Embed Size (px)
DESCRIPTION
PARATHYROID GLAND PHYSIOLOGY. 99% calcium of our body is in the crystalline form in the skeleton and teeth Of the remaining 1% 0.9% intracellular less than 0.1% in the ECF. The extracellular fluid calcium concentration is about 9.4 mg/dl. - PowerPoint PPT Presentation
Citation preview

PARATHYROID GLAND PHYSIOLOGY

• 99% calcium of our body is in the crystalline form in the skeleton and teeth
• Of the remaining 1%
0.9% intracellular
less than 0.1% in the ECF
• The extracellular fluid calcium concentration is about 9.4 mg/dl

Calcium in Plasma and Interstitial Fluid
• 41% of the calcium is bound with plasma proteins(non-diffusible)
• 9% bound with anionic substances(citrate, phosphate(diffusible, non-ionized)
• Remaining 50% calcium is both diffusible and ionized

Hypocalcemia(low blood calcium)
• Fall in free calcium results in over excitability of nerves and muscles
• Decrease in free calcium increases neuronal sodium permeability with resultant influx of sodium moving the resting potential closer to threshold
Tetany
• Hypocalcemia causes tetany
• At plasma calcium ion concentration about 50% below normal the peripheral nerve fibers become so excitable that they begin to discharge spontaneously
• Tetany usually occurs at calcium conc of 6 mg/dl from normal value of 9 mg/dl

Hypercalcemia (elevated blood calcium)
• Depresses neuro-muscular excitability
• Depressive effects begin to appear at calcium concentration of 12mg/dl (constipation, poor appetite, decreased QT interval)

Role of Free Fraction of ECF Calcium
• Neuromuscular excitability
Even minor variations in concentration of free ECF calcium have profound and immediate impact on the sensitivity of excitable tissues

• Excitation-contraction coupling in cardiac and smooth muscles

• Stimulus-secretion coupling
The entry of calcium into secretory cells which results from increased permeability to calcium in response to appropriate stimulation triggers the release of secretory product by exocytosis

• Excitation-secretion coupling
In pancreatic beta cells calcium entry from the ECF in response to membrane depolarization leads to Insulin secretion

• Maintenance of tight junctions between cells (part of intercellular cement)
• Clotting of blood (acts as a co-factor)

Intracellular Calcium
• Second messenger
• Involved in cell motility
• Calcium in Bone and teeth(structural and functional integrity)

Absorption of Calcium
• Calcium is absorbed from duodenum by carrier mediated active transport and in the rest of small intestine by facilitated diffusion (poorly absorbed)
• Vitamin D is essential for absorption of calcium from GIT

Calcium Excretion
• 98-99% of the filtered calcium is reabsorbed from renal tubules into blood
• 90% of the filtered calcium is reabsorbed from the proximal tubule, loop of Henle and early distal tubule
• Remaining 10% is reabsorbed selectively from the late distal tubule and early collecting ducts depending on calcium conc in blood

Calcium Homeostasis & Calcium Balance
• Urinary excretion of calcium is hormonally controlled
• Absorption of Calcium from intestine is also hormonally controlled and depends on the calcium status of body
• Bones are the large reservoirs of calcium and exchange of calcium between ECF and bone is also subject to hormonal control

Calcium Homeostasis
• Regulation of calcium homeostasis involves the immediate adjustments required to maintain a constant free plasma calcium concentration on a minute-to-minute basis.
• This is mainly accomplished by rapid exchanges between the bone and the ECF and to a lesser extent by modifications in urinary excretion of calcium
Calcium Balance
• Regulation of calcium balance involves the slowly responding adjustments required to maintain a constant total amount of calcium in the body. Calcium is maintained by adjusting the extent of intestinal calcium absorption and urinary calcium excretion

Phosphate
• The average total quantity of phophorus represented by both the ionic forms is 4mg/dl (3-4mg/dl in adults and 4-5mg/dl in children)
• Good Intestinal absorption• Excretion in faeces in combination with
unabsorbed calcium• Remaining absorbed in blood and excreted in
urine
Excretion of Phosphate
• Renal phosphate excretion is controlled by an over-flow mechanism
• When phosphate conc in the plasma is below the critical value of 1mmol/L, all the phosphate in the glomerular filtrate is reabsorbed
• But above this conc the rate of phosphate loss is directly proportional to the additional increase
Bone
• Tough organic matrix strengthened by deposits of calcium salts
• 30% matrix, 70% salts
• Newly formed bone has a higher percentage of matrix than salts

