Embed Size (px)
Citation preview
9/18/2017
1
UW MEDICINE
HOW CAN WE PREPARE FOR A MASS SHOOTING EVENT
Eileen M. Bulger, MDProfessor of Surgery
Chief of Trauma
• Joseph Ibrahim, MD Trauma Surgeon Orlando Regional Medical Center
• Joshua Corsa, MD Chief resident during Orlando Pulse Nightclub shooting
• Anne Newcombe, RN Director of Emergency services and Disaster planning HMC
• John Hess, MD Director HMC Transfusion services
• Stephen Morris, MD Emergency Medicine, Disaster response HMC
• Saman Arbabi, MD Trauma Surgeon HMC
OUR PANEL
2
• Identify our risks• EMS and Law enforcement
preparedness• Individual hospital preparedness• Healthcare system preparedness• Enabling bystanders
• Public access bleeding control kits
• Public education
AREAS OF FOCUS
3
9/18/2017
2
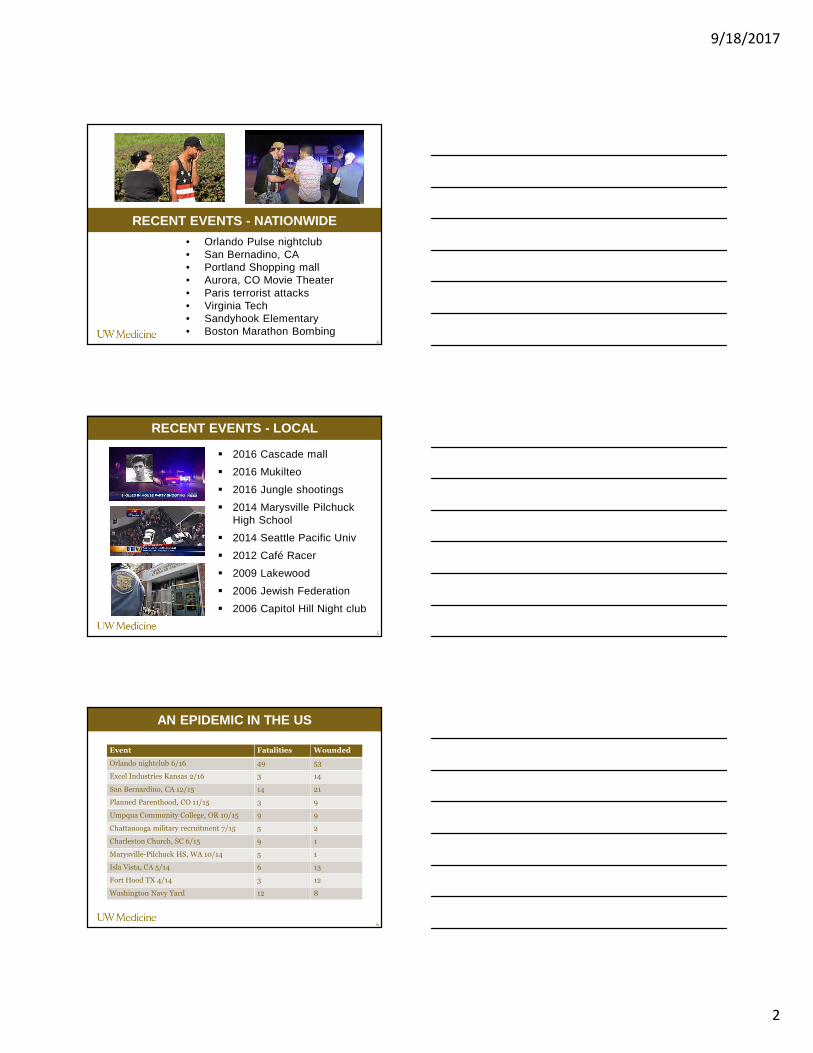
RECENT EVENTS - NATIONWIDE
4
• Orlando Pulse nightclub• San Bernadino, CA• Portland Shopping mall• Aurora, CO Movie Theater• Paris terrorist attacks• Virginia Tech• Sandyhook Elementary• Boston Marathon Bombing
RECENT EVENTS - LOCAL
5
� 2016 Cascade mall
� 2016 Mukilteo
� 2016 Jungle shootings
