Embed Size (px)
Citation preview

PAPERS
Maternal serum screening for Down's syndrome in earlypregnancy
Nicholas J Wald, Howard S Cuckle, JamesW Densem, Kiran Nanchahal, Patrick Royston,Tim Chard, James E Haddow, George J Knight, Glenn E Palomaki, Jacob A Canick
Department ofEnvironmental andPreventive Medicine,Medical College of StBartholomew's Hospital,London ECIM 6BQNicholas J Wald, FRCP,professorHoward S Cuckle, DPHIL,CRC technical lecturerJamesW Densem, PHD,computer managerKiran Nanchahal, MSC,computer scientistPatrick Royston, MSC,lecturer
Department ofReproductive Physiology,St Bartholomew's Hospital,London ECIA 7BGTim Chard,FRCOG, professor
Foundation for BloodResearch, PO Box 190,Scarborough, Maine,United StatesJames E Haddow, MD,associate medical directorGeorge J Knight, PHD,director, immunoassaylaboratoryGlenn E Palomaki,Bs,biostatistician
Department of Pathologyand Laboratory Medicine,Brown University, Womenand Infant's Hospital,Providence, Rhode Island,United StatesJacob A Canick, PHD,associate professor
Correspondence to:Professor Wald.
AbstractThe possibility of improving the effectiveness ofantenatal screening for Down's syndrome bymeasuring human chorionic gonadotrophin concen-trations in maternal serum during the secondtrimester to select women for diagnostic amnio-centesis was examined. The median maternal serumhuman chorionic gonadotrophin concentration in 77pregnancies associated with Down's syndrome wastwice the median concentration in 385 unaffectedpregnancies matched for maternal age, gestationalage, and duration of storage of the serum sample.Measuring human chorionic gonadotrophin inmaternal serum was an effective screening test,giving a lower false positive rate (3%) at a 30%detection rate than that for maternal age (5%) and thetwo existing serum screening tests, unconjugatedoestriol (7%) and a fetoprotein (11%). The mosteffective screening results were obtained with allfour variables combined; at the same 30% detectionrate the false positive rate declined to 0-5%.The new screening method would detect over 60%
of affected pregnancies, more than double thatachievable with the same amniocentesis rate inexisting programmes (5%), and could reduce thenumber of children bom with Down's syndrome inthe United Kingdom from about 900 a year to about350 a year.
IntroductionDown's syndrome is the most common congenital
cause of severe mental retardation, with an incidence atbirth of about 1-3 per 1000. The current method ofantenatal screening is to select women for a diagnosticamniocentesis on the basis of advanced age. Age is,however, a poor basis for screening and has had littleimpact on the incidence at birth. With age as a basis forscreening only about 30% of all Down's syndromepregnancies can be detected by carrying out amnio-centesis on the 5% of women most at risk-that is,those aged 36 years or greater-though in practicefewer than 15% of affected pregnancies are detectedbecause fewer than half of these older women actuallyhave amniocentesis.' Additional antenatal screeningtests such as maternal serum measurements of cfetoprotein and unconjugated oestriol can increasethe rate of detection to about 45% if the 5% of pregnantwomen at highest risk undergo amniocentesis.-
Recently Bogart and his colleagues found thathuman chorionic gonadotrophin concentrations in thematernal serum during the second trimester weresignificantly higher in pregnancies with chromosom-ally abnormal fetuses than in unaffected pregnancies.3The study included 17 cases of Down's syndrome, ofwhich 11 (65%) had human chorionic gonadotrophin
concentrations greater than 20 IU/ml compared withonly one among 74 unaffected pregnancies (1 4%).These results encouraged us to assess whether humanchorionic gonadotrophin measurement might be aworthwhile antenatal screening test for Down'ssyndrome used either alone or in combination withthose already available.
