Embed Size (px)
Citation preview

Human Movement Science 6 (1987) 17-36
North-Holland 17
PAIN INDUCED BY NERVE COMPRESSION BLOCKS AFFECTS VOLUNTARY MOVEMENTS AND ASSESSMENT OF PERIPHERAL NERVE ISCHAEMIA *
Kerry GREER and Nigel HARVEY
University College London, England
Greer, K. and N. Harvey, 1987. Pain induced by nerve compression blocks affects voluntary movements and assessment of peripheral nerve ischaemia. Human Movement Science 6, 17-36.
Ischaemic cuffs are a common means of experimentally inducing pain. The pain they cause should
be taken into account when they are used to assess the importance of joint and cutaneous
feedback in motor control. A first experiment suggests that the wrist cuff does not exclude joint
and cutaneous input. Instead, it raises pain levels so high that these cues in the presence of pain
cannot be distinguished from pain alone. The cues may, however, still contribute to movement
control. A second experiment demonstrates that a thumb cuff produces only mild discomfort and,
therefore, that sensory cut-off is likely to be related more to a decline in sensitivity than to an
increase in pain. However, a third experiment shows that this discomfort may have a beneficial
arousing effect. Ischaemic cuffs may have no overall effect on movement because this centrally
mediated facilitation counteracts impairment produced at the periphery.
Nerve compression blocks have been used in attempts to dissociate joint and cutaneous components of human voluntary movements from their muscle receptor and non-sensory components. (Laszlo 1966, 1967; Laszlo and Bairstow 1971a; Davies et al. 1964; Goodwin et al. 1972; Kelso 1977; Kelso and Holt 1980.) A block consists of a pressurised cuff which, when applied to the limbs of conscious human subjects, induces first degree nerve injury (i.e., an interruption of axonal conduc- tion at the site of application). The injury, which is totally reversible, results from anoxia induced by circulatory occlusion. When the pres- sure in the cuff is greater than the subject’s systolic blood pressure, the
* Requests for reprints should be sent to K. Greer, Dept. of Psychology and Centre for Neuroscience, University College, Gower Street, London WC1 6BT, England.
0167-9457/87/$3.50 0 1987, Elsevier Science Publishers B.V. (North-Holland)

18 K. Greer, N. Harvey / Incomplete and masked effects of nerue block
oxygen-carrying blood is prevented from flowing past the application site. This renders the part of the limb distal to the cuff ischaemic.
Laszlo and her colleagues used nerve compression blocks on the upper arm in order to investigate the effects on motor performance of removal of kinaesthetic information. Evidence from Sunderland (1951) and Sinclair and Hinshaw (1951) had suggested that efferent nerve ischaemia lagged afferent nerve ischaemia by 5-10 minutes. Laszlo thought that during this period subjects could produce hand/digit movements in the absence of certain proprioceptive cues. However, from a neuroanatomical viewpoint, it is difficult to understand why there should be a temporal dissociation between afferent and efferent nerves under block. Indeed, Kelso et al. (1974) and Kelso et al. (1975) have cited and produced physiological and behavioural evidence to the contrary. Kelso et al. (1975) argue that the upper arm nerve compres- sion block confounds kinaesthetic loss and motor impairment. How- ever, their criticisms only apply in cases where the nerve compression block impairs the efferent nerves that supply the musculature of the limb under observation. Thus they do not hold when a compression block is applied to the wrist in order to induce ischaemia of the hand because the major muscle groups that operate the hand and its digits lie proximal to the wrist. They are therefore unaffected by the block.
Davis et al. (cited by Merton (1964)), Goodwin et al. (1972) Kelso (1977) and Kelso and Holt (1980) are among the experimenters who have studied digital movement under wrist block conditions and who have argued that their results show that motor tasks can be performed without joint and cutaneous feedback. We have no criticism of their rationale. Theoretically, joint and cutaneous cues consequent on the subject’s movements should be eliminated by a wrist block. Our con- cern arose because we felt that movement scientists have tended to underestimate other well documented effects of cuff procedures, namely pain and anxiety. Roy and Williams (1979) did address this issue but even they seem to be unaware of the fact that ischaemic cuffs are used in studies of another quite different kind. They are used as a means of experimentally inducing pain (e.g., Aberger et al. 1983; Clark and Hunt 1971; Johnson 1973; Smith et al. 1966). Pain is known to decrease subjects’ ability to discriminate between stimuli (e.g., Jones et al. 1982; Malow et al. 1980). This ability is required for performing the psycho- metric tasks that are used to determine whether or not an ischaemic cuff has produced sensory cut-off. Thus sensory cut-off may occur not

