Embed Size (px)
Citation preview

C H A P T E R 5
Palin Parent–Child InteractionWILLIE BOTTERILL AND ELAINE KELMAN
CHAPTER OUTLINEINTRODUCTION
Principles of Treatment: Parents (or KeyCaregivers) Are Involved inDirecting and Delivering Therapyin the Home
Principles of Treatment: Understandingthe Child’s Needs
Principles of Treatment: Stuttering IsDiscussed Openly
Principles of Treatment: Parents AreAlready Helping
Goals of TreatmentTHEORETICAL BASIS FOR TREATMENT
APPROACHFactors That May Contribute to the Onset of
StutteringFactors That Contribute to the
Development of Stuttering andRisk of Persistence
Factors That Contribute to the Moment ofStuttering
The Michael Palin Centre MultifactorialFramework
Assessment and TherapyProfile of VulnerabilityTherapy – Palin PCI
EMPIRICAL BASIS FOR TREATMENTPhase 1Phase 2Phase 3Phase 4Phase 5Summary
PRACTICAL REQUIREMENTSTrainingAssessment SkillsTherapeutic SkillsTechnical Equipment and Skills
AccommodationTime Requirements
KEY COMPONENTSOverviewMultifactorial AssessmentStage 1: Within Clinic SessionsStage 2: The Home-Based Consolidation
PeriodStage 3: The Review Session and Clinical
Decision MakingAdvantages of Palin PCISummary
ASSESSMENT METHODS TO SUPPORTONGOING DECISION MAKINGInitial Assessment to Support Decision
Making Regarding InterventionOngoing Assessment to Monitor Treatment
EffectivenessTAILORING THE TREATMENT TO THE
INDIVIDUAL CLIENTAPPLICATION TO AN INDIVIDUAL CHILD
Session 1Session 2Session 3Session 4Session 5Session 6
CASE STUDYCase Study Questions
FUTURE DIRECTIONSTrainingApplication of Palin PCI to Other DisordersResearchSummary
CHAPTER SUMMARYCHAPTER REVIEW QUESTIONSSUGGESTED READINGS
KEY TERMS
Palin Parent–Child Interaction: therapy pro-gram using video feedback to help parentsdevelop styles of interaction to facilitate theirchild’s fluency.
Multifactorial perspective: a number of differ-ent factors may be relevant in the onset, de-velopment, and persistence of a stutteringproblem and are therefore also considered inits treatment.
63

Special Time: 5-minute, play-based sessionsfor the parent and child to practice specificfluency-facilitating targets in the home.
INTRODUCTION
Palin Parent–Child Interaction (Palin PCI)(Kelman & Nicholas, 2008) is a therapy programconducted at the Michael Palin Centre (PalinCentre) for children up to 7 years of age that usesplay-based sessions with parent–child pairs, videofeedback, and facilitated discussions to helpparents support and increase their child’s naturalfluency. It is often the first and only interventionfor young children at the Palin Centre. It differsfrom other approaches to modifying parent–childinteraction in the following ways:
• It is a facilitative rather than an instructiveapproach: parents’ instinctive expertise is eli-cited, reinforced, and developed.
• Parents use video feedback to set their owntargets and reinforce progress.
There are some children who also benefitfrom other interventions such as language ther-apy or speech sound work, as indicated, oncePalin PCI has been completed.
PRINCIPLES OF TREATMENT:UNDERSTANDING THECHILD’S NEEDSPalin PCI is based on the therapist’s andparents’ shared understanding of the child’s par-ticular profile of speech motor and linguisticstrengths and vulnerabilities. These are identi-fied during the assessment and provide the con-text for exploring what the child needs in orderto plan, organize, and deliver a message fluently.
PRINCIPLES OF TREATMENT:PARENTS ARE ALREADY HELPINGA key principle is that parents of children whostutter are already interacting with their chil-dren in ways that support natural fluency. Theyoung children seen at the Palin Centre are flu-ent much more often than they stutter. Parentsseek help because they are worried about the de-velopment of persistent stuttering, and they feelill equipped to help their child. Palin PCI pro-vides the means by which parents becomeincreasingly knowledgeable about their child’s
communication skills and helps them to identifywhat they do that supports the development offluency. Palin PCI aims to empower and rein-force parents’ ability to interact in ways thatmatch the child’s fluency needs and focus onincreasing these interactions in the homeenvironment.
PRINCIPLES OF TREATMENT:PARENTS (OR KEY CAREGIVERS)ARE INVOLVED IN DIRECTINGAND DELIVERING THERAPYIN THE HOMEPalin PCI is based on the principle that parentinvolvement in therapy is essential to reducestuttering in the young child. Where appropri-ate, both parents attend the initial assessmentand all therapy sessions, carry out homeworktasks with their child, and provide feedback onprogress. Central to this approach is the estab-lishment of a collaborative therapeutic relation-ship in which the parents’ and the therapist’sknowledge and perceptions are shared and inwhich parents are encouraged to make theirown observations, draw their own conclusions,set their own goals, and reflect on their progresseach week. Within this relationship, the thera-pist’s role is to facilitate and affirm, rather thaninstruct, advise, or model.
PRINCIPLES OF TREATMENT:STUTTERING IS DISCUSSED OPENLYParents are encouraged to acknowledge stutter-ing openly; they are helped to identify their fearsabout acknowledging stuttering and are encour-aged to use age-appropriate, child-centered ter-minology. Normalizing the problem from thebeginning can substantially reduce the anxietyand fear associated with stuttering for parentsand for children. Although anxiety does notcause stuttering, stuttering causes anxiety.
GOALS OF TREATMENTThe primary goal of Palin PCI is to establish afoundation of parental understanding, knowl-edge, skill, and confidence in managing stutter-ing, which will support and augment the child’sfluency during each stage of therapy. Anothergoal is to reduce the family’s anxiety about stut-tering and ultimately reduce the instances of stut-tering in young children to within normal limits.
64 Treatment of Stuttering

THEORETICAL BASIS FORTREATMENT APPROACH
It is our view that any therapeutic approach toearly stuttering must not only account for themany factors that may be contributing to theonset and development of stuttering in the indi-vidual child, but also acknowledge and harnessthe strengths and resources that the child andfamily bring to the clinical setting. This under-standing of the nature of each child’s difficultiesas well as their strengths informs the therapyprocess from the beginning.
A multifactorial perspective (Smith &Kelly, 1997; Starkweather & Gottwald, 1990;Wall & Meyers, 1995) is supported by growingevidence that there are factors that may accountfor the child’s underlying vulnerability to stut-tering and its onset; factors that contribute tothe development of the problem and, in somecases, its persistence; and factors that contributeto the moment of stuttering.
FACTORS THAT MAY CONTRIBUTETO THE ONSET OF STUTTERINGGeneticsThe underlying vulnerabilities to stuttering arehighly complex and continue to be the focus ofextensive research. It seems incontrovertiblethat genetic factors play a role in the onset ofstuttering, and linkage studies are getting closerto finding the specific genes that predisposechildren to the disorder (Cox et al., 2000;Drayna, 1997; Shugart et al., 2004; Suresh et al.,2006). However, it is important to note thatgenes alone do not produce or determine behav-ior, especially one as complex and variable asstuttering; they only increase the probabilitythat it will occur (Starkweather, 2002). It isacknowledged that a wide range of factors influ-ences the extent to which a behavior trait suchas stuttering finds expression (Starkweather,2002). The complexity of the genetic predispo-sition was also discussed by Ambrose, Cox, andYairi (1997), who suggested that an otherfactor—such as rapid rate of speech, low toler-ance for frustration, slow reaction time, wordretrieval or sentence formulation skills, chronicor excessive muscle tension, or any combinationof these—may be the inherited variable thatresults in stuttered speech.
In addition to whether or not stuttering islikely to occur, Ambrose, Cox, and Yairi (1997)and Suresh et al. (2006) both report data thatsuggest the predisposition to recover or persistin stuttering is also inherited.
Neurophysiologic FactorsWhile the nature of the genetic transmission isstill being investigated, parallel areas of researchsuggest that the onset of stuttering may berelated to some underlying structural and orfunctional differences in the brain (Foundaset al., 2000; Fox et al., 2000; Sommer et al., 2002).
Findings from brain imaging and brainfunction studies have not yet been replicated inchildren, so it is not possible to determinewhether any identified differences are responsi-ble for the onset of stuttering or are a responseto it. However, it has been suggested that anunderlying neurologic dysfunction may bedisrupting the complex two-way interactionbetween language planning and motor process-ing in children who stutter (Caruso, Max, &McClowry, 1999; Ingham & Cordes, 1998;Peters, Hulstijn, & Van Lieshout, 2000).
Speech Motor SkillsStuttering presents as a breakdown in speechmotor control, and as a result, there has beenconsiderable research related to this area overthe years, particularly in adults. The results aresometimes conflicting but suggest that there aredifferences in the speech production processesof adults who stutter compared with adults whoare typically fluent. Although there has been lessresearch on speech motor skills in children thanin adults, there are indications of some subtledeficits in children (see review by Conture,1991). In particular, studies have suggested thatchildren who stutter have reduced oromotorskills (Riley & Riley, 1980), slower vocal and man-ual response times (Bishop, Williams, & Cooper,1991), and difficulty stabilizing and controllinglaryngeal movements, even during perceptuallyfluent speech (Conture, Rothenberg, & Molitor,1986).
The Communication Environment:Interaction StylesConsiderable research has been carried outconcerning the role that the communication
65Chapter 5 • Palin Parent–Child Interaction

