Embed Size (px)
Citation preview

www.picaheadstart.org
PARENTS IN COMMUNITY ACTION, INC. HEAD START & EARLY HEAD START
EN
RO
LL
YO
UR
CH
ILD
RE
N A
GE
S 0-
5
PICA’s Hotline
612-377-4444
© 2018 Parents In Community Action, Inc.-skc

SOME OF THE SERVICES AVAILABLE AT PICA HEAD START
SERVICES FOR FAMILIES SUPPORT
ü Door to Door Transportation ü Chemical Health
ü Monthly Food Shelf ü Disability Support – English/Spanish
ü Onsite Dental Services ü Literacy Support
ü Family Connect ü Mental Health
ü School Readiness ü New Lease on Life (Homeless Program)
ü Speech & Mental Health ü Prenatal Support
PARENT INVOLVEMENT
OPPORTUNITIES
ü Advisory Committees ü Center Committee ü Citizenship Classes ü English as a Second Language (ESL) ü First Aid and CPR Classes ü General Educational Development (GED)
ü Grandparents’ Group ü Male Involvement Committee ü Parent Lounge Activities ü Parent and Child Time (PAC)
ü Policy Council ü Valuing the Involvement of Parents (VIP)
PARENT TRAINING OPPORTUNITIES
ü Bus Monitor
ü Child Development
ü Clerical Support
ü Family Wellness
ü Food Service
ü Transportation
!$4)5);)4)&.(*#)&$#)"(
1+<(2+()(=%+<()9(,.(*1)42()'($4)5);4$>(
1$"2('&"#&?$"#4.(1$"2('&"#&@('!4)&7<$$=(+!&)+%(A*1)42("&&$%2'(B7C(2".'?<$$=D(
( $"#4.(1$"2('&"#&@(9-447&),$(+!&)+%(A*1)42("&&$%2'(8(2".'?<$$=D(
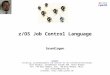
•! 8'$B)/$*/I/!((?*>J/;(&,*/ / •! 8'$B)/$*/I/!((?*/+-/K/;(&,*/• 8'$B)/B$D(*/$6/L(66(#$6/8-:6+; / • 8'$B)/B$D(*/$6/L(66(#$6/8-:6+;•! F&9$B;/,(%($D(*/AF75/%&*'=/EE7=/-,/9((+*/
F()(,&B/76%-9(/M:$)(B$6(*/•! 8'$B),(6/!$+'/)$&.6-*()/)$*&N$B$+$(*/O&6)/&6/
7P5Q/&,(/(B$.$NB(/,(.&,)B(**/-R/$6%-9("/E#(%$&B/6(()*/-,/R-*+(,/%&,(/%'$B),(6/&.(*/I/!((?*/+-/J/;(&,*/!'-/B$D(/$6/L(66(#$6/8-:6+;/&,(/&B*-/(B$.$NB("/
/ •! F&9$B;/$*/(B$.$NB(/R-,/%'$B)%&,(/*:N*$);/N(%&:*(/+'(/#&,(6+O*QS.:&,)$&6O*Q/!-,?/-,/.-/+-/*%'--B/-,/+'(/%'$B)/'&*/&/)$&.6-*()/)$*&N$B$+;/-,/*#(%$&B/6(()"/
FPCPT<U/7V8WAP/MX7CPU7VPE/1234// / 9",)4.(')E$( ,"F(.$"#4.()%*+,$(1$"2('&"#&@(9-447&),$(+!&)+%(A*1)42("&&$%2'(8(2".'?<$$=D(
/ 3/ Y31=Z42// 1/ Y3I=432// K/ Y13=KK2/
