Embed Size (px)
Citation preview

Parathyroid Scanning
Barbara Ratliff, Patrick Soon, Steve MacFarlane, and Laurence Hanelin
The Mason Clinic, Seattle, Washington
This is the first in a series of four Continuing Education arlicles on imaging techniques. After studying this arlicle, the reader should be able to: 1) understand the clinical importance, the procedures, and technical pitfalls of parothyroid imaging; and 2) discuss computer manipulations such as subtroction techniques.
ANATOMY
The parathyroids are paired endocrine glands which usually lie between the posterior borders of the thyroid and the thyroid capsule, near the lateral aspect of each lobe (1). There are commonly four glands: two superior and two inferior in position. Occasionally there is a fifth gland, frequently ectopic to the thyroid. The average weight of the normal parathyroid gland is 35-50 mg. It has the appearance of yellowish brown fatty tissue and is 6 mm long, 3-4 mm wide, and 1-2 mm thick.
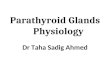
Embryologically, the superior parathyroids originate in the fourth branchial clefts and inferior parathyroids in the third branchial clefts. During fetal development, the superior glands descend along with the thyroid and the inferior glands descend along with the thymus to their adult locations. The inferior glands tend to be more variable in location because of the greater distance that they migrate. Parathyroid glands may be found anywhere from the angle of the mandible to the level of the aortic arch. Ectopic glands are commonly: a) lateral to the thyroid; b) retropharyngeal; c) retroesophageal; d) in the thymic tongue; or e) in the mediastinum. Figure 1 illustrates the normal and most common ectopic locations of the parathyroid glands.
The parathyroids are difficult to locate surgically because of their small size, appearance, the variability of their locations, and their proximity to the recurrent laryngeal nerves; the superior glands are usually dorsal and the inferior glands are ventral to those nerves. Pathologic conditions that cause enlargement such as tumor or hyperplasia tend to extend the inferior glands into the posterior mediastinum, or they may descend along the inferior thyroid veins into the anterior mediastinum.
FUNCTION AND PATHOPHYSIOLOGY
The functions of the parathyroid glands are to synthesize, store, and secrete parathyroid hormone (PTH). PTH directly regulates the level and distribution of calcium and phosphorus.
For reprints contact: Barbara Ratliff. The Mason Clinic, llOO 9th Avenue, P.O. Box 900, Seattle, WA 98lll-0900.
34
When ionic calcium blood concentrations fall, PTH is released. PTH acts rapidly on the osteocytes in bone to increase the rate of ionic calcium release from bone mineral into the blood stream (2). PTH also influences ion transport mechanisms in the kidney, increasing the excretion of phosphates, sodium, and potassium while decreasing excretion of calcium. PTH also acts indirectly with vitamin D to increase intestinal absorption of calcium.
The effect of prolonged excess excretion of PTH, as in primary hyperparathyroidism because of tumor or four gland hyperplasia, is the removal of such large amounts of calcium from the bone mineral that they become weak and break easily. The state of excess calcium ion in the blood stream is known as hypercalcemia. Hypercalcemia causes nervous system depression, muscle weakness, and, in extreme cases, calcium phosphate may precipitate in tissues such as the alveoli of the lungs, the walls of the arteries, the thyroid, the gastric mucosa, and the renal tubules. Death may result from renal failure.
Treatment for primary hyperparathyroidism is surgical resection of the tumor or hyperplastic glands. The surgical procedure is technically difficult, requiring careful neck dissection to avoid injury to the recurrent laryngeal nerves. Although success in locating and removing parathyroid tumors is 95% ~r greater, surgical time may be greatly prolonged or reoperatJon required ifthe tumor is ectopic to the thyroid and not found in the neck exploration. Presurgical localization can identify ectopic tumors and thereby shorten surgical time. Localization would be particularly desirable in the high-risk patient and also in cases of reexploration, where scarring may further complicate the surgery.
Most methods used to locate parathyroid tumors are invasive, unreliable, and expensive. Invasive procedures such as arteriography and venous PTH sampling are tedious and limited in their success. Noninvasive CT and ultrasound techniques, though more effective in the neck region, cannot adequately examine the mediastinum.