MethodsOur study population consisted of women who
attended the John Radcliffe Hospital, Oxford, for theirantenatal care between 1973 and 1983. During thistime a sample ofserum was collected from each womanand stored at -40°C. In the antenatal serum bank thatwas accumulated in this way serum was available fromall 77 singleton pregnancies associated with Down'ssyndrome. For each of these, five unaffected singletoncontrol pregnancies were identified. The controls werematched with each case for maternal age (within thesame year), gestational age (usually within one week),and duration of storage of sample (within one year).The serum from these 77 cases and 385 controls hadbeen previously used to investigate unconjugatedoestriol and a fetoprotein concentrations as antenatalscreening tests for Down's syndrome.2The samples were assayed for human chorionic
gonadotrophin, with an immunoradiometric assay(Serono MAIA-clone kit calibrated to the first inter-national reference preparation) at a dilution of 1 in 500.All the assays were performed within three days, andcases and controls were always assayed in the sameanalytical batch without knowing whether the sampleswere from affected or unaffected pregnancies.As the assays were performed under research con-
ditions an estimate of the long term between batchassay variance was obtained, and this was added tothe estimate of the observed variances of maternalserum human chorionic gonadotrophin concentrationsin affected and unaffected pregnancies at each week ofpregnancy to yield estimates of the standard deviationsthat would be found in routine practice. The longterm variance was derived from two quality controlspecimens with mean human chorionic gonadotrophinconcentrations of 22 IU/ml and 75 IU/ml that had beenassayed 122 and 163 times, respectively, over sixmonths.To allow for the appreciable decline in maternal
serum human chorionic gonadotrophin concentrationin the second trimester of pregnancy, humanchorionic gonadotrophin concentrations were ex-pressed in multiples of the median (MoM) for un-affected pregnancies of the same gestational age.Because at some weeks of gestation there were too fewpregnancies to provide reliable medians a regressionof human chorionic gonadotrophin concentration ongestational age among unaffected pregnancies was
BMJ VOLUME 297 8 OCTOBER 1988 883
on 9 Decem
ber 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.297.6653.883 on 8 O
ctober 1988. Dow
nloaded from

performed to yield "regressed" normal medians. Weused an exponential regression, incorporating aconstant term, of the median human chorionic gonado-trophin concentration and median gestation (in days)for pregnancies in each completed week of pregnancyfrom 13 to 27, weighted for the number of women ateachweek(7, 3,20, 122, 113, 50, 29, 19, 11, 1,2,0,3,0, and 5, respectively). The equation of the regression
250200
150 X
100
50
10
.
.04 00
09
0 :0
0
\ 0
NN, 5
0O5MoM
51.13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28
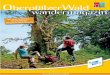
Gestational age (weeks)FIG 1-Human chorionic gonadotrophin concentrations in maternal serum in 77 pregnancies with Down'ssyndrome, and regressed medians derived from 385 unaffected pregnancies. MoM =Multiple of medianvalue for unaffected pregnancies ofthe same gestational age
TABLE I-Number (percentage) of Down's syndrome and unaffectedpregnancies
Maternal serumhuman chorionic No (%) of No (%) ofgonadotrophin Down's syndrome unaffectedconcentration pregnancies pregnancies
(MoM) (n=77) (n= 385)
Ii00 66(86) 195(51)w125 60 (78) 129 (34)- l150 56 (73) 96 (25)al-75 49 (64) 64 (17)2-00 42 (55) 40 (10)-2-25 29 (38) 26 (7)w2-50 25 (32) 17 (4)-2 75 21 (27) 11 (3)-3 00 17 (22) 8 (2)
MoM=Multiple of median value for unaffected pregnancies of samegestational age.
c
a0
, 0
0
oc,o
C,
C -
0as
00
Unaffected
0-2 03 0405
Down's syndrome
1.0 2 0 3 0 4 0 5-0 10
Maternal serum human chorionic gonadotrophin(MoM) [log scale]
FIG 3-Gaussian frequency distributions oflog maternal serum humanchonionic gonadotrophin concentration in Down's syndrome and un-affected pregnancies, with standard deviations increased to allow forlong term imprecisions in assays. MoM=Multiple of median forunaffected pregnancies ofsame gestational age
line was: human chorionic gonadotrophin concentra-tion (IU/ml)=16 00+23 28 e 0061 (dayst5O) The valuesthat were observed and those predicted from theregression line were very close: at 13-15 weeks theywere 33 IU/ml and 31 IU/ml, respectively, at 16-18weeks 22 IU/ml and 22 IU/ml, at 19-21 weeks 19 IU/mland 18 IU/ml, and at 22-27 weeks 14 IU/ml and16 IU/ml.The means and standard deviations used in the dis-
tributions were estimated from the observed mediansand the ranges between the 10th and 90th centiles forthe variables concerned. Following usual practice"detection rate" is defined as the proportion of affectedpregnancies that gave positive results and "false posi-tive rate" is defined as the proportion of unaffectedpregnancies that gave positive results.
