Embed Size (px)
DESCRIPTION
pankreatic chronic
Citation preview

The American Journal of GASTROENTEROLOGY VOLUME 106 | DECEMBER 2011 www.amjgastro.com
ORIGINAL CONTRIBUTIONS nature publishing group2192 P
AN
CR
EA
S A
ND
BIL
IAR
Y T
RA
CT
INTRODUCTION Chronic pancreatitis (CP) is an infl ammatory disorder of the pan-
creas typically associated with heavy alcohol consumption. Clinical
features of CP consist of abdominal pain, recurrent attacks of clinical
acute pancreatitis (AP), and exocrine and / or endocrine insuffi ciency
( 1 ). Recent US estimates of the economic burden from all pancrea-
titis combined in 2004 was $ 3.7 billion ( 2 ). Among all digestive dis-
orders, pancreatitis ranked eighth in terms of the overall costs and
seventh for hospital admissions and charges ( 3 ). Discharges for CP
from US hospitals based on the Nationwide Inpatient Sample were
estimated to be 8.1 / 100,000 population in 2004 ( 4 ).
Most literature on CP epidemiology is based on cross-sectional
and / or longitudinal evaluation at centers with specifi c interest in
pancreatic disorders ( 5 – 14 ). Large epidemiology studies from the
United States are limited to two cross-sectional non-population-
based experiences — one from the Mayo Clinic based on patients
evaluated from 1976 to 1982 ( 11 ), and a recent multicenter experi-
ence from 2000 to 2006 ( 15 ).
Th ere are scarce population-based data on the incidence, preva-
lence, or natural history of CP ( 16 – 21 ). In the United States, this
information is limited to a study from Rochester from 1940 to 1969
( 22 ), and admissions to non-federal acute care hospitals or ambu-
latory visits in nonunique patients ( 3,4 ). Th e use of administrative
data is also limited by a lack of verifi cation of diagnosis. Th erefore,
population-based studies in the United States are warranted to
provide a better understanding of CP epidemiology.
Olmsted County and Mayo Clinic ’ s comprehensive databases
provide an ideal setting for population-based studies in the United
Incidence, Prevalence, and Survival of Chronic Pancreatitis: A Population-Based Study Dhiraj Yadav , MD, MPH 1 , Lawrence Timmons 2 , Joanne T. Benson , BA 2 , Ross A. Dierkhising , MS 2 and Suresh T. Chari , MD 2
OBJECTIVES: Population-based data on chronic pancreatitis (CP) in the United States are scarce. We determined incidence, prevalence, and survival of CP in Olmsted County, MN.
METHODS: Using Mayo Clinic Rochester ’ s Medical Diagnostic Index followed by a detailed chart review, we iden-tifi ed 106 incident CP cases from 1977 to 2006 (89 clinical cases, 17 diagnosed only at autopsy); CP was defi ned by previously published Mayo Clinic criteria. We calculated age- and sex-adjusted incidence (for each decade) and prevalence rate (1 January 2006) per 100,000 population (adjusted to 2000 US White population). We compared the observed survival rate for patients with expected survival for age- and sex-matched Minnesota White population.
RESULTS: Median age at diagnosis of CP was 58 years, 56 % were male, and 51 % had alcoholic CP. The overall (clinical cases or diagnosed only at autopsy) age- and sex-adjusted incidence was 4.05 / 100,000 per-son-years (95 % confi dence interval (CI) 3.27 – 4.83). The incidence rate for clinical cases increased signifi cantly from 2.94 / 100,000 during 1977 – 1986 to 4.35 / 100,000 person-years during 1997 – 2006 ( P < 0.05) because of an increase in the incidence of alcoholic CP. There were 51 prevalent CP cases on 1 January 2006 (57 % male, 53 % alcoholic). The age- and sex-adjusted prevalence rate per 100,000 population was 41.76 (95 % CI 30.21 – 53.32). At last follow-up, 50 patients were alive. Survival among CP patients was signifi cantly lower than age- and sex-specifi c expected survival in Minnesota White population ( P < 0.001).
CONCLUSIONS: Incidence and prevalence of CP are low, and ~ 50 % are alcohol related. The incidence of CP cases diagnosed during life is increasing. Survival of CP patients is lower than in the Minnesota White population.
Am J Gastroenterol 2011; 106:2192–2199; doi: 10.1038/ajg.2011.328; published online 27 September 2011
1 Division of Gastroenterology and Hepatology, University of Pittsburgh Medical Center , Pittsburgh , Pennsylvania , USA ; 2 Mayo Clinic , Rochester , Minnesota , USA . Correspondence: Dhiraj Yadav, MD, MPH , Division of Gastroenterology and Hepatology, University of Pittsburgh Medical Center , 200 Lothrop Street , M2, C-Wing, Pittsburgh , Pennsylvania 15213 , USA . E-mail: [email protected] These data were presented as a Poster at the Digestive Disease Week in New Orleans, LA, in May 2010 and published in abstract form in Gastroenterology 2010;138 (Suppl 1):S-391. Received 29 April 2011; accepted 20 July 2011

© 2011 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
2193
PA
NC
RE
AS
AN
D B
ILIA
RY
TR
AC
T
Chronic Pancreatitis Epidemiology in Olmsted County, MN
States (see Methods). We conducted a population-based study in
Olmsted County, MN, to determine: (i) the incidence of CP from
1977 to 2006, (ii) prevalence of CP as of 1 January 2006, and (iii)
overall mortality in CP patients in comparison with the Minnesota
White population of the same age and sex.
METHODS Th e study was approved by the Institutional Review Boards of the
Mayo Clinic Foundation and University of Pittsburgh.