K. Greer, N. Harvey / Incomplete and masked effects of nerue block 19
when transmission of afferent information has been eliminated but when the level of pain has risen to the point at which it prevents use of that information.
The experiments reported here convinced us that the feedback-at- tenuation and pain-induction effects of ischaemic cuffs cannot be treated independently. We suggest that the point of sensory cut-off determined by psychometric techniques reflects an increase in pain as well as a reduction in feedback. Furthermore, pain-induced stress may influence the efficiency of central processing of feedback and/or motor programs.
Experiment 1
Cut-off occurs when the subject reports insentience to all intensities of the stimuli in the set under consideration. If it occurs long before the cuff causes pain, then movement scientists need not be concerned with nocioception. However, although movement scientists have usually reported time to sensory cut-off and pain researchers have usually reported time to pain onset, neither group of researchers have reported both. The two separate sets of published data cannot be used to determine whether sensory cut-off occurs before pain onset. This is because pain researchers have generally employed higher cuff pressures than movement scientists. Thus our first aim was to record the pain levels (if any) reported by subjects at the point at which sensory cut-off is obtained.
For the wrist block, cut-off time has been assessed to be the order of one hour (Goodwin et al. 1972; Merton 1964). This is approximately 40 minutes longer than the cut-off time for the upper arm block reported by other workers (Laszlo and Bairstow 1971a; Sinclair and Hinshaw 1951). It is known that pain increases with duration of cuff application (Aberger et al. 1983). Consequently, if pain is present at sensory cut-off, it should be greater when the wrist cuff is used to produce sensory cut-off than when the upper arm cuff is used. Our second aim was to test this hypothesis.
Previous studies have examined cut-off for light and/or heavy touch stimuli or appreciation of passive and/or active movement of blocked digits. Cut-off time varies somewhat with the stimulus set that is used. Thus to examine pain levels at cut-off under different types of block,

20 K. Greer, N. Harvey / Incomplete and masked effects of nerue block
an identical stimulus set must be employed in each condition. It is easier to ensure that this criterion is met for touch stimuli than for movement stimuli. There are various reasons for this, the most perti- nent being that ischaemia induced by cuffs in different locations may affect the physical characteristics (e.g., stiffness, viscosity) of a given set of muscles in different ways. Thus the dynamics of active and passive movements involving these muscles would be different for different types of cuff, and may even vary for a given cuff. Hence we decided to use a set of von Frey hairs to test for sensitivity to touch in a small demarcated area of the right thumb. All previous work has shown that cut-off in the tactile modality precedes that of the kinaesthetic modal- ity and so if pain is present in the former case it is certain to be no less present in the latter. We used the staircase method for establishing thresholds because it is the most sensitive psychometric technique for tracking changes in threshold over time. This is because ‘no time is wasted on stimuli to which the subject is either clearly sensitive or clearly insensitive’ (Brown and Deffenbacher 1979: 33). It also, there- fore, minimises the duration of any pain that the subjects suffer.
Method
Apparatus The von Frey hairs consisted of a set of twenty nylon hairs attached
at right angles to rigid plastic rods. Pressure was exerted by placing the tip of the hair against the skin and pressing down with the rod until the hair bent in the middle. Once a given hair had bent, the same pressure was exerted on the skin despite of variations in force applied to the rod by the experimenter. The compression blocks consisted of two sphygmomanometer cuffs. The upper arm cuff was the standard British adult blood pressure cuff, approximately 25 x 11 cm. The wrist cuff was the standard British child’s cuff, 14 x 6 cm. Force applied is a function of the surface area to which pressure is applied (Force = Pressure X Area). Thus in order to attain approximately the same applied force for the two cuffs, the pressure in the wrist cuff (300 mm Hg) had to be almost double that in the upper arm cuff (180 mm Hg). Some of the pressure is required to inflate the cuff itself. Larger cuffs will require more ‘inflation pressure’ than smaller cuffs. The pressure in the wrist cuff is not exactly double that of the upper arm cuff because it is smaller and required less inflation pressure.

