed age-dependent dischargesurvival ratesof3.3%for infants(youngerthan 1 year), 9.1% for children (1 to11years), and8.9%foradolescents (12 to19 years).6 More recently published datafrom this network demonstrate 8.3%survival to hospital discharge across allage groups.7
For the purposes of these guidelines:
� Infant BLS guidelines apply to infantsyounger than approximately 1 yearof age.
� Child BLS guidelines apply to chil-dren approximately 1 year of ageuntil puberty. For teaching purpo-ses, puberty is defined as breastdevelopment in females and thepresence of axillary hair in males.
� Adult BLS guidelines apply at andbeyond puberty (see “Part 5: Adult
Basic Life Support and Cardiopulmo-nary Resuscitation Quality” in thissupplement regarding the use ofthe automated external defibrillator(AED) and methods to achieve high-quality CPR).
The following subjects are addressedin this 2015 pediatric BLS guidelinesupdate:
� Pediatric BLS Healthcare ProviderPediatric Cardiac Arrest Algorithmsfor a single rescuer and for 2 ormore rescuers
� The sequence of compressions, air-way, breathing (C-A-B) versus airway,breathing, compressions (A-B-C)
� Chest compression rate and depth
� Compression-only (Hands-Only) CPR
Pediatric Advanced Life Support topicsreviewed by the ILCOR Pediatric TaskForce are covered in “Part 12: PediatricAdvanced Life Support.”
ALGORITHMS
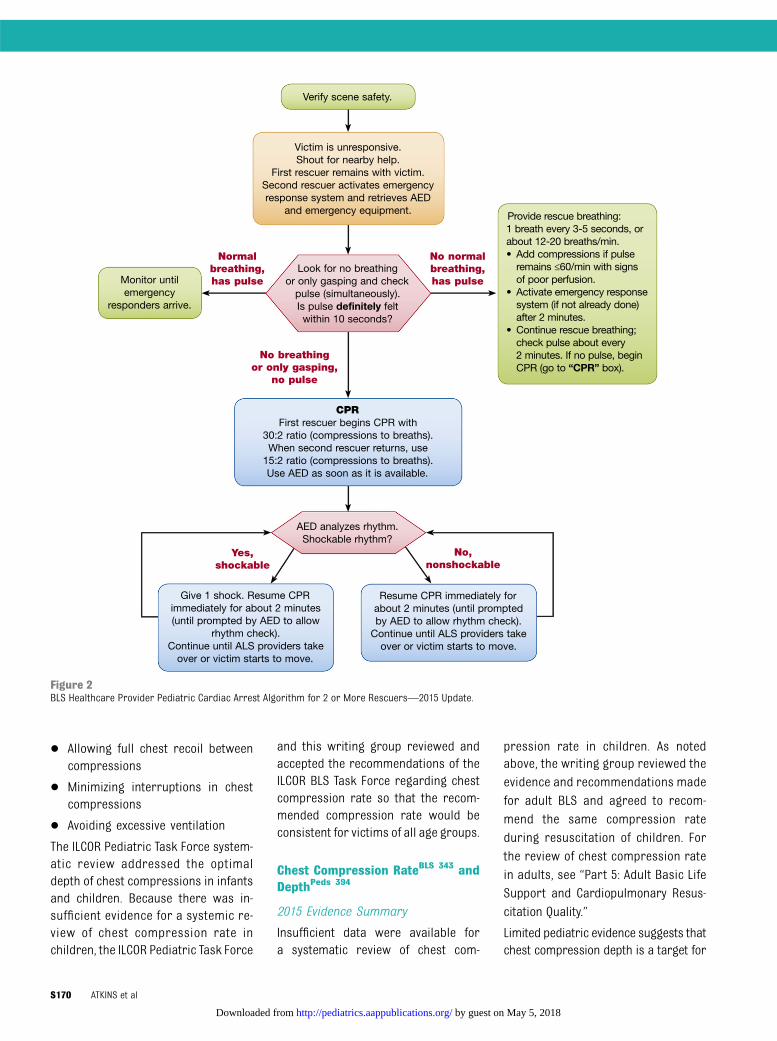
Algorithms for 1- and 2-person health-care provider CPR have been separatedto better guide rescuers through theinitial stages of resuscitation (Figures 1and 2). In an era where cellular tele-phones with speakers are common, thistechnology can allow a single rescuer toactivate the emergency response sys-tem while beginning CPR. These algo-rithms continue to emphasize the highpriority for obtaining an AED quickly ina sudden, witnessed collapse, becausesuch an event is likely to have a cardiacetiology.
