Embed Size (px)
Citation preview

อ.พ.ญ. สหสา หมนด
ภาควชาวสญญวทยา
คณะแพทยศาสตรศรราชพยาบาล
Pain Management In Pediatric Patient

Pain: What is it?
•Pain: “unpleasant sensory and emotional experience associated with actual or potential tissue damage”
•Pain is subjective
•Pain is both a sensory and emotional experience:
ดงนนการประเมนควรใหครอบคลมทกดาน

Pain in Pediatric patient Often under-medicated
Often cannot tell you how they feel
May be difficult to assess (under-rating, atypical behavior)
Deserve protection (social responsibility)
Short-term effects may have long-term consequences
Taddio et al.: Lancet 1995, 1997; NEJM 1997 Page et al. – Pain 2001; 90:191-9 Brain Behav Immun 2005; 19:78-87

Barriers to Pediatric Pain Control Belief that children, especially infants, do not feel pain the
way adults do Lack of routine pain assessment Lack of knowledge in pain treatment Fear of adverse effects of analgesics, especially respiratory
depression and addiction Belief that preventing pain in children takes too much time
and effort
Pediatrics, 18 (3) 2001

Adverse Physiologic effects of Postoperative Pain
Pulmonary system - atelectasis - V/Q mismatching - hypoxemia - pneumonia CVS system - hypertesion - tachycardia - myocardial ischemia - cardiac dysrhythmias

Adverse Physiologic effects of Inadequate Pain Control
Endocrine system
- hyperglycemia
- sodium and water retention
- Protein catabolism
Immune system
Coagulation system
- increase platelet adhesiveness
- decreased fibrinolysis
- hypercoagulation
- DVT

Adverse Physiologic effects of Inadequate Pain Control
GI system
- ileus
GU system
- urinary retention

Good pain control requires
accurate and detailed assessment, and reassessment, of each pain
‘ make the pain visible’ knowledge of the different types of pains a different therapeutic approach to pain knowledge of which treatment modalities to use knowledge of the actions, adverse effects and pharmacology
of analgesics multidisciplinary assessment and treatment of other aspects
of suffering that may aggravate pain - physical, psychological, social, cultural and spiritual distress.

Type of Pain
Acute / Chronic Pain
Cancer pain/ Chronic non cancer pain
Mechanism
: nociceptive pain : autonomic, somatic
neuropathic pain
mixed pain

Classification of Pain: By mechanism Nocioceptive Somatic
Bone, joint, muscle, skin, or connective tissue
Well localized Aching & throbbing
Visceral Visceral organs such as GI tract Poorly localized Cramping
Neuropathic Central
Injury to peripheral or central nervous system causing phantom pain
Dysregulation of the autonomic nervous system (e.g. Complex regional pain syndrome)
Peripheral Peripheral neuropathy due to
nerve injury Pain along nerve fibers
http://www.med.umich.edu/PAIN/pediatric.htm

5 General Principles of Pain Management
คาดประเมนความปวดและปองกน (Anticipate & prevent pain)
ประเมนความปวดอยางเหมาะสม(Adequately assess pain)
ใชหลกการรกษาแบบผสมผสาน(multi-modal approach)
ควรใหพอแมมสวนรวมในการรกษา(Involve parents)
เลอกใชวธทไมเจบปวดในการใหยา (Use non-noxious routes )
Pediatrics in Review 2003; 24 (10)

1: คาดประเมนความปวดและปองกน (Anticipate & Prevent Pain) เตรยมผ ปวยและพอแม ถงการทาหตถการตางๆ
ใหการรกษา และปองกนความปวดอยางเหมาะสม Following surgery or local anesthetic for lumbar puncture Pre-emptive analgesia : pre incision infiltration topical analgesia

ควรคานงถงพฒนาการตามวย
ควรเลอกใชเครองมอทเหมาะสมกบวยของผ ปวย
2. ประเมนความปวดอยางเหมาะสม (Adequately assess pain)