Organic Matrix
• 90-95% collagen fibers(tensile strength) and the remaining homogeneous gelatinous medium called ground substance (ECF plus proteoglycans)
Bone Salts
• Are crystalline salts containing calcium and phosphorus
• Major crystalline salt is Hydroxyapatite
• Magnesium, sodium, potassium and carbonate ions etc are also conjugated
• Collagen fibers and the crystalline salts together give the bony structure extreme tensile and compressional strength

• Hydroxyapatite does not precipitate in the extracellular fluid although the conc of calcium and phosphate ions is considerably greater than those required to cause precipitation of hydroxyapatite
• Role of pyrophosphate (inhibitor of precipitation)

Bone Calcification
• Secretion of collagen molecules (monomers) and ground substance by osteoblasts
• Polymerization of collagen monomers to form collagen fibers (osteoid)
• As osteoid is formed some of the osteoblasts become entrapped in it and become silent (osteocytes)
• Calcium salts begin to precipitate on the surfaces of collagen fibers
• The initial calcium salts are not hydroxyapatite crystals but are amorphous compounds
• By process of substitution, addition, reabsorption these salts are converted into hydroxyapatite crystals over a period of weeks or months

• Some of the salts remain in the amorphous form
• The osteoblasts supposedly secrete a substance into the osteoid that neutralizes the pyrophosphate

Calcium Exchange Between Bone and ECF
• Most of the exchangeable calcium is in the bone
• This exchangeable calcium is in equilibrium with the calcium ions in the extracellular fluid
• The exchangeable calcium provides a buffering mechanism to keep the calcium ion conc in the ECF from rising to excessive levels or falling to low levels
Remodeling of Bone
• Deposition of bone by Osteoblasts
• Absorption of bone by Osteoclasts

• Bone deposition and absorption are normally in equilibrium

Value of Continual Bone Remodelling
• Bone can adjust its strength in proportion to the degree of bone stress.
• The shape of the bone can be rearranged for proper support of mechanical forces by deposition and absorption of bone in accordance with
stress patterns• When old bone becomes brittle and weak new
organic matrix is laid down and normal toughness of bone is maintained
HORMONAL REGULATION OF CALCIUM AND
PHOSPHATE HOMEOSTASIS
• PTH
• Vitamin D
• Calcitonin

PARATHYROID GLANDS
• Four glands located on the posterior surface of the thyroid gland
• Derived from the 3rd and 4th pharangeal pouches
• Chief cells secrete the polypeptide hormone PTH