ResultsMATERNAL SERUM HUMAN CHORIONIC GONADOTROPHIN
Figure 1 shows the individual human chorionicgonadotrophin concentrations for each pregnancyassociated with Down's syndrome, together with theregressed median for unaffected pregnancies and linescorresponding to 0 5 MoM and 2-0 MoM, which wereroughly equivalent to the 10th and 90th centiles of thenormal range. The precise values of these centiles were0 51 and 2-01, respectively. The median humanchorionic gonadotrophin concentration in Down'ssyndrome pregnancies was 2 04 MoM, significantlyhigher than that in unaffected pregnancies (p<0-001,based on an analysis of variance of ranks withinmatched sets; 95% confidence interval 1-72 to 2-42MoM). The 10th and 90th centiles for affected preg-nancies were 0 90 MoM and 4- 13 MoM, respectively.
Table I shows the observed numbers and propor-tions of affected and unaffected pregnancies withmaternal serum human chorionic gonadotrophinvalues greater than or equal to specified values. Figure2 is a probability plot of the human chorionic gonado-trophin concentrations (expressed in logarithms) foraffected and unaffected pregnancies. The humanchorionic gonadotrophin values for each group ofpregnancies form a straight line, showing that they aredistributed in a Gaussian manner. There was nosignificant deviation from the fitted Gaussian distribu-tions (p=0-98 for Down's syndrome and p=0-56 forunaffected pregnancies). Figure 3, which shows theextent of discrimination between affected and un-affected pregnancies that would apply if this test wereto be used in antenatal screening, shows the distribu-tions, with standard deviations increased to allow forlong term assay imprecision. The discriminationwas greater than that achievable by screening usingmaternal age alone, maternal serum a fetoproteinconcentration alone, or maternal serum unconjugatedoestriol concentration alone. At human chorionicgonadotrophin cut off levels that would yield detection
BMJ VOLUME 297 8 OCTOBER 1988
c0
0
cn-~0cm
c _i0E cmu =c-
C
CentileFIG 2-Probability plot of centiles of human chorionic gonadotrophin in moternal serum in Down'ssyndrome and unaffected pregnancies. Continuous lines are those defined byfitted Gaussian distributions (seestatistical appendix). MoM =Multiple ofmedian for unaffected pregnancies ofsame gestational age
884
on 9 Decem
ber 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.297.6653.883 on 8 O
ctober 1988. Dow
nloaded from

rates of 20%, 30%, 40%, and 50%, the estimated falsepositive rates would be 2%, 3%, 7%, and 10%,respectively. The corresponding false positive rates forscreening using maternal age would be 2%, 5%, 11%,and 19% using the age distribution of pregnancies forEngland and Wales in 1981-5 (see footnote to table 4 inWald and Cuckle'); for screening using a fetoproteinmeasurement the false positive rates would be 6%,11%, 17%, and 24%, and for unconjugated oestriol,4%, 7%, 11%, and 16%.2
COMBINING SCREENING TESTS
When using several variables in combination toscreen for a particular disorder it is necessary to
TABLE i1-Median human chorionic gonadotrophin concentrations inDown's syndrome and unaffected pregnancies by maternal age andserum unconjugated oestriol and cc fetoprotein concentrations
Down's syndrome Unaffectedpregnancies pregnanciesMlo.NM (No) MNoM (No)
Age (years):<30 1-94(20) 1-10(100)30- 1-62 17) 0-96 (85)35- 2-11 (19) 095 '95)40 2-19 (21 1-02(105)
Unconjugated oestriol concentration (MloMN):<0-60 2-71 20) 1-25 (19)0-60- 188 20) 121 (36>0-75- 1 85(18! 0-97 (77)0-90 1-84(19) 1-00(253)
u Fetoprotein concentration (MoM):<0-60 1-64(17) 1-02 (22)0-60- 2-05 (24) 0-91 (75)0-80- 2-12 (23) 0-89 (95)
I 00 2-24 (13) 1-10 (193)
Total 2-04 (77) 1-02 (385)
.NMoMNi=Multiple of median value for unaffected pregnancies of samegestational age.