Study setting: Olmsted County Olmsted County, MN, USA (2000 census population, 124,277),
and its central city Rochester (2000 census population, 85,806)
are located in the southeastern part of the State, ~ 128 km from the
nearest major metropolitan area (the twin cities of Minneapolis
and Saint Paul). Rochester is home to the Mayo Clinic, one of the
world ’ s largest medical centers. Since its inception, over 8 million
diff erent patients have registered at Mayo Clinic Rochester. In the
year 2000, medical care was provided to 311,377 diff erent patients
who made a total of 1.19 million visits to the Clinic that year.
Nearly all of the medical care delivered to Olmsted County resi-
dents is provided by either the Mayo Clinic or the Olmsted Medical
Center and their respective affi liated hospitals. Th e Olmsted Medi-
cal Center does not have a gastroenterologist and all patients with
chronic, severe gastrointestinal diseases (such as CP) are cared for
jointly by a primary care physician in Olmsted Medical center and
a specialist in Mayo Clinic.
Th e presence of a major medical center in relative isolation
makes Olmsted County an ideal setting for population-based epi-
demiologic research ( 23 ). Mayo Clinic is also renowned for main-
taining large longitudinal population-based databases of patient
information. Mayo Clinic has maintained the original records of
every patient seen since 1907, with less than a thousand of the 8
million records being lost. Various interlinked electronic databases
maintain records of patient appointments, clinical and pathologi-
cal diagnoses, laboratory tests, surgical procedures, vital status,
and cause of death ( 23 ).
Case ascertainment We used the Mayo Diagnostic index to identify all Olmsted
County residents who received a diagnosis of CP from 1977 to
2006. Th e diagnostic index is designed to be a sensitive method
for identifi cation of patients with a particular disease condition.
Medical records of all patients identifi ed on the initial search
were manually reviewed by a professional data abstractor (L.T.)
using predefi ned guidelines under the supervision of two physi-
cian investigators (D.Y. and S.T.C.). Each case was reviewed by
the physician investigators and medical records were reviewed as
needed by one of them (S.T.C.) to confi rm the diagnosis of CP.
Only patients who were residents of Olmsted County at the time
of disease diagnosis were included in the incidence results. Resi-
dents who received a previous diagnosis of CP elsewhere but were
living in Olmsted County as of the reference date were included
only in the calculations of prevalence.
Th e diagnosis of CP was considered as defi nite if the patient
fulfi lled the Mayo criteria ( 11 ). Th e Mayo scoring system assigns
a score to individual fi ndings as follows: typical histology for CP,
including histology (4); pancreatic calcifi cations (4); characteris-
tic fi ndings on endoscopic retrograde cholangiopancreatography
(3); pancreatic exocrine insuffi ciency (steatorrhea defi ned by
abnormal qualitative or quantitative fecal fat excretion > 7 g / day,
or abnormal cholecystokinin test result (normal range trypsin
output (25.3 – 54.2 × 10 3 U / h), lipase output (77.2 – 322 × 10 3 U / h))
(2); attacks of pancreatitis or chronic upper abdominal pain (2);
and diabetes mellitus (disturbed glucose tolerance requiring
continuous control by diet alone or with addition of oral agents
or insulin) (1). A defi nite diagnosis of CP is established if the
Mayo score is ≥ 4.
During 1977 – 2006, 331 Olmsted County residents received a
diagnosis of CP (329 while Olmsted residents and 2 while previ-
ously living in another location). Among these patients, 100 cases
of defi nite CP were identifi ed aft er a detailed chart review. Th e
remaining 231 cases were excluded because of the following rea-
sons: diagnosis made while previously living in another location
( n = 2); AP ( n = 46) or recurrent AP ( n = 45), failed to meet CP
diagnostic criteria; no AP or recurrent AP, failed to meet CP diag-
nostic criteria ( n = 35); pancreatic enzyme elevation on multiple
occasions ( n = 14); chronic indeterminate abdominal pain ( n = 11);
alcoholism with or without elevated pancreatic enzymes ( n = 10);
CP changes on histology (changes seen because of obstruction,
no evidence of pre-existing CP) in patients with pancreaticobil-
iary malignancy ( n = 17); proven ( n = 6) or suspected ( n = 2) cystic
tumor; pancreas cyst but no features of CP ( n = 3); CP mentioned
in records but no workup done or available for review ( n = 3);
diagnosis other than CP ( n = 4); cystic fi brosis ( n = 2); diagnosis
fell outside study period ( n = 18); Federal Medical Center patient
( n = 12); and chart not available for review ( n = 1).
It is unclear if selecting patients based on the assigned diagnosis
of CP will capture all true cases. To better understand this and to
minimize underestimation of true cases of CP who may not have
received a correct coding, we also reviewed medical records of a sub-
set of patients who received a diagnosis of “ AP ” without mention of
CP (171 / 471, 36 % ), and a subset of patients who received a diagnosis
of “ pancreatitis – not otherwise specifi ed ” without a mention of CP
(210 / 700, 30 % ) during the study period. Among these patients, we
identifi ed 6 additional cases of defi nite CP (4 in the “ AP ” and 2 in the
“ pancreatitis – not otherwise specifi ed ” diagnosis group).
For all 106 patients who met criteria for defi nite diagnosis of CP,
we noted the date when the patients fi rst met diagnostic criteria,
age when diagnosis was established, gender, residency status at the
time of diagnosis and on 1 January 2006, and date and vital status
at the time of last follow-up. We defi ned etiology (alcohol related
vs. nonalcohol related) based on the treating physician ’ s diagno-
sis. For patients who had died, the cause of death was obtained by
review of the death certifi cates.
