Embed Size (px)
Citation preview

Palliative Care Approach to Breathlessness
Dr. Thiru Thirukkumaran CMO / Palliative Medicine Senior Lecturer in Palliative Medicine Northwest Palliative Care Services Rural Clinical School, Burnie, Tasmania University of Tasmania

What is ‘Breathlessness’ ?
Why “Breathlessness” is important in Palliative care?
What are the mechanisms of Breathlessness?
What are the different causes & how do we manage the different situations?
Why Cancer patients get breathlessness..?
Care Management guidelines for breathlessness in Palliative care Setting
Outline of the session

What is ‘Breathlessness’ ?

Definition:
“a sense of awareness of increased respiratory effort that is unpleasant & that is recognized by the patient as being inappropriate” - Kumar & Clark / Text Book Of Medicine
Breathlessness / SOB / Dyspnoea

Breathlessness should be assessed in relation to the patient’s life-style
Healthy Person
COPD Person
Resting
Exercising
15%
35% - 40% 10% - 15%
4%
Better Living with Chronic Obstructive Pulmonary Disease - A Patient Guide (2nd Edition)
The State of Queensland (Queensland Health) and The Australian Lung Foundation 2012.

We manage patients’ symptoms throughout their cancer or their chronic illness journey (From reasonable physical fitness status to poor functional status)
We communicate with colleagues (oncologists, CNs, ) in specific language
- Australian Karnofsky Performance Scale (AKPS)
Why patient’s life-style or Functional status is important to us?

Grade 1: No Breathlessness
Grade 2: Breathlessness on severe exertion
Grade 3: Breathlessness on mild exertion
Grade 4: Breathlessness at rest
Functional & Therapeutic Classification of dyspnoea The New York Heart Association

Why “Breathlessness” is important in Palliative care?