TABLE III-Probability of a 35 year old woman having a Down'ssyndrome term pregnancy according to selected maternal serum humanchorionic gonadotrophin, unconjugated oestriol, and ca fetoproteinconcentrations
HumanUnconjugated chorionic
oestriol gonadotrophin (e Fetoprotein concentration (.MoM)concentration concentration
(MoM) (MNo\M) 0-4 1.0 2-5
0-5 1:370 1:2800 1:220000-4 1.0 1:84 1:480 1:2800
2-0 1:16 1:69 1:3100-5 1:820 1:4800 1:28000
1-0 1-0 1:330 1:1400 1:64002-0 1:110 1:360 1:12000- 5 1:2200 1:11000 1:52000
1-4 1-0 1:1300 1:4600 1:170002-0 1:630 1:1 700 1:4 700
MoM==Multiple of median value for unaffected pregnancies of samegestational age.
assess the extent of correlation among the variablesconcerned. Iftwo variables are perfectly correlated oneadds nothing to the other in determining the risk ofhaving the disorder; if they are completely unrelatedeach provides an independent measure of risk. If theyare partially correlated there will be some independentinformation. We therefore examined the associationsbetween human chorionic gonadotrophin and maternalage, unconjugated oestriol concentrations, and afetoprotein concentrations in affected and unaffectedpregnancies (table II). There was no evidence of anassociation between human chorionic gonadotrophinconcentrations and maternal age, but there was a smallnegative association between human chorionic gonado-trophin and unconjugated oestriol concentrations.The relation between human chorionic gonadotrophinand a fetoprotein concentrations was less evident, butas unconjugated oestriol and a fetoprotein concen-trations have been shown to be associated,2 and humanchorionic gonadotrophin and unconjugated oestriolconcentrations are associated, there probably is anunderlying association. The correlation coefficientsbetween the serum variables are given in the statisticalappendix together with a description and validation ofthe statistical methods used to estimate a woman's riskof having an affected pregnancy from information onher age and biochemical test results.
Table III shows the risk of having a Down'ssyndrome term pregnancy according to selected valuesof the three biochemical screening tests as they wouldapply to a 35 year old woman. It shows how, if theresults of any two tests are known, the third is stillinformative. For example, if a 35 year old woman hadan a fetoprotein concentration of 1-0 MoM and anunconjugated oestriol concentration of 0-4 MoM,the risk would be 1:2800 at a human chorionicgonadotrophin concentration of 0-5 MoM and 1:69 at2-0 MoM.When screening with several tests simultaneously a
difficulty arises because no single cut off level for eachof the tests will be suitable; the cut off level for any onetest will depend on the results of the others. A simplesolution is to estimate each woman's risk of having aDown's syndrome pregnancy as in table III and to usethis risk estimate as the screening variable in much thesame way as if it were the result of a biochemical test.Table IV shows the estimated false positive rateassociated with specified detection rates of Down'ssyndrome using maternal age together with variouscombinations of concentrations of human chorionicgonadotrophin, a fetoprotein, and unconjugatedoestriol in maternal serum (see statistical appendix).The table shows the extra benefit of using differentcombinations of tests. If only two of the three bio-chemical tests are to be used a fetoprotein and human
TABLE i\ - False positive rates corresponding to specified detection rates ofDown's syndrome using maternal age and serum ctfetoprotein, unconjugated oestriol, and human chorionicgonadotrophin concentrations alone or in combination*
False positive rate (%( for age with:
o Fetoprotein,a Fetoprotein and Unconjugated oestriol unconjugated oestriol,