การประเมนความเจบปวดในผปวยเดก
Pain assessment : History, physical exam Location, type, severity, characteristics Assessment tools : depend on age and condition
- Self report measures of pain - behavioral measures of pain - Physiological measures of pain
….. รวมกบการสงเกตอาการทางคลนกของผปวยรวมไปดวยเสมอ

Age related measures
Age(y) Physio. Behavior. Self-report < 3 + + - 3-5 + + +/- > 5 - +/- +

การประเมนทางสรรวทยา อาการแสดงของการกระตนประสาท sympathetic เชน HR, RR, BP,
SaO2 Stress hormone เพมขน
ไว(sensitive)แตไมจาเพาะ (specific)
มประโยชนในผปวยทไมสามารถบอกความปวดของตนได

การประเมนทางพฤตกรรม
สหนา (facial expression)
การรองไห
การแสดงออกทางรางกาย
(body language)
ควรใชเมอผปวยไมสามารถบอกความปวด
ของตนเองได

สหนา
0 = เฉยๆ สบาย
1=แสยะ ปากเบะ จมก
ยน หวควยน ปดตา
แนน
รองไห
0=ไมรอง
1=รองคราง
2=กรดรอง
การหายใจ
0=สมาเสมอ
1=หายใจเรวขน
หรอชาลงหรอ
กลนหายใจ แขน
0=วาง
สบายๆ
1=งอ
ขา
0=วางสบายๆ
1=งอ / เหยยด
ระดบการตน
0=หลบ / ตน
1=กระสบกระสาย วนวาย
Neonatal Infant Pain Scale (NIPS)

1-6 ป

CHEOPS รองไห 1=ไมรอง
2=คราง,รองไห
3=หวดรอง
สหนา 0=ยม 1=เฉย 2=เบ
การสงเสยง 0=พดสนกราเรง หรอไมพด 1=บนอนๆเชนหว,หาแม 2=บนปวด+ บนอนๆ

CHEOPS ทาทาง(ลาตว) 1=ธรรมดา สบายๆ 2=ดน/เกรง/สน /ยน/ดนจนถก จบตรงไว
สมผสแผล 1=ไมสมผส 2=เออมมอมา/ แตะเบาๆ/ตะปบ/ เออมมอมาจนตอง จบมอหรอแขนไว
ขา 1=ทาสบาย 2=บดตว/ เตะ/ดงขาหน/ เกรง/ยน/ดน จนถกจบหรอ ตรงไว

สหนา
0=เฉย, ไมย ม
1=หนาตาเบะ หรอขมวดคว ถอยหนไมสนใจ
สงแวดลอมเปนบางครง
2=คางสน, กดฟนแนนเปนบอยๆหรอตลอดเวลา
ขา
0=อยในทาปกตสบายๆ
1=อยในทาไมสบาย, กระสบกระสาย, เกรง
2=เตะ หรองอขาขน
การเคลอนไหว
0=นอนเงยบๆ, ทาปกต, เคลอนไหวสบายๆ
1=บดตวไปมา, แอนหนาแอนหลง, เกรง
2=ตวงอ เกรงจนแขงหรอสนกระตก
รองไห
0=ไมรอง (ตนหรอหลบกได)
1=ครางฮอๆ หรอครางเบาๆ บนเปนบางครง
2=รองไหตลอด หวดรอง สะอกสะอน บนบอยๆ
การสนองตอการปลอบโยน
0=เชอฟงด, สบายๆ
1=สามารถปลอบโยนดวย การสมผสโอบกอด พดคย
เพอดงดดความสนใจเปนระยะๆ
2=ยากทจะปลอบโยนหรอทาใหสบาย
FLACC

อาย 6 ป

การประเมนความปวดจากตวผปวยเอง
Gold standard เดกพดคาวาปวดหรอเจบไดตงแตอาย 18 เดอน
บอกระดบความปวดไดตงแตอาย 3-4 ป
บอกความรนแรง ลกษณะและตาแหนงของความ
ปวดไดตงแตวยเขาเรยน

Pain Assessment Self report
1. Verbal descriptor scales
___0. None
___1. Mild / a little
___2. Moderate / some
___3. Severe / a lot
___4. Worst pain imaginable
2. Visual analogue scale
3. Numerical rating scale