•! 8'$B)/$*/K>J/;(&,*/ / Z/ Y1J=[J2/•! 8'$B)/B$D(*/$6/L(66(#$6/8-:6+;/ / J/ YK2=3[2/•! F&9$B;/$*/(B$.$NB(/R-,/&/%'$B)%&,(/*:N*$);/N(%&:*(/
+'(/#&,(6+O*QS.:&,)$&6O*Q/!-,?/-,/.-/+-/*%'--B=/-,/+'(/%'$B)/'&*/)$&.6-*()/)$*&N$B$+$(*/-,/*#(%$&B/6(()*"/
/ I/ YKZ=J42// [/ YK4=232// \/ YZK=ZK2// FWT/P<8L/<CC7H7WV<U/5PTEWV/<CC/YZ=Z12"/
/1+<(&+($%#+44@( / /!GHIJH(KLMNO(PQH(RSGGSTMNO(RSLUJ@( / /
!! *VLLHNP(!QWJMXIG($YIUMNIPMSN(INZ()UUVNM[IPMSN(#HXSLZJ0((F$BB/-:+/+'(/+-#/#&,+/-R/+'(/(6%B-*()/!"#$%&'"()#*+$&&6)/+'(/,--./#0+1#2/&324-5& H'(*(/R-,9*/!$BB/N(/%-9#B(+()/&6)/*$.6()/N;/;-:,/)-%+-,"
!! 2HNPIG($YIUMNIPMSN0((7R/;-:,/%'$B)/'&*/&/)(6+$*+=/'&D(/+'(9/%-9#B(+(/&6)/*$.6/+'(/(6%B-*()/67/1+$&89+-&:&;47+1-7/1&<7=2415(
!! )NJVLINXH(*ILZJ0((@,$6./;-:,/%'$B)]*/9()$%&B/&6)/)(6+&B/$6*:,&6%(/%&,)*"(!! $UHLOHNXW()NRSLUIPMSN0((8-9#B(+(/+'(/(6%B-*()/8-74>7/*(&!+4%?&$6%B:)(/
+'(/6&9(*=/&)),(**(*=/&6)/#'-6(/6:9N(,*/-R/+',((/(9(,.(6%;/%-6+&%+*"(!! !LSSR(SR()NXSUH0((@,$6./-RR$%$&B/)-%:9(6+&+$-6/-R/$6%-9("//F-,/(^&9#B(_//
A$66(*-+&/F&9$B;/76D(*+9(6+/5B&6/OAF75Q=/E:##B(9(6+&B/E(%:,$+;/76%-9(/OEE7Q=/E-%$&B/E(%:,$+;/C$*&N$B$+;/76%-9(/OEEC7Q=/R-*+(,/%&,(/-,/:6(9#B-;9(6+/%-9#(6*&+$-6"//7R/;-:/&,(/(9#B-;()=/N,$6./;-:,/G>1/R-,9*=/+&^/,(+:,6=/#&;%'(%?/*+:N*=/-,/-+'(,/$6%-9(/D(,$R$%&+$-6"(
!! )NZM\MZVIG(*QMGZ(*ILH(!GIN0((7R/;-:/%'$B)/'&*/&/'(&B+'/%-6)$+$-6/*:%'/&*_//&*+'9&=/R--)/&BB(,.;=/(6D$,-69(6+&B/&BB(,.;=/*($`:,(*=/-,/&6;/-+'(,/'(&B+'/%-6)$+$-6"(
!! )R(WSVL(I]]GMXIPMSN(MJ(NSP(XSU]GHPH/(TH(TMGG(NSP(KH(IKGH(PS(HNLSGG(WSVL(XQMGZ0((

Head Start’s commitment to wellness embraces a comprehensive vision of health for children and families. A complete physical exam is required so that we can ensure that if children’s health and developmental concerns are identified, children and families are linked to a source of continuous, accessible care (Medical Home) to meet their basic health needs. The focus of Head Start health services is prevention and early intervention.
APPLY IN PERSON AT ANY OF THE CENTERS LISTED BELOW
Applications are taken from 9:00 a.m. to 5:00 p.m. You may call ahead of time to make an appointment if you cannot apply during those hours.