environment and interaction styles may have inthe onset of stuttering. The results suggest thatthere is no evidence that the interaction styles ofparents of children who stutter and childrenwho do not stutter are different (for a review,see Nippold & Rudzinski, 1995) or have arole in the onset of stuttering. Miles and Bern-stein Ratner (2001), however, suggested thatalthough the input of parents of children whostutter is parallel to that of parents of childrenwho do not stutter, children who stutter mighthave more difficulties assimilating or respond-ing to this input as a result of their underlyinglinguistic and or temperamental vulnerabilities.Perhaps the underlying vulnerabilities that pre-dispose children to stutter also make it more dif-ficult for them to be fluent in the context oftypical adult-child interactions.
SummaryMany researchers agree that, for most children,the onset of stuttering will be shown to have aphysiologic base that affects the delicate andcomplex balance of the child’s developing lin-guistic and motor skills.
FACTORS THAT CONTRIBUTETO THE DEVELOPMENT OFSTUTTERING AND RISK OFPERSISTENCEThere is considerable agreement that it is theinterplay between the child’s underlying vulner-abilities and his or her temperament and linguis-tic and social environment that contributes tothe development of stuttering and the risk ofpersistence (Yairi & Ambrose, 2005).
Linguistic FactorsThus far, research suggests that there are no dif-ferences in the overall linguistic abilities of chil-dren who stutter (see Kloth et al., 1999; Watkins& Yairi, 1997; and Yairi et al., 2001 for a discus-sion). However, in a recent study, Anderson,Pellowski, and Conture (2005) assessed the ex-pressive and receptive language and phonologicskills of children who stutter and children who donot stutter and looked at the dissociations or mis-matches within or between components of theseskills. They found that children who stutter arethree times more likely to exhibit these mis-matches than their fluent peers. The fact that
there were children who exhibited dissociationsbut who did not stutter and there were childrenwho stuttered but who did not exhibit dissocia-tions means that linguistic dissociations on theirown cannot account for stuttering onset but maybe relevant in combination with other factors orin relation to persistence.
The role of phonologic skills has also been wellresearched, with high proportions of childrenwho stutter also having speech sound impair-ments (Yaruss, Lasalle, & Conture, 1998). Inaddition, an association has been found betweenreduced phonologic skills and persistence of stut-tering (Paden, Yairi, & Ambrose, 1999).
GenderResearch seems to indicate that more boys thangirls persist in stuttering (Yairi & Ambrose,2005). The ratio of boys to girls who stutter isreported to be as low as 1:1 (Yairi, 1983) close toonset and increases with age to about 6:1(Bloodstein, 1995).
Time since OnsetFor the majority of children, recovery occurswithin the first 12 months (Yairi & Ambrose,1992; Yairi et al., 1996) to 18 months (Johann-sen, 2000) after stuttering begins. Althoughsome children will still achieve fluency after this(Yairi & Ambrose, 1999), the probability of re-covery decreases with age (Seider, Gladstien, &Kidd, 1983) and length of time stuttering (Yairiet al., 1996). These studies also identified thatchildren who persist in stuttering demonstrate arelatively stable level of stuttering over time. Incontrast, children who recover show a markedreduction in the amount of stuttering during thefirst year after onset, and this pattern of improve-ment continues over time.
Psychological-Emotional FactorsSignificant research continues to investigate therole of psychological factors, particularly tem-perament, in contributing to the developmentof persistent stuttering. Researchers such asConture (2001) and Guitar (2006) suggest thattemperament traits, such as sensitivity, inhibi-tion, and reactivity, among others, may maintainor exacerbate stuttering. The research suggeststhat children who stutter are more sensitive andinhibited (Anderson et al., 2003; Embrechts
66 Treatment of Stuttering

et al., 2000). It is suggested that children whostutter may be intolerant of disruptions in theirspeech and react in ways that exacerbate theproblem rather than ameliorate it. Recentresearch findings by Conture’s research team atVanderbilt University have suggested that ‘‘therelatively greater emotional reactivity experi-enced by preschool children who stutter, to-gether with their relative inability to flexiblycontrol their attention and regulate the emo-tions they experience, may contribute to thedifficulties these children have establishing rea-sonably fluent speech and language’’ (Karrass etal., 2006, p. 402).
Within the clinical environment at the PalinCentre, parents frequently describe their childwho stutters as being ‘‘highly sensitive,’’ ‘‘easilyupset,’’ and ‘‘a bit of a worrier.’’ In addition,parents say their children who stutter seem to‘‘set themselves high standards,’’ ‘‘be perfec-tionists,’’ and ‘‘like to get things right’’ and areoften ‘‘anxious to please.’’ It has also been pro-posed that a child’s temperament may influencehow he or she responds to different parentalinteraction styles (Felsenfeld, 1997), and there isa growing body of research that seems to sup-port the idea that the temperament of the childhas an important role to play in the developmentand possibly the persistence of stuttering.Therefore, temperament may be an importantvariable to consider in therapy.
The Communication Environment:Interaction StylesAlthough there is no evidence that parents’interaction styles have a role in the onset of stut-tering, Kloth et al. (1998) provide evidence fromtheir longitudinal study that mothers madechanges in their interactions in response to thestuttering of their children. This study showedthat after the onset of stuttering in their chil-dren, mothers tended to be more intervening,take more turns, use shorter pauses, make morerequests for information, and use more affir-matives than they had used before onset. Rom-mel (2000) was also looking at factors that affectthe development of stuttering and found that themore complex the mother’s language and thegreater the discrepancy between mother andchild linguistic variables were, the higher thechances of persistence.
SummaryAnderson et al. (2005) concur red with Hall(2004) by suggesting that ‘‘it is the child’sattempt to reconcile or manage dissociations inspeech and language that contributes to disrup-tions in their speech and language production,which in combination with a genetic predisposi-tion towards stuttering or, perhaps a tempera-mental disposition that is relatively intolerant ofany such disruptions, that results in the emer-gence of persistent stuttering’’ (p. 242).
FACTORS THAT CONTRIBUTE TOTHE MOMENT OF STUTTERINGLinguistic FactorsThere are a number of research studies thathave looked more closely at the relationshipbetween length and complexity of utterancesand stuttering frequency. These have shownthat children are more likely to stutter whenusing longer, more complex sentences (Logan& Conture, 1995; 1997; Logan & LaSalle, 1999;Melnick & Conture, 2000). However, Yaruss(1999) pointed out that this was true of onlysome children in his study.
Other studies have looked at factors that influ-ence the location of stuttering and demonstratedthat it tends to occur at the beginning of an utter-ance (Howell & Au-Yeung, 1995), on functionrather than content words (Howell, Au-Yeung, &Sackin, 1999), and on longer words (Rommel,2000).
The Communication Environment:Interaction StylesParents and their children live in a socially inter-active environment. Children’s social, emo-tional, and behavioral development is influencedby the way their parents ‘‘parent.’’ Furthermore,the way in which children respond and developaffects their parents. It is a dynamic, constantlyevolving relationship that is unique to each childand family.
Many early intervention approaches havebeen based on helping parents make changes inthe communication environment of the child inthe belief that this will reduce the amount ofstuttering. There is at least some evidence thatparental interaction styles can be modified(Nicholas, Millard, & Cook, 2003), and stutter-ing has been shown to decrease when parents
67Chapter 5 • Palin Parent–Child Interaction

slow down their rate of speech (Guitar et al.,1992), when they increase pause time andresponse latency time (Newman & Smit, 1989),and when they put in place structured turn tak-ing (Winslow & Guitar, 1994). Interestingly,closer inspection of the results indicates that theimpact of the changes made by parents seems tohave been somewhat idiosyncratic (Zebrowskiet al., 1996), with the frequency of stutteringreducing in some children but not in others.
Not only is there some evidence that modifi-cations in a parent’s interaction style canreduce the frequency of stuttering, but there isalso evidence that stuttering influences parentinteraction style (Meyers & Freeman, 1985a;1985b; Zenner et al., 1978). These studiesshowed that mothers of both children who stut-ter and children who do not stutter use a fasterrate of speech (Meyers & Freeman, 1985b),interrupt more frequently (Meyers & Freeman,1985a), and are more anxious (Zenner et al.,1978) when interacting with children who stut-ter compared with children who do not stutter.Several authors emphasized the important roleplayed by the family and family dynamics in thetherapy process (Cook & Botterill, 2005; Kelly& Conture, 1992; Manning, 2001; Wall &Myers, 1995). Shapiro (1999) concluded, ‘‘stut-tering, and other communication disordersexist and must be addressed within a familycontext’’ (p. 125).
SummaryThere are important linguistic considerationsand interaction styles that influence the momentof stuttering during communication. These areunique to each child and family and are impor-tant to take into account when planning anddelivering therapy.
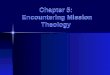
THE MICHAEL PALIN CENTREMULTIFACTORIAL FRAMEWORKThe multifactorial framework depicted inFigure 5.1 interprets the previously outlinedresearch as suggesting that predisposing physio-logic and linguistic factors may be significant inthe onset and development of stuttering. Fur-thermore, the interaction of these factors withemotional and environmental aspects is thoughtto contribute to the severity and persistence ofthe disorder and the impact it has on a child and
the family. For each child, there is a uniquecombination of these factors that contributes tothe onset and subsequent development of stut-tering toward either recovery or persistence.
ASSESSMENT AND THERAPYBecause of the relationships described earlier,it is essential to conduct a comprehensive,multifactorial assessment to identify the factorsthat are pertinent to each child’s difficulties.Assessment of the child’s speech, language, andfluency skills, as well as information from struc-tured interviews with children and their parentsor caregivers, provides the basis for identifyingchildren at risk of persistence. It also providesthe information necessary to make recommen-dations and tailor therapy to meet the needs ofindividual children.
PROFILE OF VULNERABILITYIt is not yet possible to predict precisely the levelof risk or the ‘‘weighting’’ of those factors thatmake one child more vulnerable than another.Furthermore, it is still not possible to predictwith any accuracy what the eventual outcome isfor any individual child, either with or withouttherapy (Bernstein Ratner, 1997). However,research has been able to isolate factors that aremost likely to help identify children who are atsome risk of stuttering (Kloth et al., 1999; Yairi& Ambrose, 1999). On the basis of currentresearch and clinical expertise, therapists at thePalin Centre select children for therapy accord-ing to their vulnerability to persistence. This isbased on information about family history, timesince onset, the changes in stuttering sinceonset, and the child’s or parents’ concern aboutthe problem. Children who are involved in theresearch program are only selected if they havebeen stuttering for more than 12 months. Rou-tinely, treatment is offered to children who havebeen stuttering for less time if the levels of con-cern are high.
THERAPY – PALIN PCIPalin PCI is based on the premise that theunderlying vulnerabilities that predispose chil-dren to stuttering may also make it more diffi-cult for them to be fluent in the context oftypical adult-child interactions.
68 Treatment of Stuttering

The main focus of Palin PCI is the child, hisor her profile of skills, and facilitating furtherdevelopment of the naturally occurring fluencywithin the environment. It also aims to buildon parents’ or caregivers’ knowledge and confi-dence in what helps and enhances existingbehaviors that support fluency.
The intention of therapy is to establish strat-egies that support the child’s natural fluency andminimize the impact of the stuttering on boththe child and the family through:
1. Interaction strategies: These may include, forexample, changes in rate, length, and complex-ity of utterances; turn taking; use of pausing;comments; and following the child’s lead.
2. Family strategies: These can include strat-egies such as managing anxiety about stutter-ing, coping with highly sensitive children,confidence building, behavior management,and turn taking.
3. Child strategies: These are included for somechildren as appropriate. They may includedirect speech modification, fluency-enhancingstrategies, language therapy, or speech soundtherapy.
EMPIRICAL BASIS FORTREATMENT
The previous section has provided the rationalefor the Palin Centre conceptualization of stut-tering and some of the evidence that supportsthis view.
Palin PCI was developed at the Palin Centrein the early 1980s (Rustin, Botterill, & Kelman,1996). Since then, it has drawn on the experienceof expert clinicians and the families that they haveworked with, and it has been influenced andshaped by the work of academic researchers andrespected authorities in the field.
Evidence-based practice is now an essentialcomponent of ethical working within the fieldof speech and language therapy. Sackett et al.(2000) emphasize the multidimensional nature ofevidence-based practice and describe it as the‘‘integration of best research evidence with clini-cal expertise and patient values’’ (p. 1). The clini-cal work at the Palin Centre is informed by a widerange of theoretical perspectives from the field ofpsychology as well as speech and language ther-apy, providing a broad evidence base to support
e.g., Family history Motor Co-ordination
e.g.,Speech Rate
e.g., Delayed language Advanced language Utterance length
e.g., Time pressurese.g., Health worries
e.g.,Parents’ anxietyTeasing
e.g., Sensitive temperamente.g., Linguistic environment
Physiological Factors
Stuttering
Linguistic Factors
Psychological/EmotionalFactors
Environment Factors
Figure 5.1. The Palin Centre Multi-factorial Framework.
69Chapter 5 • Palin Parent–Child Interaction