J Potter et al. Palliative Medicine 2003; 17: 310 - 314
Symptoms in 400 patients referred to palliative care services: prevalence & patterns
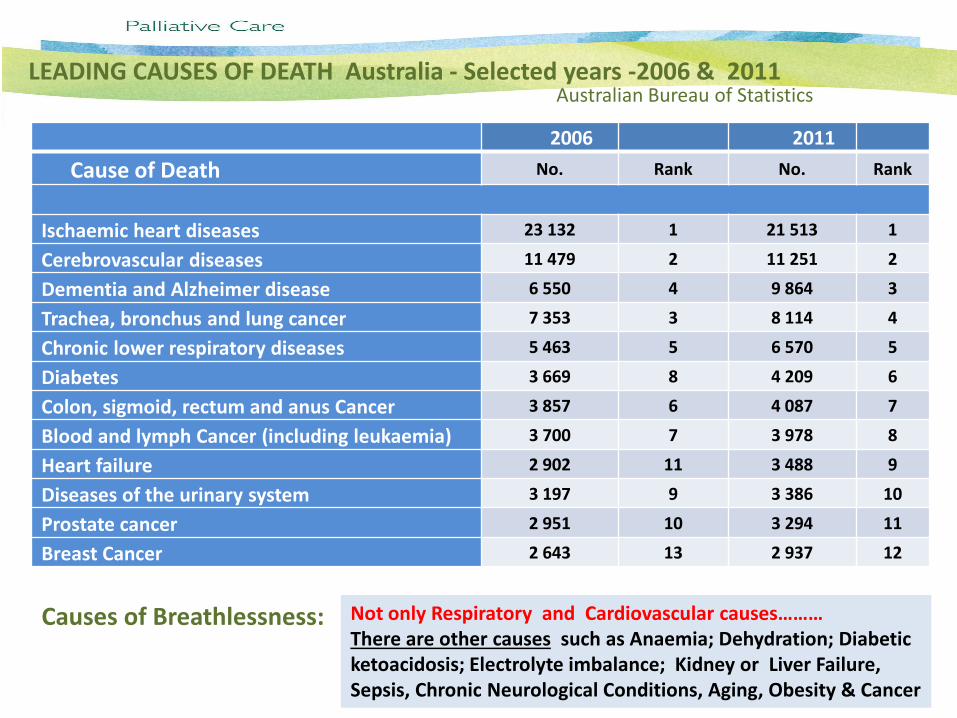
LEADING CAUSES OF DEATH Australia - Selected years -2006 & 2011
2006 2011
Cause of Death No. Rank No. Rank
Ischaemic heart diseases 23 132 1 21 513 1
Cerebrovascular diseases 11 479 2 11 251 2
Dementia and Alzheimer disease 6 550 4 9 864 3
Trachea, bronchus and lung cancer 7 353 3 8 114 4
Chronic lower respiratory diseases 5 463 5 6 570 5
Diabetes 3 669 8 4 209 6
Colon, sigmoid, rectum and anus Cancer 3 857 6 4 087 7
Blood and lymph Cancer (including leukaemia) 3 700 7 3 978 8
Heart failure 2 902 11 3 488 9
Diseases of the urinary system 3 197 9 3 386 10
Prostate cancer 2 951 10 3 294 11
Breast Cancer 2 643 13 2 937 12
Australian Bureau of Statistics
Causes of Breathlessness: Not only Respiratory and Cardiovascular causes……… There are other causes such as Anaemia; Dehydration; Diabetic ketoacidosis; Electrolyte imbalance; Kidney or Liver Failure, Sepsis, Chronic Neurological Conditions, Aging, Obesity & Cancer
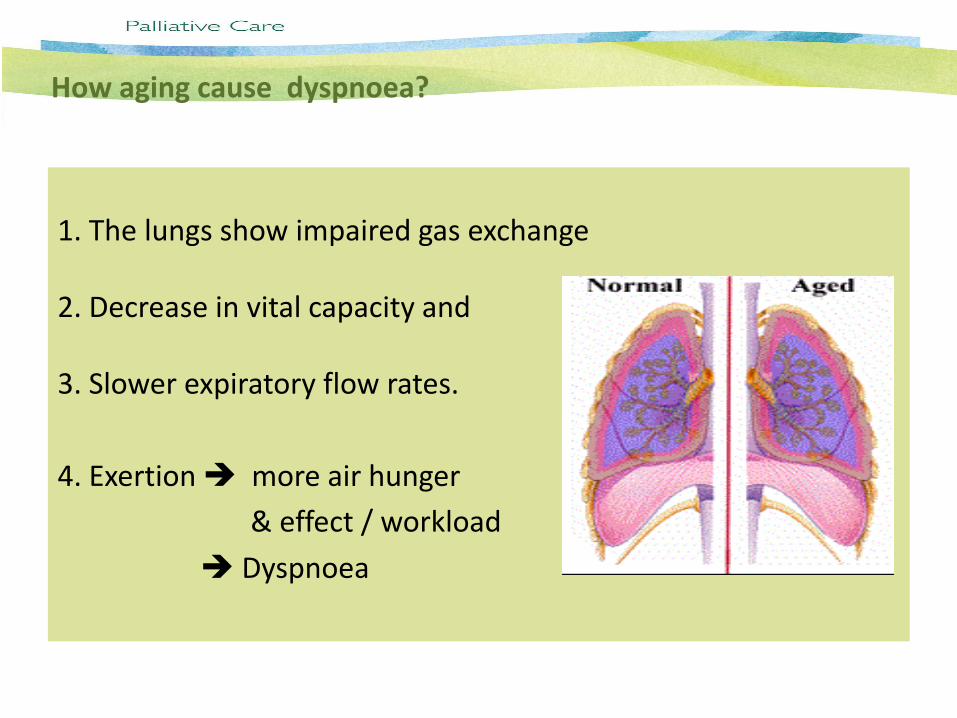
1. The lungs show impaired gas exchange 2. Decrease in vital capacity and 3. Slower expiratory flow rates.
4. Exertion more air hunger
& effect / workload
Dyspnoea
How aging cause dyspnoea?