Self - report measure
Color analogue scale Worst pain No pain
Visual analogue scale
0 100

Self - report measure
Poker Chip tool Verbal rating scale 0 = no pain
1 = mild pain
2 = moderate pain
3 = severe pain
4 = worst pain

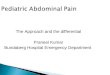
FACES scale

Faces Pain Scale - Revised (FPS-R)
0 (neutral) means “no pain”. The faces show “more and more pain”. The right hand one means “very much pain” (or “the worst pain”). Ask the child to point to “the face which shows how much you hurt right now”.
www.painsourcebook.ca - Hicks et al. [Pain 2001; 93: 173-183]based on Bieri et al. [Pain 1990; 41: 139-50]

ในคาชแจงตอไปนใหใชคาวา “เจบ” หรอ“ปวด” ตามความเหมาะสมแกผปวยเดกแตละคน
“รปหนาตอไปนจะแสดงใหเหนวามความปวดมากเทาไร
รปหนาน (ซายสด) แสดงวาไมปวดเลย
รปหนาถดมาแสดงวาปวดมากขนมากขน (ชรปหนาจากซายมาขวา)
จนถงรปหนาน(ชรปขวาสด) แสดงวาปวดมากๆ
ใหหนชรปหนาทแสดงวาหนปวดมากแคไหน (ตอนน)”
ใหคะแนนตามรปหนาทเลอก 0, 2, 4, 6, 8, 10 ตามลาดบจากซายไปขวา
คะแนน 0 = ไมปวดเลย คะแนน10 = ปวดมากๆ ไมควรใชคาวา“สข” หรอ“เศรา”
การใหคะแนนนมจดประสงคเพอวดวาผปวยเดกมความปวดมากแคไหน
ไมใชการใหคะแนนจากการดลกษณะสหนาของเดก Translation credit: Wimonrat Krisanaprakornkit & Duenpen Horatanaruang Dept of Anesthesiology, Srinagarind Hospital, Khon Kaen University, Khon Kaen, Thailand Instructions for administering the Faces Pain Scale – Revised in languages other than English. 4th Ed. – August 2005. Pediatric Pain Sourcebook, www.painsourcebook.ca
0 2 4 6 8 10
Faces Pain Scale – Revised (FPS-R) Hicks CL, et al. Pain 2001;93:173-83.


3: ใชหลกการรกษาแบบผสมผสาน
Multi-modal Approach
Multiphasic = pre-intra-post-operative
Mutimodal = LA+ opioids+NSAIDs

4: ใหผปวยและผปกครองมสวนรวมในการรกษา
ผปกครอง เปนผ รขอมล ลกษณะนสยของเดกมากทสด ชวยลดความตงเครยดของผ ปวยได
ผ ปวย เลอกใชวธใหเหมาะสมตามวยและพฒนาการ อาจใหมสวนรวมในการเลอกวธระงบปวดไดตามความเหมาะสม

5: เลอกวธระงบปวดทไมเจบปวด
Non-noxious Routes Administer analgesia through most painless route Avoid IM injections Oral and Intravenous routes are preferred Oral route for mild to moderate pain Intravenous route for immediate pain relief and severe
pain


ชนดของความเจบปวดทพบไดบอยในผปวยเดก
Acute Pain
Procedure related pain : LP, MBA, ICU care
post-operative pain
Pain in Life limiting Patient Childhood malignancy Neurodegenerative disorders Cystic fibrosis Cerebral palsy Chromosomal abnormalities congenital malformations HIV

Acute Pain Management

Neonates and Infants
•Barriers to treatment of pain in infants and neonates
•The myth that infants do not feel pain
•Lack of pain assessment &reassessment tools
•Lack of knowledge of pain treatment
•Notion that addressing pain in children takes too much time and effort
•Fears of adverse effects of analgesic medications