our practices. In addition, the Palin Centre iscommitted to continuing professional develop-ment, updating the Centre’s research knowledge,and maintaining an active clinical research pro-gram that consistently seeks the opinions of thechildren and parents who use the services.
This section provides a description of theclinical research framework that the PalinCentre is using to explore the effectiveness ofPalin PCI. The framework is based on themodel proposed by Robey and Schultz (1998),which Pring (2005, p. 245) applied to stutteringresearch. The model advocates a progressionfrom treatment efficacy research, where therapyis investigated under optimal conditions, totreatment effectiveness research, where therapyis investigated under clinical conditions. As theprocess develops, the factors that influence out-come are isolated and investigated. There arefive phases of research described in a logicalseries but that are not discrete.
PHASE 1In phase 1, clinical reports, small group studies,and single-case studies are used to demonstratepotential therapeutic effects. Clinical reportsdetailing the positive impact of Palin PCI forindividual clients, such as the case reported inthis chapter, have been available for a number ofyears (Rustin, Botterill, & Kelman, 1996). Mat-thews, Williams, and Pring (1997) presented asingle case study reporting stuttering frequencydata relating to Palin PCI. In this study, the pro-gress of a 4-year-old boy was monitored for6 weeks before therapy, 6 weeks during therapy,and 6 weeks after therapy. The percentage ofwords stuttered was calculated from speech sam-ples obtained while the child played with eachparent in the clinic for a period of 20 minutesonce a week. The therapy resulted in a signifi-cant reduction in the frequency of the child’sstuttering during therapy that was maintainedduring the posttherapy phase.
The design and methods employed by Mat-thews, Williams, and Pring (1997) were adaptedand improved by Millard, Nicholas, and Cook(2008) to include increased participant numbers,nonclinic measures, and long-term follow-updata. Millard, Nicholas, and Cook used a single-subject methodology to investigate fluency de-velopment in six children, less than 5 years of
age, who had been stuttering in excess of 12months. Stuttering frequency measures wereobtained from video recordings of the childplaying at home with each parent. From theserecordings, stuttering frequency data wereobtained weekly during a 6-week pretherapybaseline phase, a 6-week clinic therapy phase, a6-week home-based therapy phase, and once amonth during a 1-year posttherapy follow-upphase. Cusum analyses were conducted on eachparticipant’s stuttering frequency data to deter-mine whether there was a systematic change inthe data that was outside the range of variabilityof stuttering in the baseline phase and that couldnot be accounted for by chance (Montgomery,1997). The analyses demonstrated that four ofthe six children significantly reduced the fre-quency of their stuttering with both parents bythe end of the consolidation phase. Therapy forthese four children focused on the developmentof interaction and management strategies only.One child reduced his stuttering with one par-ent, while the remaining child significantlyreduced her stuttering by the end of the follow-up period. Both of these children went on toreceive direct therapy input during the 1-yearposttherapy follow-up phase.
There are a number of advantages to using sin-gle-subject designs with children who stutter.The use of repeated measures prior to the intro-duction of therapy allows the detection of anysigns of pretreatment recovery. It also enables ob-servation of each child’s individual variability andprovides a more representative picture of a child’soverall fluency skills (Ingham & Riley, 1998). Thechild’s progress can then be measured against hisor her normal variability in fluency, which elimi-nates the problem of withholding therapy. It isalso argued that it is a more clinically relevantdesign, particularly for heterogeneous disorders,because it can be used within the context of regu-lar clinical work (Pring, 2005).
PHASE 2In phase 2 research, studies are designed toshow how the therapy works, which clients aresuitable for a particular program, the amount oftherapy needed, and the method of delivery.
Consideration of the information from phase1 clinical reports and single-subject data, alongwith evidence from other researchers in the
70 Treatment of Stuttering

field, led to the development of hypothesesabout why and how Palin PCI might work. Ex-ploration of the mechanisms of change wouldconstitute phase 2 in the research framework.
Because Palin PCI places a strong emphasison modifications to parent interaction style, itmight be assumed that this would change as partof the therapy process. Using the recordingscollected as part of the Millard, Nicholas, andCook (2008) study, preliminary data reportedby Nicholas, Millard, and Cook (2003) sug-gested that parents are able to make changesduring Palin PCI and that these changes can bemaintained over time. Nicholas et al. found thatfathers significantly reduced the proportion ofutterances that were requests for informationand reduced the length of their turn, whereasmothers significantly reduced the number oftheir utterances that were instructions. There isevidence, therefore, that this line of inquiryshould be extended in a larger study involvingthe analysis of longer term data and increasedsubject numbers.
Millard, Edwards, and Cook (2009) observed arelative reduction in the expressive languagescores of five children who began therapy withabove-average scores. Each of these children didnot maintain the above-average scores 6 monthsafter therapy but achieved scores that were withinthe normal range. Since their receptive skillsmaintained the advanced developmental trajec-tory, Millard et al. concluded that the observedrelative reduction could not be explained by a lin-guistic environment that was inadequate to main-tain language growth, as has been proposed in thepast (Miles & Bernstein Ratner, 2001). They sug-gested that the data adds further support to thepossibility of a fluency-language trade-off (Miles& Bernstein Ratner, 2001).
Phase 2 also seeks to identify the appropriateoutcome measures for use in effectiveness studies.We consider that outcome measures shouldreflect not only stuttering frequency, but also themultidimensional nature of stuttering, the impactthat it may have on both children and parents,and the expectations and needs of the client.
Frequency of stuttering represented as apercentage of syllables stuttered is usuallycited as the only evidence of success in therapyfor young children who stutter. Although thisis clearly an essential measure, it provides a
somewhat one-dimensional perspective of stut-tering behavior. It is well known that stutteringin young children varies considerably from day today and situation to situation, and it is commonfor children to be much more fluent in clinic thanat home, or vice versa. Obtaining a single measureof stuttering frequency from one speech sample isunlikely to be representative of a child’s overallfluency. Although use of multiple measures andcontexts partly addresses this issue (Ingham &Riley, 1998), other important aspects of the prob-lem are not reflected. The aims of Palin PCI aremuch broader than singularly reducing stutteringfrequency and include developing parents’ knowl-edge about stuttering, reducing their worriesabout their child’s speech, and increasing theirknowledge and confidence about strategies formanaging their child’s stuttering more effectively.Because parents/caregivers are an integral part ofthe therapy process, it is essential that they areinvolved in providing additional clinical outcomedata. However, there are few assessment toolsthat adequately evaluate these broader issues.
Parents’ Ratings of OutcomeIn an attempt to address the need for parentalinput, Millard (2002) conducted a qualitativestudy to find out what parents consider to be themost important outcomes in therapy and to de-velop an outcome measurement tool for parentswho receive Palin PCI. The design of the studyfollowed the principles of the Delphi approach.This is a structured methodology that aims toobtain a group’s opinion or judgment on a topic(Goodman, 1987) and to arrive at consensusthrough a specified procedure (Mosley & Mead,2001). In this instance, the ‘‘group’’ consisted ofparents who had attended the Palin Centre fortherapy with their children during the previousyear. The resulting rating scales contained awide range of themes that reflected the broadnature of the therapy they had received. In addi-tion to reductions in stuttering frequency andseverity, the parents considered reductions inthe child’s anxiety, frustration, and concernabout speech and increases in the child’s confi-dence in speaking and turn-taking skills to beimportant indicators of improvement. Theparents also considered positive changes in theirown level of concern and confidence in manag-ing the stuttering effectively, along with the
71Chapter 5 • Palin Parent–Child Interaction

impact on the family as a whole, to be importantoutcomes of the therapy program. The resultingquestionnaire consists of a series of visual analogscales that allows a numerical value to be obtainedbefore therapy and at intervals throughout thetherapy process so that change can be evaluated.This rating scale is used routinely at the PalinCentre, in conjunction with fluency and languagemeasures and is available in Millard, Edwards, andCook (2009).
PHASE 3Phase 3 of the research framework relates tolarge-scale efficacy research. Although random-ized controlled trials (RCTs) are generallyviewed as the ‘‘gold standard’’ methodology fortreatment efficacy research (Jones et al., 2001),they are not without their limitations.
The strength of large-scale RCTs is that theresults can be generalized to a wider populationthan the participants studied. The limitation isthat group studies do not capture individualresponses to therapy and group findings cannotbe used to predict how an individual willrespond to a given therapy. The need for largesubject numbers can restrict the range of de-pendent variables that can be monitored, whichcould result in potentially informative findingsor new discoveries being missed (Schwartz &Conture, 1988; Watkins & Yairi, 1997). On apractical level, the large subject numbers thatare required to account for the heterogeneity ofstuttering and individuality of therapy have sig-nificant implications for recruitment andresources. There are also ethical considerationsin withholding treatment from a ‘‘no treatment’’control group and methodologic limitationsin substituting a best practice control group(Pring, 2005). In our attempts to conduct anRCT to investigate Palin PCI with young chil-dren who are at risk of persistent stuttering, wehave encountered all of these difficulties. LikeOnslow, Andrews, and Lincoln (1994), wefound that the practical and ethical difficultiesof maintaining a no treatment control groupresulted in a design that was impractical andinappropriate and that had to be abandoned
The emphasis in single-subject studies is toincorporate controls to obtain high internal va-lidity—that is, that the findings can be justifiablyapplied to the individual studied. The external
validity of single-subject studies is low—that is,the findings cannot be generalized to the popu-lation as a whole and it is this that is importantin a phase 3 study. However, replicating find-ings across individuals helps to increase externalvalidity (Pring, 2005), and there is an argumentthat appropriately designed and well-controlledsingle-subject experimental designs that arereplicated can be considered to be strong sour-ces of evidence alongside RCTs (Kully & Lan-gevin, 2005). Because of the advantages of usingsingle-subject studies to investigate therapy withthis client group and because of the difficultiesinherent in conducting an RCT, we havedecided to continue and advance our researchprogram through the implementation of repli-cated single-subject studies.
In addition to the children reported byMillard, Nicholas, and Cook (2008), results froma further six children who received Palin PCIwere described by Millard, Edwards, and Cook(2009). Once again, stuttering frequency datawere obtained from video recordings made athome while the child played with a parent. Thesewere made once a week for 6 weeks prior to ther-apy, 6 weeks during clinic therapy, and 6 weeksduring the home-based therapy period. The fol-low-up phase took place 6 weeks prior to the6-month review appointment and again involvedonce-weekly video recordings. All six childrenshowed a reduction in stuttering by the end of thestudy, according to the cusum analyses, and wecan be confident that this was associated with thetherapy in four cases because the data reached sig-nificance in the therapy phases. None of the par-ticipants received direct therapy focusing on thedevelopment of child strategies. In addition to areduction in stuttering frequency, the parent rat-ing scales indicated that parents perceived thechild’s fluency to have improved; they felt moreknowledgeable and confident about managing thestuttering and were less worried and anxiousabout it 6 months after receiving therapy thanthey had been before.
The combined findings of both the Millard,Nicholas, and Cook (2008) and Millard, Edwards,and Cook (2009) studies indicate that Palin PCIcan be effective in reducing stuttering in youngchildren who are at risk of persistent stuttering.The results seem to indicate that approximatelytwo-thirds of children will show a reduction in
72 Treatment of Stuttering