Unconjugated Human chorionic ca Fetoprotein and human chorionic and human chorionic and human chorionicDetection rate (%K of a Fetoprotein oestriol gonadotrophin unconjugated oestriol gonadotrophin gonadotrophin gonadotrophinDown's syndrome concentration concentration concentration concentrations concentrations concentrations concentrations
80 44 34 27 29 20 20 1675 37 27 21 23 15 15 1270 30 22 16 18 12 1 1 8-665 25 18 12 15 8-8 8-1 6-460 20 14 9-5 12 6-7 6-0 4-755 16 11 7-2 9-1 5-0 4-4 3-450 12 8-8 5-4 7-0 3-7 3-2 2-545 9-8 6-7 3-9 5-3 2-7 2-3 1-740 7-3 5-0 2-8 3-9 1-9 1-6 1-235 5-3 3-7 1-9 2-8 1-3 1-0 0-830 3-6 2-5 1-2 1-9 0-8 0-7 0-525 2-2 1-6 0-8 1-2 0-5 0-4 0-320 1-3 0-9 0-4 0-7 0-3 0-2 0-2
*Result is positive if risk of Down's svndrome is high when estimated from maternal age and results of biochemical test or tests.
BMJ VOLUME 297 8 OCTOBER 1988 885
on 9 Decem
ber 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.297.6653.883 on 8 O
ctober 1988. Dow
nloaded from

chorionic gonadotrophin concentrations is the pair ofchoice, as a fetoprotein concentration is of separatevalue in screening for neural tube defects and theperformance of a fetoprotein and human chorionicgonadotrophin concentrations in combination is notmuch worse than that of unconjugated oestriol andhuman chorionic gonadotrophin concentrations incombination. The best overall results are, however,obtained by using all three tests together with maternalage. This yielded, for example, a detection rate of60%with a false positive rate of 5%.The false positive rates shown in the table are subject
to errors in estimation, the extent of which will dependon the numbers of pregnancies studied. We carried outa sensitivity analysis, varying the underlying statisticalparameter (means, standard deviations, and correla-tion coefficients). This showed that our estimates arelikely to be reasonably reliable. For example, in tableIV, in which the estimated false positive rate is shownto be 5%, further studies would be unlikely to yieldestimates outside the range 4-6%.
Screening centres will need to know the effect ofusing different cut off levels of risk on the detectionrates and false positive rates as well as on the prob-ability of being affected given a positive result. TableV shows these rates for different combinations ofscreening variables with six selected cut off levels ofrisk.
karyotypes that would otherwise be needed to obtainthe same detection rate. For example, to achieve 60%detection, out ofevery 1000 women screened using ageand all three biochemical tests 48 (47 unaffected andabout one affected) would need an amniocentesis and akaryotype compared with 201 (200 unaffected andabout one affected) using age and a fetoprotein concen-tration alone (table IV). The cost of 153 amniocentesesand karyotypes saved would be about five times higherthan the cost of 1000 human chorionic gonadotrophinand unconjugated oestriol tests. Implementing suchscreening should be straightforward but will probablyrequire computer software capable of interpretingcombined test results.Our results imply that maternal age should no longer
be regarded as the primary screening variable; it issimply one of several variables that need to be used incombination for all pregnant women. For example, itwould be illogical to offer amniocentesis to all womenabove a certain age and to restrict the use of thebiochemical tests to younger women, as some may beinclined to do because of a reluctance to withholdamniocentesis from some women who would have itunder current medical practice. If such a selectiveapproach were adopted some older women with a fairlylow risk would have an amniocentesis while someyounger women with a higher risk would not.The effectiveness of maternal serum screening for