WESTERN SUBURBS Helen H. Taylor Center
4901 Olson Memorial Highway Golden Valley, MN 55422
Phone: (763) 541-7422
NORTH MINNEAPOLIS Donald M. Fraser Center
700 Humboldt Avenue North Minneapolis, MN 55411 Phone: (612) 377-7422
SOUTH MINNEAPOLIS McKnight Center
4225 Third Avenue South Minneapolis, MN 55409 Phone: (612) 825-7422
Park Place Center
2745 Park Avenue South Minneapolis, MN 55407 Phone: (612) 870-7422
Portland Village Center
1829 Portland Avenue South Minneapolis, MN 55404 Phone: (612) 871-7422
PICA Training Center
4255 Third Avenue South Minneapolis, MN 55409 Phone: (612) 822-7422
SOUTHERN SUBURBS South Branch Center
7145 Harriet Avenue Richfield, MN 55423
Phone: (612) 871-7422
Pond Center 9600 Third Avenue South Bloomington, MN 55420
Phone: (612) 871-7422
NORTHEAST MINNEAPOLIS
Northeast Center 342 Thirteenth Avenue N.E.
Minneapolis, MN 55413 Phone: (612) 379-7422
NORTHWESTERN SUBURBS Town Hall Center
8500 Zane Avenue North Brooklyn Park, MN 55443
Phone: (763) 425-7422
Aubrey Della Center 6415 Brooklyn Boulevard
Brooklyn Center, MN 55429 Phone: (763) 535-7422
SOUTHEAST MINNEAPOLIS Glendale Center
96 St. Mary’s Avenue S.E. Minneapolis, MN 55414 Phone: (612) 874-7422
HEALTH REQUIREMENTS FOR HEAD START Your child needs a physical exam called a Child and Teen Check-up, which includes:
o A blood test for lead and results o A total body checkup o A blood test for iron (hemoglobin) and results o A blood pressure reading o Vision and hearing screening o An up-to-date immunization record
Ask my doctor to give me a
Child & Teen Checkup.
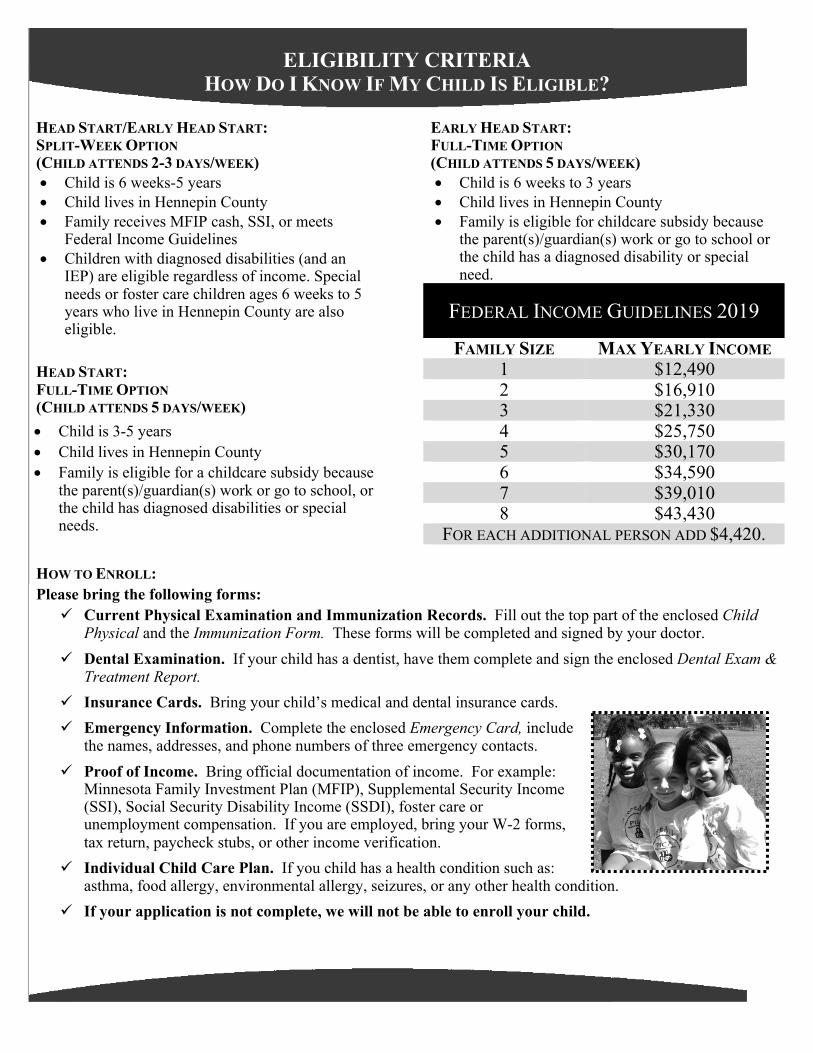
Parents In Community Action, Inc. 700 Humboldt Avenue North Minneapolis, MN 55411 (612) 377-7422
CHILD PHYSICAL Please complete attached Individual Child
Care Plan for Chronic Health Issues.