RADIONUCLIDE IMAGING
Early attempts at radionuclide imaging ofhyperfunctioning parathyroid glands and tumors proved unsuccessful because a properly localizing radiopharmaceutical with good imaging characteristics could not be found (3-8).
Interest in radionuclide imaging of parathyroid tumors was revived recently by reports of preoperative localization of parathyroid tumors using 201 Tl chloride (9,10). In 1983, Ferlin, eta!. (11) published data on 24 patients who were imaged with a double tracer subtraction technique using [99mTc]pertech-
JOURNAL OF NUCLEAR MEDICINE TECHNOLOGY
by on May 22, 2020. For personal use only. tech.snmjournals.org Downloaded from
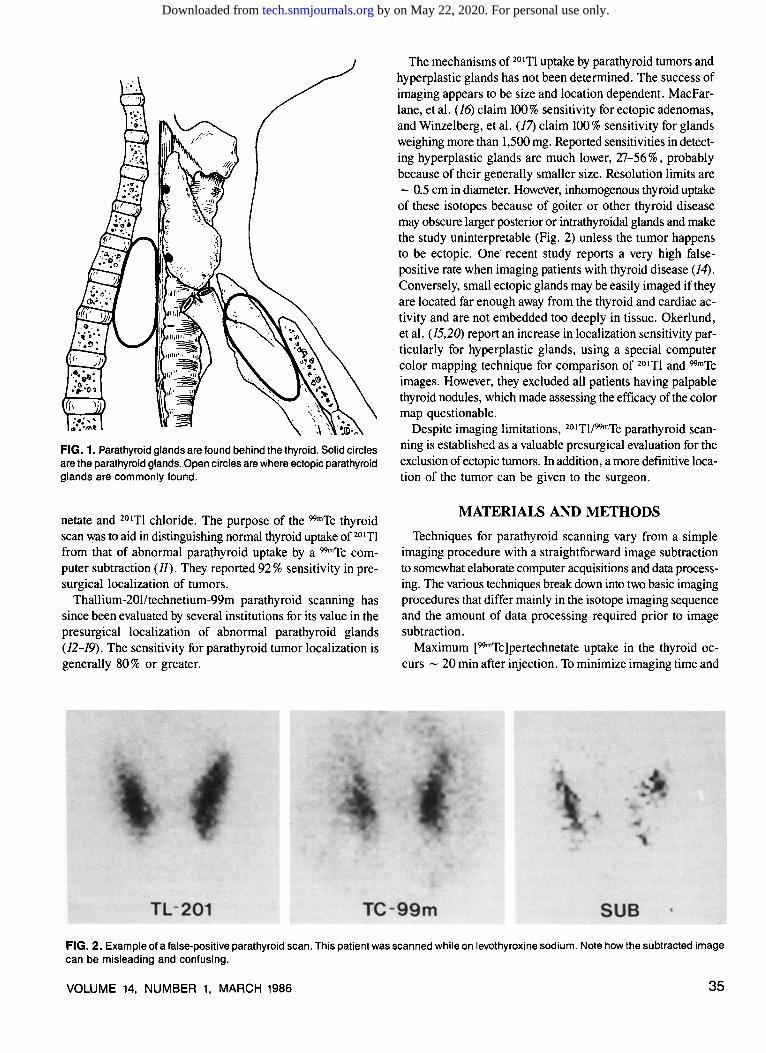
FIG. 1. Parathyroid glands are found behind the thyroid. Solid circles are the parathyroid glands. Open circles are where ectopic parathyroid glands are commonly found.
netate and 201Tl chloride. The purpose of the 99mTc thyroid scan was to aid in distinguishing normal thyroid uptake of 201Tl from that of abnormal parathyroid uptake by a 99mTc computer subtraction (11). They reported 92% sensitivity in presurgical localization of tumors.
Thallium-201/technetium-99m parathyroid scanning has since been evaluated by several institutions for its value in the presurgical localization of abnormal parathyroid glands (12-19). The sensitivity for parathyroid tumor localization is generally 80% or greater.