stuttering during the clinic therapy or home-based therapy (consolidation) periods and requireonly the indirect components of Palin PCI. Thisis similar to outcomes reported by Conture andMelnick (1999). There are also indications thatstuttering may be reduced over a longer term inchildren who have received Palin PCI, althoughit is not possible within the current designs andmethods to attribute this directly to the therapy.
PHASE 4Within phase 4, researchers continue to definethose clients who benefit, and variations to treat-ment and delivery are explored. Importantly, theresearch emphasis shifts towards the investiga-tion of treatment effectiveness. Thus, havingdemonstrated that Palin PCI is effective underoptimal conditions, which include being imple-mented by speech and language therapists whoare expert in the approach within a well-resourced, specialist environment, it is necessaryto establish whether the approach is effectivewhen implemented in other settings with differ-ent subgroups of the clinical population of chil-dren who stutter. The Matthews, Williams, andPring (1997) study described earlier could beconsidered to be phase 4 research because a non-specialist clinician in a nonspecialized clinicalcontext conducted it. This single-case study wassubsequently replicated by Crichton-Smith(2002), who demonstrated a reduction of stutter-ing to within normal with a 4-year-old child whoreceived Palin PCI. Therefore, there is early evi-dence that Palin PCI can be successfully imple-mented by speech and language therapists whohave received training in Palin PCI but who arenot necessarily specialists in the approach.
PHASE 5Phase 5 research focuses on the issues of costeffectiveness, client satisfaction, and the effectof therapy on quality of life. The parent ratingscales already provide useful information relatedto these issues and are incorporated into the de-velopment of phase 2 and phase 3 research.
SUMMARYThe research at the Palin Centre has developedand advanced with increasing pace over the last5 years. The framework adopted has helped tostructure and prioritize research activities.
Careful consideration and experience with arange of methods have resulted in relevant andrealistic research designs and protocols. The evi-dence indicates that Palin PCI can be effectivewith children who stutter, and this research evi-dence is used to inform the clinical decisionsmade within the Palin Centre. However,research evidence is not the only informationconsidered. Expert experience and opinion arehighly valued, and informal feedback from clientsis regularly sought.
PRACTICAL REQUIREMENTS
TRAININGAs with all therapeutic methods that are notroutinely taught within undergraduate or post-graduate education, additional training andsupervision are necessary to ensure that PalinPCI is delivered ethically and appropriately.The Palin PCI training course is a workshopthat lasts 3 days and is designed to provide train-ees with the knowledge and skills they need tocarry out Palin PCI in their clinics. The 3-dayworkshop includes:
• Review of current literature and evidence as itapplies to this age range
• Theoretical perspective of the multifactorialnature of stuttering and implications fortherapy
• Rationale for the case history and detailedchild assessment
• Developing skills in the formal and informalmeasures of fluency, speech, language, andsocial communication skills
• Clinical decision making• Rationale and practical clinical skills for deliv-
ering Palin PCI• Clinical skills in working collaboratively with
parents
The training course is an interactive work-shop in which trainees are involved in practicaland experiential exercises; in the viewing of vid-eotapes of clinicians, parents, and children whostutter; and in role-play activities. The trainingis evaluated routinely using a standard question-naire that is filled out before and after trainingand then 6 months later. The data collated fromthese questionnaires demonstrate that traineesgain knowledge, skills, and confidence in
73Chapter 5 • Palin Parent–Child Interaction

managing stuttering and that this has resulted inpositive changes in their clinical practice (Botterill,Biggart, & Cook, 2006). Trainees are also encour-aged to telephone or email and ‘‘troubleshoot’’with the team at the Palin Centre.
A new manual (Kelman & Nicholas, 2008) hasrecently been published that provides a step-by-step guide to Palin PCI and incorporates recentresearch evidence. This manual, in conjunctionwith the practical training course described ear-lier, will equip therapists to carry out Palin PCIas it is conducted at the Palin Centre.
ASSESSMENT SKILLSClinicians are required to use formal and infor-mal assessments to measure children’s speech,language, and social skills. The ability to under-take a quantitative and qualitative analysis ofstuttering using video or audio recording equip-ment is also necessary. The clinician is alsorequired to take a case history from the parentsand then process this information together withthe rest of the assessment findings to develop acase summary, which is presented to the parentsin clear and accessible terms.
THERAPEUTIC SKILLSCentral to the Palin PCI approach is the idea ofcollaboration and partnership between the clini-cian and the parent. This involves the therapistsdrawing on their core counseling skills and lis-tening to and observing the parents carefully sothat they can facilitate the parents’ discovery ofwhat they already know and are already doing tohelp their child. In this way, the therapist elicitsand uses knowledge from the parents ratherthan imparting information, teaching, or offer-ing advice.
TECHNICAL EQUIPMENTAND SKILLSA video camera and television monitor are inte-gral to Palin PCI. A tripod is also useful. A levelof competence and confidence is required to op-erate this equipment.
ACCOMMODATIONThe therapy room will need to have a range ofplay materials appropriate to the child’s age andwith space for the child to play on the floor or at atable. The room should be sufficiently large for
video recordings to be made and viewed. A sepa-rate viewing room from which the play can beremotely video recorded can be a useful option.
ADMINISTRATIONThe following paperwork is required:
• Consent forms for treatment and videorecording
• Assessment record forms, including detailedcase history form
• Special Time instruction sheet and home-work sheet; this records the details of thishome-based task and facilitates a discussion atthe beginning of each therapy session
• Praise logs to record the specific praise thatthe parents are encouraged to give to theirchildren each day
• Treatment record forms
Parents are also encouraged to read How toTalk So Kids Will Listen and Listen So Kids WillTalk (Faber & Mazlish, 1980). This is a parent-ing book that is easily accessible and that mostparents find helpful in a variety of ways. Thechapter on dealing with feelings is especially rel-evant for parents who describe their children asvery sensitive. The chapter on praise offersparents a way of praising their children that spe-cifically describes the child’s actions and thenprovides the child with a positive attribute/adjective that describes the behavior. An exam-ple is: ‘‘Thank you for putting your clotheson the chair (description) that was very help-ful/thoughtful/responsible (attribute) of you.’’Parents are often aware of the effect confi-dence has on their child’s fluency and arepleased to notice the difference when they addthese details to the praise they already give totheir children.
TIME REQUIREMENTSPalin PCI involves more assessment time thanother approaches; however, less time is usuallyrequired in the treatment phase. The childassessment and analysis takes approximately 90minutes, and the parent interview takes an addi-tional 90 minutes. These 3 hours ensure an indi-vidually tailored approach to the child’s andfamily’s specific needs.
Treatment then involves six 1-hour therapysessions (including 5 minutes for record keeping)
74 Treatment of Stuttering

during the first 6-week phase, followed by six10-minute contacts (by telephone, letter, oremail) during the consolidation phase. A 1-hourreview session follows the consolidation period.Thus a total of 8 hours is required to deliver aprogram of Palin PCI over a course of 3 months.
Following this, the child is monitored every3 months for 1 year. Some children require fur-ther direct fluency input, which can be deliveredin up to six once-weekly therapy sessions. Chil-dren who present with concomitant speech orlanguage problems may receive further therapytargeting these specific difficulties.
KEY COMPONENTS
OVERVIEWThe main focus of the Palin PCI approach is thechild and his or her profile of skills. The aim isto facilitate natural fluency within the child’susual social environment by building on theparents’ knowledge of what helps fluency andaugmenting behaviors that are already inevidence. The approach is based on the beliefthat parents can and do influence their child’scommunication skills and confidence and that,in the case of young children, they are pivotal tothe process of change (Kelman & Nicholas,2008).
The approach is flexible and adapted accord-ing to each child’s individual and changingneeds. For most children, the goal of Palin PCIis to achieve fluency within normal limits (<3%SS) or until the parents are no longer con-cerned. For children with more complex needs,the intention is to establish family strategies thatsupport the child’s natural fluency and developthe child’s confidence. For the small proportionof children who continue to stutter despiteintervention, the approach aims to minimize theimpact of the stuttering on both the child andthe family.
During Palin PCI sessions, parents viewvideo recordings made while they are playingwith their child in the clinic. Drawing on theshared understanding of their child’s needs,parents are guided through a process of iden-tifying and augmenting those interaction andcommunication styles that they judge will pro-mote their child’s fluency. Parents are alsointroduced to ideas and strategies that build
confidence and self-esteem. In addition, whenparents raise concerns about the impact of otherissues such as tiredness and lack of routines onthe child’s fluency, these are addressed as part oftherapy.
After the multifactorial assessment, PalinPCI is implemented in three distinct stages. Thefirst stage consists of six once-weekly, clinic-based sessions that both parents (as appropriate)attend with their child. In the second stage, theConsolidation Period, parents continue toimplement Palin PCI for a further 6 weeks instructured home-based practice sessions that areclosely monitored by both parents and the ther-apist. The third stage starts with a Review Ses-sion in which further clinical decisions are madebased on progress reports from parents and for-mal reassessments in the clinic. In some cases,supplementary clinic-based therapy sessionsmay be offered for further Palin PCI, languageor phonology therapy, or direct fluency therapy,as appropriate. All children are monitored for atleast 1 year after therapy.
MULTIFACTORIAL ASSESSMENTThe multifactorial assessment comprises a thor-ough evaluation of the child’s strengths andunderlying vulnerabilities within the context ofthe family, including the child’s receptive andexpressive language, articulation, speech rate,social communication skills, and general presen-tation. Detailed case history information isgathered from both parents to identify develop-mental, familial, psychosocial, health, and per-sonality factors that they consider to beinfluencing their child’s stuttering, and theparents complete the parent rating scales.
At the end of the assessment, parents aregiven a formulation or summary of the assess-ment findings. This formulation aims to provideparents with a clear understanding of the multi-factorial nature of stuttering with particular ref-erence to the factors that are relevant to theirchild’s current difficulties. It provides the ra-tionale for the recommendations that are madeand the therapy that is considered most appro-priate for the child’s difficulties. Throughoutthe process, great emphasis is placed on devel-oping the client-clinician relationship and help-ing parents make the best use of their ownproblem-solving and management skills.
75Chapter 5 • Palin Parent–Child Interaction

