Embed Size (px)
Citation preview

PALS – 2010 GUIDELINESHELPFUL INFORMATION
Life Support Education

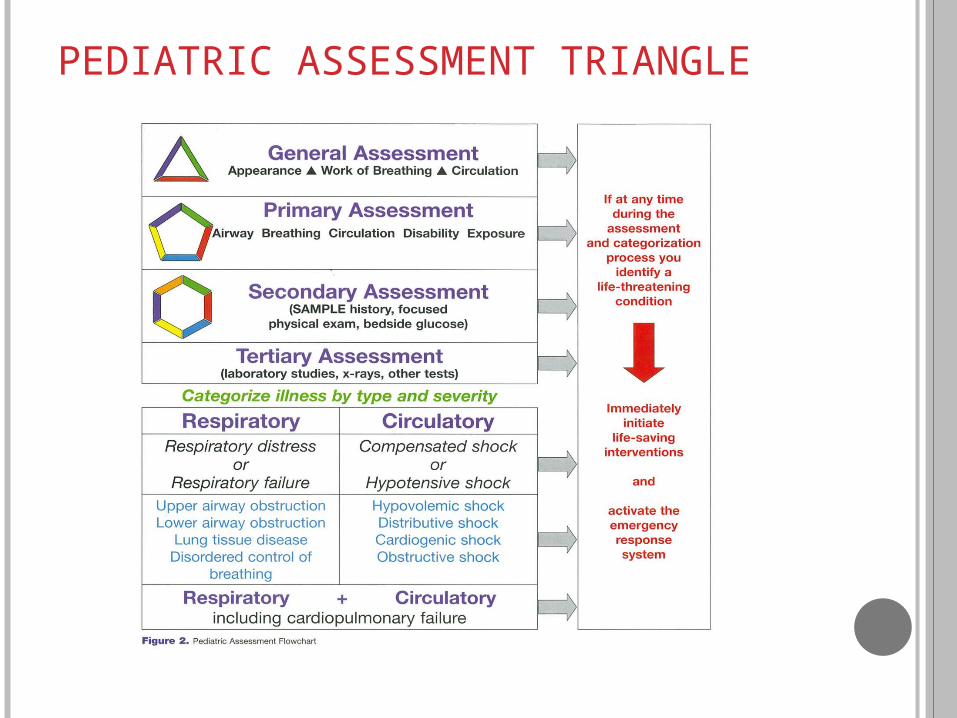
PEDIATRIC ASSESSMENT TRIANGLE
P A TApp
eara
nce
Work of B
reathing
Circulation
PEDIATRIC ASSESSMENT TRIANGLE

PEDIATRIC CHAIN OF SURVIVAL
Prevention
Early CPR
Prompt Access to EMS
Rapid Pediatric Advanced Life Support (PALS)
Integrated Post-Cardiac Arrest Care

SYSTEMATIC APPROACH
Evaluate Primary Assessment
Identify Secondary Assessment Focused Exam SAMPLE History
Intervene Diagnostic Tests Tertiary Assessment

ASSESSMENT

AIRWAY & RESPIRATORY CONSIDERATIONS
OPA – NPA – When do we use them
Signs of progressive Respiratory Failure -Respirations decreasing and more lethargic
Following Breathing Treatments – ABC’s
Indications for needle decompression
Treatment options for allergic reactions

AIRWAY MANAGEMENT RESCUE BREATHING
One (1) Rescue Breath every 3 – 5 Seconds
Pediatric Patient with a pulse but not breathing BVM = 1 Breath every 3 – 5 seconds
Has an ET Tube = 1 Breath every 3 – 5 seconds
CPR with advanced airway – Continuous Compressions and 1 breath every 6 –
8 seconds (8 – 10/minute)

ET Tube Sizes
UN-Cuffed Age/4 + 4
Cuffed Age/4 + 3.5
Listen------- Epigastric AXilla Lungs

BREATHING Diminished breath sounds
Diminished rise of the chest on one side
Respiratory distress with stridor (possible allergic reaction (Epi IM)
Barking cough (moderate stridor & retractions) (Nebulized Epi)

AIRWAY & RESPIRATORY CONSIDERATIONS
Oxygen should be administered to patients with low O2 saturations and increased work of breathing
Nebulized Epinephrine is for stridor, mild to moderate retractions, barking cough

ADDITIONAL INFORMATION
Tracheal deviation – absence of breath sounds - Needle decompression
Following a seizure – ABC’s manage airway/breathing
Equipment Treat patient