� 2014 Marysville PilchuckHigh School
� 2014 Seattle Pacific Univ
� 2012 Café Racer
� 2009 Lakewood
� 2006 Jewish Federation
� 2006 Capitol Hill Night club
Event Fatalities Wounded
Orlando nightclub 6/16 49 53
Excel Industries Kansas 2/16 3 14
San Bernardino, CA 12/15 14 21
Planned Parenthood, CO 11/15 3 9
Umpqua Community College, OR 10/15 9 9
Chattanooga military recruitment 7/15 5 2
Charleston Church, SC 6/15 9 1
Marysville-Pilchuck HS, WA 10/14 5 1
Isla Vista, CA 5/14 6 13
Fort Hood TX 4/14 3 12
Washington Navy Yard 12 8
AN EPIDEMIC IN THE US
6
9/18/2017
3
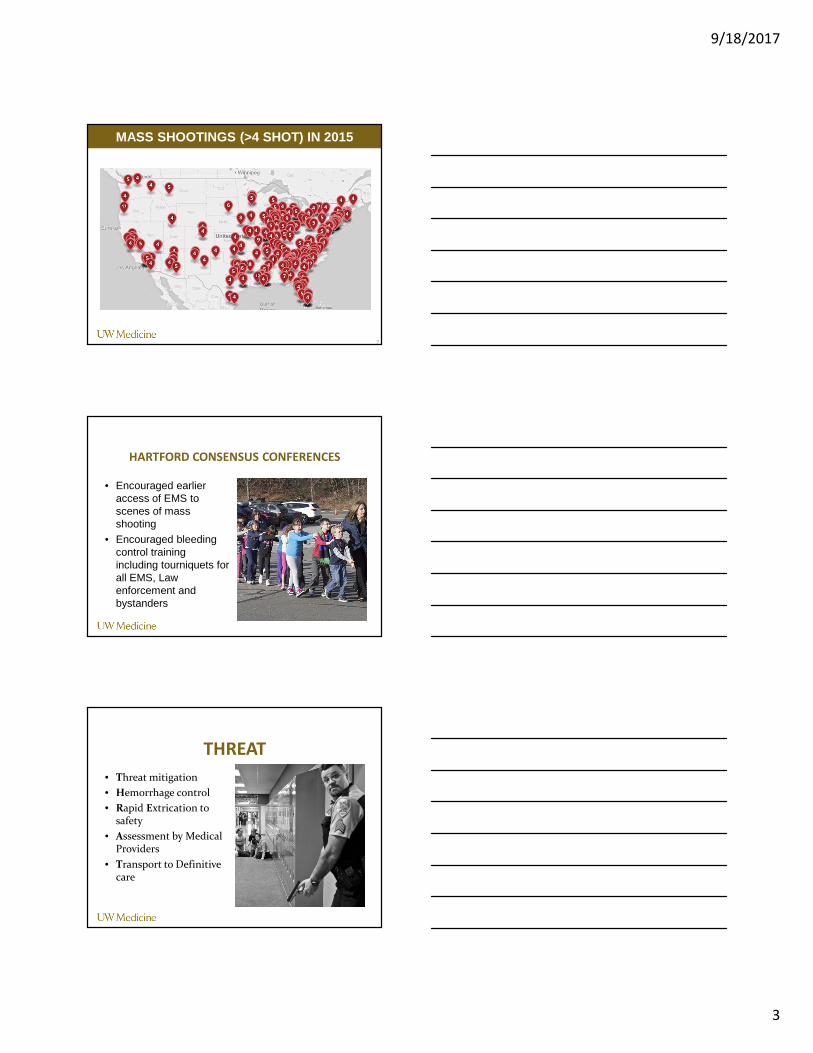
MASS SHOOTINGS (>4 SHOT) IN 2015
7
HARTFORD CONSENSUS CONFERENCES
• Encouraged earlier access of EMS to scenes of mass shooting
• Encouraged bleeding control training including tourniquets for all EMS, Law enforcement and bystanders
THREAT
• Threat mitigation
• Hemorrhage control
• Rapid Extrication to safety
• Assessment by Medical Providers
• Transport to Definitive care
9/18/2017
4
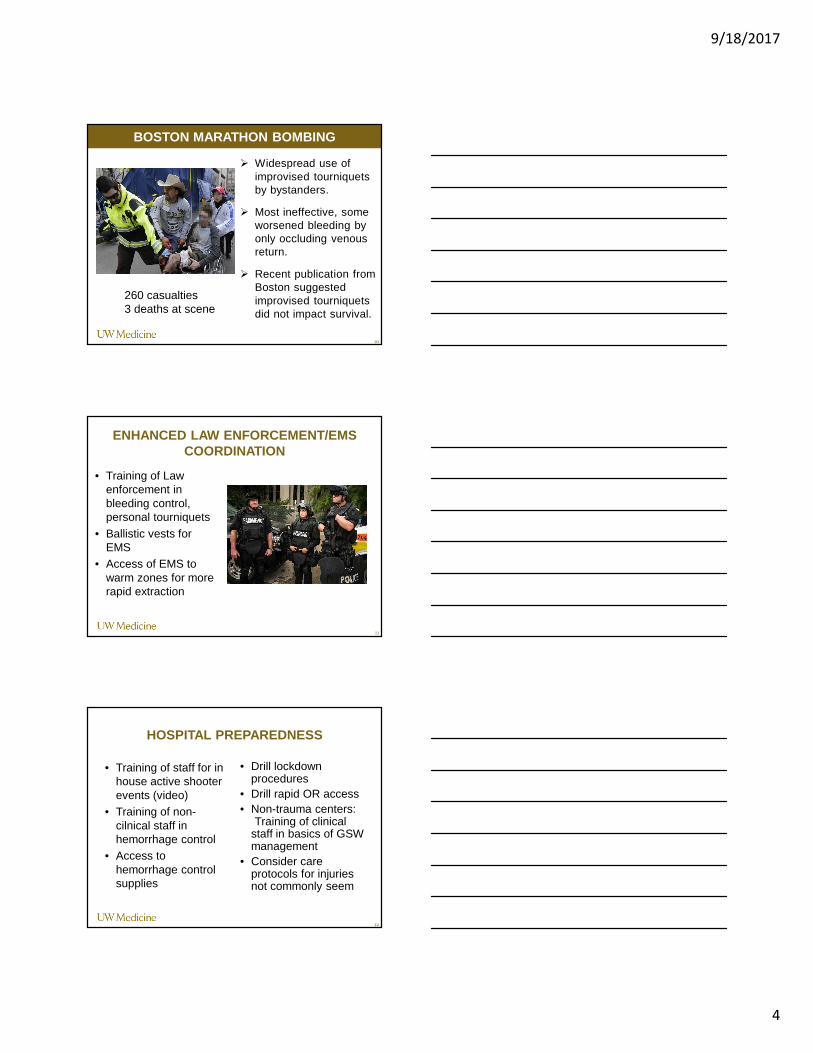
BOSTON MARATHON BOMBING
10
� Widespread use of improvised tourniquets by bystanders.