SEQUENCE OF CPR
C-A-B Versus A-B-CPeds 709
Historically, the preferred sequenceof CPR was A-B-C (Airway-Breathing-Compressions). The 2010 AHA Guide-lines recommended a change to theC-A-B sequence (Compressions-Airway-Breathing) to decrease the time toinitiation of chest compressions and
reduce “no blood flow” time. The 2015ILCOR systematic review addressed evi-dence to support this change.2,3
Pediatric cardiac arrest has inherentdifferences when compared with adultcardiac arrest. In infants and children,asphyxial cardiac arrest is more com-monthancardiacarrest fromaprimarycardiac event; therefore, ventilationmay have greater importance duringresuscitation of children. Data fromanimal studies8,9 and 2 pediatric stud-ies10,11 suggest that resuscitation out-comes for asphyxial arrest are betterwith a combination of ventilation andchest compressions.
Manikin studies demonstrated thatstarting CPR with 30 chest com-pressions followed by 2 breaths delaysthe first ventilation by 18 seconds fora single rescuer and less (by about 9seconds or less) for 2 rescuers. A uni-versal CPR algorithm for victims ofall ages minimizes the complexity ofCPR and offers consistency in teach-ing CPR to rescuers who treat infants,children, or adults. Whether resus-citation beginning with ventilations(A-B-C) or with chest compressions(C-A-B) impacts survival is unknown.To increase bystander CPR rates aswell as knowledge and skill retention,the use of the same sequence forinfants and children as for adults haspotential benefit.
2015 Evidence Summary
Nohumanstudieswithclinicaloutcomeswere identified that compared C-A-B andA-B-C approaches for initial manage-ment of cardiac arrest. The impact oftime to first chest compression for C-A-Bversus A-B-C sequence has been evalu-ated. Adult12,13 and pediatric14 manikinstudies showed a significantly reducedtime to first chest compression withthe use of a C-A-B approach comparedwith an A-B-C approach. Data from 2 ofthese 3 studies demonstrated that timeto first ventilation is delayed by only
S168 ATKINS et al
by guest on May 5, 2018http://pediatrics.aappublications.org/Downloaded from

approximately 6 seconds when usinga C-A-B sequence compared with anA-B-C sequence.12,14
2015 Recommendation—New
Because of the limited amount andquality of the data, it may be reasonable
to maintain the sequence from the2010 Guidelines by initiating CPR withC-A-B over A-B-C sequence (Class IIb,LOE C-EO). Knowledge gaps exist, andspecific research is required to ex-amine the best approach to initiatingCPR in children.
COMPONENTS OF HIGH-QUALITY CPR
The 5 components of high-quality CPR are
� Ensuring chest compressions ofadequate rate
� Ensuring chest compressions ofadequate depth
Figure 1BLS Healthcare Provider Pediatric Cardiac Arrest Algorithm for the Single Rescuer—2015 Update.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 2, November 2015 S169
by guest on May 5, 2018http://pediatrics.aappublications.org/Downloaded from
� Allowing full chest recoil betweencompressions
� Minimizing interruptions in chestcompressions
� Avoiding excessive ventilation
The ILCOR Pediatric Task Force system-atic review addressed the optimaldepth of chest compressions in infantsand children. Because there was in-sufficient evidence for a systemic re-view of chest compression rate inchildren, the ILCOR Pediatric Task Force
and this writing group reviewed andaccepted the recommendations of theILCOR BLS Task Force regarding chestcompression rate so that the recom-mended compression rate would beconsistent for victims of all age groups.
Chest Compression RateBLS 343 andDepthPeds 394
2015 Evidence Summary
Insufficient data were available fora systematic review of chest com-
pression rate in children. As notedabove, the writing group reviewed theevidence and recommendations madefor adult BLS and agreed to recom-mend the same compression rateduring resuscitation of children. Forthe review of chest compression ratein adults, see “Part 5: Adult Basic LifeSupport and Cardiopulmonary Resus-citation Quality.”
Limited pediatric evidence suggests thatchest compression depth is a target for
Figure 2BLS Healthcare Provider Pediatric Cardiac Arrest Algorithm for 2 or More Rescuers—2015 Update.