Child’s Last Name First Name Middle Initial Birth Date Age
Parent/Guardian Names Address Telephone Numbers:
Early and Periodic Screening Diagnosis and Treatment (EPSDT) exam required.
Starred items (*) are required by Federal Head Start and Early Head Start regulations. Enter date if date of test is other than “exam date” recorded below.
FINDINGS, TREATMENTS, AND RECOMMENDATIONS
TEST DATE RESULTS TEST DATE RESULTS A. HEIGHT (CM)* H. Vision (Type of Test)* B. WEIGHT (KG)* (1) ACUITY, R/L C. BMI (2) CORNEAL REFLEX D. BLOOD PRESSURE (3) COVER TEST E. HEMATOCRIT or HEMOGLOBIN*
Result (4) COMMENTS
I. OTHER TESTS Complete or send past results)
(1) TB (2) Sickle Cell (3) Ova & Parasites (4) Urinalysis (5) Other
F. LEAD* G. HEARING (Type of Test)* Pure Tone at 20dB
1000 Hz 2000 Hz 4000 Hz RIGHT EAR q Pass q Fail q Pass q Fail q Pass q Fail
LEFT EAR q Pass q Fail q Pass q Fail q Pass q Fail
PHYSICAL EXAMINATION/ASSESSMENT Normal for Age Abnormal Not
Evaluated Note to physician: Please fill out all items in Health Record.
A. GENERAL APPEARANCE q NL q AB q NE Specify any condition that may result in an emergency situation.
How is child’s overall physical status?
B. POSTURE, GAIT q NL q AB q NE C. SPEECH q NL q AB q NE D. HEAD q NL q AB q NE E. SKIN q NL q AB q NE F. EYES: Specify type and dose of any current medication or therapies:
(1) External Aspects q NL q AB q NE (2) Optic Fundoscopy q NL q AB q NE
G. EARS Environmental Allergies:
(1) External & Canals q NL q AB q NE (2) Tymanic Membranes q NL q AB q NE
H. NOSE, MOUTH, PHARYNX q NL q AB q NE I. DENTAL
(1) Examine Teeth q NL q AB q NE Food Allergies: Describe any dietary substitutions:
(2) Examine Gums q NL q AB q NE (3) Referral to Dentist? q Yes q No q NE
J. HEART q NL q AB q NE K. LUNGS q NL q AB q NE L. ABDOMEN (Include hernia) q NL q AB q NE M. GENITALIA q NL q AB q NE Describe any diagnosed disabilities:
N. BONES, JOINTS, MUSCLES q NL q AB q NE O. NEUROLOGICAL/SOCIAL q NL q AB q NE
(1) Gross Motor q NL q AB q NE (2) Fine Motor q NL q AB q NE Please print or type physician or nurse practitioner’s name and telephone
number. (3) Communication Skills q NL q AB q NE (4) Cognitive q NL q AB q NE Print MD/NP Name (5) Self-Help Skills q NL q AB q NE First Last
(6) Social Skills q NL q AB q NE P. GLANDS (Lymphatic/Thyroid) q NL q AB q NE MD/NP Signature Q. DEVELOPMENTAL ASSESSMENT q NL q AB q NE
Phone Exam Date
Abnormal Findings/Diagnoses Treatment Plan and Recommended Follow-Up or Results Date
© 2018 Parents In Community Action, Inc.-skc

Parents In Community Action, Inc. 700 Humboldt Avenue North Minneapolis, MN 55411 (612) 377-7422
INDIVIDUAL CHILD CARE PLAN
Please send the Asthma Action Plan or Anaphylaxis Plan, if applicable.