Breathlessness is a common symptom in patients with advanced malignancy. Approximately 70% of patients experience breathlessness during the last six weeks of life.
Breathlessness in the patient with advanced cancer is usually multifactorial. It is important to consider potentially reversible causes of SOB & treat where appropriate
Causes of Breathlessness in patients with advanced Cancer Anaemia Iatrogenic e.g. Chemotherapy Pericardial Effusion
Anxiety Infection Pleural Effusion
Ascites Intra-thoracic malignancy Pneumothorax
Bronchospasm Ischemic Heart Disease Pulmonary Embolism
CCF Lymphangitis Carcinomatosis Pulmonary Fibrosis
COPD Neuromuscular Disorders Stridor
Fatigue/Cachexia Pain SVCO

What are the mechanisms of Breathlessness?

Dyspnoea is the result of a complex interaction of physiological, psychosocial, social, and environmental factors & it not fully understood
Sensory receptors (chemoreceptors, mechanoreceptors, vagal (cold) receptors, slowly adapting stretch receptors (SARs), rapidly adapting stretch receptors (RARs), & C-fibre receptors) located through out the respiratory system are considered to be responsible for generation of dyspnoea.
Afferent information from the sensory receptors is processed at the cortex along with the respiratory motor command from the cortex and brainstem, and a mismatch between the motor command and the incoming afferent information may result in dyspnoea
1. Nishino, T. (2011). Dyspnoea: underlying mechanisms and treatment. Br. J. Anaesth. (2011) 106 (4): 463-474. 2. Torres M, Moayedi S (May 2007). "Evaluation of the acutely dyspnoeic elderly patient". Clin. Geriatr. Med. 23 (2): 307–25. 3. Harrison's Principles of Internal Medicine (Kasper DL, Fauci AS, Longo DL, et al (eds)) (16th ed.). New York: McGraw-Hill
What are the mechanisms of Breathlessness?

Motor command–afferent mismatch

Stimulation Receptors Quality
1. Hyperpnoea Central chemoreceptors Air hunger
2. Hypoxia Peripheral chemoreceptors
3. Respiratory motor command Central corollary discharge Work/effort
Muscle contraction Chest wall receptors
Muscle fatigue Muscle spindles
Mechanical loads Joint receptors
Tendon receptors
Mechanoreceptors
4. Bronchoconstriction RARs, C-fibre receptors Chest tightness
5. Lung inflation SARs Dyspnoea relief
Quality of Dyspnoea and the underlying mechanisms
Nishino, T. (2011). Dyspnoea: underlying mechanisms and treatment. British Journal of Anaesthesia (2011) 106 (4): 463-474.
Hyperpnea is increased depth of breathing when required to meet metabolic demand of body tissues
Dyspnoea is not a single sensation and there are at least three distinct sensations including (1) air hunger,
(2) work/effort, and
(3) chest tightness.
Like pain, dyspnoea has at least two distinct separate dimensions, that is, (a) a sensory and (b) an affective dimension.
Recent neuro-imaging studies suggest that neural structures subserving pain and dyspnoea might be shared, and therefore the neurophysiological and psychophysical approaches used to understand pain can be applied to dyspnoea research.
Nishino, T. (2011). Dyspnoea: underlying mechanisms and treatment. British Journal of Anaesthesia
(2011) 106 (4): 463-474.
Neural pathways of dyspnoea