Statistics Incidence and prevalence rates . For calculation of incidence rates,
the entire population of Olmsted County from 1977 to 2006 was

The American Journal of GASTROENTEROLOGY VOLUME 106 | DECEMBER 2011 www.amjgastro.com
2194 P
AN
CR
EA
S A
ND
BIL
IAR
Y T
RA
CT
Yadav et al.
considered to be at risk for CP. Th e study period was divided into
three 10-year intervals and incidence rates were calculated per
100,000 person-years for the entire study period as well as each
10-year interval. Th e denominator for age- and gender-specifi c
person-years was derived from decennial US Census fi gures. Th e
rates were age and gender adjusted to the 2000 US White popula-
tion, and 95 % confi dence intervals (CIs) of incidence rates were
calculated usin g the Poisson distribution. Th e incidence rates
(overall, by gender) were calculated for all cases (i.e., cases diag-
nosed during life or only at autopsy) and for cases diagnosed dur-
ing life (clinical cases). Among the cases diagnosed during life,
etiology-specifi c incidence rates (alcohol and nonalcohol related)
were also calculated. Trends in the incidence rates (all cases, all
clinical cases, and etiology-specifi c clinical cases) by age of di-
agnosis (0 – 34, 35 – 44, 45 – 54, 55 – 64, 65 – 74, and 75 + ), gender,
and calendar period of diagnosis (1977 – 1986, 1987 – 1996, and
1997 – 2006) were evaluated using multivariable Poisson regres-
sion models with all three terms included. Interactions between
gender and calendar period were assessed. None were signifi cant,
and hence only models with main eff ects for gender and calendar
period were used for inferences.
Prevalence rates were calculated based on the number of CP cases
who were alive on 1 January 2006 and were residents of Olmsted
County. Th e denominator for calculation of age- and gender-spe-
cifi c prevalence was the 2006 mid-year Olmsted County population
derived from decennial US Census fi gures. Th e rates were age and
gender adjusted to the 2000 US White population, and 95 % CIs of
prevalence rates were calculated using the Poisson distribution. Th e
prevalence rates were calculated for all cases, by gender and etiol-
ogy (alcohol and nonalcohol related). Th e overall and etiology-spe-
cifi c prevalence rates were compared between genders, age groups
(0 – 34, 35 – 44, 45 – 54, 55 – 64, 65 – 74, and ≥ 75), and calendar periods
(1977 – 1986, 1987 – 1996, and 1997 – 2006) using multivariable Pois-
son regression models with all three terms included.
Survival rate . Th e overall survival for CP cases diagnosed
during life (overall, by gender, by etiology) was estimated using
Kaplan – Meier methodology. Th e observed survival was com-
pared with the expected survival using the age- and gender-
specifi c expected death rates for Minnesota Whites in 2000 using
the log-rank test. Standardized mortality ratios (overall, by gen-
der, by etiology) were computed as the observed number of deaths
divided by the expected number of deaths in the 2000 Minnesota
White population. Th e 95 % CIs were calculated using the Poisson
distribution. For all comparisons, a P value of < 0.05 was consid-
ered signifi cant. Data analysis was performed with SAS system
version 9.2 (SAS Soft ware Institute, Cary, NC).
RESULTS Incidence Th e total number of incident cases of CP in Olmsted County
from 1977 to 2006 was 106, of whom 89 were clinical cases and
17 were diagnosed only at autopsy. Th e median age at diagnosis
was 58 years (interquartile range 50 – 70; range 7 – 91) and 60 / 106
(57 % ) were male. Th e overall age- and sex-adjusted incidence rate
(i.e., clinical cases or diagnosed at autopsy) for the entire study
period was 4.05 / 100,000 person-years (95 % CI 3.27 – 4.83; Table 1 ).
Th ere was no signifi cant increase in the overall incidence rates
during the three decades of study ( P = 0.27). Th e incidence was
higher for males compared with females (male / female Poisson
rate ratio 1.56, P = 0.025). Th e age groups were signifi cantly
diff erent overall ( P < 0.001), with the 0 – 34 and 35 – 44 age groups
signifi cantly lower than those ≥ 75 (Poisson rate ratios 0.05 and
0.19, P < 0.001 and P < 0.001, respectively). Th e other age groups
were not signifi cantly diff erent from those ≥ 75 (all P values > 0.26).
Th e number of cases diagnosed only at autopsy decreased during
the study period from 10 cases during 1977 – 1986 to 6 cases
during 1987 – 1996 to only 1 case during 1997 – 2006.
For the 89 clinical cases, the median age at diagnosis was 58
years (interquartile range 48 – 67; range 7 – 87) and 50 / 89 (56.2 % )
were male. Th ere was no signifi cant association between gen-
der and age at diagnosis ( P = 0.19, rank-sum test). Th e number
of cases diagnosed with an alcohol etiology were 46 / 89 (51.7 % ),
whereas the remaining 43 / 89 cases (48.6 % ) were nonalcohol
related. Patients diagnosed with alcohol etiology were somewhat
more likely to be male (28 / 46, 60.9 % ), whereas patients with non-
alcohol etio logy were equally distributed between sexes (males
22 / 43, 51.1 % ). Th e age at diagnosis in patients with alcohol etiol-
ogy was signifi cantly lower compared with nonalcohol etiology
(median 51.5 vs. 64 years; P < 0.001, rank-sum test). Th e preva-
lence of ever, current (at the time of diagnosis), and heavy ( ≥ 1
packs per day) smoking among clinical cases was 76 % , 52 % , and
60 % respectively. Compared with patients with nonalcohol etiol-
ogy, those with alcohol etiology were more likely to be ever (67 vs.
85, P = 0.054), current (27 vs. 72 % , P < 0.001), and heavy smokers
(40 vs. 74 % , P < 0.001).
Th e age- and sex-adjusted incidence rate for clinical cases for the
entire study period was 3.34 / 100,000 person-years (95 % CI 2.64 –
4.05; Table 1 ). Males had a somewhat higher clinical incidence rate
than females (Poisson rate ratio 1.48, P = 0.069). Th e age groups
were signifi cantly diff erent overall in their clinical incidence rates
( P < 0.001), with the 0 – 34 and 35 – 44 age groups signifi cantly lower
than the ≥ 75 group (Poisson rate ratios: 0.09 and 0.29, P < 0.001
and P = 0.009, respectively). Th e other age groups were not dif-
ferent than the ≥ 75 group (all P values > 0.15). Th e three decades
were diff erent for the clinical rates overall ( P = 0.033). Th e Poisson
rate ratios for the two earlier periods were 0.62 and 0.55 ( P = 0.074
and P = 0.020) when compared with the latest period, respectively.