STAGE 1: WITHIN CLINIC SESSIONSInitial Session: Introducing and SettingUp Palin PCIThe goal of the initial session is to establish anopen dialogue about stuttering and fluency, todevelop mutual responsibilities in the therapyprogram, to review the assessment findings andclarify any questions, to set up Special Timecontracts, and to ensure that parents have a clearunderstanding of what therapy will involve.
Video and treatment consent forms are signed,and an initial 5-minute video recording is made ofeach parent playing with their child within theclinic setting. It is important to explain that thevideo will be used as a basis for exploring ways inwhich the parents can build on and enhance theirchild’s fluency in future sessions. Parents’ initialself-consciousness about the video camera isquickly offset by their child’s naturalness and cu-riosity about new toys and activities. Between thesessions, the therapist will view the video andidentify examples of interactions that facilitatefluency. The parents will watch the video at thebeginning of the next session.
Next, parents are introduced to the conceptof Special Time. These are designated homepractice sessions with their child that continuethroughout the therapy program. They consistof a fixed 5-minute playtime that each parentcompletes individually with the child. Parentsare asked to agree to a set number of SpecialTimes per week, with a minimum of three and amaximum of five. During the week after the firstsession, parents establish the routine of SpecialTimes for the agreed number of sessions.
The aim of Special Time is to provideparents with a designated time to practiceimplementing an interaction target in a relaxed,one-on-one, play setting. Following SpecialTime, parents/caregivers complete a homeworksheet, which helps them to reflect on their targetin a structured way. The therapist uses this re-cord sheet to monitor how the parents areimplementing the targeted change.
Second SessionThe initial task in this session is to make surethat the Special Time routine has been success-fully established. When, from time to time,parents discover that they have committedthemselves to more than they can manage, their
contract is adjusted appropriately. If parentshave been unable to do Special Time, this is dis-cussed constructively to discover what is gettingin the way and to problem solve how this can beresolved. The Palin PCI program only startswhen the minimum number of Special Times isestablished because they are the ‘‘vehicle ofchange’’ within the home environment.
The therapist and parents then revisit theassessment summary to focus on the factors thatseemed to be affecting the child’s fluency andreview what the parents already know that seemsto help the child. For example, the assessmentmay reveal that the child has well-developedlanguage skills but his speech sound skills arestill developing, that he stutters most when he iscompeting with his siblings to speak, and that itseems to help when he can ‘‘take his own time.’’The first two video clips on the publisher’s web-site for the book (thePoint) illustrate this proc-ess with parents.
See Video Clip 1, Evan’s mother and father arediscussing the factors that they think have contrib-uted to Evan’s current difficulties as revealed in theassessment completed 2 weeks previously. This is fol-lowed by a discussion about what they think Evanneeds in light of this to help him with his fluency.
See Video Clip 2, Elaine asks Jayneequa’s motherwhat her instincts tell her that Jayneequa mightneed to help with her fluency.
The next step in this session is to use the vid-eotape made in the clinic the previous week tobegin to identify interaction styles that supportthe child’s fluency by looking at examples fromthe tape where parents are already doing thingsto help. These might include helping the childto take his time by following his lead in theplay, by encouraging pauses, or by having anunhurried manner. The next clip on the DVDshows a clinician helping a mother identify afluency-facilitating behavior that she is alreadyengaging in.
See Video Clip 3, Jayneequa’s mother has justwatched the first video of her playing with Jaynee-qua. Elaine asks her what she noticed that seemed tobe helping. She notices that she is patient and givesJayneequa time. Elaine then asks her how this helpsJayneequa’s fluency.
76 Treatment of Stuttering

Each parent observes their own section of theinteraction video, and the therapist asks themindividually to comment on aspects of theirinteraction with which they were pleased. Start-ing with this encouraging approach is reassuringand sets the stage for a positive experience. Ini-tially their observations might be quite general,for example: ‘‘We both seemed to be enjoyingthe game’’ or ‘‘We were doing lots of laughing!’’The therapist’s role is then to guide the parentsto notice the behaviors that they are alreadyengaged in that support the child’s fluencyneeds and to reinforce these observations. Someparents find it difficult to see what is going welland focus instead on more negative aspects.Watch the next video clip to see how a cliniciancan help a reluctant parent find something quitehelpful he is already doing.
Video Clip 4 demonstrates how to turn this aroundfor a parent. Dylan’s father is finding watching thevideo hard and is describing how nervous and unnatu-ral he felt. Elaine asks what was going well, and hefinds this question difficult to answer. She selects apiece of the video and helps him to look again and focuson something positive. They work it out together untilhe can see how following Dylan’s leads helps to slowdown the pace of the interaction to suit Dylan. Theythen set this as a target for Special Times.
In addition, the therapist may prompt theparents when necessary by highlighting keymoments during the video—for example, bydrawing attention to pauses in the interactionwhen no one is talking:
Therapist: ‘‘What is happening here?’’Parent: ‘‘Nothing, no one is talking.’’Therapist: ‘‘With your child’s needs in mind,
how will pauses like that be useful?’’Parent: ‘‘It helps calm things down.’’Therapist: ‘‘What difference does that make?’’Parent: ‘‘It slows us both down and lets him
know there is no hurry. He can respond or notin his own time.’’
Therapist: ‘‘And how does that help?’’Parent: ‘‘Well…he’s usually more fluent
when that happens.’’Parents often find it easier to be critical of
themselves when they watch the video than tosee what is working well. Therefore, it is impor-tant for therapists to develop ways to help
parents focus on the things they are doing thatsupport the child’s fluency.
Parent: ‘‘I can see that I’m busy doing it allfor him.’’
Therapist: ‘‘And when you are not doing itfor him, what is happening?’’
Parent: ‘‘I am watching and waiting for himto do it.’’
Therapist: ‘‘And how does that help?Parent: ‘‘Well, he gets to do it for himself.’’Therapist: ‘‘And what difference does that
make?’’Parent: ‘‘He finds out he can do it himself
and that helps his confidence.’’Therapist: ‘‘And when he’s more confident?’’Parent: ‘‘He’s often more fluent.’’Therapist: ‘‘So let’s look for the times when
that is happening.’’
General questions such as ‘‘What are youdoing that seems to help?’’ or ‘‘What is workingwell here?’’ provide a general orientation andcan be effective in eliciting observations fromsome parents. For others, the therapist will pro-vide more specific guidance and orientation byreferring to particular moments captured on thevideo. The therapist uses carefully focused ques-tions to help parents notice supportive behav-iors that are already present, no matter howbrief they might be. Pausing or replaying sec-tions of the video and using questions (such as‘‘What did you do there that worked well?’’‘‘What happened when you did that?’’ ‘‘Whatdifference does that make?’’ or ‘‘How does thathelp his/her fluency?’’) help parents to observetheir interaction in a positive way that links itspecifically to their child’s needs.
As explained earlier, the process of watchingthe video, discussing observations, and settinggoals is done on an individual basis with eachparent. Parents quickly learn to observe theirvideos objectively. While each parent is party totheir partner’s discussion with the therapist,they are not invited to comment on each other’svideos. However, if they wish to do so, they arereminded that their comments should be posi-tive and constructive.
The therapist uses facilitative questions to elicitideas or thoughts from the parents about whythese particular interactions might support theirchild’s fluency. For example, having observed a
77Chapter 5 • Palin Parent–Child Interaction

noticeable pause before responding to the child,a question such as ‘‘How is that pause helping?’’makes parents consider the positive consequen-ces of their behavior and ensures that a clearrationale is established for encouraging this par-ticular interaction style. Each parent then indi-vidually selects an interaction style that he or shewould like to try to perform more often; this isbriefly practiced in a video-recorded play sessionwith the child and then played back on thevideo. When each parent is confident that theyknow what they are targeting and why, the iden-tified parent behavior becomes a goal for prac-tice during Special Time at home for thecoming week.
The interaction style that parents noticemost often as helpful in increasing fluencyseems to be related to the child leading the playand setting the pace of an interaction. Once aparent notices this and waits for the child totake the lead more often, the child then sets theplay agenda, the language level, and the pace ofthe interaction. The more the child takes thelead, the more the parent needs to observe andlisten in order to follow the child and the easierit is to match their own level of language andpace to that of the child. Parents also begin tonotice that making a change in one aspect oftheir interaction style often has an effect onanother aspect, for example, resulting inchanges in patterns of turn taking or in the bal-ance of turns or the number of pauses thatoccur.
As parents identify target behaviors that theythink are helpful and would like to do more of-ten, they also explore with the therapist howincreasing these targets might also support thechild’s language skills, phonology, general con-fidence, and autonomy. It is important to notethat parents rarely have more than three targetsthroughout the therapy because change in onetarget area usually involves shifts in another; forexample, targeting an increase in the use ofpauses often results in shorter, simpler senten-ces and an overall reduction in rate.
Once parents are satisfied that the targets theyare working on are having the desired effect (i.e.,a reduction in the type or frequency of disfluen-cies within the Special Times), they are encour-aged to begin to identify other key times duringthe day when they can interact with the child in
ways that they know facilitate the child’s fluency,for example, on the walk home from school, inthe car, or at mealtimes. These are in addition totheir regular Special Times and can also belogged on the homework sheets along with Spe-cial Time. (See Figs. 5.2 and 5.3 for an example ofhow these sheets might be organized and com-pleted.) Parents continue to make commentsabout the effect that this intervention has andgradually increase the occasions when they moni-tor their interactions until it becomes routine andnatural.
Parents/caregivers leave every session with ahomework sheet that identifies their targets andthe number of sessions of Special Times theyhave agreed to undertake. They fill in theirhomework sheet at the end of each SpecialTime and return to the next session with home-work completed and comments made abouttheir experience of putting the targets intopractice.
Structure of Sessions 2 to 6Each treatment session includes the followingcomponents. First, the therapist checks thefeedback from the parents’ homework sheetsand answers any queries about Special Timetargets and their impact. Then, a new video ismade of each parent playing for 5 minuteswith their child, putting into practice theirinteraction targets. The therapist and theparents watch the new interaction video andhave a discussion about the video that focuseson the positive changes that will support theirchild’s communication needs. Questions areasked, such as ‘‘What is going well?’’ Follow-up questions are also asked, such as ‘‘Whatelse can you see that is helping?’’ and ‘‘Whatdifference does that make?’’ Parents then iden-tify a new goal for their Special Time and takeaway a homework sheet to complete. The nextvideo clip illustrates what this scenario mightlook like.
See Video Clip 5, Evan’s parents are in session 3.They talk about the targets they set for themselvesand discuss what they have learned from the exercise.Evan’s father was trying to match Evan’s rate oftalking and to pause more often. He talks about real-izing that Evan’s natural rate of speech is very slow.
78 Treatment of Stuttering