Blood Pressure- Lower 5th percentile
Estimate of Minimum Systolic Blood Pressure
Age Minimum systolic blood pressure
0 to 1 month 60 mm Hg >1 month to 1 year 70 mm Hg 1 to 10 years of age 70 mm Hg + (2 x age in years) >10 years of age 90 mm Hg
RHYTHM DISTURBANCES
Hypovolemic – Fluid boluses
SVT- Vagal Maneuvers – Adenosine 0.1 mg/kgAdenosine 0.2 mg/kgSynchronized Cardioversion - 0.5 - 1 joulesSynchronized Cardioversion – 2 joules/kg

Bradycardia in Pediatrics
Initial thoughts - Oxygenation and Ventilation CPR if HR <60/min with poor perfusion
despite oxygenation and ventilation
Expert Consultation Epinephrine - .01 mg/kg every 3 – 5 minutes May consider Atropine 0.02 mg/kg if vagal response Consider pacing if not responding or heart blocks Treat underlying cause (H’s & T’s)

Narrow Complex Tachycardia in Pediatrics
SVT (Supraventricular tachycardia) Children - > 180 Infants - > 220
History – Level of Consciousness Vagal Maneuvers IV/IO Access Adenosine 0.1 mg/kg (max 6mg)
0.2 mg/kg (max 12 mg) [second dose]
No Access or condition deteriorates – Synchronized Cardioversion 0.5 – 1 joule/kg
If condition continues – 2 joules/kg

Wide Complex Tachycardia in Pediatrics
History – Level of Consciousness Consider Adenosine if time Stable Patient –
Amiodarone 5 mg/kg over 20 to 60 min. Expert Consultation Unstable Patient –
Synchronized Cardioversion 0.5 – 1 joule/kg
CARDIAC ARREST Scene Safety PPE Establish Unresponsiveness and Lack of Normal Breathing Sudden Collapse - Activate Emergency System Get AED/Defibrillator Check Pulse Begin Chest Compressions C – A – B Activate EMS after 2 minutes of CPR if not already done For victims of Sudden Collapse = Use AED as soon
as it arrives ! If there are no Pediatric Pads – Use the Adult Pads

Cardiac Arrest
Shockable Rhythm (VF/Pulseless VT) Deliver 1 shock – 2-4 joules/kg Resume CPR immediately (Chest Compressions) IV/IO Access Epinephrine 0.01 mg/kg every 3 – 5 minutes Consider advanced airway Defibrillate at 4 joules/kg Amiodarone – 5 mg/kg
May repeat 1 or 2 times Consider Reversible Causes

Cardiac Arrest
Non-Shockable Rhythm CPR – starting with Chest Compressions IV/IO Access Epinephrine 0.01 mg/kg every 3 – 5 minutes Consider advanced airway CPR Consider Reversible Causes
H’s & T’s Hypovolemia Hypoxia Hypoglycemia Hydrogen Ions (Acidosis) Hypo/Hyperkalemia Hypothermia TRAUMA Tension Pneumothorax Tamponade – Cardiac Toxins Thrombosis – Pulmonary Thrombosis – Coronary

IO Access
DO NOT USE if: Fracture Crush injury Bone disease Previous attempts

VENTILATIONS DURING CPR
Compression to Ventilation Ratio 30:2 – 1 Rescuer CPR
15:2 – 2 Rescuer CPR
CPR with ETT in place Continuous Chest Compressions Ventilations – 1 Breath every 6 to 8 seconds
(8 – 10 breaths/minute)

POST ARREST CARE
Goals – Preserve neurologic function Prevent secondary organ injury Diagnose & Treat cause of illness Enable patient to arrive at Pediatric Tertiary-Care
facility in optimal physiologic state
Frequent assessment is necessary because of risk of deterioration
Maintain Oxygen saturation between 94 and 99% following ROSC

CAPNOGRAPHY FOR ROSCCAPNOGRAPHY FOR ROSC
Capnography is used for verification of advance airway and for indication of return of spontaneous circulation (ROSC) during CPR.
5037.52512.50
mm
Hg
[1 Minute Interval]
DEFIBRILLATION EXAMPLEVF/PULSELESS VT
2 – 4 Joules/kg CPR Epinephrine 0.01mg/kg every 3 – 5 minutes CPR Defibrillate 4 joules/kg CPR Epinephrine OR Amiodarone 5 mg/kg CPR Defibrillate 4 joules/kg up to 10 joules/kg or max adult
dose CPR Consider Causes (H’s & T’s)

WHY ADENOSINE MAY BE HELPFUL VT VS PRE-EXCITED ATRIAL FIBRILLATIONIN A 9 YEAR OLD

TWO MAJOR CAUSES OF DEATH IN PEDIATRIC TRAUMA…….
____ I ____ W ____ ____
____ O ____ P ____ ____ M ____ ____ ____
AND
U ____ ____ ____ C ____ ____ NI ____ ____ D
____ E ____ O ____ ____ H ____ ____ E





