S170 ATKINS et al
by guest on May 5, 2018http://pediatrics.aappublications.org/Downloaded from
improving resuscitation. One observa-tional study demonstrated that chestcompression depth is often inadequateduring pediatric cardiac arrest.15 Adultdata have demonstrated the importanceof adequate chest compression depth tothe outcome of resuscitation,16 but suchdata in children are very limited. A caseseries of 6 infants with heart diseaseexamined blood pressure during CPR inrelation to chest compression depthand observed a higher systolic bloodpressure during CPR in association withefforts to increase chest compressiondepth.17 Another report of 87 pediatricresuscitation events, most involvingchildren older than 8 years, found thatcompression depth greater than 51 mmfor more than 60% of the compressionsduring 30-second epochs within the first5minuteswas associatedwith improved24-hour survival.18
2015 Recommendations—New
For simplicity in CPR training, in theabsence of sufficient pediatric evi-dence, it is reasonable to use the adultBLS-recommended chest compressionrate of 100/min to 120/min for infantsand children (Class IIa, LOE C-EO). Al-though the effectiveness of CPR feed-back devices was not reviewed by thiswriting group, the consensus of thegroup is that the use of feedback de-vices likely helps the rescuer optimizeadequate chest compression rate anddepth, and we suggest their use when
available (Class IIb, LOE C-EO; see also“Part 14: Education”).
It is reasonable that for pediatricpatients (birth to the onset of puberty)rescuers provide chest compressionsthat depress the chest at least one thirdthe anterior-posterior diameter of thechest. This equates to approximately1.5 inches (4 cm) in infants to 2 inches(5 cm) in children (Class IIa, LOE C-LD).Once children have reached puberty,the recommended adult compres-sion depth of at least 5 cm, but nomore than 6 cm, is used for the ado-lescent of average adult size (Class I,LOE C-LD).16
Compression-Only CPRPeds 414
The 2015 ILCOR pediatric systematic re-view addressed the use of compression-only CPR for cardiac arrest in infantsand children. Compression-only CPRis an alternative for lay rescuer CPR inadults.
2015 Evidence Summary
In a large observational study examin-ing data from a Japanese nationalregistry of pediatric OHCA, the use ofcompression-only CPR,whencomparedwith conventional CPR, was associatedwith worse 30-day intact neurologicsurvival.10 When analyzed by arrestetiology, although the numbers aresmall, in patients with presumed non-asphyxial arrest (ie, a presumed arrestof cardiac etiology), compression-only
CPR was as effective as conventionalCPR. However, in patients with presumedasphyxial cardiac arrest, outcomes aftercompression-only CPR were no betterthan those for patients receiving no by-stander CPR.
A second large observational studyusing a more recent data set fromthe sameJapanese registry examinedthe effect of dispatcher-assisted CPRin pediatric OHCA. In this study, theuse of compression-only CPR wasassociated with worse 30-day intactneurologic survival compared withpatients who received conventionalCPR.11 Although not stratified foretiology of arrest, outcomes aftercompression-only CPR were no betterthan for patients who received no by-stander CPR.
2015 Recommendations—New
Conventional CPR (chest compres-sions and rescue breaths) should beprovided for pediatric cardiac arrests(Class I, LOE B-NR). The asphyxial na-ture of the majority of pediatric car-diac arrests necessitates ventilationas part of effective CPR. However,because compression-only CPR iseffective in patients with a primarycardiac event, if rescuers are un-willing or unable to deliver breaths,we recommend rescuers performcompression-only CPR for infants andchildren in cardiac arrest (Class I,LOE B-NR).
REFERENCES
1. Berg MD, Schexnayder SM, Chameides L, TerryM, Donoghue A, Hickey RW, Berg RA, SuttonRM, Hazinski MF. Part 13: pediatric basic lifesupport: 2010 American Heart AssociationGuidelines for Cardiopulmonary Resuscitationand Emergency Cardiovascular Care. Circula-tion. 2010;122(suppl 3):S862–S875. doi: 10.1161/CIRCULATIONAHA.110.971085.
2. de Caen AR, Maconochie IK, Aickin R, AtkinsDL, Biarent D, Guerguerian AM, KleinmanME, Kloeck DA, Meaney PA, Nadkarni VM, NgKC, Nuthall G, Reis AG, Shimizu N, Tibballs J,
Veliz Pintos R; on behalf of the PediatricBasic Life Support and Pediatric AdvancedLife Support Chapter Collaborators. Part 6:pediatric basic life support and pediatricadvanced life support: 2015 InternationalConsensus on Cardiopulmonary Resusci-tation and Emergency Cardiovascular CareScience With Treatment Recommendations.Circulation. 2015;132 (suppl 1):S177–S203.doi: 10.1161/CIR.0000000000000275.