The mother’s targets were leaving gaps in the inter-action and not feeling the need to fill in the pauses.The parents then watch the video. Willie asks themwhat they saw that was going well. She reinforces
their ideas and continues with ‘‘What else?’’ and‘‘How does that help?’’ or ‘‘What difference does thatmake?’’ Finally, Willie helps both parents identify atarget for the coming week.
SPECIAL TIME TASK SHEET
NAME OF PARENT: ________________________ NAME OF CHILD: _____________________
NUMBER OF SPECIAL TIMES: __________
TARGETS FOR SPECIAL TIME: ____________________________________________________
________________________________________________________
DATE ACTIVITY COMMENTS ABOUT THE TARGETS
IN ONE SENTENCE, WRITE DOWN WHAT YOU HAVE LEARNED FROM THIS WEEK’SACTIVITIES:
Figure 5.2. Sample of sheet used to record observations made about Special Time activities conducted as part of treatmenthomework and a completed example showing how the sheet is used.
79Chapter 5 • Palin Parent–Child Interaction

Other Components of Palin PCIIn addition to the major components describedearlier, sessions 2 to 6 routinely incorporatetopics such as openly acknowledging stuttering,
building confidence, turn taking, dealingwith feelings/emotions, and managing problembehavior. The discussion of these topics is facili-tated by referring to specific chapters in the
SPECIAL TIME TASK SHEET
NAME OF PARENT: ________________________ NAME OF CHILD: _____________________
NUMBER OF SPECIAL TIMES: __________
TARGETS FOR SPECIAL TIME: ____________________________________________________
________________________________________________________
DATE ACTIVITY COMMENTS ABOUT THE TARGETS
IN ONE SENTENCE, WRITE DOWN WHAT YOU HAVE LEARNED FROM THIS WEEK’SACTIVITIES:
Mary Jo
4
follow Jo’s lead, use more pauses
22/01/08
24/01/08
26/01/08
Played shops I waited and watched for a bit so I could follow whatJo was doing rather than doing my own thing. It washard pausing more as I love to talk but I think Imanaged it a bit more than usual, I felt more relaxed.
Played with her dolls She loves to play dolls and got quite bossy with metelling me what to do! I did as I was told and sheloved it!
Played tummy ache game Jo showed me how to play it and I joined in. I thinkI am better at leaving pauses and now find it easierand it all feels a bit more like there is more timewhich is good.
Figure 5.3. Sample of completed Special Time task sheet.
80 Treatment of Stuttering

book by Faber and Mazlish (1980) in which par-enting skills are described in a clear and accessi-ble style. The parents then record examples ofpraise that they give the child on a daily basisand note the child’s response on a praise log,which is returned weekly along with the home-work sheets.
If, during the assessment, parents highlightedconcerns related to child management or theestablishment of routines (e.g., bedtime routines)that they feel are affecting the child’s fluency,additional strategies are discussed and included inthe 6-week program. Therapists typically talkthrough the situation and then help the parentsproblem solve alternative ways to manage theproblem. These may include negotiating somefamily rules (e.g., for bedtimes or turn taking),using praise and/or a reward system, setting clearboundaries, and being consistent.
STAGE 2: THE HOME-BASEDCONSOLIDATION PERIODSession 6 of Palin PCI begins with the same for-mat as previous sessions followed by a discussionabout the next 6 weeks, which is referred to asthe home-based consolidation period. Duringthese 6 weeks, the parents continue to do Spe-cial Time with their child at home, implement-ing their targets and completing the homeworksheets. They also continue to incorporate activ-ities for developing the child’s confidence, forpromoting turn taking within the family, andfor any other relevant management issues.Although the family does not attend the clinicduring the consolidation period, they continueto send in their homework sheets so that thetherapist is able to monitor progress and re-spond by letter, telephone, or email. If there isany deterioration in the child’s fluency duringthis time or if other problems arise, the parentsagree to telephone the therapist as soon as possi-ble. It is also agreed that if the therapist does notreceive the homework sheets, contact will bemade with the family. A review session is held atthe end of the 6-week consolidation period.
STAGE 3: THE REVIEW SESSION ANDCLINICAL DECISION MAKINGIn the Review Session, parents complete ratingscales and discuss the Special Times and any
other matters that may have arisen during the con-solidation period. They also have an opportunityto share their observations of the changes theyhave made and the effects of these changes onthe child’s fluency and communication skills. Aformal fluency analysis is made from a tape-recorded speech sample, and a parent–childinteraction video is made and viewed with bothparents. This provides objective evidence of pro-gress and gives the parents an opportunity toconsider the impact of the changes they havemade over the 6 weeks. The therapist reinforcesthe progress and invites a discussion about thefactors that the parents consider to be particu-larly important in increasing the child’s fluencyand confidence and how they will continue tomake progress.
The results of the assessment, the parents’questionnaires, and the feedback from theweekly homework sheets will help the parentsand the therapist decide whether they are readyto go on to the Monitoring Only phase. The cri-teria for moving to Monitoring Only are a com-bination of factors, such as a noticeable increasein fluency and a decrease in the amount and/orseverity of the stuttering, an increase in parentalconfidence, and a reduction in parental concern.At this point, we expect that two-thirds of chil-dren will go on to Monitoring Only, and theparents will continue regular Special Times andcomplete homework sheets that they will con-tinue to send in. They will be reviewed again atintervals negotiated with the family, usually 6 to12 weeks, and for a period of at least 1 year aftertherapy.
Children who are not improving sufficientlyor who have reached a plateau and whose parentscontinue to be concerned will start sessions ofdirect fluency work within the clinic, which willbe supported by parents during home practicesessions in addition to their Special Time. In thesection on the theoretical basis of Palin PCI,we indicated that we believe some children havea greater vulnerability to stuttering. It may bethat these children have a greater physiologic‘‘weighting’’ for persistent stuttering and needsupport to manage their speech motor controlsystems more efficiently. Alternatively, it may benecessary to address any identified mismatches intheir speech, language, and/or motor systems byworking directly on those domains.
81Chapter 5 • Palin Parent–Child Interaction

ADVANTAGES OF PALIN PCIThere are a number of advantages to Palin PCI.First, it can be implemented with children forwhom direct therapy would not be indicated.For instance, it can be used with very youngchildren and is not reliant on a child havingwell-developed attention, listening, cognitive,meta-linguistic, or self-monitoring skills.
Second, although the approach encouragesparents to acknowledge their child’s stuttering,the main focus of the initial stages of theprogram is not on the child’s speech. This focushas the advantage that it can be used withchildren whose temperament is described ashighly sensitive and who may interpret directtherapy as suggesting that stuttering behavior isunacceptable.
Third, Palin PCI lays the foundations for thosechildren for whom the direct therapy componentof the program is also recommended. The insight,knowledge, and skills gained by parents during theassessment and therapy process play an importantrole in helping the child to transfer the speechmanagement skills learned during the direct ther-apy stage of the program.
SUMMARYThe key component of the Palin PCI approachis the use of video feedback to help parents de-velop strategies to facilitate their child’s fluency,based on their unique profile of skills. Thesestrategies are practiced at home in structuredSpecial Time sessions, and then generalized andcombined with other strategies, such as turntaking and confidence building. The familyattends six clinic sessions and then continues theprogram in a 6-week home-based ConsolidationPeriod, followed by a review and further directinput or other therapies as necessary or by mov-ing into a Monitoring Only stage.
ASSESSMENT METHODS TOSUPPORT ONGOING DECISIONMAKING
INITIAL ASSESSMENT TO SUPPORTDECISION MAKING REGARDINGINTERVENTIONThe assessment protocol encompasses the cogni-tive, linguistic, social, emotional, and physiologic
components of the child’s stuttering. The infor-mation is collected during a comprehensive childassessment and a detailed interview with bothparents.
The assessment protocol includes thefollowing:
• Formal and informal measures of the speech,language, and social communication skills ofthe child.
• A recorded speech sample is transcribed andused to calculate a percentage of syllablesstuttered (%SS) and to make comments aboutthe type and duration of stuttered moments.
• An interview to gauge the level of the child’sconcern and his or her perception of theproblem.
• A video recording of each parent/caregiver play-ing with the child. This provides a naturalisticsample of the child’s speech while interactingwith each parent/caregiver and allows furtherinsight into the child’s skills. It also provides aninitial record of the parent–child interactionstyle.
• A detailed case history from both parents (asappropriate) to explore the history and devel-opment of the stuttering and other pertinentissues within the family (e.g., difficultiesmanaging family routines such as bedtimes,getting to school in the morning, or siblingrivalry).
• Parent rating scales provide an insight intotheir level of knowledge, concern, and confi-dence in managing the child’s difficulties(Millard, 2002).
This detailed assessment procedure ensuresthat a profile of the child’s strengths and needswithin the context of the family can be obtained.The information from all these sources providesthe basis for the formulation. This is a summaryof the assessment findings and the factors thatwe have identified that seem to be relevant tothe onset and development of their child’s stut-tering. This summary is discussed with theparents and explained within the context of themultifactorial framework of stuttering. This isimportant in establishing a shared understand-ing of the problem and encouraging the collabo-rative relationship that is fundamental to PalinPCI. Parents and children are also encouragedto acknowledge and discuss stuttering openly
82 Treatment of Stuttering

from the beginning with an implicit rationalethat talking about difficulties reduces anxietyand makes them easier to manage.
Once it has been established that interven-tion is appropriate, the information from theassessment indicates which areas should beaddressed in the therapy program.
Palin PCI routinely involves parents in con-sidering their interaction and behavior manage-ment strategies. It also involves the child indeveloping speech-related strategies. Althoughthe delivery of Palin PCI will be similar acrossfamilies in terms of number of sessions and ses-sion plan, the content of the sessions will vary,depending on the individual needs of the childand the family. These are determined in consul-tation with the parents and in response to indi-vidual needs identified in the assessment.
ONGOING ASSESSMENT TOMONITOR TREATMENTEFFECTIVENESSThe program is delivered as a 6-week packageof once-weekly sessions followed by a 6-weekconsolidation period during which the SpecialTimes are continued by the parents at home.Progress is monitored throughout the 12 weeksthrough the parents’ written and verbal reportsof the child’s fluency, confidence levels, and thefamily’s progress with other strategies. Writtenhomework sheets, which record the interactiontargets identified by each parent during thetherapy sessions, are completed by the parentseach week and brought or sent to the therapistfor monitoring and feedback. Parents are alsoencouraged to provide verbal feedback abouttheir child’s progress and their own perceptionof how the therapy is going. During the clinicsessions, a video recording is made, providing asample of the child’s fluency during play and arecord of the changes in the parent–child inter-actions. The therapist also observes the child’sfluency levels throughout the session. The com-bination of this verbal and written parental feed-back, together with the therapist’s observations,enables decision making about next steps intreatment and about the appropriateness andeffectiveness of the intervention.
At the end of 12 weeks, the family returnsto the clinic for a reassessment and review ofthe child’s progress. As before, this includes a
recorded speech sample from which an analysisof the fluency is made and another completionof the rating scales by parents. A further videorecording is made of the parent and child inter-acting. Based on these reassessments and discus-sions with the parents, decisions are maderegarding the need for further therapy and, if itis needed, what form it should take. The optionsinclude working with the child more directly onthe stuttering or therapy directed at other areasof difficulty in the child’s speech and languageskills that were identified during the compre-hensive assessment and that are not resolving(e.g., a phonologic problem).
Therapy sessions are no longer indicatedwhen the level of stuttering is within normallimits (<3% SS) and/or the parents are no longerconcerned, as recorded in the clinic measures,and the family is reporting a similar pattern athome. Parents would also be reporting reduc-tions in their anxiety about the problem andhigher levels of confidence in their ability tomanage the stuttering, as indicated by theirverbal feedback and the rating scales.
Most families reach this stage at the end ofthe 12 weeks and continue to be monitored andreviewed at regular intervals as agreed by theparents, usually every 6 to 12 weeks for up to1 year. The same assessments are completed atthe review sessions for at least 1 year. If theparents express concerns, a review appointmentwill be made earlier to determine if furtheraction needs to be taken.
TAILORING THE TREATMENTTO THE INDIVIDUAL CLIENT
Therapy programs provide a useful structurefor clinicians, guiding them through a series ofsteps and treatment stages. However, a one-size-fits-all approach is unlikely to meet theneeds of all clients, and this is certainly true withchildren who stutter. Most researchers andclinicians agree that no two children who stutterare the same; therefore, each child will requiretreatment to be tailored to his or her specificneeds.
As stated earlier, Palin PCI starts with adetailed assessment from which an individual-ized treatment program is devised. The child’sneeds, together with the family’s circumstances,
83Chapter 5 • Palin Parent–Child Interaction