Th e observed incidence rate for clinical cases increased from
2.94 / 100,000 person-years (95 % CI 1.61 – 4.27) during 1977 – 1986 to
4.35 / 100,000 person-years (95 % CI 3.12 – 5.58) during 1997 – 2006.
Th is increase at least partially resulted from a signifi cant increase
in the incidence of CP from alcohol etiology from 1.05 / 100,000
in 1976 – 1987 to 2.48 / 100,000 person-years in 1997 – 2006. Th e
alcohol etiology incidence was signifi cantly diff erent between the
decades overall ( P = 0.016), with the Poisson rate ratios between
the earliest two decades and the latest decade being 0.40 and 0.44
( P = 0.028 and 0.027). Th e proportion of cases attributed to alcohol
etiology increased from 36.8 % during 1977 – 1986 to 47.6 % during

© 2011 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
2195
PA
NC
RE
AS
AN
D B
ILIA
RY
TR
AC
T
Chronic Pancreatitis Epidemiology in Olmsted County, MN
1986 – 1997 to 59.2 % during 1997 – 2006. Th e incidence rate for CP
because of nonalcohol etiology remained relatively stable across
the three decades ( P = 0.60).
Th e incidence rate for alcohol-related CP was somewhat
higher in males compared with females (Poisson rate ratio 1.69,
P = 0.082), but was similar for both genders for nonalcohol etiol-
ogy ( P = 0.41).
Th e distribution of age at the time of diagnosis remained similar
across the fi rst two decade periods, but was somewhat lower in the
last decade (medians 59, 64, and 52.5; P = 0.013, Kruskal – Wallis
test). Th e peak age group for diagnosis of clinical CP diff ered based
on the etiology. Th e peak age for diagnosis of alcohol-related clini-
cal CP was the 45 – 54 age group, but was not signifi cantly diff er-
ent than those ≥ 75 (Poisson rate ratio 3.32, P = 0.11). Th e only age
group that at least suggested a diff erence was the 0 – 34 group (rate
ratio vs. ≥ 75: 0.22, P = 0.070). Th e nonalcoholic clinical CP was
most common in the 65 – 74 age group, but was not signifi cantly
diff erent than the ≥ 75 group (rate ratio 1.67, P = 0.27). Th e only age
groups that at least suggested a diff erence relative to the ≥ 75 group
were the 0 – 44 (age groups were combined because of no incidence
cases in the 35 – 44 group) and 45 – 54 age groups (rate ratios 0.04
and 0.41, P < 0.001 and P = 0.099; Figure 1 ).
Prevalence Th e number of Olmsted County residents who were alive with
a defi nite diagnosis of CP on 1 January 2006 was 51 (56.8 %
male), of whom 50 were from the incidence cohort. Th e other
patient diagnosed with CP elsewhere was no longer an Olmsted
County resident on the date for prevalence estimation. Th e
number of prevalent cases diagnosed with alcohol etiology was
27 / 51 (52.9 % ). Th e age- and sex- adjusted prevalence rate of CP
on this date was 41.76 / 100,000 population (95 % CI 30.21 – 53.32;
Table 2 ). Th e age-adjusted prevalence rate for all cases was
higher in males than females (51.45 vs. 33.88 / 100,000). How-
ever, there was not a statistically signifi cant diff erence in prev-
alence of any etiology between genders (Poisson rate ratio:
males vs. females 1.44, P = 0.20). Th e genders were also not
statistically diff erent for prevalence of alcohol- and nonalco-
hol-related CP (rate ratios: males vs. females 1.57 and 1.32,
P = 0.25 and P = 0.50). Th e age and sex-adjusted prevalence of
Table 1 . Incidence of chronic pancreatitis in Olmsted County, Minnesota, by age and time period from 1977 to 2006
Age (years) 1977 – 1986 1987 – 1996 1997 – 2006 Total
N Rate N Rate N Rate N Rate
All cases (diagnosed during life or at autopsy)
0 – 34 0 0.00 0 0.00 9 1.41 9 0.50
35 – 44 3 2.43 2 1.18 5 2.26 10 1.94
45 – 54 7 7.96 5 4.16 14 8.46 26 6.96
55 – 64 7 10.31 7 8.71 8 7.67 22 8.71
65 – 74 6 12.42 9 15.64 9 13.14 24 13.77
≥ 75 6 14.85 4 7.57 5 7.36 15 9.31
Total 29 3.12 27 2.51 50 3.95 106 3.24
Age adjusted (95 % confi dence interval (CI)), men *
— 5.80 (2.86 – 8.75) — 4.51 (2.05 – 4.54) — 5.37 (3.29 – 7.44) — 5.21 (3.25 – 4.80)
Age adjusted (95 % CI), women * — 3.67 (1.66 – 5.68) — 2.16 (0.82 – 3.51) — 3.75 (2.21 – 5.29) — 3.11 (2.20 – 4.02)
Age and sex adjusted (95 % CI) * — 4.56 (2.88 – 6.23) — 3.30 (2.04 – 4.55) — 4.44 (3.20 – 5.68) — 4.05 (3.27 – 4.83)
Cases diagnosed during life (clinical cases)
0 – 34 0 0.00 0 0.00 9 1.14 9 0.50
35 – 44 2 1.62 2 1.18 5 2.26 9 1.75
45 – 54 7 7.96 4 3.33 13 7.85 24 6.42
55 – 64 6 8.84 6 7.46 8 7.67 20 7.92
65 – 74 2 4.14 7 12.16 9 13.14 18 10.32
≥ 75 2 4.95 2 3.79 5 7.36 9 5.86
Total 19 2.04 21 1.95 49 3.87 89 2.72
Age adjusted (95 % CI), men* — 3.96 (1.66 – 6.25) — 3.04 (1.31 – 4.77) — 5.19 (3.15 – 7.23) — 4.20 (3.01 – 5.39)
Age adjusted (95 % CI), women* — 2.12 (0.54 – 3.70) — 1.97 (0.68 – 3.26) — 3.75 (2.21 – 5.29) — 2.63 (1.80 – 3.46)
Age and sex adjusted (95 % CI)* — 2.94 (1.61 – 4.27) — 2.52 (1.44 – 3.61) — 4.35 (3.12 – 5.58) — 3.34 (2.64 – 4.05)
* Denotes per 100,000 person years.