K. Greer, N. Harvey / Incomplete and masked effects of nerue block 21
Subjects There were four male and two female subjects, all of whom were
medically screened prior to testing. They were all right-handed academics and their average age was 28 years.
Design There were two sessions in the experiment separated by a recovery
interval of 30 minutes. Half the subjects (two male and one female) were fitted with the upper arm cuff in session one and with the wrist cuff in session two. The other half of the subjects were fitted with the cuffs in the opposite order.
Procedure Subjects performed the experiment individually in the University
Health Centre under medical supervision. After an initial medical examination, each one was asked to remove their upper garments and to put on a jacket from which the right arm had been removed. He or she was then seated in a comfortable adjustable chair, so that the right elbow was level with a foam covered table. The lower right arm rested on this table with the palm facing upwards. The appropriate cuff was then fitted but not inflated. The subject was then blindfolded and a circular area marked out on the top phalanx of the right hand thumb. Sensory testing using the staircase method began prior to cuff inflation. The basic feature of the method is that the subjects’ judgements control the sequence of stimuli that are presented. Thus, each series of stimuli started randomly from one extreme of the stimulus range and, after each judgement, the stimulus intensity was either increased or de- creased. The direction of the change depended upon whether the subject decided the stimulus was present or absent. If the subject reported the stimulus as present, then there was a decrease in stimulus intensity on the next trial. Conversely, if the stimulus was not per- ceived, there was an increase in stimulus intensity on the next trial. In our experiment, this staircase procedure continued prior to cuff infla- tion until the stimulus intensity oscillated around a constant value. This value represented the tactile threshold without nerve block. The cuff was then inflated. After the subject reported the cessation of ‘pins and needles’ and the hot and cold sensations that follow them (sensory disturbances that occur a few minutes after cuff application), the staircase procedure recommenced from the threshold value that had

22 K. Grew, N. Harvey / Incomplete and masked effects of nerue block
been obtained prior to cuff inflation. It continued until no response was obtained to the maximum stimulus intensity on ten successive trials. (Where subjects were still reporting presence of stimuli after 100 minutes, testing was stopped.) The pressure in the sphygmomanometer cuff was then released and the subject was asked to stamp on the floor for a few minutes to aid venous return. The cuff and the blindfold were then removed for the 30minute recovery period. Session two then commenced with the other type of cuff. On completion of the experi- ment subjects reported the level of pain they had experienced (absent, mild, unpleasant, extremely unpleasant, unbearable).
Results
Table 1 shows the cut-off times that were obtained for each of the six subjects under the two types of nerve block. Wilcoxon’s matched pairs test showed that, as expected from previous work, cut-off time was less with the upper arm block than with the wrist block (z = 2.41, p c 0.01). However, both cut-off times were longer than those obtained in these other studies. Median cut-off time for the upper arm block was 38.5 minutes - almost double previously reported estimates. Median cut-off time for the wrist block was 93 minutes - over half an hour more than previously supported estimates.
All subjects reported that the upper arm block produced mild discomfort but that the wrist block procedure produced pain. The four subjects who reached cut-off with this block in less than 100 minutes reported that this pain was almost unbearable after approximately 40 minutes and the other two subjects found it exceedingly unpleasant.
Table 1 Sensory cut-off time (min) for six subjects under two types of nerve block.
Subject Upper arm wrist
1 41 100 2 32 85 3 31 90 4 40 100 5 33 89
6 42 96
Median 38.5 93

K. Greer, N. Harvey / Incomplete and masked effects of neroe block 23
Discussion
A major assumption underlying the psychometric assessment of sensory cut-off is that a reduction in sensitivity to joint and tactile stimulation is the only consequence of cuff procedures. This is not the case. There is a concomitant increase in sensations of pain, the levels of which can become quite intense in the case of the wrist block. Pain is known to reduce stimulus discriminability (Jones et al. 1982; Malow et al. 1980). Because of this, it is necessary to consider the effects of the cuff-induced pain on the psychometric assessment of sensory cut-off. Signal detection theory (Green and Swets 1966; Egan 1978) can account for the effects of pain on stimulus discriminability. Within its frame- work, the problem that faced our subjects should be seen not merely as one of detecting whether or not a stimulus was present but rather as one of discriminating between pain alone and pain with added tactile stimulation. An estimate of sensory cut-off is then an estimate of the point at which a stimulus in the presence of pain can no longer be distinguished from pain alone.
Pain alone trials may be conceptualised as producing a distribution of values along some internal dimension related to subjective intensity of stimulation. Trials in which both pain and and a tactile stimulus are present also produce a distribution of values along this dimension but do so around a higher mean value. The two distributions overlap to some degree. On each trial, a value is produced somewhere along the dimension and the subject has to decide which of the two distributions it belongs to. Because the distributions overlap, false negatives (re- sponding as if the tactile stimulus is absent when it is actually present) and false positives (responding as if the tactile stimulus is present when it is actually absent) are bound to occur. However, both types of error are less likely when the distributions are well separated.
As time from cuff inflation increases, the means of the two distribu- tions come closer and closer together. This is because cuff inflation raises the mean of the pain alone distribution and/or lowers the mean of the pain plus tactile stimulus distribution. At some point the distributions will come to overlap to such an extent that the experi- menter’s criterion for successful performance in the task will no longer be met. The rate at which a cuff attenuates feedback relative to that at which it induces pain will determine the relative importance of these two effects in the production of sensory cut-off. If pain is induced