TARGET ORGANS FOR PTH
• Bone
• Kidney
• Hyperfunction of Parathyroid gland-------Hypercalcemia
• Hypofunction of Parathyroid gland---------Hypocalcemia
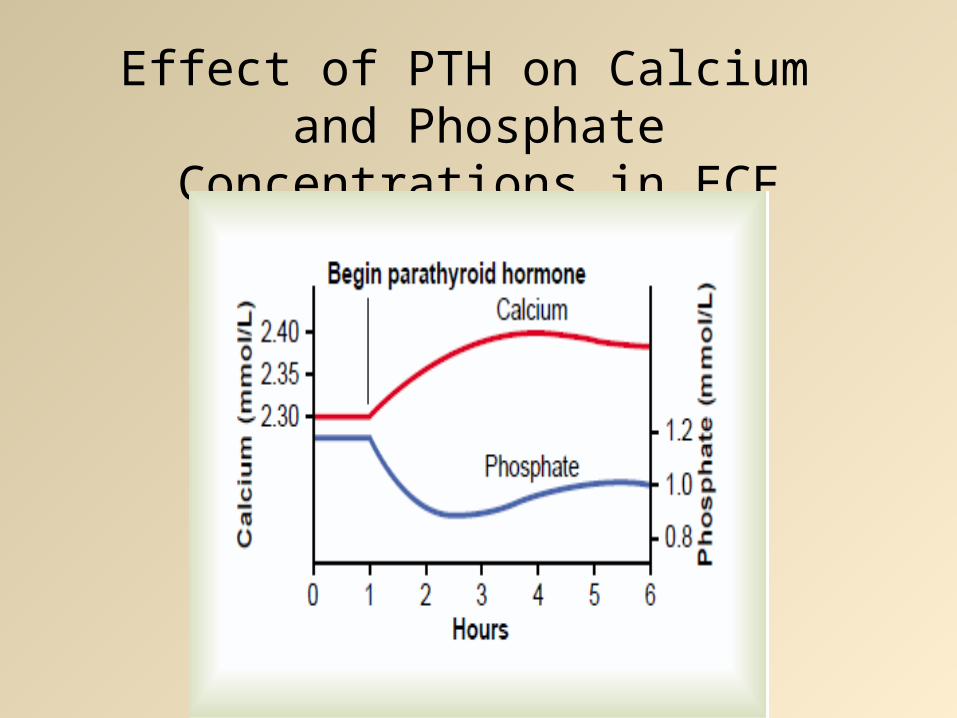
Effect of PTH on Calcium and Phosphate Concentrations in ECF
• Rise in calcium levels is due to
1.Effect of PTH to increase calcium and phosphate absorption from bone
2.Rapid effect of PTH to decrease the excretion of calcium by kidneys
• The decrease in Phosphate conc is due to
1.Effect of PTH to increase renal phosphate excretion

ACTIONS OF PTH ON BONE
• Rapid Phase - osteocytic osteolysis
• Slow Phase - osteoclastic osteolysis
Osteocytic Osteolysis
• The calcium ion conc in the blood begins to rise with in minutes
• There is removal of bone salts
1.From the bone matrix in the vicinity of osteocytes
2.In the vicinity of osteoblasts along the bone surface

Osteocytic Membrane System
• Long processes extend from osteocyte to osteocyte through out the bone structure and theses processes also connect with the surface osteocytes and osteoblasts
• This membrane separates the bone from ECF
• Between the processes and the bone there is small amount of bone fluid


Osteolysis
• The osteocytic membrane pumps calcium ions from bone fluid into ECF
• When it becomes excessively activated the bone fluid calcium conc falls and calcium and phosphate salts are absorbed from the bone (osteolysis)
• When the pump is inactivated the bone fluid calcium conc rises and calcium and phosphate salts are deposited in the bone

• The cell membranes of both osteoblasts and osteocytes have receptors for binding PTH
• PTH strongly stimulates Calcium pump by increasing the calcium permeability of bone fluid side of osteocytic membrane