Quality of Dyspnoea
Treatments Specific Pharmacological and Non-pharmacological approaches
Air hunger Decrease in ventilatory drive Opioids, THAM, bicarbonate, oxygen
Changes in perceptual sensitivity to sensation Opioids, anxiolytics
Alterations in vagal afferent information Airway anaesthesia, vagal block, inhaled furosemide
Work / effort Decrease in ventilatory drive Opioids, THAM, bicarbonate, oxygen
Alterations in afferent information from chest wall and respiratory muscles
Vibration
Changes in perceptual sensitivity to sensation Opioids, anxiolytics
Chest tightness Alterations in vagal afferent information Airway anaesthesia, vagal block, inhaled furosemide
Changes in perceptual sensitivity to sensation Opioid, anxiolytics
Different quality of dyspnoea and Proposed treatment
(THAM) tris-hydroxymethyl aminomethane
Nishino, T. (2011).
Nishino, T. (2011). Dyspnoea: underlying mechanisms and treatment. British Journal of Anaesthesia (2011) 106 (4): 463-474.

Changes in perceptual sensitivity:
Opioids and anxiolytics can alter perceptual sensitivity, and this change in perception can blunt the patient’s response to dyspnoea stimuli.
Although the effectiveness of opioids in improving dyspnoea is fairly consistent, there are conflicting results from trials of the effectiveness of various anxiolytics in reducing dyspnoea. (Diazepam & Promethazine studies)
Despite these conflicting observations, it is reasonable to use anxiolytics in those with morbid anxiety or those having the panic and fear associated with acute episodes of severe dyspnoea.
Treatment of dyspnoea based on the neurophysiological mechanisms
1. Decrease in ventilatory drive
Several studies have shown that opioids improve both dyspnoea and
exercise performance in patients with COPD.
In cancer patients, a significant improvement in dyspnoea after a single
bolus dose of morphine has been reported in placebo-controlled
crossover studies.
Opioids have also been shown to produce a significant improvement in
aerobic exercise capacity in patients with heart failure.
The mechanisms of action of opioids are not fully understood. However,
opioids are respiratory depressants that reduce the central processing
of neural signals within the CNS.
Endogenous opioids modulate the increase in ventilatory output and dyspnoea
during severe acute bronchoconstriction in asthmatic patients. Thus, opioids
are the mainstay of the drug management of dyspnoea in many different
clinical situations.
Treatment of dyspnoea – More evidence….!
Care Management guidelines for breathlessness in Palliative care Population

Management approaches include both Non-Pharmacological & pharmacological Measures:
How Non-Pharmacological Measures works in Dyspnoea?
Concept of ‘Total dyspnoea’
Dyspnoea is the result of a complex interaction, of physiological psychosocial, social, and environmental factors
MDT approach in Palliative care Services Medical team, Psychologist, social worker, chaplain, allied health team, & others
Palliative Care Guidelines for Dyspnoea

What are the Non-Pharmacological Measures use in Pal care?

Non-pharmacological options are important and may be used alone or in conjunction with medication.
They include:
1. Reassurance and Explanation
2. Fan or Cool Air across the face.
3. Adequate positioning of the patient to aid breathing
4. Breathing exercises and Relaxation training
5. Advice on modifying life style
6. Acupuncture, aromatherapy and reflexology
Non-pharmacological Options

Breathing exercises and Relaxation training

Opioids, Short acting Benzodiazepines & Oxygen are the mainstay of medical management
Benzodiazepine: Commonly used are Oxazepam / Lorazepam / Alprazolam Short acting Benzos are useful in cutting the “SOB Anxiety cycle”
Pharmacological Measures:

Oxazepam 7.5 -15mg sub-lingual or oral route prn [T1/2 = 4–15 hrs]
Lorazepam 0.5-1mg sub-lingual or oral route prn [T1/2 =10–20 hrs]
Alprozolam 0.25-0.5mg orally tds to 4-6hourly prn [T1/2 =6.3 to 26.9 hrs]
Short acting Benzos are useful for paroxysmal breathlessness
Diazepam is used for more persistent symptoms The dosage should be titrated according to the response. Usually 2-5mg orally nocte.
In patients unable to tolerate oral-medication, or those in the dying phase, sc route of Midazolam 2.5-5mg prn (2-4 hourly);
If the prn doses are effective, this can be given as subcutaneous infusion via syringe driver over 24 hours: 10-20 mg /24 hours
Benzodiazepine - 01