dictate the specific components of the therapy.This means that personal and cultural factorsfor the child and family are integral to theassessment and therapy process.
To ensure that children and families fromdiverse cultural and linguistic backgrounds haveaccess to this approach, it is frequently necessaryto arrange for advocates and/or interpretersto assist in assessment and therapy. At the PalinCentre, professional interpreters who havebeen appropriately trained are used, rather thanfamily members, to ensure that interpersonalfactors are not interfering with the informationthat is being exchanged. Interpreters can alsobe invaluable in providing the clinician withgeneral information about a particular culture;for example, attitudes to disability, roles of moth-ers and fathers, and expectations of therapy.However, these generalizations about a culturemust always be regarded as such, as each familywill have its own unique set of attitudes andcustoms.
In a similar way, it is important that familieshave equal access to Palin PCI, whatever theirpersonal circumstances may be. When there aretwo parents with the child at home, both areinvolved in the assessment and therapy program.When one parent is living away from home (e.g.,working or studying abroad), therapy would pro-ceed with the parent who is available, and thenfurther input would be arranged when the otherparent is at home. If parents have separated ordivorced but are both caring for the child, theyare asked whether they want to attend sessionstogether or separately. In the case of single-parent families, if there is a significant other care-giver (e.g., a new partner or a grandparent whothe parent wishes to include), they are invited toparticipate in sessions. If another person cares forthe child (e.g., foster parent, child minder, nanny,or grandparent), this person can be involved inassessment and therapy.
Other personal factors may have an impacton the timing and nature of therapy. Parentswho are experiencing relationship issues orhealth, finance, or housing concerns may find itdifficult to engage with the therapy processbecause these issues may be a greater priorityfor the family. Clinicians may be able to providesupport, give practical guidance, or help parentsto find support elsewhere. In circumstances like
these, it is important to be realistic about expect-ations of what therapy can achieve. For parents,taking on new tasks as a part of therapy is alwaysa challenge, and to try to do this in the contextof other stresses requires sensitivity and flexibil-ity to reach a successful conclusion.
As with all speech and language therapy, thereare some cultural groups who find aspects of PalinPCI challenging. For example, there are someparents who may not be accustomed to the idea ofplaying with toys and do not usually engage inimaginative play with their preschool child. How-ever, they may be encouraged to consider otheractivities they engage in at home that are also suit-able for Special Times, such as a cooking activityor going to the park together. Furthermore,cultural differences may exist with regard to useof eye contact, taking turns to speak, or sleepregimens. However, these can usually be man-aged within the framework of Palin PCI becausethe fundamental principle of the therapy is towork with the family to identify what works forthem and how this can be adapted to support theneeds of the child who is stuttering.
One of the strengths of Palin PCI is that it isbased on the premise that parents instinctivelyknow what helps their children and are alreadyacting on this knowledge much of the time. PalinPCI helps them to do more. Therefore, they arenot being asked to stop doing something or tostart using a new and different style. This meansthat whatever a parent’s cultural or personal stylemay be of interacting with and managing theirchild, they will be developing the aspects of thisthat they understand to be most helpful to theirstuttering child. In this way, Palin PCI has, at itscore, the means to be sensitive to individual fami-lies’ needs, both culturally and personally.
APPLICATION TO ANINDIVIDUAL CHILD
M and his parents came for a full assessment ofhis fluency when he was age 3 years 8 months.He started to stutter gradually at the age of 2.5years. He was reported as talking late with a lim-ited vocabulary compared with his peers, and hismother said that ‘‘he had never spoken clearlyand his sounds weren’t right.’’ M was referred tothe Palin Centre by his local speech and lan-guage therapist who had been offering advice
84 Treatment of Stuttering

and monitoring over an 18-month period. M’smother said that during that time, his fluencyhad been patchy and that each time stutteringre-emerged it stayed longer. She said that thestuttering had become increasingly severe overthe last 6 months with no periods of remission,and she noticed that excitement and tirednessmade the stuttering worse. She also reportedthat he had been a confident little boy but thatthis confidence had been decreasing over 6months. At the time of the assessment, shenoticed that he was hesitant in new situationsand talking less and that other people were be-ginning to talk for him. M’s mother describedherself as becoming increasingly anxious as shewatched him struggle to get the words out, anddespite following all the advice she had beengiven, nothing she did seemed to help. She wasalso worried that he might get teased or bulliedwhen he started school. His father had a morelaid back approach to M’s stuttering, believing itwould get better in time.
There was a maternal family history of stut-tering. M’s grandfather stuttered throughouthis life, and an uncle stuttered until he was ateenager but subsequently recovered.
During the initial assessment, a speech sam-ple was video recorded and analyzed, identifyinga rate of 6.4% syllables stuttered. There wererepetitions of up to 12 times, prolongations thatlasted up to 6 seconds, and blocks accompaniedby facial tension.
When asked about his talking, M said thatsometimes ‘‘it was hard for him to say things.’’His parents said he would refer to his ‘‘badvoice,’’ and they had noticed times when hewould give up or change words that were prov-ing hard to get out. M’s parents described hisspeech on the day of the assessment as being ‘‘ina good phase’’ and that his stuttering was oftenmuch more severe. On a rating scale of 0 to 7,where 0 is normal and 7 is very severe, bothparents rated M’s speech as 5 on the day of theassessment (in a good patch) and 7 at othertimes. In terms of their worry about the stutter-ing, they rated themselves as 6, where 0 is notworried at all and 7 is extremely worried.
During the assessment, The British PictureVocabulary Scale (BPVS) (Dunn et al., 1997), aformal measure of M’s receptive language skills,was administered and demonstrated that he had
above-average scores for his age. The RenfrewAction Picture Test (Renfrew, 1997), an expres-sive language test, placed him above average forgiving information but only average in hisknowledge and use of grammatical skills. Fur-thermore, there was evidence of immaturities inhis speech sound system. At age 3:8, he was stillfronting sounds such as /k/ and /g/ and reducingblends such as ‘‘weet’’ for ‘‘sweet,’’ which some-times made his speech difficult for people tounderstand. M’s attention span was observed tobe short. In terms of temperament, M wasdescribed by his parents as a sensitive child wholikes to get things right and is easily upset.
These assessment findings identified the fac-tors that seemed most relevant in the develop-ment of M’s stuttering and indicated his level ofvulnerability to persistent stuttering.
M’s level of vulnerability to persistent stut-tering was judged to be moderate to high, basedon the following indicators:
• History of delayed speech and languagedevelopment
• Mismatch in speech and language skills• Time since onset of stuttering• Stuttering getting worse over time• Family history of stuttering• Parental anxiety• Child’s sensitivity and reactivity to errors
On the strength of this assessment, it wasdecided to offer the family a course of PalinPCI. M’s age, his short concentration span, andhis sensitivity to the breakdown in his fluencymade this a more appropriate option than amore direct speech approach at this stage.
Palin PCI was tailored to M and his family’sneeds by focusing on the following areas:
• Establishing Special Time• Building M’s confidence• Helping M manage his feelings more easily• Monitoring tiredness and bedtime routines• Interaction strategies aimed at helping M give
himself sufficient time to think and plan whathe is going to say
SESSION 1Session 1 started with a reminder of the results ofthe assessments and M’s particular needs, such ashaving complex things to say and needing moretime to plan, structure, and produce them. M’s
85Chapter 5 • Palin Parent–Child Interaction

parents were also concerned about his sensitivityand were wondering how best to handle his wor-ries. They reported that after the assessment,they were already being more open about hisstruggles with words and they had noticed thatthey had all been more relaxed about it.
Special Time was introduced, and the num-ber of sessions was negotiated with M’s mother,who decided she could do six a week, and M’sfather, who agreed to do four. A video was madeof each parent playing with M for 5 minutes inthe clinic.
The parents were also interested in readingabout children’s feelings, and a chapter called‘‘Helping Children Deal with Their Feelings’’in the book by Faber and Mazlish (1980,pp. 1-47) was recommended.
SESSION 2After checking that the homework had beencompleted, M’s parents were invited to considerwhat M needed based on their understanding ofhis current skills in order to be more fluent.They said they thought that ‘‘his brain wasgoing faster than his mouth’’ and he needed togive himself more time to plan and structure thecomplicated ideas he was often trying to express.They then watched the video made the previousweek. They were encouraged to look at theircommunication with M and notice the thingsthey were doing that seemed to help. M’s fatherfound this difficult at first, but once directed tolook at a particular section, he noticed that thepace of the conversation was relaxed and unhur-ried and that there were often pauses when noone spoke. He also noticed that they each had anequal share of the turns. These observations werediscussed in terms of how they might help sup-port M’s fluency. When asked to consider a tar-get that he would like to concentrate on duringhis Special Times, M’s father said that he thoughtcomments worked better for M than questions,and so he would concentrate on making morecomments. M’s mother noticed that she waspausing at times, had good eye contact, and wassitting at his level and opposite him so she couldsee his face and he could see hers. She decidedthat it helped when she paused and followed M’sleads in play, and she decided to work on follow-ing his leads more because this would help himdictate the pace and focus of the play. These
targets were also discussed in terms of M’s identi-fied needs and how they might help him with hisfluency, his language, and also his confidence.
The chapter on helping children deal withtheir feelings from Faber and Mazlish (1980)was discussed with the parents, and they decidedto implement some of the strategies suggestedin the book, such as listening, acknowledginghis feelings, and resisting the temptation to giveadvice.
The targets for the week included to followM’s leads for the mother and to make morecomments instead of questions for the father.
SESSION 3Both parents had completed their homeworkbut were worried that they had not been able toimplement their targets as well as they wouldhave liked. However, once they had made a newvideo and looked at it, they realized they weredoing much better than they thought. M’s fathernoticed that he was making many more com-ments and pausing and pacing himself in a waythat he could see was helpful to M. He thoughtthat his new target could be to use shorter sen-tences that matched M’s more often because hecould see how that might help M keep his lan-guage simple and increase his fluency.
M’s mother was pleased with her ability tofollow his lead and also thought she was pausingmore and matching his rate better. She hadbecome aware that M’s natural rate was slowand that he seemed to need the extra time.
M’s parents were also keen to help build M’sconfidence, so the chapter on praise from Faberand Mazlish (1980) was recommended.
The targets for the week included matchingM’s rate of speech for the mother and matchingM’s sentence length for the father.
SESSION 4Under normal circumstances, six consecutive ses-sions would be arranged. However, for M’s fam-ily, the fourth session came after a short breakbecause the family had been away. There hadbeen an increase in stuttering for several daysover this period. M’s parents reported that theybelieved this increase was due to excitement,tiredness, and lack of the normal routines. Theyreported that they had managed the situation verydifferently this time because they knew what to
86 Treatment of Stuttering