3. Maconochie IK, de Caen AR, Aickin R, AtkinsDL, Biarent D, Guerguerian AM, Kleinman
ME, Kloeck DA, Meaney PA, Nadkarni VM,Ng KC, Nuthall G, Reis AG, Shimizu N,Tibballs J, Veliz Pintos R; on behalf of thePediatric Basic Life Support and PediatricAdvanced Life Support Chapter Collabo-rators. Part 6: pediatric basic life supportand pediatric advanced life support: 2015International Consensus on Cardiopulmo-nary Resuscitation and Emergency Car-diovascular Care Science With TreatmentRecommendations. Resuscitation. 2015. Inpress.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 2, November 2015 S171
by guest on May 5, 2018http://pediatrics.aappublications.org/Downloaded from

4. Girotra S, Spertus JA, Li Y, Berg RA, NadkarniVM, Chan PS; American Heart AssociationGet With The Guidelines–Resuscitation In-vestigators. Survival trends in pediatric in-hospital cardiac arrests: an analysis fromGet With The Guidelines-Resuscitation. CircCardiovasc Qual Outcomes. 2013;6:42–49.doi: 10.1161/CIRCOUTCOMES.112.967968.
5. Matos RI, Watson RS, Nadkarni VM, HuangHH, Berg RA, Meaney PA, Carroll CL, BerensRJ, Praestgaard A, Weissfeld L, Spinella PC;American Heart Association’s Get With TheGuidelines–Resuscitation (Formerly the NationalRegistry of Cardiopulmonary Resuscitation)Investigators. Duration of cardiopulmonaryresuscitation and illness category impactsurvival and neurologic outcomes for in-hospital pediatric cardiac arrests. Circulation.2013;127:442–451. doi: 10.1161/CIRCULATIONAHA.112.125625.
6. Atkins DL, Everson-Stewart S, Sears GK,Daya M, Osmond MH, Warden CR, Berg RA;Resuscitation Outcomes Consortium Inves-tigators. Epidemiology and outcomes fromout-of-hospital cardiac arrest in children: theResuscitation Outcomes Consortium Epistry-Cardiac Arrest. Circulation. 2009;119:1484–1491. doi: 10.1161/CIRCULATIONAHA.108.802678.
7. Sutton RM, Case E, Brown SP, Atkins DL,Nadkarni VM, Kaltman J, Callaway C, IdrisA, Nichol G, Hutchison J, Drennan IR, AustinM, Daya M, Cheskes S, Nuttall J, Herren H,Christenson J, Andrusiek D, Vaillancourt C,Menegazzi JJ, Rea TD, Berg RA; ROC In-vestigators. A quantitative analysis ofout-of-hospital pediatric and adolescent re-suscitation quality - A report from the ROCepistry-cardiac arrest. Resuscitation. 2015;93:150–157. doi 10.1016/j.resuscitation.2015.04.010.
8. Berg RA, Hilwig RW, Kern KB, Babar I, EwyGA. Simulated mouth-to-mouth ventilation
and chest compressions (bystander cardio-pulmonary resuscitation) improves outcomein a swine model of prehospital pediatricasphyxial cardiac arrest. Crit Care Med.1999;27:1893–1899.
9. Yannopoulos D, Matsuura T, McKnite S,Goodman N, Idris A, Tang W, Aufderheide TP,Lurie KG. No assisted ventilation cardiopul-monary resuscitation and 24-hour neurolog-ical outcomes in a porcine model of cardiacarrest. Crit Care Med. 2010;38:254–260. doi:10.1097/CCM.0b013e3181b42f6c.
10. Kitamura T, Iwami T, Kawamura T, Nagao K,Tanaka H, Nadkarni VM, Berg RA, Hiraide A;implementation working group for All-Japan Utstein Registry of the Fire and Di-saster Management Agency. Conventionaland chest-compression-only cardiopulmo-nary resuscitation by bystanders for childrenwho have out-of-hospital cardiac arrests:a prospective, nationwide, population-based cohort study. Lancet. 2010;375:1347–1354. doi: 10.1016/S0140-6736(10)60064-5.
11. Goto Y, Maeda T, Goto Y. Impact ofdispatcher-assisted bystander cardiopul-monary resuscitation on neurological out-comes in children with out-of-hospitalcardiac arrests: a prospective, nationwide,population-based cohort study. J Am HeartAssoc. 2014;3:e000499. doi: 10.1161/JAHA.113.000499.