First Name Last Name Birthdate
HEALTH CARE PROVIDER TREATING THE CHILD’S CONDITION: Site Class Session
Name/Title Clinic
Address City Zip
Telephone Fax
1. Diagnosed Medical Condition:
a) When was your child first diagnosed? Is it an ongoing health issue? ☐ Yes ☐ No
b) If yes, describe how often it occurs:
c) What symptoms and behaviors does your child experience?
d) List any restrictions at day care:
2. Treatment and Medications (Complete MEDICATION PERMISSION form)
a) Routine treatment(s) and medication(s):
b) As needed (PRN) treatment(s) and medication(s):
3. Emergency Care: If your child does not respond to medication and treatment, the emergency plan is:
4. Additional Information and/or Health Care Provider Recommendations:
5. Child’s Knowledge (to be completed by parent):
a) What is your child’s understanding of the medical condition?
b) Does your child understand about any restrictions at day care?
c) Can your child tell the teacher when treatment or medication is needed? ☐ Yes ☐ No
d) Does your child cooperate with treatment and medication? ☐ Yes ☐ No
Parent or Guardian Signature and Date Health Care Provider Signature and Date (not needed for eczema)
© 2018 Parents In Community Action, Inc. – skc

Child Care Immunization Form Must be on file before a child attends child care
Name Birthdate
Minnesota law requires children enrolled in child care to be immunized against certain diseases or have a legal medical exemption or conscientious exemption on file.
Parent/Guardian: You may attach a copy of the child’s immunization history to this form OR enter the MONTH, DAY, and YEAR for all vaccines your child received. Enter MED to indicate vaccines that are medically contraindicated including a history of disease or laboratory evidence of immunity, and CO for vaccines that are contrary to parent or guardian’s conscientiously held beliefs.
Sign or obtain appropriate signatures on reverse. Complete section 1A or 1B to certify immunization status, section 2A to document medical exemptions (including a history of varicella disease), and 2B to document a conscientious exemption.
For updated copies of your child’s vaccination history, talk to your doctor or call the Minnesota Immunization Information Connection (MIIC) at 651-201-5503 or 800-657-3970.