The American Journal of GASTROENTEROLOGY VOLUME 106 | DECEMBER 2011 www.amjgastro.com
2196 P
AN
CR
EA
S A
ND
BIL
IAR
Y T
RA
CT
Yadav et al.
Survival During a median follow-up period of 9.68 years (range 0.01 – 29.42
years), 39 of the 89 incident cases died. Th e median age at the time
of death was 75 years (interquartile range 59, 82). Th e median sur-
vival in the cohort was 12.44 years. Th e causes of death are listed
in Table 3 . Th e most common causes of death included malig-
nancies (23 % ) and cardiovascular causes (21 % ). CP was indicated
as the primary or contributing cause for 5 % and 18 % of deaths,
respectively.
Log-rank tests showed a signifi cantly lower survival in CP
patients (overall, both genders, alcohol, and nonalcohol etiology)
when compared with age- and gender-matched Minnesota White
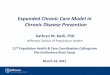
population ( Figure 3 ). Th e overall standardized mortality ratio
(SMR) for CP patients was almost twice that of the Minnesota
alcohol-related CP was similar to nonalcohol-related CP (21.57
vs. 20.20 / 100,000). Most prevalent cases of any etiology were
middle-aged and older individuals (ages 45 – 74). However,
these ages were not statistically diff erent from the ≥ 75 group
( P values ≥ 0.15). Th e prevalence rates of any etiology were lower
in the 0 – 34 age group (rate ratio vs. ≥ 75: 0.24, P = 0.038; Figure
2 ). Th e peak ages for prevalent cases due to alcohol etiology was
between 45 and 64 years. However, no age group was statisti-
cally diff erent from the ≥ 75 group ( P values ≥ 0.14). Th e peak
age for cases of nonalcohol-related etiology was between 45 and
74 years. However, the only age group that was statistically dif-
ferent from the ≥ 75 group was the 0 – 44 group (age groups were
combined because of no prevalence cases in the 35 – 44 group;
rate ratio 0.15, P = 0.031).
12
10
8
6
4
2
0
Inci
denc
e pe
r 10
0,00
0 pe
rson
-yea
rs
0–34 45–54
Age groups (years)
55–64 65–74 ≥7535–44
Males, alcohol etiologyFemales, alcohol etiology
Males, nonalcohol etiologyFemales, nonalcohol etiology
Figure 1 . Age-specifi c incidence rates for clinical cases of chronic pancreatitis in Olmsted County from 1977 to 2006 by gender and etiology.
120
100
80
60
40
20
0
Pre
vale
nce
per
100,
000
popu
latio
n
0–34 45–54
Age groups (years)
55–64 65–74 ≥7535–44
Males, alcohol etiologyFemales, alcohol etiology
Males, nonalcohol etiologyFemales, nonalcohol etiology
Figure 2 . Age-specifi c prevalence rates for chronic pancreatitis as of 1 January 2006 in Olmsted County by gender and etiology.
Table 2 . Prevalence of chronic pancreatitis in Olmsted County, Minnesota, on 1 January 2006 by age and etiology
Age (years) All etiologies Alcohol etiology Nonalcohol etiology
N Rate N Rate N Rate
0 – 34 7 10.33 3 4.43 4 5.90
35 – 44 4 16.75 4 16.75 0 0.00
45 – 54 19 106.12 12 67.02 7 39.10
55 – 64 11 97.83 5 44.47 6 53.36
65 – 74 7 95.35 2 27.24 5 68.11
≥ 75 3 41.01 1 13.67 2 27.34
Total 51 37.65 27 19.93 24 17.72
Age adjusted (95 % confi dence interval (CI)), men * — 51.45 (32.37 – 70.55) — 26.86 (13.45 – 40.27) — 24.59 (11.00 – 38.19)
Age adjusted (95 % CI), women * — 33.88 (19.65 – 48.10) — 16.99 (6.90 – 27.09) — 16.88 (6.86 – 26.91)
Age and sex adjusted (95 % CI) * — 41.76 (30.21 – 53.32) — 21.57 (13.37 – 29.76) — 20.20 (12.05 – 28.35)
*Denotes per 100,000 person years.

© 2011 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
2197
PA
NC
RE
AS
AN
D B
ILIA
RY
TR
AC
T
Chronic Pancreatitis Epidemiology in Olmsted County, MN
White population. Th e SMR was specifi cally high ( ~ 3.5-fold) in
patients with alcoholic CP and in females ( Table 4 ).
DISCUSSION In this population-based study, we report the incidence and
survival of CP in Olmsted County, MN, over a 30-year period,
and prevalence as of 1 January 2006. We observed a signifi cant
increase in the number of incident cases of clinical CP. Alcohol
was the predominant etiology and accounted for at least 50 % of
all incident and prevalent CP cases. Survival in CP patients was
signifi cantly lower, and mortality in females and alcohol-related
CP was ~ 3.5 times higher when compared with an age- and
gender-matched Minnesota White population.
Th e incidence rates in our study are not directly comparable to
the previous report from Rochester ( 22 ) because of diff erences
in case defi nition (more stringent in our study) and the choice of
population (Olmsted County rather than the city of Rochester).
