Embed Size (px)
Citation preview

Palliative care/medicine
Dr. Reino Pöyhiä, MD, PhDHead of the Dept of Anaesthesia, Helsinki University Central Hospital, Helsinki, FinlandAssosciate Professor of Anaesthesiology and Palliative MedicineConsultant Anaesthesiologist, Special Competence in Cardiac Anaesthesia, Palliative Care and Pain MedicineFinnish Christian Medical Society

Mr Jacob, 35 yrs, HIV+
• comes to clinic because of nausea & diarrhea.
• 6 mo ago his ART regimen was changed to Nelfinavir, AZT, and ddI ←immunologic treatment failure.
• previously CNS toxoplasmosis + lung TB. • he lost his job and started drinking ETOH daily
since his wife died in a car accident 1 year ago. STAGE 4 illness, gi symptoms probably due to ART, but more info is needed about the onset and nature of symptoms, OI´s, CD4 and ARV relationship

Mr Jacob (cont)
• alert and oriented, but fatigued, chronically ill• T 37.7 HR 110 BP 90 / 70 • 47 kg (7 kg weight loss since last visit)• pale conjunctivae• white plaques on soft palate • normal exam otherwise
•Usually BP 120/80 -130/85 , HR 60-80.•At the last clinical visit previously no documented thrush/ pale conjunctivae. • Ideal body weight 55kg.

Mr Jacob (cont)
• volume depletion• nausea & diarrhea• clinical treatment failure (new thrush, wt loss)• pallor• alcohol dependence• unemployment
• What are his palliative care needs?

What´s palliative care?
• "an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual."

History of palliative carebackground: Roman catholic monasteries – Knights
Hospitalier of St John of Jerusalem 1300- hospice > hospes (lat., master) & hospitium (lat., meeting
place, hospitality)
a hospice movement in the 20th century, religious orders created hospices that provided care for the sick and dying in London and Ireland.
- Dame Cicely Saunder´s St Christopher´s Hospice 1967
palliative care has become a large movement internationally

International movement• USA: from a volunteer-led movement to a vital part of the
health care system, 1st US hospital-based palliative care programs 1980s
• Africa- WHO “community health approach to palliative care for HIV/AIDS
and cancer patients in Africa project.” 2001- Botswana, Ethiopia, Uganda, Tanzania, Zimbabwe - Tanzania: 1999 HBC, National Multisectoral HIV/AIDS Conference
2002, PASADA/ORCI/Muheza District Hosp 2005 projects, TPCA 2004• Australia: 320 palliative care services since 1987• Japan: 120 palliative care services since 1997• Mongolia: palliative care incorporated into National health
plan• Europe

EAPC: Atlas of palliative care services 2013

Principles of palliative care
1. goal: QoL ↑for patients and their families2. prevention and relief of suffering
- pain and other physical problems - psychosocial and spiritual issues
3. an integral part of a comprehensive care and support framework - multidisciplinarity
4. in a continuum of care from the time the incurable disease is diagnosed until the end of life
5. dying as a normal process and affirms life- intends neither to hasten or postpone death
6. offers support to help the patient and family cope during the patient’s illness & dying and in the bereavement period

Essential attitudes“staff requirements”
• care and treatments are based on the needs of the patient
• hope• dignity = state of being worthy of honour or
respect• resilience = the capacity to withstand
exceptional stress and demand• a good deal of creativity and readiness to
change old habits!

Philosophy = Christianity!
• Albert Schweitzer: “We must all die. But, that I can save him from days of torture, that is what I feel as my great and ever new privilege. Pain is a more terrible lord of mankind than even death itself.”
• Our Lord Jesus suffered because of us – we don´t need to suffer
• Gal 6:2

Who receives palliative care?
individuals struggling with various diseases
individuals with chronic diseases such as- cancer- cardiac disease- COPD, lung fibrosis- kidney failure- dementia, Alzheimer's- HIV/AIDS- amyotrophic Lateral Sclerosis (ALS)- hereditary neuromuscular diseases

African population 2008
• 22 million people living with HIV/AIDS (= 67 per cent of the global disease burden)
• 1.9 million new infections reported in 2008• 700,000 new cancer cases• Expected increase in non-communicable
diseases

Patient
andFamily
VolunteersPhysicians
Spiritual Counselo
rs
Social Workers
Pharmacists
Home Health Aides
Therapists
Nurses
Providers – TEAM WORK!!