NICU Pain
•Diagnostic procedures: Arterial punctures, heel lancing, lumbar puncture, ROP exams
•Therapeutic procedures: bladder catheterization, peripheral IV and central line insertion, dressing changes,OG/NG tube insertion, IM injections, mechanical ventilation, removal of adhesive tape, tracheal suctioning
•Localized infections/inflammation
•Post-operative pain
•Burns or abrasions from probes, leads & topical agents

Pharmacologic Pain Control
Sucrose for analgesia Non-pharmacological analgesia : kangaroo bag, pacifier Pharmacological analgesia should be chosen carefully based on
patient, medication and environment Subsequent doses should be modified based on cause of the pain,
previous response, clinical condition, concomitant drug use, and pharmacodynamics of the drugs used

WHO 3-Step Ladder for Pain
Step 1 - Mild
Step 2 - Moderate
Step 3 - Severe
Non-opioids
Weak opioids
Strong opioids
Always consider adding an adjuvant Rx

Morphine Available orally, subcutaneously, intravenous Moderate to severe pain
Hepatic conversion with renally excreted metabolites
Use in caution with renal failure
Duration of I.V. analgesia 2-4 hours Oral form comes in an immediate and sustained release
Side effect of significant histamine release

Fentanyl Available intravenous, transdermal patch
Severe pain
Rapid onset, brief duration of action With continuous infusion, longer duration of action
I.V. Dose 1 mcg/kg/dose every 30-60 minutes Side effect of rapid administration may produce glottic and
chest wall rigidity

Level II and III Medications
Parenteral route
Morphine 0.1 mg/kg IV bolus, prn. 1-2hr .05 mg/ kg/hr, CI - IV or SQ , PCA
Hydromorphone (Dilaudid) Approximately 6 times stronger than morphine
Fentanyl Approximately 10 times stronger than morphine Wide dosing range 1-2 mcg/kg IV slow push 0.5-1.0 mcg/kg/hr, CI - IV or SQ Total hourly dose as a transderm patch

Level II and III Medications
Enteral route Codeine 1 mg/kg, Q 2-4 hrs, PO
Tramadol 0.7 - 2.0 mg/kg/dose PO Q 4-6 hours Morphine immediate release 0.3 mg/kg PO Q 2-4hr
Morphine SR (MS Contin) : acute pain 0.5 mg/kg, BID, PO (Do not crush)


Patient Controlled Analgesia : PCA

PCA : Patient Controlled Analgesia สามารถใชไดตงแตอาย 6 ปขนไป
การตง background infusion ชวยเสรมประสทธภาพในการระงบปวดในผปวยเดกได
การตง lockout period ปกตตงประมาณ 5 นาท
การตง 4-hourly dose limit เพอประเมนความเหมาะสมการใหยาระงบปวดขณะน

Acetaminophen
Antipyretic
Mild analgesic
Administer PO or PR
Pediatric Oral dose 10-15 mg/kg/dose every 4-6 hr
Infant dose is 10-15 mg/kg/dose every 6-8 hr Maximum dose in children> 6mo = 90mg/ka/day Maximum dose in children< 6mo = 60mg/ka/day
Onset 30 minutes

Acetaminophen Per rectum dose 40 mg/kg once followed by 20
mg/kg/dose every 6 hours Uptake is delayed and variable Peak absorption is 60-120 minutes Contraindication in neutropenic patient

Side Effects of Acetaminophen Generally a good safety profile Do not use in hepatic failure
Causes hepatic failure in overdose Infant drops are MORE concentrated than the children’s
suspension Infant’s Acetaminophen 80 mg/0.8 mL Children’s Acetaminophen 160 mg/5 mL

Ketorolac Intravenous NSAID Dose 0.5-1 mg/kg/dose every 6 hours Onset 10 minutes Maximum I.V. dose 30 mg every 6 hours
Monitor renal function Do not use more than 5 days Significant increase in side effects after 5 days

Contraindication to the use of NSAIDS in children
Hypersensitivity or allergy to aspirin or NSAIDs
Peptic ulcer
Bleeding diatheses
Severe asthma, especially if aspirin sensitive of corticosteriod dependent
Nasal polypitis
Renal dysfunction, hypovolemia, diuretic therapy
Planed major surgery