24 K. Greet-, N. Harvey / Incomplete and masked effects of nerve block
rapidly but feedback reduced only slowly, cut-off will primarily reflect the former process. Thus a subject will report cut-off even though the kinaesthetic receptors under investigation are still functioning. Subjec- tive pain reports taken in conjunction with the psychophysical mea- sures provide a crude means of determining the relative importance of the two effects. In our experiment they indicate that relatively little pain had been induced by the upper arm block by the time that cut-off occurred. It is reasonable, therefore, to conclude that the major determinant of cut-off with this type of block was the decrease in tactile sensitivity. In the case of the wrist block, however, cut-off was not obtained until pain had reached extreme levels. Within the signal
detection framework outlined here, this suggests that the primary determinant of cut-off was not a reduction in tactile sensitivity but rather the increase in pain. The fact that the two subjects (Sl and S4) who reported least pain with the wrist block were the ones who continued to respond correctly to tactile stimulation, even after 100 minutes, supports this view.
The differences between the two types of block are clearly related to differences of anatomy between the upper arm and the wrist. The upper arm contains a single bone against which blood vessels are compressed under applied force. The pressure in the cuff is transmitted to the blood vessels both easily and rapidly. Since this pressure exceeds systolic pressure, ischaemia is induced quickly and with minimal dis- comfort. This is not the case with the wrist cuff. The bones of the wrist form a jointed bracelet. Under applied pressure, they not only grate together painfully, but also provide a cavity into which the blood vessels sink. Consequently, total pressure in the wrist cuff is not transmitted to the blood vessels and systolic pressure is unlikely to be exceeded. This is the cause of the inadequacy of the wrist cuff as an ischaemia-inducing device - a feature reflected in the relatively long cut-off times we obtained. Over the experimental session, the grinding of the wrist bones induces progressively more pain and this leads to the high levels of pain reported by our subjects.
The finding that cut-off times reported in the present experiment are longer than in previous studies was unexpected for two reasons.
(1) The staircase method was employed to ensure that estimates of cut-off time were as accurate as possible. Other psychometric tech- niques are slower to respond to changes in threshold over time and so

K. Greer, N. Harvey / Incomplete and masked effects of nerve block 25
they would be expected to provide less accurate and longer cut-off times than those obtained here.
(2) Many of the cut-off times reported in other studies are estimates of the time to produce kinaesthetic ischaemia. Previously, this has been found to be longer than the time required to produce tactile ischaemia _ the cut-off time reported here.
In previous experiments, sensory cut-off time for the wrist block has been estimated to be of the order of one hour and movement data have been collected soon after that point. If our method of assessing cut-off produces more veracious estimates, then movement data in previous studies may have been collected prematurely.
The results of this experiment convinced us that the wrist block should not be used as a means of eliminating feedback. First, estimates of cut-off probably reflect an increase in pain more than a reduction in tactile sensitivity. Second, the duration of exposure to wrist cuff necessary to induce actual ischaemia would far exceed the maximum exposure time to nerve blocks recommended by medical opinion.
Experiment 2
To examine the contribution of joint and cutaneous feedback to motor control, a cuff is needed that has the ischaemic properties of the upper arm cuff but the logical properties of the wrist cuff. Like the upper arm, the proximal phalanx of the thumb consists of a single bone against which blood vessels could be compressed by an applied pres- sure greater than the subjects’ systolic blood pressure. This would induce ischaemia of the joint and distal phalanx of the thumb, and do so with the minimal pain levels associated with the upper arm cuff. Flexion movements of the distal phalanx are produced by activity in the flexor pollicus longus, a muscle in the forearm. Since this muscle lies proximal to the proposed site of a thumb cuff, such a device should meet both the above criteria.
Marsden et al. (1972) used an elastic band tightly wrapped around the proximal phalanx of the thumb to produce nerve block. However, this method does not allow for exact measurement of the pressure applied to the thumb. Also, in pilot work, we found that it produced