The mechanisms of 201Tl uptake by parathyroid tumors and hyperplastic glands has not been determined. The success of imaging appears to be size and location dependent. MacFarlane, eta!. (16) claim 100% sensitivity for ectopic adenomas, and Winzelberg, eta!. (17) claim 100% sensitivity for glands weighing more than 1,500 mg. Reported sensitivities in detecting hyperplastic glands are much lower, 27-56%, probably because of their generally smaller size. Resolution limits are - 0.5 em in diameter. However, inhomogenous thyroid uptake of these isotopes because of goiter or other thyroid disease may obscure larger posterior or intrathyroidal glands and make the study uninterpretable (Fig. 2) unless the tumor happens to be ectopic. One· recent study reports a very high falsepositive rate when imaging patients with thyroid disease (14). Conversely, small ectopic glands may be easily imaged if they are located far enough away from the thyroid and cardiac activity and are not embedded too deeply in tissue. Okerlund, eta!. (15,20) report an increase in localization sensitivity particularly for hyperplastic glands, using a special computer color mapping technique for comparison of 201Tl and 99mTc images. However, they excluded all patients having palpable thyroid nodules, which made assessing the efficacy of the color map questionable.
Despite imaging limitations, 201Tl/99mTc parathyroid scanning is established as a valuable presurgical evaluation for the exclusion of ectopic tumors. In addition, a more definitive location of the tumor can be given to the surgeon.
MATERIALS AND METHODS
Techniques for parathyroid scanning vary from a simple imaging procedure with a straightforward image subtraction to somewhat elaborate computer acquisitions and data processing. The various techniques break down into two basic imaging procedures that differ mainly in the isotope imaging sequence and the amount of data processing required prior to image subtraction.
Maximum [99mTc]pertechnetate uptake in the thyroid occurs - 20 min after injection. To minimize imaging time and
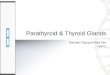
FIG. 2. Example of a false-positive parathyroid scan. This patient was scanned while on levothyroxine sodium. Note how the subtracted image can be misleading and confusing.
VOLUME 14, NUMBER 1, MARCH 1986 35
by on May 22, 2020. For personal use only. tech.snmjournals.org Downloaded from

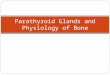
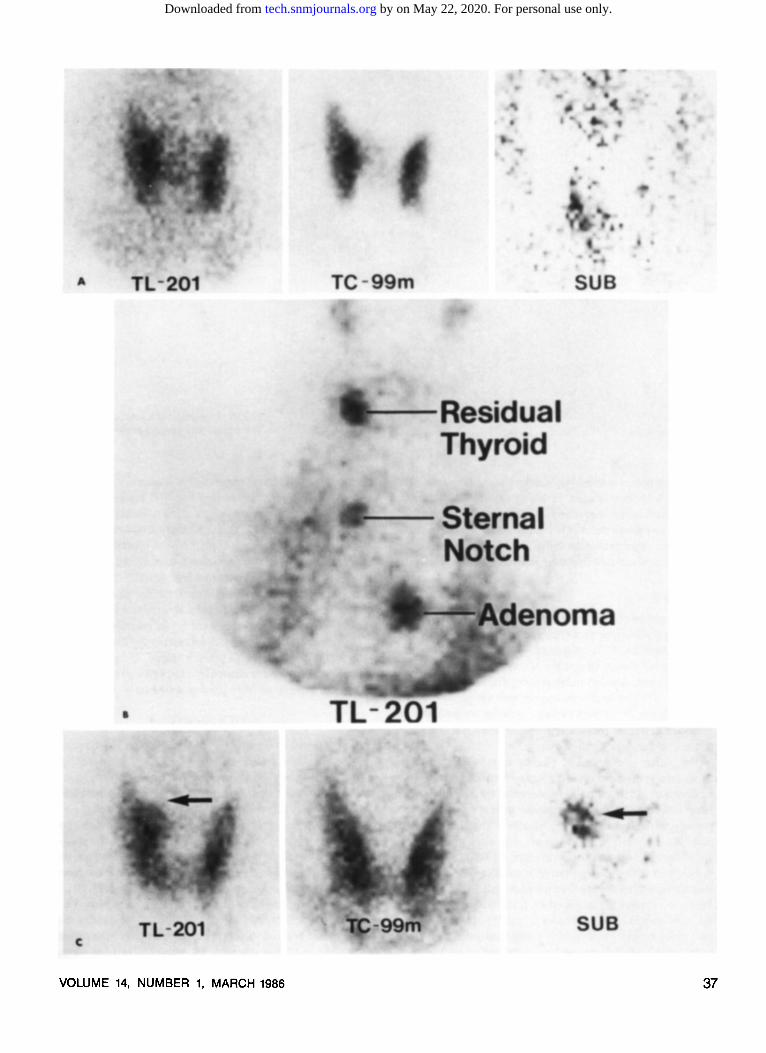
FIG. 3. (A) The subtraction image was very helpful in locating this adenoma on the medial aspect of the right lobe. Comparison of the 201 TI image and the 99mTc image, however, shows the adenoma without the subtraction image. (B) In a patient with thyroid disease, the subtraction image is very misleading.