Codeine Oral analgesic (also anti-tussive) Weak opioid Used often in conjunction with acetaminophen to increase
analgesic effect Metabolized in the liver and demethylated to morphine Some patients ineffectively convert codeine to morphine
so no analgesia is achieved Dose 0.5-1 mg/kg every 4-6 hours

Tramadol
weak receptor
Inhibit serotonin และ nor-epinephrine reuptake

Local Anesthetics For needle procedures, suturing, etc.
Topical or infiltration
Acts by blocking nerve conduction at Na-channels
If administered in excessive doses, can cause systemic effects
CNS effects of perioral numbness, dizziness, muscular twitching, seizures & cardiac toxicity
Aspirate back before injecting to avoid direct injection into blood vessels Calculate maximum mg/kg dose to avoid overdose
Buffering lidocaine can help with pain of infiltration 9 mL lidocaine mixed with 1 mL sodium bicarbonate

Dosing of oral medication commonly use in children Paracetamol paracetamol : 10-15 mg/kg orally q 4-6 hr. 40 mg for 1st dose then 20 mg/kg rectally q 6 h
NSAIDs diclofenac 1 mg/kg orally q 8 hr 20 mg/kg rectally q 6 hr
(max 3mg/kg/day) ibuprofen 5-10 mg/kg orally q 8 hr indomethacin 1 mg/kg orally q 8 hr naproxen 5 mg/kg orally q 12 hr

Dosing of oral medication commonly use in children
Weak Opioids codeine 0.5-1 mg /kg orally q 4-6 hr
(max 3mg/kg/day)
tramadol 1-2 mg /kg orally q 8 hr
(max 6mg/kg/day)

Pain in Life limiting Patient

Pediatric principles and practice
Advanced disease in pediatric palliative care
Childhood malignancy Neurodegenerative disorders Cystic fibrosis Cerebral palsy Chromosomal abnormalities and congenital malformations

Pediatric patients with cancer Pain in a cancer patient can result from
tumor invasion
procedures
therapy : mucositis, neuropathy, surgical incisions, corticosteroid
other causes unrelated to cancer

How to assess pain in patients Pain assessment : Location, type, severity Assessment tools : depend on age and condition
- Self report measures of pain : gold standard - behavioral measures of pain - Physiological measures of pain ….. combined with clinical observation
For chronic pain changing in pain behavior

In palliative care
the analgesic program should be kept simple, even for patients in severe pain
oral medication is the mainstay of treatment and should only be abandoned if the patient is unable to take or retain oral preparations

WHO 3-Step Ladder for cancer pain
Step 1 - Mild
Step 2 - Moderate
Step 3 - Severe
Aspirin
Acetaminophen
NSAIDs
Codeine
Hydrocodone
Oxycodone
Tramadol
Morphine
Hydromorphone
Methadone
Levorphanol
Fentanyl
Always consider adding an adjuvant Rx

Non pharmacological approach for managing procedure pain in children Distraction
Infants : toys, dummy, bubble blower
Preschool children : songs, books, toys
School age children : stories, counting, DVDs
Rewards
etc…

What about when the pain seem intractable?

Intractable pain
Combination of clinical factors and patient factors.
Need review pathology
: Fracture? Cord compression?
Neuropathic pain?

Neuropathic pain symptoms and signs
Radicular/dermatomal distribution
Quality of pain : burning, pins and needles, electrical shock-like, pain in numb area, phantom pain
Associated features : numbness, weakness, abnormal reflexes
Allodynia : pain cause by light touch
Hyperalgesia
Wind up: rapidly escalating pain with decreasing opioid responsiveness

Management for Neuropathic pain
Pharmacological therapy : Acetaminophen, NSAIDs Tricyclic antidepressants Anticonvulsant (carbamazepine, phenytoin, gabapentin)
systemic local anesthetics
opioids (morphine, methadone given PO or IV or through a regional technique especially in cancer patients)
Ketamine infusion
Regional blockades Non-pharmacological treatment
: hypnosis, biofeedback,TENS, physical
therapy etc.