However, in combination, results from these two studies provide
an insight into CP epidemiology in a defi ned US White popula-
tion over the past 6 to 7 decades and how it relates to data from
other populations. Th e incidence rates of CP and the propor-
tion of cases attributed directly to alcohol etiology (50 – 55 % ) in
Olmsted County are lower than in other population ( 16,17,24 )
and cross-sectional ( 5,8,13 ) studies in Europe and other centers
(67 – 89 % ) ( 6,9,10 ), but similar to those from Japan (56 % ) ( 18 ).
Interestingly, the proportion of subjects attributed to alcohol
etio logy has been in the range of 45 – 55 % in recent studies from
the United States ( 25 ) and Europe ( 19,26 ). Th e gender and age
distribution for alcohol- and nonalcohol-related CP observed in
our study is similar to previous reports indicating that the etiol-
ogy-specifi c groups are comparable across studies ( 5,8,11 – 13 ).
Th e prevalence rates for CP observed in Olmsted County in the
year 2006 are higher than the only available estimates from Japan
for the year 1994 ( 18 ).
Our defi nition for alcohol etiology also diff ered from a previous
epidemiological study from the Mayo Clinic ( 11,27 ). In this study
of all CP patients ( n = 429) evaluated at the Mayo Clinic from 1976
Table 4 . SMRs in incident chronic pancreatitis cases in Olmsted County, MN, from 1977 to 2006 compared with age- and sex-matched Minnesota White population
Group Observed deaths Expected deaths SMR 95 % CI of SMR Log-rank P value
All patients 39 20.12 1.94 1.38 – 2.65 < 0.001
Alcohol etiology 15 4.21 3.56 1.99 – 5.88 < 0.001
Nonalcohol etiology 24 15.91 1.51 0.97 – 2.24 0.043 a
Males 23 15.46 1.49 0.94 – 2.23 0.055
Females 16 4.66 3.43 1.96 – 5.57 < 0.001
CI, confi dence interval; SMR, standardized mortality ratio. a Seemingly incongruent results for 95 % CI (crossing 1) and P value ( < 0.05) due to different underlying theories for computation. Whereas the log-rank χ 2 test does not assume a statistical model for the mortality rates, the CI for the SMR is based on the Poisson distribution, a specifi c statistical model for the event rates. Regardless, the P value is very close to 0.05 and one side of the interval is close to 1, and hence the conclusions are not affected.
Table 3 . Causes of death in incident cases of chronic pancreatitis from 1977 to 2006 in Olmsted County, Minnesota
Organ / system Cause of death ( n =39)
Cancer (9) Pancreas (2), colon (2), breast (2), ovarian (1), hepatocellular (1), unknown primary (1)
Cardiovascular (8) Coronary artery disease / myocardial infarction (5), congestive heart failure (1), arrhythmia (1), intra-cerebral hemorrhage (1)
Gastrointestinal (6) Chronic pancreatitis (2), liver failure (1), perforated bowel (1), gastrointestinal bleeding (1), acute mesenteric ischemia (1)
Pulmonary (5) Chronic obstructive pulmonary disease or its complications (4), aspiration (1)
Other (11) Infectious causes (sepsis, pneumonia, or urinary tract infection, etc.) (5), renal failure (2), seizure disorder (1), gunshot (1), opoid overdose (1), unknown cause (1)
Chronic pancreatitis in seven patients and recurrent acute pancreatitis in one patient were listed as a contributing cause of death.
100
60
40
20
0
0 5 10 15
ObservedExpected
Sur
viva
l
80
Years
Figure 3 . Mortality in patients with chronic pancreatitis in Olmsted County, MN, compared with age- and gender-matched Minnesota White population.

The American Journal of GASTROENTEROLOGY VOLUME 106 | DECEMBER 2011 www.amjgastro.com
2198 P
AN
CR
EA
S A
ND
BIL
IAR
Y T
RA
CT
Yadav et al.
SMR for females appears to be higher compared with males, their
overlapping CI suggests that the true SMRs may be the same.
One limitation of our study is underestimation of incident cases.
To minimize this, we reviewed medical records of approximately
one-third of patients who only received a diagnosis of AP or non-
specifi c pancreatitis without a specifi c mention of CP and identifi ed
six cases. Although the records from these additional patients were
not reviewed in a random order, as the total additional cases found
were small relative to the initial cohort, we believe that the estimates
between patient categories (e.g., age and gender) were not aff ected.
Extrapolating these numbers to the remaining cases that were
not reviewed would have yielded an additional 12 cases, thereby
increasing the overall incidence rates by 10 – 15 % . Assuming that
the proportion of cases diagnosed only at autopsy was similar dur-
ing the study period, an additional 20 cases would have been identi-
fi ed. Our study would also not have detected subclinical cases, cases
with one or more attack of AP, or patients with chronic abdominal
pain who did not develop morphological or functional changes to
fulfi ll the Mayo criteria. Th erefore, it is likely that the true incidence
of CP is ~ 30 – 35 % higher than the estimates in our study.
Another limitation of our study is the generalizability of results.
Although the Olmsted County population is predominantly white
of Northern European decent, it is considered to be fairly repre-
sentative of the US White population ( 23 ), to whom our results
may be applicable. Our results, however, will not be generalizable
to other ethnic groups, the rates of pancreatitis in whom, specifi -
cally Blacks, have been reported to be higher than Whites ( 4,30 ).
Finally, although the sample size of our study is small, these are the
only population-based estimates of defi nite CP in the United States
in the past few decades.
In conclusion, the incidence and prevalence rates of CP are low,
and at least 50 % are alcohol related. Th e incidence rate over time
for clinical CP cases is increasing, mainly because of an increase
in the diagnosis of alcohol-related CP. Th e epidemiology of CP in
the United States is diff erent from European centers with regard
to incidence rates and the proportion of cases directly attributed
to alcohol use. Survival in CP patients is signifi cantly lower when
compared with an age- and sex-matched population. Most deaths
in CP cases are because of nonpancreatic causes.