26 K. Greer, N. Harvey / Incomplete and masked effects of netwe block
long-term blood bruising and was painful to the subject. The smallest of the standard sphygmomanometer cuffs cannot be used because it would be too large and, even if a sphygmomanometer cuff of a suitable size were made, it would not be capable of transmitting the required pressure without rupturing the cuff material. Consequently, we decided to have a cuff custom built using a strong rubber that was elastic enough to transmit high pressures without bursting. Experiment 2 was designed to examine cut-off time for tactile stimuli using this cuff and to estimate the levels of pain that it induces.
Method
Apparatus The cuff consisted of a narrow circle of inflatable rubber encased in
a series of rings. The rubber was inserted inside the central cuff body and gripped between two gauge rings. The cuff was held together by two retaining rings placed on either side of the cuff body and screwed together. The rubber insert was inflated from a large compressed air source. For the cuff to be effective, it was important that, in its non-inflated state, it fitted tightly around the proximal phalanx of each subject’s thumb. To achieve this, thumb size was sampled, a set of gauge rings ranging across the sample were produced and each experi- mental subject was fitted with the cuff using the appropriate sized rings. Pilot work indicated that a pressure of approximately 2620 mm Hg was required to induce ischaemia and so in the experiment we decided to use a pressure of 2920 mm Hg. The pressure in the cuff was indicated by a pressure gauge. Separate rubber inserts were used for each subject. Tactile sensitivity was measured with the same set of von Frey hairs as were used in experiment 1.
Subjects There were five male and five female subjects. All were right-handed
and their average age was 25 years. They were screened for skin diseases, diabetes, abnormalities in blood pressure and skin damage.
Procedure Each subject was tested individually in the University Health Centre.
He or she was fitted with the appropriate sized gauge rings before the cuff was assembled. This ensured maximum efficiency of the compres-

K. Grew, N. Harvey / Incomplete and masked effects of nerve block 21
sion block. The subject was then blindfolded and testing proceeded in a manner identical to that outlined for experiment 1.
Results
The ten subjects had a median cut-off time of 34.8 minutes (range 32-41 minutes). This is somewhat less than that obtained for the upper arm cuff in experiment 1. Recovery time was very short (median: 2-3 minutes; range: 2-5 minutes). Subjects reported mild discomfort.
Discussion
The results indicate that the ischaemic properties of the thumb cuff were indeed comparable to those of the upper arm cuff. Only mild discomfort was reported, making it likely that cut-off was predomi- nantly due to a decrease in tactile sensitivity rather than to an increase in pain. We would argue therefore that the thumb cuff is more appropriate than the wrist cuff for examining the contribution of joint and cutaneous feedback to motor control. Previous work with a wrist cuff has been taken to indicate that the production of skilled movement is not dependent on these types of feedback. In Kelso’s (1977) first experiment, for instance, performance under wrist cuff conditions was worse than that under no-cuff conditions for all the movement ranges examined but in no case did the difference reach significance. Conse- quently, Kelso concluded that neither encoding nor reproducing these movements was dependent on joint or cutaneous receptor output. In experiment 3, we attempted to replicate these findings using a thumb cuff. In our experiment, we included an additional condition that allowed us to estimate the size of any central stress-related effects of cuff-induced pain on performance. In all previous experiments, these effects have been confounded with those arising from reduced joint and cutaneous sensitivity.
Experiment 3
Kelso (1977) examined reproduction of criterion movements that had been preselected by the subject from a movement range specified by the experimenter. In our experiment, also, movement extent was not

28 K. Grew, N. Harvey / Incomplete and masked effects of nerve block
physically constrained by the experimenter but preselected by the subject on the basis of verbal instructions given prior to the session. However, in our case, subjects were told to preselect movements as close to 20 degrees as possible and were given verbal feedback as to the actual extent of movement after each trial. Absolute error relative to the 20-degree target movement was recorded.
Laszlo and Bairstow (1971b) have pointed out that cuff application can be upsetting and even induce fainting in some subjects. However, for the population as a whole, the discomfort produced by the thumb cuff is best characterised as a mild stressor. Repetitive finger movement is a fairly simple monotonous task not demanding a division or broad spread of attention and, typically, mild stressors tend to improve performance in such tasks (Broadbent 1971; Hockey 1979; Kahneman 1973). Thus, the difference between cuff and no-cuff conditions ob- served by Kelso (1977) may have failed to reach significance because additional stress-induced arousal improved performance and partially compensated for the deficits arising from nerve block. If cuff applica- tion on a moving hand produces arousal that reduces the size of impairment due to nerve block, then cuff application on the other non-moving hand would be expected to improve performance. This is because the subject’s movements would be produced with intact joint and cutaneous feedback and the positive effects on performance of arousal induced by the cuff would not be counteracted by negative effects of removal of feedback.
We examined three groups of subjects. The experimental group (E) had the cuff inflated on the moving thumb; the control group (C) had the cuff inflated on the thumb of the other hand and a third group (0) wore a non-inflated cuff. (Half of group 0 had the non-inflated cuff on the non-moving thumb, while the other half wore it on the moving thumb.) If, as postulated for Kelso’s (1977) experiment, arousal effects do reduce the difference between E and 0 groups to below significance levels, then they would be expected to result in the ordering of absolute error as follows: E > 0 > C. This is the hypothesis we tested.
Method
Apparatus The subject’s forearm rested on a foam covered table. The subject’s
wrist was strapped to a plywood board that was clamped to the table.