Oxazepam or Alprozolam are less likely to lead over-sedation & concentration issues
Oxazepam & Lorazepam have no active metabolites, and more easily tolerated in patients with hepatic impairment. (use reduced dose!)
Clonazepam drops is widely used in Tassie for SOB & be aware of its long half life & cumulative effect (elimination half-life of 19–60 hours)
Midazolam has amnestic effects, and more sedative than the other benzodiazepines; beneficial for acute episode of anxiety with SOB
Doses need to be titrated according to effect, monitor the target symptoms and adverse effects.
If patients are on benzodiazepine for sometime, there is strong possibility of ‘tolerance’ to the drug, either substantial increase of doses needed or opioids will be the mainstay of therapy!
Benzodiazepine - 02

Opioids
Opioids are the drug of choice & should be considered in Grade 3 or 4 SOB (Abernethy, Currow et al. 2003)
If the patient is opioid naïve start with Morphine Mixture (Ordeine Susp) 2.5mg 4 hourly PRN +/- background long-acting Morphine 5-10mg po bd
If the patient is established on regular opioid Increase the dose by 30-50% every 2-3 days {Titrate according to response; benefit versus side-effects}
Nebulised Opioids: There is on going research work….. The current evidence does not supporting the use of nebulised opioids in the management of intractable breathlessness!
Subcutaneous injection or infusion of Opioids: Use only if the patient unable to swallow or tolerate oral morphine or oral mal-absorption issues (The dose will be decided on whether patient is already on opioid or not)

Take care of renal impairment patients: Available Options – either give reduced dose of morphine / oxycodone according to patient’s eGFR numbers or give Hydromorphone preparations
Doses in renal impairment eGFR Morphine Dose Oxycodone Dose Hydromorphone Dose
20-50 75% of normal dose Dose as normal Dose as normal
10-20 use small doses Use small doses Start with reduced dose (e.g.: 2.5 to 5mg) & titrate up to response
< 10 use very small doses Avoid Start with educed dose (e.g.: 1. 25 to 2.5mg) & titrate up to response [The Renal Drug Hand Book edited by Caroline Ashley & Aileen Currie; UK Renal Pharmacy Group]
? Alfentanil / Hydromorphone subcutaneous Infusion
Opioids – Renal Impairment

Supplemental oxygen therapy (o2) is not necessarily the answer to Breathlessness and is not without risk!
For Dyspnoeic patients with oxygen saturation at rest or on exertion ≤ 90% (Corresponding to PaCo2 approx. 55 mmhg) a therapeutic trial of oxygen therapy may be reasonable, but continued use (continuous, short burst, or ambulatory) can only be justified if there is acknowledged symptomatic relief!
The role of long-term continuous o2 therapy in reducing mortality & improving quality of life for hypoxaemic (Pa O 2 ≤ 55mmHg) patients with chronic lung disease is well established.
There is only little evidence concerning the use of o2 therapy for advanced cancer patients, However, the Position statement of the Thoracic Society of Australia & New Zeland asserts that intermittent o2 therapy may be helpful! (“for the patients with intractable dyspnoea due to terminal illnesses,…who will usually have a life expectancy with less than 3 months, supplementary o2 therapy may provide symptomatic relief….”)
No evidence of symptomatic benefit in non-hypoxic (ABG - (Pa O 2 ≥ 55mmHg) patients
Role of Supplemental Oxygen therapy