12. Marsch S, Tschan F, Semmer NK, Zobrist R,Hunziker PR, Hunziker S. ABC versus CABfor cardiopulmonary resuscitation: a pro-spective, randomized simulator-based trial.Swiss Med Wkly. 2013;143:w13856. doi:10.4414/smw.2013.13856.
13. Sekiguchi H, Kondo Y, Kukita I. Verificationof changes in the time taken to initiatechest compressions according to modifiedbasic life support guidelines. Am J Emerg
Med. 2013;31:1248–1250. doi: 10.1016/j.ajem.2013.02.047.
14. Lubrano R, Cecchetti C, Bellelli E, Gentile I,Loayza Levano H, Orsini F, Bertazzoni G,Messi G, Rugolotto S, Pirozzi N, Elli M.Comparison of times of intervention duringpediatric CPR maneuvers using ABC andCAB sequences: a randomized trial. Resus-citation. 2012;83:1473–1477. doi: 10.1016/j.resuscitation.2012.04.011.
15. Sutton RM, Wolfe H, Nishisaki A, LeffelmanJ, Niles D, Meaney PA, Donoghue A, MalteseMR, Berg RA, Nadkarni VM. Pushing harder,pushing faster, minimizing interruptions…but falling short of 2010 cardiopulmonaryresuscitation targets during in-hospital pe-diatric and adolescent resuscitation. Resus-citation. 2013;84:1680–1684. doi: 10.1016/j.resuscitation.2013.07.029.
16. Kleinman ME, Brennan EE, Goldberger ZD,Swor RA, Terry M, Bobrow BJ, Gazmuri RJ,Travers AH, Rea T. Part 5: adult basic lifesupport and cardiopulmonary resuscita-tion quality: 2015 American Heart Associa-tion Guidelines Update for CardiopulmonaryResuscitation and Emergency Cardiovas-cular Care. Circulation. 2015;132(suppl 2):S414–S435.
17. Maher KO, Berg RA, Lindsey CW, Simsic J,Mahle WT. Depth of sternal compressionand intra-arterial blood pressure duringCPR in infants following cardiac surgery.Resuscitation. 2009;80:662–664. doi: 10.1016/j.resuscitation.2009.03.016.
18. Sutton RM, French B, Niles DE, Donoghue A,Topjian AA, Nishisaki A, Leffelman J, Wolfe H,Berg RA, Nadkarni VM, Meaney PA. 2010American Heart Association recommendedcompression depths during pediatric in-hospital resuscitations are associated withsurvival. Resuscitation. 2014;85:1179–1184.doi: 10.1016/j.resuscitation.2014.05.007.
S172 ATKINS et al
by guest on May 5, 2018http://pediatrics.aappublications.org/Downloaded from
DISCLOSURES
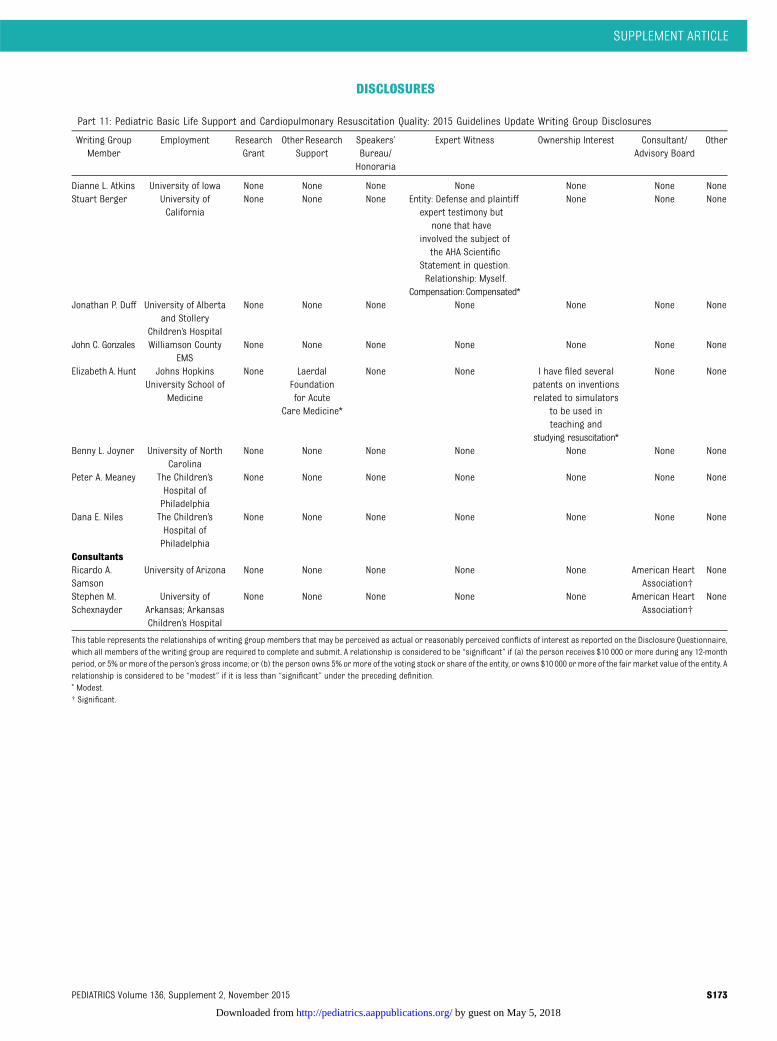
Part 11: Pediatric Basic Life Support and Cardiopulmonary Resuscitation Quality: 2015 Guidelines Update Writing Group Disclosures
Writing GroupMember
Employment ResearchGrant
Other ResearchSupport
Speakers’Bureau/Honoraria
Expert Witness Ownership Interest Consultant/Advisory Board
Other
Dianne L. Atkins University of Iowa None None None None None None NoneStuart Berger University of
CaliforniaNone None None Entity: Defense and plaintiff
expert testimony butnone that have