CONFLICT OF INTEREST Guarantor of the article: Dhiraj Yadav, MD, MPH.
Specifi c author contributions: Dhiraj Yadav: study design, obtain-
ing funding, study supervision, data interpretation, draft ing and
revising the article, and fi nal approval of the version to be published;
Lawrence Timmons: data acquisition and fi nal approval of the ver-
sion to be published; Joanne T. Benson and Ross A. Dierkhising: sta-
tistical analysis and interpretation, revising the article critically for
important intellectual content, and fi nal approval of the version to
be published; Suresh T. Chari: study design, study supervision, data
interpretation, draft ing and revising the article, and fi nal approval of
the version to be published.
Financial support : Th is work was supported by the Department of
Medicine, University of Pittsburgh (to D.Y.).
Potential competing interests: None.
to 1982 ( 11,27 ), patients with alcohol consumption of > 50 g / day
were defi ned as alcoholic CP (58 % ). Alcohol consumption in
the remaining patients was < 50 g / day (13 % ), unknown (13 % ),
or they were lifetime abstainers (16 % ). Alcohol consumption at
lower levels ( < 50 g / day) was suggested to play a modifying role
in disease development and these patients were believed to repre-
sent a subset of late-onset idiopathic CP ( 27 ). We defi ned etiology
based on the treating physician ’ s diagnosis. Of the 89 clinical cases,
physicians considered alcohol as an etiology in 46 (52 % ). Among
the remaining 43 (48 % ) patients, the diagnosis was idiopathic in
34, hereditary pancreatitis in 1, other autoimmune diseases in 2
(Crohn ’ s disease, polyarteritis nodosa in 1 each), pancreas divisum
in 1, hypertriglyceridemia in 3, and unknown in 2. Although 32 / 41
patients in the nonalcohol etiology group reported ever drinking
(19 light ( ≤ 3 drinks / week), “ rare or social ” ; 4 moderate ( < 2 drinks /
day); 1 heavy (2 – 5 drinks / day); 8 details not available), it was not
considered suffi cient by physicians to assign an alcohol etiology.
No patient in this group was diagnosed with alcoholic liver dis-
ease or cirrhosis, and none self-reported a “ yes ” on the alcoholism
screening questions routinely asked on intake forms during Mayo
Clinic visits. Th e role of alcohol at lower levels of consumption in
these patients needs further study. Interestingly, the distribution of
alcohol consumption in our study was mostly similar to the earlier
report ( 11,27 ).
We found a signifi cant increase over time in the incidence for
clinical cases of CP in Olmsted County but not for the overall inci-
dence. Th is observation was because of a progressive decline in the
number of cases diagnosed by autopsy during the study period
(from 34 % during 1977 – 1986 to only 2 % during 1997 – 2006). Th ese
numbers are consistent with the overall decline in the autopsy rates
in the United States over the past few decades ( 28 ). Th e increased
number of cases diagnosed during life was mainly because of an
increase in the diagnosis of alcohol-related CP. Patients with early-
onset idiopathic and alcoholic CP are more likely to have clinical
symptoms when compared with subjects with late-onset idiopathic
CP ( 11 ). It is likely that an increase in the incidence of clinical CP
may be related to increasing use of highly sensitive cross-sectional
imaging studies (computed tomography and magnetic resonance
imaging) for evaluation of abdominal symptoms, thereby leading to
detection of early changes or milder abnormalities of CP. Evaluation
of the distribution of age does in fact reveal that the cases diagnosed
during 1997 – 2006 were younger than the two earlier decades.
Our results of signifi cantly lower survival rates compared with
expected rates and causes of death in CP patients are similar to
previous reports ( 8,11,13,19,29 ). Importantly, almost three-quar-
ters of deaths were unrelated to pancreatitis. Additionally, we
evaluated the SMR in CP patients aft er stratifi cation by gender as
well as etiology. Although the SMR of 3.6 in patients with alco-
hol-related CP was similar to a recent Danish study ( 19 ), those
for nonalcoholic CP was only 1.5 times larger than an age- and
sex-matched population (and it was only marginally signifi cant,
P = 0.043). A lower SMR for nonalcohol-related CP is likely
because of older age at diagnosis in this group, thereby having a
lower life expectancy. Th e SMR for both sexes were signifi cantly
higher than age- and sex-matched population. Although the

© 2011 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
2199
PA
NC
RE
AS
AN
D B
ILIA
RY
TR
AC
T
Chronic Pancreatitis Epidemiology in Olmsted County, MN
Study Highlights
WHAT IS CURRENT KNOWLEDGE 3 Population-based data are critical to understand disease
burden, formulate health policy, and for resource allocation.
3 Population-based estimates of chronic pancreatitis (CP) are scarce. Available data on incidence originate mainly from Europe, while prevalence has been reported only from Japan. US data in the past 4 decades are limited to hospital admissions in nonunique patients.
3 Olmsted County, MN, provides an ideal setting to conduct population-based studies in the United States.
WHAT IS NEW HERE 3 Incidence of clinical CP in Olmsted County, MN, increased
signifi cantly over three decades (1977 – 2006), mainly from an increase in the diagnosis of alcoholic CP.
3 Proportion of patients attributed to alcohol etiology in this study is somewhat lower than European estimates but similar to those from Japan.
3 Survival in CP patients was signifi cantly lower when com-pared with age- and sex-matched Minnesota population, and most deaths were unrelated to pancreatitis.
REFERENCES 1 . Etemad B , Whitcomb DC . Chronic pancreatitis: diagnosis, classifi cation,
and new genetic developments . Gastroenterology 2001 ; 120 : 682 – 707 . 2 . Everhart JE , Ruhl CE . Burden of digestive diseases in the United States
part I: overall and upper gastrointestinal diseases . Gastroenterology 2009 ; 136 : 376 – 86 .