do. They made efforts to restore the normal rou-tines and get M to bed on time. As a result, whenthey came for the session, they felt that M’sspeech was beginning to get back on track. Theymade a video and were able to reinforce them-selves for the changes they could now see in theircommunication styles. The mother was awarethat her comments were more helpful than ques-tions, and the father noticed that M respondedwell when he followed his leads in play.
The targets for the week included makingmore comments for the mother and followingM’s lead more often for the father.
SESSION 5When asked to indicate what was going wellconcerning their son, both parents were pleasedto report that they were noticing more fluency,especially in their Special Times. They said theywere more relaxed about M’s speech and feelingmore confident about what they were doing.They also reported feeling more comfortablewith the changes they were making and theimpact these were having. Both parents had readthe Faber and Mazlish (1980) praise chapter.Although they were aware of the importance ofpraise and felt they were quite good at praisinggenerally, they could see the added value of thespecific praise described in the chapter. Theyagreed to praise M once a day in this way and re-cord it on the praise log. They made a new videoand reinforced the strategies that were goingwell, of which there were many; they also com-mented that M was often more fluent during the
Special Times. Both parents decided that theircurrent three targets were sufficient.
SESSION 6This session followed the same format as beforeand included a discussion about how to continueworking on their targets during the home-basedConsolidation Period.
After 6 weeks, they returned for a reassess-ment of M’s speech, and the parents again com-pleted the parents’ rating scales. M’s fluency hadincreased, and both parents were pleased withthe progress he was making. They were moreconfident in managing his fluency. In fact, theywere sufficiently confident to want to continueon their own, sending in homework sheets withoccasional monitoring over the next 3 months.
Figure 5.4 tracks M’s stuttering over time.These measures were obtained from 10-minutevideo samples of M interacting with his motherat home in a play session. The tapes were col-lected at weekly intervals for (a) 6 weeks prior totherapy to establish a baseline, (b) 6 weeks dur-ing therapy, (c) 6 weeks during the home-basedconsolidation phase, and (d) 6 weeks after theconsolidation. The next six occasions were col-lected at intervals of approximately 6 weeks.The increase in stuttering in phase (b) was asso-ciated with considerable excitement over a holi-day break. The two increases in phase (d) wereassociated with starting nursery school and set-tling in. M took a little time to settle in, but hisparents felt very comfortable about seeing himthrough this time without further help.
30
25
20
15
10
5
0 Baseline Therapy Consolidation Follow up (d) Follow up (e)
% S
S
Phase
Figure 5.4. M’s fluency in percent syllables stuttered (%SS) over the five phases of baseline, treatment, and follow-up.
87Chapter 5 • Palin Parent–Child Interaction

CASE STUDY
P was 4 years 2 months old when the family wasreferred to the Palin Centre for an assessment.She had been stuttering for 18 months, and herparents were very concerned because it was notgetting any better.
The child assessment indicated that P had aboveaverage verbal comprehension. However, her ex-pressive language scores indicated that she hadsome difficulties with planning and organizingcomplex grammatical structures and had specificdifficulties with word retrieval. She was aware ofher stuttering and had no strategies for managingit. She said that sometimes it was ‘‘hard to get thewords out’’ and that it made her feel ‘‘a bit upset.’’
The interaction video demonstrated that P’sparents were supporting her fluency in a varietyof ways, some of which could be built upon toaddress her particular difficulties, such asincreasing the use of pauses, reducing the paceof interactions, and following P’s leads more.
During the parent interview, P’s parents saidshe had started talking later than her sisters andthat her speech had never been very fluent.They said they were worried because the stut-tering had changed and P was now getting stuckat times and screwing up her face in an effort toget the words out. They said that her speech wasmost fluent in one-to-one situations and whenthere was no time pressure. She had two articu-late older sisters and a younger brother, andthere was a strong family history of persistentstuttering on both sides of the family. She wasdescribed by her parents as sensitive, a worrier,and easily upset by little things. The family sawa therapist when P was 3, and they were advisedthat she was too young for therapy and her stut-tering was quite normal at that age. They weretold that they should not draw attention to itand it would probably go away.
P’s parents rated her stuttering severity as 5out of 7 on a 7-point scale and rated their worryabout her stuttering as 6 out of 7 on a 7-pointscale. They identified turn taking as an issue inthe household and were worried about how tohandle it fairly. They had been trying to makeeveryone stop and wait for P, but the siblingswere not so accommodating. They also reportedthat P’s speech was worse when she was tired,under pressure, or the center of attention. P’s
parents talked about the difficulties they hadorganizing routines such as getting the childrento bed on time. They said that P needed hersleep and often went to bed later than they feltwas good for her.
The parents said they wanted to understandwhat they could do to help and for P to get somehelp ‘‘so she doesn’t struggle so hard to get thewords out.’’
CASE STUDY QUESTIONS
1. What factors in the case history indicate thatthis child is at risk of persistence?
2. What role might parental anxiety play in themanagement of early stuttering?
3. How might following a child’s lead influencethe interaction between parent and child?
4. How is transfer managed in Palin PCI?5. What factors should be considered in the
timing and nature of more direct work onfluency?
FUTURE DIRECTIONS
TRAININGThe Palin Centre has a comprehensive trainingprogram and offers postgraduate training inPalin PCI across the United Kingdom (UK). Asa result, Palin PCI is used extensively in speechand language therapy clinics throughout theUK as a standard package of care for early stut-tering. This training program is being extendedoutside the UK into European countries and theUnited States.
APPLICATION OF PALIN PCITO OTHER DISORDERSThe Palin PCI package of care has been modi-fied (Kelman & Schneider, 1994) and is cur-rently offered to children with speech andlanguage delay in many Early Years Centres inthe UK. It has also been further adapted for usewith other adults who care for children withcommunication difficulties (e.g., in schools andpreschools). Palin PCI has been used effectivelywith children who have additional and/orcomplex speech and language difficulties (e.g.,children with autistic spectrum disorder, chil-dren with learning difficulties).
88 Treatment of Stuttering

RESEARCHFuture research needs to focus on further devel-oping hypotheses regarding which children arelikely to respond to Palin PCI, which childrenmay need additional direct fluency therapy,and which may need only direct fluency therapy.In addition, further research is needed tounderstand the mechanisms by which Palin PCIsignificantly reduces stuttering and which com-ponents of the program are essential in bringingabout this change. It will be important to con-sider clinical effectiveness of Palin PCI in awider range of nonspecialist settings, as well asmeasuring its effects as it is applied to otherpopulations, such as other speech and languagedisorders or bilingual children.
SUMMARYWe expect that Palin PCI will continue to changeand evolve over time. This is as it should be.Reflective practice, user feedback, and advancesin research will continue to inform this process,and Palin PCI will develop accordingly.
CHAPTER SUMMARY• Stuttering is viewed as multifactorial; predis-
posing physiologic and linguistic factors maybe significant in the onset and development ofstuttering, and the interaction of these withemotional and environmental aspects maycontribute to the severity and persistence ofthe disorder and the impact it has on a childand the family.
• A detailed multifactorial assessment identifiesthose factors that may be contributing to thestuttering, as well as the child’s level of vul-nerability to persistence, and indicates areasfor therapeutic intervention
• The main focus of Palin PCI is the child, hisor her profile of skills, and facilitating furtherdevelopment of the naturally occurring flu-ency within the environment.
• Palin PCI is conducted over six once-weeklytreatment sessions with Special Time as homepractice, followed by a home-based consoli-dation period of 6 weeks, and then review andfurther input as appropriate.
Palin PCI achieves its effects by:
• Building on parents’ or caregivers’ knowledgeand confidence in what helps and enhancingexisting behaviors that support fluency.
• Developing with parents a shared understand-ing of the child’s particular profile of speechand language strengths and vulnerabilities.
• Acknowledging that the underlying vulner-abilities that predispose children to stutteringmay also make it more difficult for them to befluent in the context of typical adult-childinteractions.
• Using video feedback to help parents discoverwhat they are already doing that supports theirchild’s fluency, and reinforcing their ability tointeract in ways that match the child’s fluencyneeds.
• Collaborating with parents in setting theirown targets and reinforcing themselves andtheir children as they make progress.
• Facilitating parents rather than telling themwhat to do; a parent’s instinctive expertise iselicited, developed, and reinforced.
• Providing parents with a better understand-ing of the problem and confidence in theirability to use a number of strategies to man-age the problem successfully.
CHAPTER REVIEW QUESTIONS1. What factors might indicate that a child is at
risk of more persistent stuttering?2. What are the similarities and differences
between this program and a direct therapyprogram for this age group, such as theLidcombe Program?
3. When compared with other programs thatinvolve parents, what is different about theway this program engages parents intherapy?
4. What are the key principles of Palin PCI?5. How might you help parents identify targets
to work on?6. What skills might a therapist need to sup-
port parents in the therapy process?7. What factors might explain variability in the
outcome of therapy?8. What factors would indicate that a child is
appropriate for therapy?
89Chapter 5 • Palin Parent–Child Interaction

9. How could this program be adapted to allowfor cultural differences?
10. How might this program be applied to astuttering child who also has significantdelays in speech and language development?
SUGGESTED READINGS
Guitar, B. (2006). Stuttering: An Integrated Approach toIts Nature and Treatment (3rd ed.). Baltimore:Lippincott Williams & Wilkins.
Kelman, E., & Nicholas, A. (2008). Practical Interven-tion for Early Childhood Stammering: Palin PCI.
Milton Keynes, United Kingdom: SpeechmarkPublishing Limited.
Matthews, S., Williams, R., & Pring, T. (1997).Parent–child interaction therapy and dysfluency: asingle-case study. European Journal of Disorders ofCommunication, 32, 346–357.
Millard, S., Nicholas, A., & Cook, F. (2008). Isparent–child interaction therapy effective in reduc-ing stuttering? Journal of Speech Hearing andResearch, 51, 636–650.
Millard, S.K., Edwards, S. & Cook, F. (2009) Parent–child interaction therapy: Adding to the evidence.International Journal of Speech & Language Pathology,Vol 11. Issue 1. pp 61–76.
90 Treatment of Stuttering