involved the subject ofthe AHA Scientific
Statement in question.Relationship: Myself.
Compensation: Compensated*
None None None
Jonathan P. Duff University of Albertaand Stollery
Children’s Hospital
None None None None None None None
John C. Gonzales Williamson CountyEMS
None None None None None None None
Elizabeth A. Hunt Johns HopkinsUniversity School of
Medicine
None LaerdalFoundationfor Acute
Care Medicine*
None None I have filed severalpatents on inventionsrelated to simulators
to be used inteaching and
studying resuscitation*
None None
Benny L. Joyner University of NorthCarolina
None None None None None None None
Peter A. Meaney The Children’sHospital ofPhiladelphia
None None None None None None None
Dana E. Niles The Children’sHospital ofPhiladelphia
None None None None None None None
ConsultantsRicardo A.Samson
University of Arizona None None None None None American HeartAssociation†
None
Stephen M.Schexnayder
University ofArkansas; ArkansasChildren’s Hospital
None None None None None American HeartAssociation†
None
This table represents the relationships of writing group members that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure Questionnaire,which all members of the writing group are required to complete and submit. A relationship is considered to be “significant” if (a) the person receives $10 000 or more during any 12-monthperiod, or 5% ormore of the person’s gross income; or (b) the person owns 5% ormore of the voting stock or share of the entity, or owns $10 000 or more of the fair market value of the entity. Arelationship is considered to be “modest” if it is less than “significant” under the preceding definition.* Modest.† Significant.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 2, November 2015 S173
by guest on May 5, 2018http://pediatrics.aappublications.org/Downloaded from
APPENDIX
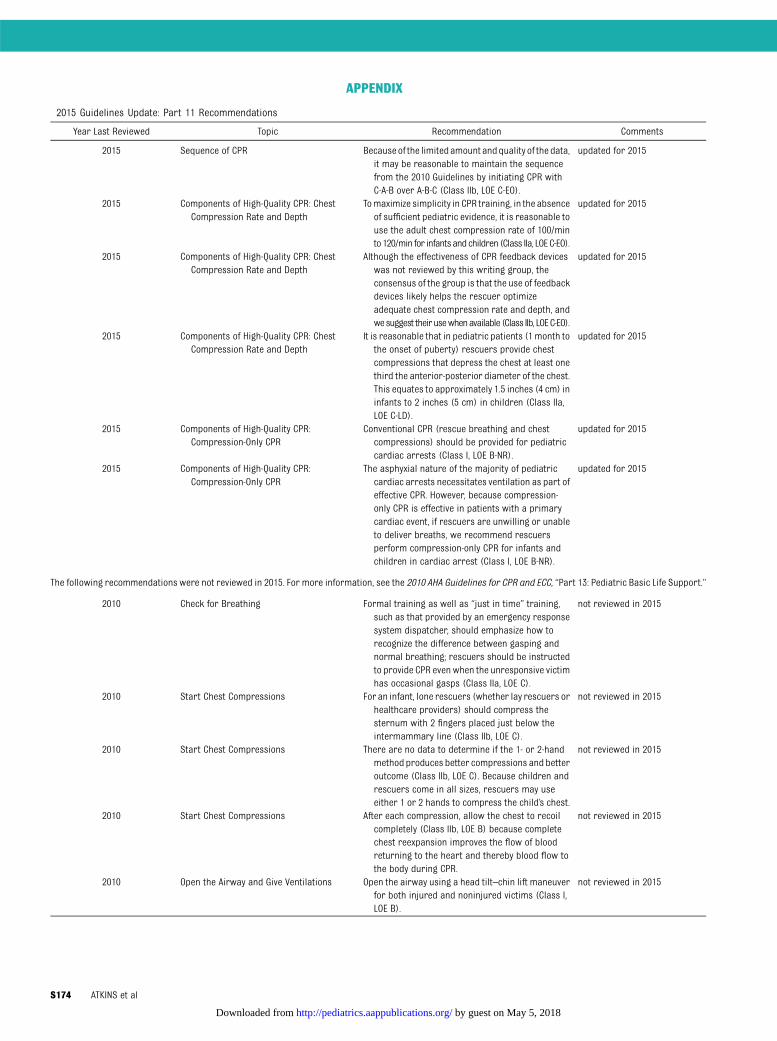
2015 Guidelines Update: Part 11 Recommendations
Year Last Reviewed Topic Recommendation Comments
2015 Sequence of CPR Becauseof the limitedamount andquality of the data,it may be reasonable to maintain the sequencefrom the 2010 Guidelines by initiating CPR withC-A-B over A-B-C (Class IIb, LOE C-EO).
updated for 2015
2015 Components of High-Quality CPR: ChestCompression Rate and Depth
Tomaximize simplicity in CPR training, in the absenceof sufficient pediatric evidence, it is reasonable touse the adult chest compression rate of 100/minto120/min for infantsandchildren (Class IIa, LOEC-EO).
updated for 2015
2015 Components of High-Quality CPR: ChestCompression Rate and Depth