Providers
• The principles of palliative are applicable at all stages of care
• Specialists are needed – for special care (e.g. palliative sedation)– for consultations– as organizators– as administrators– in research and education

Palliative medicine as a speciality
• Europe– spesiality UK (1987), Ireland (1995), Italy, Spain,
Switzerland, Norway– subspesiality: Poland (1999), Romania (2000),
Slovakia (2005), Germany (2006)– special competence: Finland, France
• USA: subspeciality• Tanzania: postgraduate diploma course• Australia, New-Zealand, Taiwan, Hong Kong
– special competence

WHO: Palliative care – where and by whom

Palliative care – where and by whom?

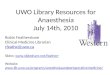
Palliative vs. E-o-L care
Image courtesy of http://www.ersj.org.uk/content/32/3/796.full

Death
High
LowTime
Function
Death
High
LowTime
Function
Organ failure
6
Dementia, frailty and decline
Death
High
LowTime
Function
5
Cancer
End-of-life care – when?

Palliative vs life-prolonging treatments
Symptom relief
•pain•dyspnea•nausea•Vomiting•etc
Support
•Emotional•Spiritual•Psychological•social
CPR
Ventilator, ICU
(“Major”) SurgeryAntibiotics for infection
Fluid-therapy
Rx of hypercalcemia
Hemodialysis
Hyperalimentation, NG tubes
End-of-life/palliative care Curative
“In-between”
The NEEDS of a dying individual differ from those of a living one!

Symptoms at E-o-L Prevalence (%) in different pathologies
Cancer AIDS CHF COPD ChRF
PAIN 35−96 63−80 41−77 34−77 47−50
DEPRESSION 3−77 10−82 9−36 35−71 5−60
DYSPNOEA 10−70 11−62 60−88 90−95 11−62
FATIGUE 32−90 54−85 69−82 68−80 73−87
Solano J ym. A comparison of symptom prevalence in far advanced cancer, AIDS, heart disease, chronic obstructive pulmonary disease and renal disease. J Pain Symptom Manage 2006;31:58-69; PMID 16442483

Pre-HAART Palliative Care Model
Diagnosis Death
Therapies to modify disease(curative, restorative intent) Hospice
BereavementCare
6m

Current model
24
Diagnosis Death
Therapies to modify disease(curative, restorative intent) Actively
Dying
BereavementCare
Life Closure
Palliative Care: interventions intended to relieve suffering and improve quality of life
6m

Palliative and ARTAntiretroviral therapy does not avert the need for palliative care
Why?• 40–50% of patients
experience virological failure
• 40% of patients have adverse reactions
• HIV-related cancers still occur
• Psychological and spiritual needs persist
What?• Treatment of antiretroviral
side effects • Management of HIV
complications• Relief of psychosocial
challenges • Improved ART adherence• Reduction of drug
resistance in the individual and community
• Preparation for end-of-life

HIV/AIDS – when EOL care starts?
• CD4 <25 despite adequate ART and functional capasity↓:
+ CNS lymfomaOR constant weight loosingOR mycobacterial infection (TBC)OR progressive leucoencephalopathyOR Kaposi´s sarcoma in the viscera or visceral
lymfomaOR another severe infection
One of these
Lamba & Quest, Ann Emerg Med 2011; 57: 282-90

Palliative care needs in Africa• pain and symptom control • financial support• emotional and spiritual support• food and shelter• recognition of the palliative care principles at all levels of
healthcare– dedicated (and educated) RN, MO, DR etc.– CTC professionals – consultation service by educated specialists for hospital wards
and outpatient units• hospice care (home and hospice center)/ expert center
– e.g. Ilembula Lutheran Hospital?– palliative care specialists: RN, DR
• legal help and school fees

Home-based care
• the most common service model in Africa• limitations
– inadequately trained care givers – lack access to essential drugs– limited access for patients in inaccessible
geographical areas– stigma