Type of Vaccine DO NOT USE (✓)or(*) 1st Dose Mo/Day/Yr
2nd Dose Mo/Day/Yr
3rd Dose Mo/Day/Yr
4th Dose Mo/Day/Yr
5th Dose Mo/Day/Yr
Required (The shaded boxes indicate doses that are not routinely given; however, if your child has received them, please write the date in the shaded box.) Diphtheria, Tetanus, and Pertussis (DTaP, DTP) • 3 doses during 1st year (at 2-month intervals) • 4th dose at 12-18 months • 5th dose at 4-6 years
Indicate vaccine type: DTaP or DTP
5th dose not required if 4th dose was given on or after the 4th birthday
Polio (IPV, OPV) • 2 doses in the first year • 3rd dose by 18 months • 4th dose at 4-6 years
4th dose not required if 3rd dose was given on or after the 4th birthday
Measles, Mumps, and Rubella (MMR) • Required for children 15 months and older • 1st dose on or after 1st birthday • 2nd dose at 4-6 years
Haemophilius influenza type b (Hib) • 2-3 doses in the first year • 1 dose required at 12 months or older • For unvaccinated children 15-59 months, 1 dose is
required • Not required for children 5 years or older
Varicella (chickenpox) • Required for children 15 months or older • 1st dose on or after 1st birthday • 2nd dose at 4-6 years
Pneumococcal Conjugate Vaccine (PCV) • Required for children age 2-24 months • 3 doses in the first year • 4th dose after 12 months • At least 1 dose is recommended for children 24-59
months in child care
Hepatitis B (hep B) • 2-3 doses in the first year • 3rd dose (final dose) by 18 months
Hepatitis A (hep A) • 2 doses separated by 6 months for children 12 months
and older
Recommended Rotavirus (2-3 doses between 2 and 6 months)
Influenza (annually for children 6 months or older) © 2018 Parents In Community Action, Inc.-skc
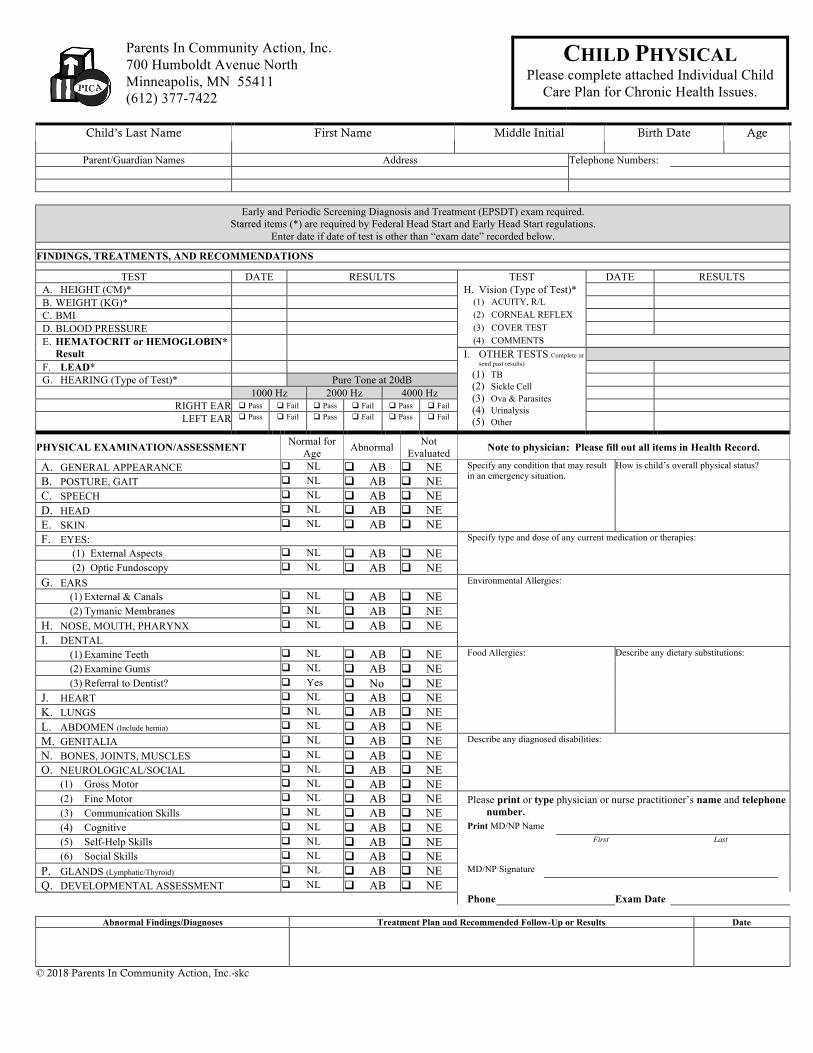
Name
Instructions, please complete: Box 1 to certify the child’s immunization status Box 2 to file an exemption (medical or conscientious)
1. Certify Immunization Status. Complete A or B to indicate child’s immunization status. A. Children who are 15 months or older: B. Children who are younger than 15 months:
For children who are 15 months or older and who have received all the immunizations required by law for child care. I certify that the above-named child is at least 15 months of age and has completed the immunizations which are required by law for child care.