Adverse effects should be discussed with patient / family
Promote anxiety – (1) Dependency on the equipment can lead to anxiety in the event of equipment failure; (2) if given whilst an in-patient, patient /family seek re- admission if not available at home; (3) Powerful Placebo & anxiety when the Placebo effect fails
Due to the dryness of gas it can cause: (1) nasal dryness /crusting / bleeding; (2) Upper airway irritation leads to increased cough symptom
Trauma due to tubing: (1) Pressure ulcers around ears / nasal trauma (2) Trips / falls
Noisy Apparatus: (1) Contributes to insomnia symptom (2) Negative impact on quality of life
Reduce mobility: Confined to the radius of O2 tubing
Apparatus discourages intimacy
Reinforces sick role /loss of independence
Rarely, may increase CO 2 retention: Somnolence / headache /death
Adverse Effects of Supplemental Oxygen therapy

Dexamethasone has assumed the position of steroid of choice in palliative care due to its high potency, low mineralocortcoid activity & convenient formulation (Tablets / suspension / injections)
For acute dyspnoea in the setting of malignancy (e.g.: SVCO or presence of Stridor) IV Dexamethasone 16mg via syringe driver over 30 mins daily may help the symptom burden.
Consider trial of dexamethasone 8mg daily (single morning dose) in the setting of chronic onset dyspnoea
Pressure from primary or metastatic tumour on lung structures
Infiltration of Lymphangitis Carcinomatosis
Use of Steroids in Dyspnoea
Contra-indications & Cautions – Proximal Myopathy; agitation; Diabetics with poor glycaemic control; insomnia patients

Nebulised sodium chloride 0.9% may help as a mucolytic. Consider a trial for 24 hours.
Dose: 5ml via nebuliser 4 hourly
A trial of nebulised bronchodilator should be considered if clinical evidence of airways spasm / constriction.
Drugs: Salbutamol / Ipratropium Bromide / Terbutaline may be
useful if patients are troubled by tremors
Doses: Salbutamol 2.5-5mg ; Ipratropium Bromide 500mcg; Terbutaline 5-10mg
Role of Nebulised medications in palliative care Patients
Co-existing depression should be actively managed.
Even in the absence of ‘clinical depression’, there is evidence of benefit
from SSRI’s in reducing sensation of breathlessness [It is postulated that serotonin may modulate central control of respiration]
Management of Co-existent issues

Common co-existing issues of dyspnoea & Specific Treatment
Anaemia Treatment : Blood Transfusion
Heart Failure Treatment : Diuretics
Infection Treatment : Antibiotics
Pulmonary Embolism Treatment : Oxygen + Anti-coagulation
Bronchospasm Treatment : Bronchodilators + Corticosteroids
Ascites Treatment : Paracentesis + Diuretics
Pleural Effusion Treatment : Pleural Tap + Pleurodesis
Lung Tumour Treatment : Radiotherapy
Lymphangitis Carcinomatosis Diagnosis: Only by CXR & even this may not be diagnostic. Suspect when severe SOB at rest /on exertion & wide spread fine Crepitations Treatment : Corticosteroids + Diuretics + Bronchodilators
Large Airway Obstruction Diagnosis: Clinically by SOB & Inspiratory Stridor
Treatment : Radiotherapy + Stent + Laser Treatment +Brachytheraphy + Corticosteroids
Radiation-induced Pulmonary Fibrosis Corticosteroids
SVC Obstruction Diagnosis: Clinically by dilated upper chest / neck veins + Swollen face/neck/arms
Treatment : Corticosteroids + Radiotherapy

Why secretions are more pronounced in terminally ill patients?
Medications: Glycopyrronium / Hyoscine
Dose ?
Commonly used drug in palliative care services is Glycopyrronium inj
0.2-0.4mg sc stats (max of 2mg/24hr) or subcutaneous S/driver D start with 600mcg – 1.2 mg/24hr
Hyoscine: Buscopan 20mg sc stats (max 240mg/24h)
or subcutaneous S/Driver start with 60 to 120mg /24 hr
End of Life care Dyspnoea can be contributed by Excessive secretions!