thus the probability of movement during the study, parathyroid subtraction scanning initially began with the 99mTc thyroid image. Imaging of the 77 keY x-ray of2° 1TI after the injection of [99mTc]pertechnetate means that the 201TI image will contain downscatter from the 140 keY emission of 99mTc. The thallium image will require correction for this downscatter prior to image subtraction, or thyroid activity will be present in the subtraction image. If this occurs, the subtraction image will be of little or no use in the interpretation of the study.
Method 1 The original imaging method described by Ferlin, et al. (JJ)
and in use by several other groups (12-14) begins with a thyroid scan using 0.5-2.0 mCi of sodium [99mTc]pertechnetate injected through an indwelling venous line. Twenty minutes later, a 50,000-100,000 count anterior pinhole image of the thyroid is stored in a nuclear medicine computer. An image of the 99mTc downscatter in the 201TI window is then acquired for a predetermined time, usually 2-5 min. Following acquisition of the downscatter image, 1.0-2.0 mCi of 201TI chloride is injected, without moving the patient, and a dynamic series of images is acquired, each for the same time as the scatter
36
image, for a total time of 30 min. Data processing involves the following: 1) subtracting the
scatter image from each 201TI image acquired in the dynamic series; 2) summing the scatter-corrected 201TI images; 3) normalizing the 99mTc and 201TI images to each other so that count densities are similar; and 4) subtracting the 99mTc image from the 201TI image to obtain an image revealing the 201Tl activity caused by abnormal parathyroid uptake.
Additional data processing may include motion correction and nonspecific background subtraction. Motion correction may be done by viewing the dynamic frames with a reference of some type (e.g., a region outlining the thyroid or a series of pixel coordinates as a reference point) and throwing out frames where patient motion is detected.
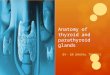
FIG. 4. (A) The adenoma in this patient is not obvious by comparing the 201 TI image to the 99mTc image, but the subtraction image is helpful. (B) This 201 TI survey image shows that an adenoma is located in the mediastinum. This adenoma would be missed using only a pinhole image which clearly demonstrates the importance of acquiring a survey image. (C) This scan shows an adenoma to be located at the medial aspect of the right lobe, which is obvious without subtraction .....
JOURNAL OF NUCLEAR MEDICINE TECHNOLOGY
by on May 22, 2020. For personal use only. tech.snmjournals.org Downloaded from
VOLUME 14, NUMBER 1, MARCH 1986 37
by on May 22, 2020. For personal use only. tech.snmjournals.org Downloaded from

Some computer systems have reregistration programs available that will align images, in which motion has occurred, to the others in the sequence (15). Nonspecific background correction requires the user to choose a representative background area or areas near the thyroid, obtain the average counts per pixel, and subtract this average from all the pixels in the image.
Method 2 The problem of downscatter correction can be avoided by
reversing the imaging sequence and acquiring the 201Tl data first. In addition, 201Tl images and 99mTc images may be acquired for the same total number of counts, producing images of similar count density, and thus normalization is usually not required. This method does require that the patient remain still while the [99mTc]pertechnetate is being accumulated by the thyroid, but we find that a 5-10 min delay is usually adequate to obtain sufficient uptake.