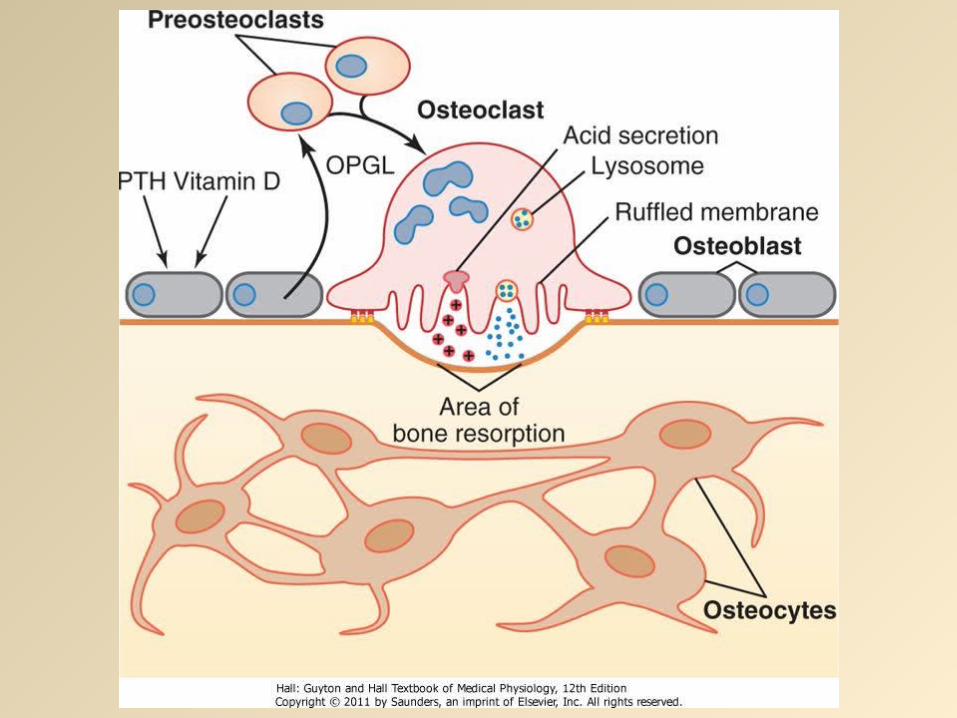
Slow phase of bone absorption and calcium phosphate release
• Immediate activation of already formed osteoclasts
• Increased osteoclastic size and number• Increased osteoclastic collagenase and lysosomal
enzyme activity • Increased osteoclastic acid phosphatase,carbonic
anhydrase,lactic acid and citric acid concentrations• Increased bone resorption
• Osteoclasts do not have membrane receptors for PTH.
• The activated osteoblasts and osteocytes send secondary "signals" to the osteoclasts (OPGL)
Activation of Osteoblats
• Excess PTH stimulated osteoclastic resorption of bone can lead to weakened bones and secondary stimulation of the osteoblasts that attempt to correct the weakened state
PTH ACTIONS ON KIDNEY
• Increased reabsorption of calcium, magnesium and hydrogen ions
• Decreased reabsorption of phosphate, sodium and potassium ions
• Increased alpha-1-hydroxalase activity

Effect of PTH on Intestinal Absorption of Calcium&Phosphate
• PTH greatly enhances both calcium and phosphate absorption from the intestines by increasing the formation in the kidneys of 1,25-dihydroxycholecalciferol

• cAMP mediates the effects of Parathyroid Hormone



Vitamin D
• Several compounds derived from sterols belong to vitamin D family
• They all perform more or less same functions
• Vitamin D3(cholecalciferol) is the most important of these
• Vitamin D receptors are present in the nuclei of target cells



Actions of Vitamin D
• It promotes Intestinal calcium absorption
• Role of Calbindins in the intestinal epithelial cells
• It also promotes Phosphate absorption from the intestine (directly & through calcium)
• It decreases renal calcium and phosphate excretion (weak effect)

Actions on Bone
• The administration of extreme quantities of vitamin D causes absorption of bone
• In the absence of vitamin D the effect of PTH in causing bone absorption is greatly reduced
• Vitamin D in smaller quantities promotes bone calcification

• These results are due to the effect of 1,25-dihydroxycholecalciferol to increase calcium transport through the cellular membranes
• Calcium ion conc controls the formation of 1,25-Dihydroxycholecalciferol
• Formation of 1,25Dihydroxycholecalciferol in the kidneys is controlled by PTH

CALCITONIN
• Polypeptide hormone
• Synthesized and secreted by the parafollicular C-cells of the thyroid gland

• Increased plasma calcium concentration stimulates Calcitonin secretion
• Calcitonin decreases plasma calcium concentration

ACTIONS OF CALCITONIN ON BONE
• Decreased osteoclastic activity
• Decreased osteoclastic number (decreased formation of osteoclasts)
• The net result is reduced osteoblastic and osteoclastic activity

• The actions of calcitonin on kidneys and intestines are opposite to that of PTH(minor effects)
• Calcitonin has a weak effect on plasma calcium concentration in adults

Control of PTH secretion by Calcium Concentration
• Decrease in calcium conc increases PTH secretion
• Persistent decrease leads to hypertrophy of the gland
(rickets, pregnancy, lactation)

• Increase in calcium conc decreases PTH secretion
• Persistent increase leads to reduced activity and size of the glands
(excess calcium and vitamin D in diet, diseases causing bone resorption)

• Changes in ECF calcium ion conc are detected by calcium-sensing receptor (CaSR) in parathyroid cell membranes