Any reversible cause & appropriate Rx Non-pharmacological Measures: - Position – Sitting upright rather than lying - Cool air from fan or open window - Diversion therapy - massage, aromatherapy or other relaxation methods Low dose regular opioid Anxiolytics – Short acting ‘pams’ are helpful (Oxazepam 7.5-15mg or Lorazepam 0.5 -1mg SL) These drugs can break SOB Anxiety cycle Oxygen therapy No clinical evidence advanced cancer (if the patient is hypoxic SaO2 < 90% Trial of Oxygen)
Consider a trial of bronchodilators MDT Approach (Feeling ‘safe’/open-up Reduce anxiety levels Less SOB)
Take Home Message – Management Guidelines


Tasmanian Health care Organisation: Care Management guidelines: Breathlessness
Therapeutic guidelines: Palliative Care (2010). Version -3
Merseyside and cheshire Palliative care network: Standards & Guidelines. Third Edition (2006)
Nishino, T. (2011). Dyspnoea: underlying mechanisms and treatment. Br. J. Anaes. (2011) 106 (4): 463-474.
Burki, NK, and Lee LY (2010). Mechanisms of Dyspnoea. CHEST 2010; 138(5):1196–1201
Travers, J et al. (2007) Mechanisms of exertional dyspnoea in patients with cancer. J Appl Physiol 104:57-66, 2008. First published 1 November 2007
Manning, HL and Mahler, DA (2001). Pathophysiology of dyspnoea. Monaldi Arch Chest Dis 2001; 56: 4, 325–330
Torres M, Moayedi S (May 2007). "Evaluation of the acutely dyspnoeic elderly patient". Clin. Geriatr. Med. 23 (2): 307–25
Harrison's Principles of Internal Medicine (Kasper DL, Fauci AS, Longo DL, et al (eds)) (16th ed.). New York: McGraw-Hill
Johnson MA, Woodcock AA, Geddes DM. Dihydrocodeine for breathlessness in pink puffers. Br J Med 1983; 286: 675–7
Rice KL, Kronenberg RS, Hidemark LL, Niewoehoer D. Effects of chronic administration of codeine and promethazine on breathlessness and exercise tolerance in patients with chronic air flow limitation. Br J Dis Chest 1987; 81: 287–92
References

Light RW, Muro JR, Sato RI, et al. Effects of oral morphine on breathlessness and exercise tolerance in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis 1989; 139:129–33
Bruera E, MacEachern T, Ripamonti C, Hanson SJ. Subcutaneous morphine for dyspnoea in cancer patients. Ann Intern Med 1993; 119: 906–7
Mazzocato C, Buclin T, Rapin CH. The effects of morphine on dyspnoea and ventilatory function in elderly patients with advanced cancer: a randomized double-blind controlled trial. Ann Oncol 1999; 10: 1511–4
Williams SG, Wright DJ, Marshall P, et al. Safety and potential benefits of low dose diamorphine during exercise in patients with chronic heart failure. Heart 2003; 89: 1085–6
Bellofiore S, DiMaria GU, Priviteria S, et al. Endogenous opioids modulate the increase in ventilatory output and dyspnoea during severe acute bronchoconstriction. Am Rev Respir Dis 1990; 142: 812–6
Taguchi N, Ishikawa T, Sato J, Nishino T. Effects of induced metabolic alkalosis on perception of dyspnoea during flowresistive loading. J Pain Symptom Manage 1996; 12: 11–7
Nishino T, Iiyori N, Isono S, et al. THAM improves an experimentally-induced severe dyspnoea. J Pain Symptom Manage 2009; 37: 212–9
Woodcock AA, Gros ER, Geddes DM. Drug treatment of breathlessness: contrasting effects of diazepam and promethazine in pink puffers. Br Med J 1981; 283: 343–6
O’Neill PA, Morton PB, Stark RD. Chlorpromazine—a specific effect on breathlessness? Br J Clin Pharmacol 1985; 19: 793–7
References





