K. Greer, N. Harvey / Incomplete and masked effects of nerve block 29
A foam-covered metal structure, mounted on the board, supported the palm and fingers of the subject’s right hand so that the palm was facing downwards in a cupped position above the horizontal movement range of the top phalanx of the thumb. (When the hand is cupped in this position of palmar adduction, no muscles other than the flexor pollicus longus should contribute to the movement (Haymaker and Woodhall 1953).) A balsa wood pointer was attached to the thumb nail with epoxy five minute glue. This pointer moved above and parallel to a large protractor so that the experimenter, who sat opposite the subject, could read the angle moved by the top phalanx of the thumb.
A perspex vice was also fixed to the plywood board. For subjects in the E condition and for half the subjects in the 0 condition, it held the thumb pressure cuff which encircled the proximal phalanx of the right thumb. For subjects in condition C, and for the remainder of the subjects in condition 0, the vice was used to maintain the proximal phalanx of the right thumb in a fixed position, while the thumb cuff encircled the proximal phalanx of the left hand thumb. In the E and C conditions, the cuff was inflated but in the 0 condition, it was not.
Subjects Sixteen right-handed male subjects were paid to participate in the
experiment. Ages ranged form 20-35 years and all were medically screened prior to the experiment.
Design Four subjects were assigned each to groups E and C. Of the 8
subjects in the 0 condition, 4 underwent a procedure identical to the E subjects but without the cuff inflated, whereas the remainder under- went a procedure identical to the C subjects but without the cuff inflated. Subjects in all conditions received 5 training and twenty test trials.
Procedure Subjects were again tested individually. First, the task was explained
to each subject. He was then fitted into the apparatus and blindfolded with a strip of black cloth to eliminate visual cues. The thumb pressure cuff was placed on the proximal phalanx of the appropriate thumb. For both E and C condition subjects the cuff was inflated to 2920 mm Hg. After 25 minutes, the von Frey pressure aesthesiometer was used to observe the final decline in tactile sensitivity. Although sensory cut-off

30 El. Greer, N. Harvey / Incomplete and masked effects of nerue block
occurred at approximately 35 minutes after cuff inflation (cf. experi- ment 2) movement training and testing did not commence until 45 minutes after cuff application. This was to ensure that joint as well as cutaneous sensitivity was at an asymptotically low level. A movement of 20 degrees was demonstrated to the subject by asking him to move his thumb slowly from a previously determined starting point and telling him when the flexion reached 20 degrees. After five of these training trials, testing began. The subject was instructed to make a 20-degree flexion movement of the right hand thumb on command from the experimenter. It was stressed that he was to say when he had finished the movement. After the angle of flexion had been recorded and the subject had been given feedback concerning his performance, he was told to return to the starting position. After the experimenter had checked that this had been accomplished, the next trial started. Data were recorded from twenty such trials. Subjects in the 0 condi- tion went through essentially the same procedure as those in the other conditions except that the cuff was never inflated.
Results
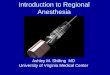
Fig. 1 shows the median absolute error in each of the three condi- tions.
We wished to test whether the ordering of the errors in the three groups was E > 0 > C against the null hypothesis that there was no difference between them. A z test appropriate for this purpose (Meddis 1984) was carried out and the results were significant (z = 1.64; p < 0.05). In contrast, an a priori test of the specific hypothesis that errors were greater in the E than in the 0 group failed to reach significance (z = 1.02; p > 0.05) (cf. Kelso 1977). Thus, taken together, these analyses indicate that inflating a cuff around a moving body segment may fail to produce a significant increase in movement error not because there are no detrimental peripheral effects of the cuff but because these effects are masked by beneficial centrally mediated ones.
Discussion
After 35 minutes application of the nerve block to the proximal phalmax of the thumb, subjects were unable to report input from the distal phalanx. Movement testing did not start until ten more minutes

K. Greer, N. Harvey / Incomplete and masked effects of nerve block 31
E 0 C EXPERIMENTAL CONDITION.
Fig. 1. Experiment 3: Median absolute error for subjects with inflated cuff on moving hand (E), with inflated cuff on non-moving hand (C) and with non-inflated cuff (0).
had elapsed but the nerve block still failed to produce a significant impairment relative to the condition where the cuff was not inflated. Thus, results from our thumb cuff experiment replicated those that Kelso (1977) obtained with a wrist cuff. Nevertheless, they should not be interpreted as indicating that joint and cutaneous feedback have no role in the encoding and reproduction of movement. This is because of our additional finding that there was a significant ordering of the three conditions such that performance was best with an inflated cuff on the non-moving thumb, intermediate with a non-inflated cuff and worst with an inflated cuff on the moving thumb. This ordering implies that cuff inflation has a beneficial central effect as well as a detrimental peripheral one.
If these two effects are additive, an estimate of the true peripheral impairment produced by inflating the cuff on the moving thumb could be obtained by adding the estimate of central facilitation (i.e., 0 - C) to the observed peripheral impairment (i.e., E - 0). Thus, in the present experiment, true peripheral impairment would be estimated to produce a 31.5’ rather than a 18’ increase in absolute error. This