• CaSR is a G-protein coupled receptor when activated by calcium ions activates phospholipase C and increases intracellular inositol triphosophate and diacylglycerol formation. This stimulates release of calcium from intracellular stores which decreases PTH secretion. Decreased extracellular fluid calcium ion concentration inhibits these pathways and stimulates PTH secretion

• Buffer Function of the Exchangeable Calcium in Bones-The First Line of Defense
• an increase in the concentrations of extracellular fluid calcium and phosphate ions above normal causes immediate deposition of exchangeable salt.
• decrease in these concentrations causes immediate absorption of exchangeable salt
•

• Mitochondria especially of the liver and intestine, contain a significant amount of exchangeable calcium that provides an additional buffer system for helping to maintain constancy of the extracellular fluid calcium ion concentration

• Hormonal Control of Calcium Ion Concentration-The Second Line of Defense
• At the same time that the exchangeable calcium mechanism in the bones is "buffering" the calcium in the extracellular fluid, both the parathyroid and the calcitonin hormonal systems begin to act. Within 3 to 5 minutes after an acute increase in the calcium ion concentration, the rate of PTH secretion decreases

• In prolonged calcium excess or prolonged calcium deficiency, only the PTH mechanism seems to be really important in maintaining a normal plasma calcium ion concentration

Hypoparathyroidism• When parathyroid glands do not produce
sufficient amounts of PTH During thyroid surgery surgical removal of
parathyroid gland can cause hypoparathyroidism
ParathyroidectomyAutoimmune diseaseDeficiency of receptors for PTH

• The osteoclasts become almost totally inactive. As a result calcium reabsorption from the bones is so depressed that the level of calcium in the body fluids decreases.

• When the parathyroid glands are suddenly removed, the calcium level in the blood falls from the normal of 9.4 mg/dl to 6 to 7 mg/dl within 2 to 3 days and the blood phosphate concentration may double. When this low calcium level is reached the usual signs of tetany develop.

Sign and Symptoms
• Hyper-reflexia and convulsions
• Carpopedal spasm
• Laryngeal stridor
• Cardiovascular changes ( e.g prolonged QT interval, hypotension, arrhythmia)


SIGNS OF HYPOPARATHYROIDISM
• Positive Chvostek’s (facial muscle twitch) sign
• Positive Trousseau’s (carpal spasm) sign
• prolongation of the QT interval

• Treatment of Hypoparathyroidism includes PTH and Vitamin D, Calcium infusion
Hyperparathyroidism
• Disease of “Bones, Stones, Abdominal groans”

Primary Hyperparathyroidism
• The cause of primary hyperparathyroidism is tumor of one of the parathyroid glands which are more common in women than in men or children mainly because pregnancy and lactation stimulate the parathyroid glands and therefore predispose to the development of such a tumor.

• Hyperparathyroidism causes extreme osteoclastic activity in the bones. This elevates the calcium ion concentration in the extracellular fluid while usually depressing the concentration of phosphate ions because of increased renal excretion of phosphate
Bone Disease in Hyperparathyroidism
• In mild hyperparathyroidism new bone can be deposited rapidly enough to compensate for the increased osteoclastic resorption of bone but in severe hyperparathyroidism the osteoclastic absorption is more than osteoblastic deposition, and the bone may be eaten away almost entirely.

Osteitis Fibrosa Cystica• The reason a hyperparathyroid person seeks
medical attention is often a broken bone. Radiographs of the bone typically show extensive decalcification and occasionally large punched-out cystic areas of the bone that are filled with osteoclasts in the form of so-called giant cell osteoclast "tumors." The cystic bone disease of hyperparathyroidism is called osteitis fibrosa cystica.