Although the effectiveness of CPR feedback deviceswas not reviewed by this writing group, theconsensus of the group is that the use of feedbackdevices likely helps the rescuer optimizeadequate chest compression rate and depth, andwesuggest theirusewhenavailable (Class IIb, LOEC-EO).
updated for 2015
2015 Components of High-Quality CPR: ChestCompression Rate and Depth
It is reasonable that in pediatric patients (1 month tothe onset of puberty) rescuers provide chestcompressions that depress the chest at least onethird the anterior-posterior diameter of the chest.This equates to approximately 1.5 inches (4 cm) ininfants to 2 inches (5 cm) in children (Class IIa,LOE C-LD).
updated for 2015
2015 Components of High-Quality CPR:Compression-Only CPR
Conventional CPR (rescue breathing and chestcompressions) should be provided for pediatriccardiac arrests (Class I, LOE B-NR).
updated for 2015
2015 Components of High-Quality CPR:Compression-Only CPR
The asphyxial nature of the majority of pediatriccardiac arrests necessitates ventilation as part ofeffective CPR. However, because compression-only CPR is effective in patients with a primarycardiac event, if rescuers are unwilling or unableto deliver breaths, we recommend rescuersperform compression-only CPR for infants andchildren in cardiac arrest (Class I, LOE B-NR).
updated for 2015
The following recommendations were not reviewed in 2015. For more information, see the 2010 AHA Guidelines for CPR and ECC, “Part 13: Pediatric Basic Life Support.”
2010 Check for Breathing Formal training as well as “just in time” training,such as that provided by an emergency responsesystem dispatcher, should emphasize how torecognize the difference between gasping andnormal breathing; rescuers should be instructedto provide CPR even when the unresponsive victimhas occasional gasps (Class IIa, LOE C).
not reviewed in 2015
2010 Start Chest Compressions For an infant, lone rescuers (whether lay rescuers orhealthcare providers) should compress thesternum with 2 fingers placed just below theintermammary line (Class IIb, LOE C).
not reviewed in 2015
2010 Start Chest Compressions There are no data to determine if the 1- or 2-handmethod produces better compressions and betteroutcome (Class IIb, LOE C). Because children andrescuers come in all sizes, rescuers may useeither 1 or 2 hands to compress the child’s chest.
not reviewed in 2015
2010 Start Chest Compressions After each compression, allow the chest to recoilcompletely (Class IIb, LOE B) because completechest reexpansion improves the flow of bloodreturning to the heart and thereby blood flow tothe body during CPR.
not reviewed in 2015
2010 Open the Airway and Give Ventilations Open the airway using a head tilt–chin lift maneuverfor both injured and noninjured victims (Class I,LOE B).