3 . Everhart JE , Ruhl CE . Burden of digestive diseases in the United States Part III: liver, biliary tract, and pancreas . Gastroenterology 2009 ; 136 : 1134 – 44 .
4 . Yang AL , Vadhavkar S , Singh G et al. Epidemiology of alcohol-related liver and pancreatic disease in the United States . Arch Intern Med 2008 ; 168 : 649 – 56 .
5 . Gastard J , Joubaud F , Farbos T et al. Etiology and course of primary chronic pancreatitis in Western France . Digestion 1973 ; 9 : 416 – 28 .
6 . Marks IN , Bank S , Louw JH . Chronic pancreatitis in the Western Cape . Digestion 1973 ; 9 : 447 – 53 .
7 . Durbec JP , Sarles H . Multicenter survey of the etiology of pancreatic diseas-es. Relationship between the relative risk of developing chronic pancreatitis and alcohol, protein and lipid consumption . Digestion 1978 ; 18 : 337 – 50 .
8 . Ammann RW , Akovbiantz A , Largiader F et al. Course and outcome of chronic pancreatitis. Longitudinal study of a mixed medical-surgical series of 245 patients . Gastroenterology 1984 ; 86 : 820 – 8 .
9 . Dani R , Mott CB , Guarita DR et al. Epidemiology and etiology of chronic pancreatitis in Brazil: a tale of two cities . Pancreas 1990 ; 5 : 474 – 8 .
10 . Robles-Diaz G , Vargas F , Uscanga L et al. Chronic pancreatitis in Mexico City . Pancreas 1990 ; 5 : 479 – 83 .
11 . Layer P , Yamamoto H , Kalthoff L et al. Th e diff erent courses of early- and late-onset idiopathic and alcoholic chronic pancreatitis . Gastroenterology 1994 ; 107 : 1481 – 7 .
12 . Lankisch PG , Seidensticker F , Lohr-Happe A et al. Th e course of pain is the same in alcohol- and nonalcohol-induced chronic pancreatitis . Pancreas 1995 ; 10 : 338 – 41 .
13 . Cavallini G , Frulloni L , Pederzoli P et al. Long-term follow-up of patients with chronic pancreatitis in Italy . Scand J Gastroenterol 1998 ; 33 : 880 – 9 .
14 . Ammann RW , Muellhaupt B . Th e natural history of pain in alcoholic chronic pancreatitis . Gastroenterology 1999 ; 116 : 1132 – 40 .
15 . Yadav D , Hawes RH , Brand RE et al. Alcohol consumption, cigarette smok-ing, and the risk of recurrent acute and chronic pancreatitis . Arch Intern Med 2009 ; 169 : 1035 – 45 .
16 . Dite P , Stary K , Novotny I et al. Incidence of chronic pancreatitis in the Czech Republic . Eur J Gastroenterol Hepatol 2001 ; 13 : 749 – 50 .
17 . Lankisch PG , Assmus C , Maisonneuve P et al. Epidemiology of pancreatic diseases in Luneburg County. A study in a defi ned German population . Pancreatology 2002 ; 2 : 469 – 77 .
18 . Lin Y , Tamakoshi A , Matsuno S et al. Nationwide epidemiological survey of chronic pancreatitis in Japan . J Gastroenterol 2000 ; 35 : 136 – 41 .
19 . Nojgaard C , Bendtsen F , Becker U et al. Danish patients with chronic pan-creatitis have a four-fold higher mortality rate than the Danish population . Clin Gastroenterol Hepatol 2010 ; 8 : 384 – 90 .
20 . Spanier BW , Dijkgraaf MG , Bruno MJ . Trends and forecasts of hospital admissions for acute and chronic pancreatitis in the Netherlands . Eur J Gastroenterol Hepatol 2008 ; 20 : 653 – 8 .
21 . Tinto A , Lloyd DA , Kang JY et al. Acute and chronic pancreatitis--diseases on the rise: a study of hospital admissions in England 1989/90-1999/2000 . Aliment Pharmacol Th er 2002 ; 16 : 2097 – 105 .
22 . O ’ Sullivan JN , Nobrega FT , Morlock CG et al. Acute and chronic pancreatitis in Rochester, Minnesota, 1940 to 1969 . Gastroenterology 1972 ; 62 : 373 – 9 .
23 . Melton LJ III . History of the Rochester epidemiology project . Mayo Clin Proc 1996 ; 71 : 266 – 74 .
24 . Andersen BN , Pedersen NT , Scheel J et al. Incidence of alcoholic chronic pancreatitis in Copenhagen . Scand J Gastroenterol 1982 ; 17 : 247 – 52 .
25 . Whitcomb DC , Yadav D , Adam S et al. Multicenter approach to recurrent acute and chronic pancreatitis in the United States: the North American Pancreatitis Study 2 (NAPS2) . Pancreatology 2008 ; 8 : 520 – 31 .
26 . Frulloni L , Gabbrielli A , Pezzilli R et al. Chronic pancreatitis: report from a multicenter Italian survey (PanCroInfAISP) on 893 patients . Dig Liver Dis 2009 ; 41 : 311 – 7 .
27 . Lankisch MR , Imoto M , Layer P et al. Th e eff ect of small amounts of alcohol on the clinical course of chronic pancreatitis . Mayo Clin Proc 2001 ; 76 : 242 – 51 .
28 . Shojania KG , Burton EC . Th e vanishing nonforensic autopsy . N Engl J Med 2008 ; 358 : 873 – 5 .
29 . Lowenfels AB , Maisonneuve P , Cavallini G et al. Prognosis of chronic pancreatitis: an international multicenter study. International Pancreatitis Study Group . Am J Gastroenterol 1994 ; 89 : 1467 – 71 .
30 . Lowenfels AB , Maisonneuve P , Grover H et al. Racial factors and the risk of chronic pancreatitis . Am J Gastroenterol 1999 ; 94 : 790 – 4 .