TABLE v-Down's syndrome detection rate (DR), false positive rate (FPR), and odds ofbeing affected given a positive result (OAPR)* for maternal age and serum human chorionicgonadotrophin concentration alone or combined with ai fetoprotein and unconjugated oestriol concentrations according to risk cut off level
Age and human chorionic gonadotrophin concentration
With (t fetoprotein With unconjugated oestriol With o fetoprotein and unconjugatedconcentration concentration oestriol concentrations
Risk cut offlevel DR (%) FPR (%) OAPR DR (%) FPR(%) OAPR DR (%) FPR (%) OAPR DR (%) FPR (%) OAPR
1:100 32 1i5 1:36 38 1-6 1:34 40 1-6 1:31 44 1 7 1:291:150 39 2-6 1:52 45t 2-8 1:48 48 2-7 1:45 52 2-8 1:421:200 45t 4 0 1:69 51 4-0 1:62 53 3-9 1:58 57 3-9 1:541:250 49 5 1 1:81 56 5 3 1:74 57 5-1 1:70 61 5-0 1:651:300 54 6-6 1:97 59 6-5 1:86 61 6-2 1:81 64 6-1 1:751:350 56 7-7 1:107 63 7-8 1:98 63 7-4 1:92 67 7-2 1:85
*Result is positive if risk of a Down's syndrome term pregnancy ¢ cut off risk.tDifferences between false positive rates for 45% detection rate shown here and those in table IV are due to rounding. Exact detection rates are 45 3% for age and human chorionic gonadotrophinconcentration and 45-4% for age and human chorionic gonadotrophin and o fetoprotein concentrations.
DiscussionOur data confirm the observation reported by Bogart
et al that human chorionic gonadotrophin concentra-tions in maternal serum are high in Down's syndromepregnancies.3 The explanation for this finding is notknown, but it may be due to fetuses with Down'ssyndrome (and their placentas) being immature, anexplanation we have suggested for the low a feto-protein and unconjugated oestriol concentrationsfound in affected pregnancies.4 Human chorionicgonadotrophin in maternal serum is derived fromthe placenta, and concentrations decline appreciablybetween about 10 and 20 weeks of pregnancy. If a fetusthat had Down's syndrome were immature and thisproduced a human chorionic gonadotrophin concen-tration typical of pregnancies about three weeksearlier this would account for the observed differencein maternal serum human chorionic gonadotrophinconcentrations between affected and unaffected preg-nancies.
Antenatal screening programmes for Down'ssyndrome using maternal age and all three biochemicalvariables in combination would be cost effective. As wehave indicated, an ac fetoprotein test is likely to beperformed routinely as part of an antenatal screeningprogramme for neural tube defects. At any levelof detection the extra cost of the human chorionicgonadotrophin and unconjugated oestriol tests wouldbe much less than the cost of the amniocenteses and
Down's syndrome might be improved still further byultrasound screening measuring, for example, fetalfemur length as a complementary technique.5 6 If so, itwould be necessary to allow for correlations betweenthe ultrasound measures and the serum markers, asthey may not be independent measures of risk.Our results indicate that it is now possible to screen
pregnant women for Down's syndrome using maternalage and the results of simple blood tests and therebyidentify about 60% of all affected pregnancies within agroup comprising about 5% of all pregnancies. Such apolicy would not require extra resources for diagnosticprocedures as in many existing screening programmesbased on maternal age alone resources have alreadybeen provided to ensure that 5% of all women can havean amniocentesis and a fetal chromosome analysis. Thenew policy, if adopted generally, would have thepotential to reduce the number of babies born withDown's syndrome in the United Kingdom from about900 a year to about 350.
We thank Professor Eva Alberman and Professor MichaelMarmot for their helpful comments, and Professor Sir AlecTurnbull for his help and support during our work in Oxford,when the antenatal serum bank used in this study wascollected.
Screening for Down's syndrome with assays of unconju-gated oestriol is subject to International Patent ApplicationPCT/GB88/00557.