not reviewed in 2015
S174 ATKINS et al
by guest on May 5, 2018http://pediatrics.aappublications.org/Downloaded from

Continued
Year Last Reviewed Topic Recommendation Comments
2010 Open the Airway and Give Ventilations In an infant, if you have difficulty making an effectiveseal over themouth and nose, try eithermouth-to-mouth or mouth-to-nose ventilation (Class IIb, LOE C).
not reviewed in 2015
2010 Open the Airway and Give Ventilations Ineithercasemakesure thechest riseswhenyougivea breath. If you are the only rescuer, provide 2effective ventilations using as short a pause inchest compressions as possible after each set of30 compressions (Class IIa, LOE C).
not reviewed in 2015
2010 BLS Sequence for Healthcare Providers andOthers Trained in 2-Rescuer CPR
It is reasonable for healthcare providers to tailor thesequence of rescue actions to the most likelycause of arrest. For example, if the arrest iswitnessed and sudden (eg, sudden collapse in anadolescent or a child identified at high risk forarrhythmia or during an athletic event), thehealthcare provider may assume that the victimhas suffered a sudden VF–cardiac arrest and assoon as the rescuer verifies that the child isunresponsive and not breathing (or only gasping)the rescuer should immediately phone theemergency response system, get the AED and thenbegin CPR and use the AED. (Class IIa LOE C).
not reviewed in 2015
2010 Pulse Check If, within 10 seconds, you don’t feel a pulse or are notsure if you feel a pulse, begin chest compressions(Class IIa, LOE C).
not reviewed in 2015
2010 Inadequate Breathing With Pulse Reassess the pulse about every 2 minutes (Class IIa,LOE B) but spend no more than 10 seconds doing so.
not reviewed in 2015
2010 Ventilations For healthcare providers and others trained in2-person CPR, if there is evidence of trauma thatsuggests spinal injury, use a jaw thrust withouthead tilt to open the airway (Class IIb LOE C).
not reviewed in 2015
2010 Coordinate Chest Compressions andVentilations
Deliver ventilations with minimal interruptions inchest compressions (Class IIa, LOE C).
not reviewed in 2015
2010 Defibrillation For infants a manual defibrillator is preferred whena shockable rhythm is identified by a trainedhealthcare provider (Class IIb, LOE C).
not reviewed in 2015
2010 Defibrillation An AED with a pediatric attenuator is also preferredfor children ,8 years of age. If neither isavailable, an AED without a dose attenuator maybe used (Class IIb, LOE C).
not reviewed in 2015
2010 Bag-Mask Ventilation (HealthcareProviders)
Avoid excessive ventilation (Class III, LOE C); use onlythe force and tidal volume necessary to just makethe chest rise.
not reviewed in 2015
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 2, November 2015 S175
by guest on May 5, 2018http://pediatrics.aappublications.org/Downloaded from

originally published online October 14, 2015; Pediatrics Stephen M. Schexnayder
Hunt, Benny L. Joyner, Peter A. Meaney, Dana E. Niles, Ricardo A. Samson and Dianne L. Atkins, Stuart Berger, Jonathan P. Duff, John C. Gonzales, Elizabeth A.
Cardiopulmonary Resuscitation and Emergency Cardiovascular Care (Reprint)Quality: 2015 American Heart Association Guidelines Update for
Part 11: Pediatric Basic Life Support and Cardiopulmonary Resuscitation
ServicesUpdated Information &
015-3373E.citationhttp://pediatrics.aappublications.org/content/early/2015/10/13/peds.2including high resolution figures, can be found at:
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.pediatrics.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
ISSN: . 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 5, 2018http://pediatrics.aappublications.org/Downloaded from

originally published online October 14, 2015; Pediatrics Stephen M. Schexnayder
Hunt, Benny L. Joyner, Peter A. Meaney, Dana E. Niles, Ricardo A. Samson and Dianne L. Atkins, Stuart Berger, Jonathan P. Duff, John C. Gonzales, Elizabeth A.
Cardiopulmonary Resuscitation and Emergency Cardiovascular Care (Reprint)Quality: 2015 American Heart Association Guidelines Update for
Part 11: Pediatric Basic Life Support and Cardiopulmonary Resuscitation
onhttp://pediatrics.aappublications.org/content/early/2015/10/13/peds.2015-3373E.citati
located on the World Wide Web at: The online version of this article, along with updated information and services, is
ISSN: . 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 5, 2018http://pediatrics.aappublications.org/Downloaded from