• When the osteoblasts become active, they secrete large quantities of alkaline phosphatase. Therefore one of the important diagnostic findings in hyperparathyroidism is a high level of plasma alkaline phosphatase
Effects of Hypercalcemia in Hyperparathyroidism
• Depression of the central and peripheral nervous systems, muscle weakness, constipation, abdominal pain, peptic ulcer, lack of appetite

Parathyroid Poisoning and Metastatic Calcification
• The calcium and phosphate in the body fluids become greatly supersaturated, so calcium phosphate (CaHPO4) crystals begin to deposit in the alveoli of the lungs, the tubules of the kidneys, the thyroid gland, the acid-producing area of the stomach mucosa, and the walls of the arteries throughout the body.
• The level of calcium in the blood must rise above 17 mg/dl before there is danger of parathyroid poisoning, but once such elevation develops along with concurrent elevation of phosphate, death can occur in few days.

Formation of Kidney Stones in Hyperparathyroidism
• The patients of hyperparathyroidism have an extreme tendency to form kidney stones. The reason is that the excess calcium and phosphate absorbed from the intestines or mobilized from the bones is excreted by the kidneys causing a proportionate increase in the concentrations of these substances in the urine.

• As a result crystals of calcium phosphate tend to precipitate in the kidney forming calcium phosphate stones. Also calcium oxalate stones develop because even normal levels of oxalate cause calcium precipitation at high calcium levels
Secondary Hyperparathyroidism
• In secondary hyperparathyroidism high levels of PTH occur as a compensation for hypocalcemia rather than as a primary abnormality of the parathyroid glands.

• Secondary hyperparathyroidism can be caused by vitamin D deficiency or chronic renal disease in which the damaged kidneys are unable to produce sufficient amounts of the active form of vitamin D, 1,25-dihydroxycholecalciferol.

Rickets• Rickets occurs in children.
• It results from calcium or phosphate deficiency in the extracellular fluid caused by lack of vitamin D.
• If the child is adequately exposed to sunlight, the 7-dehydrocholesterol in the skin becomes activated by the ultraviolet rays and forms vitamin D3, which prevents rickets by promoting calcium and phosphate absorption from the intestines
Plasma Concentrations of Calcium and Phosphate Decrease in Rickets
• The plasma calcium concentration in rickets is only slightly depressed but the level of phosphate is greatly depressed.
Rickets Weakens the Bones
• During prolonged rickets the marked compensatory increase in PTH secretion causes extreme osteoclastic absorption of the bone this in turn causes rapid osteoblastic activity
• The osteoblasts lay down large quantities of osteoid which does not become calcified because of insufficient calcium and phosphate ions.
Tetany in Rickets
• In the early stages of rickets, tetany almost never occurs because the parathyroid glands maintain almost normal level of calcium in the extracellular fluid.
• When the bones finally become exhausted of calcium, the level of calcium may fall rapidly. As the blood level of calcium falls below 7 mg/dl, the usual signs of tetany develop.
Treatment of Rickets
• The treatment of rickets depends on supplying adequate calcium and phosphate in the diet and on administering large amounts of vitamin D.

Osteomalacia-Adult Rickets
• Deficiency of both vitamin D and calcium occasionally occur as a result of steatorrhea (failure to absorb fat) because vitamin D is fat-soluble vitamin
• This almost never proceeds to the stage of tetany but often is a cause of severe bone disability

Osteomalacia and Rickets Caused by Renal Disease
• Renal rickets is a type of osteomalacia that results from prolonged kidney damage

Congenital hypophosphatemia
• This results from congenitally reduced reabsorption of phosphates by the renal tubules. This type of rickets must be treated with phosphate compounds instead of calcium and vitamin D, and it is called vitamin D-resistant rickets.

Osteoporosis (porous bones)-Decreased Bone Matrix
• Osteoporosis is the most common of all bone diseases in adults especially in old age
• It results from diminished organic bone matrix
• excessive bone resorption and decreased bone formation

• Loss of bone matrix and strength
• Bones become fragile with high risk of fracture

(1) lack of physical stress on the bones because of inactivity
(2) malnutrition to the extent that sufficient protein matrix cannot be formed

(4) postmenopausal lack of estrogen secretion because estrogens decrease the number and activity of osteoclasts
(5) old age in which growth hormone and other growth factors diminish greatly plus the fact that many of the protein anabolic functions also deteriorate with age

(6) Cushing's syndrome, massive quantities of glucocorticoids secreted in this disease cause decreased deposition of protein throughout the body and increased catabolism of protein and have depressive effect on osteoblastic activity