Signature of Parent/Guardian OR Physician/Nurse Practitioner/Physician Assistant/Public Clinic _____________________________Date
For children who are younger than 15 months OR have not received all required immunizations. I certify that the above-named child has received the immunizations indicated. In order to remain enrolled, this child must receive all required vaccines within 18 months of the initial enrollment date. The dates on which the remaining doses are to be given are: Signature of Physician/Nurse Practitioner/ Physician Assistant/Public Clinic _____________________________Date
2. Exemptions to Immunization Law. Complete A and/or B to indicate type of exemption.
A. Medical exemption: B. Conscientious exemption: No child is required to receive an immunization if they have a medical contraindication, history of disease, or laboratory evidence of immunity. For a child to receive a medical exemption, a physician, nurse practitioner, or physician assistant must sign this statement: I certify the immunization(s) listed below are contraindicated for medical reasons, laboratory evidence of immunity, or that adequate immunity exists due to a history of disease that was laboratory confirmed (for varicella disease see * below). List exempted immunization(s): Signature of physician/nurse practitioner/physician assistant _____________________________Date ∗ History of varicella disease only. In the case of
varicella disease, it was medically diagnosed or adequately described to me by the parent to indicate past varicella infection in __________(year)
Signature of physician/nurse practitioner/physician assistant (If disease occurred before September 2010, a parent can sign.)
No child is required to have an immunization that is contrary to the conscientiously held beliefs of his/her parent or guardian. However, not following vaccine recommendations may endanger the health or life of the child or others they come in contact with. In a disease outbreak, children who are not vaccinated may be excluded in order to protect them and others. To receive an exemption to vaccination, a parent or legal guardian must complete and sign the following statement and have it notarized: I certify by notarization that it is contrary to my conscientiously held beliefs for my child to receive the following vaccine(s). ¨ I am opposed to all vaccines. ¨ I am opposed only to vaccines indicated below. ___________________ __________________ ___________________ __________________ Signature of parent or legal guardian
______________________________Date Subscribed and sworn to before me this: ________day of _______________________20___ Signature of notary (A copy of the notarized statement will be forwarded to the commissioner of health.)
Developed by the Minnesota Department of Health – Immunization Program www.health.state.mn.us/immunize (12/13)

Parents In Community Action, Inc. 700 Humboldt Avenue North Minneapolis, MN 55411 (612) 377-7422
ASTHMA ACTION PLAN
SITE: ROOM:
Patient Name: Weight: # DOB: Peak Flow:
Doctor or Nurse Practitioner Name:
Asthma Severity:
Clinic Name: Phone: Symptom Triggers:
Green Zone The Green Zone means take the following medicine(s) every day:
“Go All Clear!” Controller Medicine(s): Dose:
− Breathing is easy − Can play, work, and sleep without
asthma symptoms
Peak Flow Range Spacer Used: (80%-100% of personal best)
to Take the following medicine if needed 10-20 minutes before sports, exercise, or any other strenuous activity:
Yellow Zone
The Yellow Zone means keep taking your Green Zone controller medicine(s) every day and add the following medicine(s) to help keep the asthma symptoms from getting worse.
“Caution…” Reliever Medicine(s): Dose:
− Wakes up at night − Coughs or wheezes − Chest is tight
Use Quick Reliever 2-4 puffs, every 20 minutes for up to 1 hour or use nebulizer once.
If your symptoms are not better or you do not return to the GREEN ZONE after 1 hour, follow RED ZONE instructions. If you are in the Yellow Zone for more than 12-24 hours, call your provider. If your breathing symptoms get worse, call your provider.
Peak Flow Range (50%-80% of personal best)
to
Red Zone The Red Zone means start taking your Red Zone medicine(s) and call your doctor NOW! Take these medicines until you talk with your doctor. If your symptoms do not get better and you can’t reach your doctor, go to the emergency room or call 911 immediately.
“STOP!” “Medical Alert”
− Medicine is not helping − Nose opens wide to breathe − Breathing is hard and fast − Trouble walking − Trouble talking − Ribs show
Reliever Medicine(s): Dose:
Peak Flow Range (Below 50% of personal best)
to
I give my permission for this asthma action plan to be used by the following, and for them to share information with each other about my child’s asthma for one year beginning today, so that they can work together to help my child manage his/her asthma. This plan, when signed and dated, may replace or supplement the school’s/daycare’s consent to administer medication form, and allows my child’s medicine to be administered at school/daycare.