BMJ VOLUME 297 8 OCTOBER 1988886
on 9 Decem
ber 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.297.6653.883 on 8 O
ctober 1988. Dow
nloaded from

AppendixMethod ofestimating the risk ofa Down's syndrome term
pregnancy- The risk of a Down's syndrome termpregnancy for women of a given age was estimated withthe equation in the footnote to table I in Cuckle et afand the risk expressed as an odds ratio. This odds ratiowas multiplied by the relevant likelihood ratio to yieldthe woman's risk given her age and the results of thebiochemical variables used. The relevant likelihoodratio was derived from the appropriate univariate (ifonly one biochemical variable were used), bivariate(if two were used), or trivariate (if all three wereused) Gaussian frequency distributions of unconju-gated oestriol concentration, log a fetoprotein con-centration, and log human chorionic gonadotrophinconcentration. The likelihood ratio was the height ofthe Gaussian distribution for the Down's syndromepregnancies divided by the height of the Gaussiandistribution for the unaffected pregnancies at theparticular value or values of the variable or variablesconcerned.
Parameters of distributions-Table VI shows thevalues of the parameters of the distributions of theserum screening variables.
TABLE VI -Statistical variables of distributions of unconjugated oestriol concentrations, log humanchorionic gonadotrophin concentrations, and log ct fetoprotein concentrations in Down's syndromepregnancies and unaffected pregnanctes
Down's syndrome UnaffectedVariable Biochemical variable pregnancies pregnancies
Mean Log human chorionic gonadotrophin concentration 0-30% 0-0073Unconjugated oestriol concentration 0.73* 1 00*Log a fetoprotein concentration -0-1427* 0 0000*
Standard deviation Log human chorionic gonadotrophin concentration 0-2588 0-2342Unconjugated oestriol concentration 0.26* 0.27*Log a fetoprotein concentration 0-2052* 0.2024*
Correlation coefficient Log human chorionic gonadotrophin-unconjugated'oestriol concentration -0-25 -0-08
Unconjugated oestriol concentration-log afetoprotein concentration 0 14* 0 13*
Logo fetoprotein concentration-log human chorionicgonadotrophin concentration 0-14 0-05
*Derived from Wald et al. I
Before allowing for long term variance between assays the standard deviations of human chorionic gonadotrophinconcentrations in affected and unaffected pregnancies were 0-2582 and 0-2336, respectively, and the correlationcoefficients between log human chorionic gonadotrophin and unconjugated oestriol in affected and unaffectedpregnancies were -0-29 (p=001) and -0-08 (p=0 10), respectively; for log human chorionic gonadotrophinconcentration and log a fetoprotein concentration they were 0-19 (p=0 10) and 0 07 (p=0 17) respectively, afterexcluding three controls who had outlying a fetoprotein concentrations.
Fit ofdata to Gaussian distributions- Maternal serumlog a fetoprotein concentrations fit a Gaussian distribu-tion well within the range 040-2 50 MoM7; unconju-gated oestriol concentrations fit a Gaussian distribu-tion well within the. range 0-40-1 40 MoM; and loghuman chorionic gonadotrophin concentrations fit aGaussian distribution well over the whole range ofvalues (fig 2). The Shapiro-Wilk W test applied tosquared radii as described by Royston8 was used to testfor any deviations of the observed unconjugatedoestriol concentration, log human chorionic gonado-trophin concentration, and log a fetoprotein concen-tration from each bivariate or trivariate Gaussiandistribution. There was no significant deviation from,firstly, the bivariate Gaussian distributions of un-conjugated oestriol concentration and log humanchorionic gonadotrophin concentration (p=0 55 foraffected and p=0-89 for unaffected pregnancies); loghuman chorionic gonadotrophin concentration and loga fetoprotein concentration (p=0-20 for affected andp=0-88 for unaffected; and unconjugated oestriolconcentration and log a fetoprotein concentration(0-76 for affected and p=0l10 for unaffected); and,secondly, the trivariate Gaussian distributions(p=0 79 for affected and p=0 60 for unaffected) afterexcluding 13 controls who had outlying values, fivewho had extreme a fetoprotein concentrations, andeight who had extreme unconjugated oestriol concen-
trations. These would not affect our estimates of riskbecause they were outside the ranges within which thefitted distributions were used to estimate risk.