32 K. Greer, N. Harvey / Incomplete and masked effects of nerve block
additive model implies that Kelso (1977) may have seriously under- estimated the true peripheral impairment produced by the wrist cuff. This, in turn, casts doubt on his conclusion that joint and cutaneous feedback do not contribute to movement encoding and reproduction. There may, of course, be some reason why this additive model does not hold. For instance, moving may either increase or decrease the pain caused by the cuff. This would mean that the amount of pain-induced central facilitation would depend on whether the cuff was on the moving or non-moving hand.
General discussion
Pain induction by ischaemia is an experimental technique favoured by many pain researchers (e.g., Aberger et al. 1983; Clark and Hunt 1971; Johnson 1973; Smith et al. 1966). They argue that muscle ischaemia produces the closest approximation to clinical pain. Relative to other forms of laboratory-induced pain, ischaemic pain increases gradually over a comparatively long period and it responds to the analgesic drugs commonly used to treat clinical pain. Furthermore, certain types of clinical pain are thought to arise from ischaemic conditions (Ylikorkala and Dawood 1978). Movement scientists who have used cuffs to attenuate joint and cutaneous feedback appear to have been unaware of their use in pain research. Only occasionally do they mention the painful aspects of the cuffs (Laszlo and Bairstow 1971a, b), and none have attempted to analyse the effects of cuff-in- duced pain on movement performance. What follows is a preliminary attempt at such an analysis.
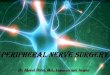
Pain experience is usually conceptualised as having a sensory dis- crimination component and a reactive component (Beecher 1959; Casey and Melzack 1967; Melzack and Wall 1965). The emotional properties of the reactive component include arousal and aversion. Fig. 2 sum- marises our account of the effects of these components of pain on the psychometric and movement responses examined by researchers inter- ested in the role of joint and cutaneous feedback in motor control.
Effects of pain on assessment of sensory cut-off
The psychometric response is used to assess sensory cut-off. We argued above that signal detection theory (Green and Swets 1966; Egan

K. Greer, N. Harvey / Incomplete and masked effects of nerue block 33
I i AROUSAL
I
AVERSION
I +’ t JOINT C _RIN MOVEMENT RETRIEVAL OF SENSORY FORtlULATloN OF
AND U RECEPTORS
FORMULATION MOTOR PROGRAMS IllSCRlMlNATlON DETECTION
CUTANEOUS F MUSCLES _ AN0 FROM LONG-TERM REFLECTED RESPONSE
RECEPTORS - F AND THEIR SPINDLES - ‘ONTRoL MEMORY BY d’ REFLECTED BY p
7- 1 i 1
AND C”iw I
Fig. 2. Model of the effects of pain on the assessment of sensory cut-off and on the performance
of movement tasks.
1978) provides an appropriate framework for discussing the psycho- logical processes responsible for producing this response. Subjects have to distinguish trials in which pain alone is present from trials in which both pain and a tactile stimulus are present. Pain alone trials may be conceptualised as producing a normal distribution of values along some internal dimension related to subjective intensity of stimulation. Trials in which both pain and a tactile stimulus are present also produce a normal distribution of values along this dimension but do so around a higher mean value. The two distributions overlap to a greater or lesser degree. On each trial, a value is produced somewhere along the dimen- sion and the subject’s task is to decide to which of the two distributions it belongs. Because of the overlap in the distributions, false negatives and false positives are bound to occur but they are less likely when the distributions are well separated. The distance between the means of the two distributions scaled by their standard deviation is known as d’ and provides an estimate of the sensory abilities contributing to the psycho- metric response. d’ may decrease not only because of a decline in the intensity of the tactile signal but also because of an increase in the level of pain. Only when subjects report no increase in the level of pain can a drop in signal detectability be attributed solely to a reduction in tactile sensitivity. Given the pain inducing properties of ischaemic cuffs, it is unlikely that subjects would give such reports and therefore doubtful that such an attribution could ever be made.
In order to decide whether trials belong to the pain plus tactile signal distribution or to the pain alone distribution, subjects set a response criterion (,f?) at some point along the dimension. Only trials which