© 2018 Parents In Community Action, Inc.-skc

Parents In Community Action, Inc. 700 Humboldt Avenue North Minneapolis, MN 55411 (612) 377-7422
CHILD EMERGENCY CARD
CHILD’S NAME:
☐ Female ☐ Male
(First) (Middle) (Last) Birth Date Gender
Parent or Guardian Full Name Relationship to Child Cell/Work or Home Phone Number
Parent or Guardian Full Name Relationship to Child Cell/Work or Home Phone Number
Home Address City Zip Code
PICK UP AND DROP OFF ADDRESS IF DIFFERENT FROM THE HOME ADDRESS:
Pick Up Address Pick Up Contact Notes
Drop Off Address Drop Off Contact Notes
IN CASE OF EMERGENCY THE FOLLOWING ADULTS ARE AUTHORIZED CONTACTS AND MY CHILD MAY BE RELEASED TO THESE PEOPLE.
In the event of an emergency, we will make every effort to contact you or one of the emergency contacts. Your child will NOT be released to anyone other than those adults listed on this form. Please allow 48 hours for changes to go into effect.
Full Name Address City & Zip Code
Relationship to Child Cell Phone Number Home Phone Number Work Phone Number
Full Name Address City & Zip Code
Relationship to Child Cell Phone Number Home Phone Number Work Phone Number
Full Name Address City & Zip Code
Relationship to Child Cell Phone Number Home Phone Number Work Phone Number
In the case of a medical or dental emergency I hereby authorize Parents In Community Action, Inc. (PICA) staff to take my child to a health facility for treatment. I also authorize any licensed medical practitioner to provide whatever treatment is deemed necessary. I accept responsibility for any costs arising from such treatment that are not covered by insurance and/or Medical Assistance.
Parent or Guardian Signature
Date
© 2018 Parents In Community Action, Inc.-skc
Parents In Community Action, Inc. 700 Humboldt Avenue North Minneapolis, MN 55411 (612) 377-7422
DENTAL EXAM & TREATMENT REPORT
☐ Female ☐ Male CHILD’S NAME:
(Last) (First) (Middle Initial) Birth Date Gender
Parent or Guardian Full Name Relationship to Child Cell/Work or Home Phone Number
Home Address City Zip Code
Child’s Dental Insurance Provider Child’s Dental Insurance Number MN Health Care Programs Number
Dear Parent or Guardian: To ensure good oral health, every child one year and older must have a dental examination within the last six months, or no later than 90 days after the child starts school. If your child does not have a regular dentist, you may choose to have your child seen at PICA through Children’s Dental Services. If your child does have a dental provider, please have them complete the section below and bring it with you to registration.
DENTAL REPORT This child received the following treatment in my office:
q Dental exam q Fillings q X-rays TAKEN q Emergency q X-rays READ q Extractions q Cleaning q Steel crowns q Topical fluoride application q Space maintainers q Sealant q Bitewing X-Rays taken
q Other, explain:
q ALL treatments ARE complete. q ALL treatments are NOT complete – the following is still needed:
q TAKE X-rays q Fillings Next Appointment q READ X-rays q Extractions Date: q Topical fluoride application q Steel crowns q Cleaning q Space maintainers q Sealant q Other, explain: Date of Initial Exam
Date of Follow-up Exam
Dentist’s Signature ( ) -
Print Dentist’s Name Dentist’s Telephone
Parent or Guardian Signature Date
© 2018 Parents In Community Action, Inc.-skc

PARENTS IN COMMUNITY ACTION, INC. 700 Humboldt Avenue North Minneapolis, MN 55411
Head Start Application & Information A publication of
www.picaheadstart.org • 24-Hour Hotline: (612) 377-4444
PICA Head Start - Child Care and So Much More • Enroll Your Children In Head Start Now! ¡Inscriba a sus niños en Head Start ahora! • Hadda U Buuxi Cunugaaga Head Start-ka!
Sau Koj Tus Menyuam Npe Kawm Head Start Tam Sim No! Head Starttii Keessat Qooda Fudhadha, Ijoollee Galcha!
© 2018 Parents In Community Action, Inc. – skc