Estimating detection rate and false positive rate usingrisk as a screening variable- The distribution of risk inDown's syndrome and unaffected pregnancies wasfound by numerically integrating the distributionof age and the appropriate univariate, bivariate, ortrivariate Gaussian density functions over a grid ofvalues of age and the corresponding biochemicalvariables. The risk associated with a fetoproteinconcentrations outside the range 0 40-2 50 MoM wastaken to be equal to the value at the nearest endpointof the range; similarly for unconjugated oestriolconcentrations outside the range 0-40-1-40 MoM.The distribution of ages in Down's syndrome andunaffected pregnancies was derived by applying theage specific risk of a Down's syndrome term pregnancyto the number of pregnant women of different ages inEngland and Wales in 1981-5.
1 Wald NJ, Cuckle HS. Recent advances in screening for neural tube defects andDown syndrome. In: Rodeck C, ed. Bailliere's clinical obstetrics and gynae-cology. International practice and research. Vol 1. Fetal diagnosis of geneticdefects. London: Bailliere Tindall, 1987:649-76.
2 Wald NJ, Cuckle HS, Densem JW, et al. Maternal serum unconjugated oestriolas an antenatal screening test for Down's syndrome. Br J Obstet Gynaecol1988;95:334-4 1.
3 Bogart MH, Pandian MR, Jones OW. Abnormal maternal serum chorionicgonadotrophin levels in pregnancies with fetal chromosome abnormalities.Prenat Diagn 1987;7:623-30.
4 Canick JA, Knight GJ, Palomaki GE, Haddow JE, Cuckle HS, Wald NJ. Lowsecond trimester maternal serum unconjugated oestriol in pregnancies withDown's syndrome. BrJ Obstet Gynaecol 1988;95:330-3.
5 Benacerraf BR, Gelman R, Frigoletto FD. Sonographic identification ofsecond-trimester fetuses with Down's syndrome. N Engl J Med 1987;317:1371-6.
6 Lockwood C, Benacerraf BR, Krinsky A, et al. A sonographic screening methodfor Down syndrome. AmJ Obstet Gynecol 1987;157:803-8.
7 Cuckle HS, Wald NJ, Thompson SG. Estimating a woman's risk of having apregnancy associated with Down's syndrome using her age and serum alpha-fetoprotein level. BrJ Obstet Gynaecol 1987;94:387-402.
8 Royston JP. Some techniques for assessing multivariate normality based on theShapiro-Wilk W. Applied Statistics 1983;32:121-33.
(Accepted 22 June 1988)
ONE HUNDRED YEARS AGO
The Paris correspondent of the Daily Telegraph narratesa case illustrating the well-known fact that in a semi-unconscious condition illusions are easily producedwhich may have disastrous results. A man, and a womanwith her young infant, were the sole occupants of acompartment in the train running from Lille to Paris. Itwas evening, and the man fell sound asleep; when hepartially awoke, the woman was feeding her infant froma bottle of milk. The half-awakened traveller appearedgreatly frightened and shrank into the corner; soon hescreamed and cried for assistance, and finally pulledthe alarm-bell, and, opening the door, he fled toa neighbouring carriage, to which he clung. He subse-quently stated that he had gone to sleep, when he wassuddenly awakened by a lady who, with menacinggestures, pointed a revolver at his head. He called outfor help, and effected his escape from his would-bemurderess. When seen he was "all of a tremble," and hebelieved fully that, but for his promptitude, he wouldhave been assassinated. It appears that he mistook thebaby's bottle for a revolver. The case was investigated bythe police, and there appears no doubt of its authenticity.Such cases of mental terror and illusions on suddenlyawaking from sleep are common among children, but donot often occur in adults; but when they do occur in asevere form important results may follow, as in the casenarrated. In children such conditions often lead topermanent impressions on the brain, producing attacksof recurring mental terror and consequent brainexhaustion. (British Medical3ournal 1888;ii: 135)
BMJ VOLUME 297 8 OCTOBER 1988 887
on 9 Decem
ber 2020 by guest. Protected by copyright.
http://ww
w.bm
j.com/
BM
J: first published as 10.1136/bmj.297.6653.883 on 8 O
ctober 1988. Dow
nloaded from