� Most ineffective, some worsened bleeding by only occluding venous return.
� Recent publication from Boston suggested improvised tourniquets did not impact survival.
260 casualties3 deaths at scene
ENHANCED LAW ENFORCEMENT/EMS COORDINATION
• Training of Law enforcement in bleeding control, personal tourniquets
• Ballistic vests for EMS
• Access of EMS to warm zones for more rapid extraction
11
HOSPITAL PREPAREDNESS
• Training of staff for in house active shooter events (video)
• Training of non-cilnical staff in hemorrhage control
• Access to hemorrhage control supplies
• Drill lockdown procedures
• Drill rapid OR access• Non-trauma centers:
Training of clinical staff in basics of GSW management
• Consider care protocols for injuries not commonly seem
12

9/18/2017
5
UW MEDICINE
THE ORLANDO EXPERIENCE
JOSEPH IBRAHIM AND JOSHUA CORSA
13
UW MEDICINE
HOW DO WE GEAR UP TRANSFUSION SERVICES?
JOHN HESS
14
UW MEDICINE
PANEL DISCUSSION QUESTIONS AND ANSWERS….
15

9/18/2017
6
UW MEDICINE
NEXT STEPS
16
17
Active Shooter Training
RUN, HIDE, FIGHT TRAINING
• http://player.theplatform.com/p/U8-EDC/ioQrJ9ffc6Uh/embed/select/fIFaJcEOM5Sz?form=html
18
9/18/2017
7
SYSTEM PREPAREDNESS
• Joint drills: law enforcement , EMS, hospitals
• Plan optimal triage for GSW victims– HD instability– TORSO/Neck/Head
wounds preferentially transported to trauma centers
19
• Expect uncontrolled flow of patients
•Self transport
•Police transport
• Least severely injured will arrive first• Closest hospital will receive a
disproportionate number of patients• Patients will not follow traditional
trauma center triage rules
WHAT CAN WE LEARN FROM OTHERS
20
DISASTER MEDICAL CONTROL• Communication –
hospitals, field, agencies
• Activation and notification
• Mitigation – event planning
• Patient distribution
• Patient acuity
• Load balancing among hospitals
9/18/2017
8
• Space
• Suspend elective operations
• Anticipate higher volume operative cases
• Expand acute care into clinic spaces
• Expand ICU spaces (Recovery room)
• Discharge as feasible• Staff
• Activate staff alert communication
• Need plan to activate surgeons and surgical teams• Equipment
• Consider cache for bleeding control supplies
• Blood Products
• SURGE CAPACITY
22
Hospital Security
•Secondary threats
•Retaliation events
Special populations
•Pediatric (School shootings)
Media controlManagement of Families
OTHER CONSIDERATIONS
24
9/18/2017
9
Stop the Bleed Campaign
1) Provide bleeding control training to the general public to enable bystanders to act in an emergency situation.
2) Provide bleeding control equipment in public places adjacent to the automated defibrillators we use for Cardiac arrest.
PUBLIC OUTREACH
26
PUBLIC CLASSES
27
9/18/2017
10
ENABLING BYSTANDERS
HOSPITAL BLEEDING CONTROL KITS
29
• American College of Surgeons, 1 day course offered at HMC
• On line version soon to be released
• Focused specifically on Hospital preparedness
30
DISASTER MANAGEMENT AND EMERGENCY PREPAREDNESS COURSE
9/18/2017
11
• Mass shootings are common and require a coordinated local/regional response
• Need joint drills which include self/bystander transport and police transport
• Anticipate poor triage
• Anticipate security threats
• Anticipate high acuity and need to OR resources and transfusion
• Need to ensure hospital staff know how to respond• Join us in promoting public education and access to
bleeding control supplies
• BECOME A STOP THE BLEED INSTRUCTOR TODAY!
SUMMARY
31
www.stopthebleedwa.org
QUESTIONS?