Management for Severe Bone Pain
Medication
-Regular paracetamol
-NSAIDS
-Opioids : background around the clock
dosing and breakthrough doses.
- Bisphosphanate

Management for Severe Bone Pain Anesthetic Procedures Epidural anesthetics Nerve Block
Radiotherpy Neurosurgical Procedures Neurolysis
Orthopedic Procedures Stabilization of pathologic fractures

Management of Visceral pain
Should respond to increased doses of opioids
Paracetamol
Dexamethasone : decrease peri-tumor edema
Avoid co-administration steroid with NSAIDS

Opioid side effects
Respiratory depression
Nausea and vomiting
Pruritus
Urinary retention
Constipation
sedation

Pain and the Reticular Activating System “The respiratory depressant effect of opioid agonists can be demonstrated easily in volunteer studies. When the dose of morphine is titrated against a patient’s pain, however, clinically important respiratory depression does not occur. This appears to be because pain acts as a physiological antagonist to the central depression effects of morphine.”
Wall, R.D., ed. Textbook of Pain. Churchill Livingstone
Opioid Side Effects : respiratory depression

ความพรอมของอปกรณและยาแกไข
Monitoring system
: Pulse oximetry : aged less than 6 month or co-existing disease
Appropriate protocol for resuscitation, oxygenation, contracting appropriate personel
Infusion pump
Syringe pump
PCA
Naloxone : 5 mcg /kg (up to max 100 mcg) IV,
repeated if necessary q 2 min

Respiratory rate Sedation score Pain score Adverse effect monitoring pruritus nausea vomiting urinary retention
Monitoring

Clinical Indicators of Respiratory Depression
Sedation score
0 = none
1 = mild, occasionally drowsy, easy to arouse
2 = moderate, constantly or frequently drowsy, easy to arouse
3 = severe, somnolent, difficult to arouse
S = normally asleep, easy to arouse
Respiratory rate 0-1 ป < 30 ครง 3-6 ป < 20 ครง 1-3 ป < 25 ครง 6-13 ป < 15 ครง
Oxygen saturation
may also unreliable, esp. receiving supplemental oxygen

Medications commonly used to treat opioid side effects
Respiratory depression :
Naloxone 10 mcg/kg (max 100 mcg / dose
q 2-3 min)
Naloxone (5-20mcg/kg/hr)
Pruritus : Diphenhydramine (0.5mg/kg/dose)
Naloxone (0.5-2mcg/kg/hr)
Nausea : Ondansetron (0.15mg/kg/dose)
Naloxone (0.5-2mcg/kg/hr)
Somnolence : methylphenidate (0.1mg/kg/dose)
Naloxone (0.5-2mcg/kg/hr)

A belief that morphine hastens death
morphine may be used for months or years and, correctly administered, is compatible with a normal lifestyle
used properly, it does not hasten death

The fear of respiratory depression
used properly, morphine should not cause respiratory depression, although care must be taken with patients who are at risk of respiratory depression for other reasons

A belief that "Morphine doesn't work"
Morphine will be ineffective in controlling pain if
it is incorrectly administered
it is used for morphine-insensitive pain
matters of psychosocial concern have not been addressed

The belief that morphine causes unacceptable side effects
side effects should not be severe
respiratory depression is uncommon
constipation occurs inevitably and requires explanation and advice about diet and laxative therapy
somnolence and nausea usually improve after several days

That means I'm going to die soon
requires explanation that morphine can be used for months or years and is entirely compatible with a normal lifestyle

“I'll become an addict”
requires explanation and reassurance about physical and psychological dependence

Morphine may not relieve pain if the dose was too low it was given too infrequently there were no instructions for breakthrough pain it was given for insensitive pain matters of psychosocial concern have not been addressed

Take Home messages
Good pain control needs pain assessment and reassessment. Pain can be well controlled in most patients. Opioids are safe if titrated to effect. Pain must be consider along with other symptoms. Patients need regular and as required medications for pain. Families need information and support. Multidisciplinary is required for providing the good care.