Challenges to palliative care in Africa
• primary health care vs palliative care• late disease presentation • cancer patients’ palliative care under-resourced• inadequate diagnostic facilities and assessment skills • poor availability of chemotherapy and radiotherapy• shortage and fear of opioids
– regulatory and pricing obstacles – ignorance and false beliefs
• bearing bad news could be seen as the cause of a terminal illness
• labeling patients as “terminally ill” may have harmful consequences– isolation– denied access to care

Mr Jacob (cont)
• Nausea• Diarrhea• Fatigue• Substance dependence• Unemployment• Lack of social support
• What are this patient’s palliative care needs?
• nausea- assessment (eg serum chemistry / LFT) and management (eg antiemetic)
• diarrhea - assessment (eg stool study) and management (eg antidiarrheal)
• fatigue - assessment (eg CBC) and management (eg volume resuscitation / transfusion)
• substance dependence and psychosocial issues - referral ?

Mr Jacob (cont)• returns to the clinic 1 mo later
– diarrhea & nausea improved with interventions offered at the last visit
– still fatigued– continues to use ETOH. – lives with his uncle 500 km away from
clinic
• returns to the clinic 4 mo later– very fatigued – new: burning lower extremity pain
•peripheral neuropathy secondary to ddI. •ddg: HIV related peripheral neuropathy (? progression - earlier tx failure•increasing time btw visits- is he taking his medicine???•duration?•examine!•tx: ddI to eg TDF or reduce dose•drugs for neuropathic pain

Mr Jacob (cont)
• returns to clinic 2 wks later with continued pain despite – dose ↓ in ddI (200 ->125 bid) – stopping ETOH– taking Ibuprofen 600mg bid.
• physical exam unchanged
→ WHO ladder •weak opioid•Note! NRTI neuropathy may take 4-6 weeks to improve, or it may not improve at all. • switch ddI to another antiviral med

Mr Jacob: What then?• J returns 2 mo later
– tachypneic, cyanotic, delirious– unable to stand – he says to you “I can’t breath”– LAB: Hgb 5 gm/dl, MCV 104, Creatinine 1.1.– T 38.5 HR 110 BP 98 / 70 – RR 35

Dyspnea – treatments at E-o-L• position patient for comfort
– prop patient forward using pillows – may allow better lung expansion / gas exchange
• provide cool circulating air (> O2)• encourage presence of family and caregivers• consider pursed-lip breathing• promote soothing activities, such as prayer or listening to
relaxing music• drugs:
– opioids: morphine!– anxiolytics– bronchodilatators– antibiotics (?)– steroids (?)– diuretics (?)

… Mr Jacob´s final:– admitted to the hospital; started on high dose Co-
trimoxazole plus steroids for treatment of PCP– a blood transfusion– despite 10 days of appropriate therapy for PCP, the
patient’s condition continues to deteriorate.– no NG tube, no iv-line, no antibiotics, stop ART – morphine– uncle and sister arrive later to the hospital– the family wants to know his status and prognosis– peaceful death in “arms of beloved”

“SPIKES” protocol for giving bad news
• Set up the interview: mental and physical preparation
• Perception: assess what the patient knows about the medical situation
• Invitation: ask how much they want to know• Knowledge: give the medical facts• Emotion: respond to patients emotions• Strategy and summary: negotiate a concrete
follow-up step

End-of-life discussions
• utilize SPIKES principles• elicit patient/family’s understanding and values• use language appropriate to the patient• align patient and clinician views• use repetition to show you are listening• acknowledge emotions, difficulty, fears• use reflection to show empathy• don´t laugh!• tolerate silences

Palliative care efficacy in AIDSHarding et al. AIDS Care 25; 795-804, 2013

Palliative care is good for HIV/AIDSHarding et al. A Systematic Review 2012

Good palliative care prolongs life!
• Temel et al. NEJM 2010• 151 pts w lung cancer
– Standard care– Palliative care– ALL patients had similar
oncological care for ca
• Palliative group– better QoL– less depressive

Summary• definition of palliative care by WHO• principles of palliative are applicable to all stages of
care• goal: alleviation of symptoms & improving QoL• end-of-life care is a final part of palliative care• death as a natural end of life – no postponing nor
hastening• special education and specialists are needed, team!• good palliative care provides quality and length in
living• high priority in health care planning internationally• philosophically and ethically based strongly on
Christian values

Thanks!
CITY OF HELSINKI, FINLAND