The patient is prepared by placing an indwelling catheter in an arm vein and positioned supine with the neck hyperextended by placing a pillow underneath the shoulders. The head is secured by sandbags and the patient remains in this position throughout the imaging sequence. Thallium-201 chloride (2.7-3.0 mCi) is injected and, after allowing - 1 min for activity in the major vessels to clear, a 100,000 count image is obtained with a general purpose parallel-hole collimator that surveys from the angle of the mandible to the top of the heart. All images are acquired on film and a computer in a 64 x 64 matrix. The collimator is quickly changed to a 2.0 mm pinhole, and the thyroid is positioned anteriorly in the center of the field of view with the surrounding neck area in-
38
FIG. 5. An example of a subclavian artifact. The patient was injected in the left arm.
eluded. A 100,000 count image of 201Tl is acquired. It is necessary to work rapidly in obtaining the 201Tl image. Although we have done no specific washout studies, we have observed rapid washout of the 201Tl from parathyroid tumors. After the 201Tl image is acquired, 5-10 mCi of [99mTc]pertechnetate is injected through a cannula without moving the patient. A 100,000 count image of the thyroid is acquired 5-10 min later. Observation of the thyroid uptake and background clearance on the persistence oscilloscope helps determine when to begin imaging. However, a 10-min limit is not exceeded.
Image processing is a direct subtraction of the 99mTc pinhole image from the 201Tl pinhole image, usually without image normalization or nonspecific background subtraction. Computer images are then photographed on 8 X 10 film.
DISCUSSION
Recent review of our data (19) of surgically confirmed parathyroid adenomas gave a sensitivity of 87%. This represents a 15% increase over what was previously reported by our institution (16). We attribute most of this increase to increased familiarity and adeptness at interpreting the images.
It has been our experience that computer subtraction contributes very little to the overall interpretation of the study. At times, it can make the study more confusing. However, the computer images can enhance the finer details that are more difficult to resolve by eye in the analog images (Fig. 3).
Both imaging methods provide similar information (i.e., comparable sensitivities for the localization of parathyroid tumors), and both are subject to the same artifacts from patient movement and thyroid disease. We prefer Method 2 by virtue
JOURNAL OF NUCLEAR MEDICINE TECHNOLOGY
by on May 22, 2020. For personal use only. tech.snmjournals.org Downloaded from

of its simplicity. Motion correction techniques may improve the diagnostic quality of both methods, but they also present some inherent hazards. Exclusion of frames in which motion has occurred may eliminate a significant amount of data. Computer reregistration techniques for motion correction are only good for motion in the x-y plane of the matrix and will not correct for rotation of the image if it occurs. We have found that thyroid disease, which is common in patients with hyperparathyroidism, causes inhomogenous uptake by the thyroid of both isotopes. This makes interpretation difficult and can lead to false-positive subtraction images. Thyroid disease will often make the subtraction image totally useless (Fig. 3). Makusick, et al. reports an extremely high number of falsepositives in patients with thyroid disease (14) using Method I.
The initial survey image obtained routinely at our institution is not commonly done by other groups; only Winzelberg, et al. acquired a similar image. The survey image is very important in evaluating the mediastinum. We have detected two low mediastinal adenomas which would have been missed on the pinhole images (Fig. 4). When no tumor can be demonstrated in the pinhole images, the survey image may also be valuable in excluding the presence of a mediastinal tumor. A common artifact seen on this image is increased uptake of 201Tl in an area below the clavical on the side of the body in which the thallium was injected (Fig. 5). We believe that this may represent uptake of 201Tl by a valve in the subclavian vein.
Proper subtraction of the 99mTc image from the 201Tl image requires that the images be of a similar count density. If the count densities are not similar, as may be the case with a summed dynamic series acquired for time, the images must be normalized to each other prior to subtraction. If your computer system does not have a reliable normalization program, then a normalization constant can be determined by comparing count densities in areas of apparent normal thyroid uptake in both images, calculating an average ratio of99mTc/201Tl activity, and multiplying the 201Tl image by this factor.
CONCLUSION
If the 201Tl images are properly corrected, summed, and normalized the results from either method of data acquisition should be equivalent. However, as with all computer image manipulation in nuclear medicine, the more you manipulate the data the greater the probability of introducing artifacts. We find Method 2 to be advantageous because of its simplicity and reliability. Our success in the localization of parathyroid tumors is comparable to that of all other groups that have published their results, and our failure to identify four-gland hyperplasia is consistent with most other groups. When combined
VOLUME 14, NUMBER 1, MARCH 1986
with ultrasound (19) of the neck, we have been able to report the location of parathyroid tumors to the surgeons 93 % of the time.
REFERENCES
1. Williams PL, Worwick R, eds. Grays' Anatomy. 36th Edition. Philadelphia: W.B. Saunders, 1980:1453-54.
2. Guyton AC. Textbook of Medical Physiology. 5th Edition. Philadelphia: W.B. Saunders, 1976:1052-71.
3. Sisson JC, Beierwaltes WC. Radiocyanocobalamine (57Co B12) concentration in the parathyroid glands. J Nucl Med 1962;3:160-66.
4. Larose JH, Whitaker RH, Reba PC. Radioiodinated Toluidine blue: An unsatisfactory scanning agent. J Nucl Med 1970;11:731-32.
5. Normann E, Rootwelt K, Salheim D, et al. Use of 131I-Toluidine blue in radionuclide imaging of enlarged parathyroid glands. Ann Chir Gynaecol 1976;65:249-59.
6: Digiulio W, Beierwaltes WH. Parathyroid scanning with "Selenium labeled methionine. J Nucl Med 1964;5:417-27.
7. Potchen EJ, Wilson RE, Dealy JB. External parathyroid scanning with 75Se selenomethionine. Ann Surg 1965;162:492-504.
8. Arkles LB. Experience in parathyroid scanning. AJR 1975;125:634-39. 9. Makiuschi M, Miyakawa M, Sugenoya A, et al. Diagnostic usefulness
of Tl-201 chloride scintigraphy for preoperative localization of parathyroid tumor. Jpn J Surg 1981;3:162-66.
1Q Ferlin G, Conte N, Borsato N, et al. Parathyroid scintigraphy with Cs-131 and Tl-201. J Nucl Med Allied Sci 1981;25:119-23.
11. Ferlin G, Borsato N, Carmerani N, et al. New perspectives in localizing enlarged parathyroids by technetium-thallium subtraction scan. J Nucl Med 1983;24:438-41.
12. Young AG, Gaunt Jl, Croft DN, et al. Localization of parathyroid adenomas by thallium-201 and technetium-99m subtraction scanning. Br Med J 1983;286:1384-86.
13. Ferguson WR, Laird JD, Russell CFJ. Experience with technetiumthallium subtraction imaging of parathyroid lesions. J Nucl Med 1984;25:P19 (abstr).
14. Makusick KA, Palmer EL, Hergenrother J. Is there a role for dual tracer imaging in detection of parathyroid disease? J Nucl Med 1984;25:P19 (abstr).
15. Okerlund MD, Sheldon K, Corpuz S, et al. A new method with high sensitivity and specificity for localization of abnormal parathyroid glands. Ann Surg 1984;200:381-88.
16: MacFarlane SD, Hanelin LG, Taft DA, et al. Localization of abnormal parathyroid glands using thallium-201. Am J Surg 1984;148:7-13.
17. Winzelberg GG, Hydovitz JD, O'Hara KR, et al. Parathyroid adenomas evaluated by Tl-201/Tc-99m pertechnetate subtraction scintigraphy and high resolution ultrasonography. Radiology 1985;155:231-36.
18. Winzelberg GG, Hydovitz JD. Radionuclide imaging of parathyroid tumors: Historical perspectives and newer techniques. Sem Nucl Med 1985;15(Apr):161-70.
19. Lee ME, Hanelin LG, MacFarlane S. Comparison of sensitivity of thallium-201 and ultrasound in the diagnosis of parathyroid disease. Clin Nucl Med 1985;10:P15.
2Q O'Connell JW, Faulkner DB, Ortendahl DA, et al. Color composites: Display of two independent parameters in a single functional image. In Esser PD, ed. Emission Computed Tomography: Current Trends, New York: The Society of Nuclear Medicine, 1983:275-87.
39
by on May 22, 2020. For personal use only. tech.snmjournals.org Downloaded from

1986;14:34-39.J. Nucl. Med. Technol. Barbara Ratliff, Patrick Soon, Steve MacFarlane and Laurence Hanelin Parathyroid Scanning
http://tech.snmjournals.org/content/14/1/34This article and updated information are available at:
http://tech.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNMT can be found at:
http://tech.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0091-4916, Online ISSN: 1535-5675)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published quarterly.Journal of Nuclear Medicine Technology
© Copyright 1986 SNMMI; all rights reserved.
by on May 22, 2020. For personal use only. tech.snmjournals.org Downloaded from