34 K. Greer, N. Harvey / Incomplete and masked effects of nerue block
produce values greater than fi lead to a response of ‘tactile signal present’. Factors such as tactile signal probability and the pay-offs associated with correct positives and negatives and with false positives and negatives affect the positioning of this criterion. In ischaemic cuff experiments where subjects know that stimuli will be presented until no signals are detected, the increasing pain provides an increasingly strong negative pay-off for positive responses. Thus, as pain increases, its aversive properties ensure that the response criterion, /3, becomes higher and higher. Consequently, the overall level of sensory stimula- tion necessary for a positive response to tactile stimuli becomes greater as the experiment progresses.
In summary, increases in pain lead simultaneously to a decrease in d’ and an increase in /3. When subjects report heightening levels of pain, it is impossible to ascertain the extent to which sensory cut-off is caused by one of these changes and the extent to which it is caused by a reduction in d’ associated with decreased tactile signal strength.
Effects of pain on production of movements
Pain may produce arousal in order to enhance a subject’s efforts to escape from its source. The Yerkes-Dodson Law (Yerkes and Dodson 1908) was originally formulated as an account of the relationship between intensity of electric shock and discrimination ability but it has since received qualified acceptance as a general expression for the effect of arousal on performance. For simple tasks, such as the ones under consideration here, optimum arousal level is higher than for more complex tasks. It is not surprising, therefore, that the mild discomfort produced by the thumb cuff was shown to benefit perfor- mance in experiment 3. This finding is consistent with recent investiga- tions of the Yerkes-Dodson Law which show that mild stressors tend to improve performance in fairly simple monotonous tasks that do not demand a division or broad spread of attention (Broadbent 1971; Hockey 1979; Kahneman 1973).
The effect of arousal on performance compounds the difficulties faced by researchers who use ischaemic cuffs to assess the importance of kinaesthetic feedback in motor control. However, the inclusion of a control condition of the type used in experiment 3 may give some idea of the size of the arousal effect resulting from application of the cuff.

K. Grew, N. Harvey / Incompleie and masked effects of nerve block 35
In summary, a nerve compression cuff that attenuates joint and cutaneous feedback may have no observable detrimental effects on motor control for one of two reasons. It may be that those types of feedback are just not necessary in the encoding and reproduction of movement (cf. Kelso 1977). Alternatively, they may be employed, but beneficial centrally-mediated changes in arousal, consequent on cuff- induced pain, may compensate for all or some of the impairment arising from their attenuation.
References
Aberger, E.W., D.R. Denney and D.F. Hutchings, 1983. Pain sensitivity and coping strategies among dysmenorrheic women: much ado about nothing. Behaviour Research and Therapy 21, 119-127.
Beecher, H.K., 1959. Measurement of subjective responses: qualitative effects of drugs. New York: Oxford University Press.
Broadbent, D.E., 1971. Decision and stress. London: Academic Press. Brown, E.L. and K. Deffenbacher, 1979. Perception and the senses. New York: Oxford University
Press. Casey, K.L. and R. Melzack, 1967. ‘Neural mechanisms of pain: a conceptual model’. In: E.
Leong Way (ed.), New concepts in pain and its clinical management. Philadelphia, PA: Davis. Clark, W.C. and H.F. Hunt, 1971. ‘Pain’. In: J.A. Downey and R.C. Darling (eds.), Physiological
bases of rehabilitative medicine. Philadelphia, PA: Saunders. Egan, J.P., 1978. Signal detection theory and ROC analysis. New York: Academic Press. Goodwin, G.M., D.I. McCloskey and P.B.C. Matthews, 1972. The contribution of muscle
afferents to kinaesthesis shown by vibration induced illusions of movement and by the effects of paralyzing joint afferents. Brain 95, 705-748.
Green, D.M. and J.A. Swets, 1966. Signal detection theory and psychophysics. New York: Wiley. Haymaker, W. and B. Woodhall, 1953. Peripheral nerve injuries: principles of diagnosis. Phila-
delphia, PA/London: Saunders. Hockey, G.R., 1979. ‘Stress and the cognitive components of skilled performance’. In: V.
Hamilton and P.M. Warbuton (eds.), Human stress and cognition: an information-processing approach. New York: Wiley.
Johnson, J.E., 1973. Effects of accurate expectations about sensations on the sensory and stress components of pain. Journal of Personality and Social Psychology 27, 261-275.
Jones, B., M. Planes and T. Anwza, 1982. Painfulness decreases discriminability of electric shock. Perception and Psychophysics 32, 187-191.
Kahneman, D., 1973. Attention and effort. Englewood Cliffs, NJ: Prentice-Hall. Kelso, J.A.S., 1977. Motor control mechanisms underlying human movement production. Journal
of Experimental Psychology: Human Perception and Performance 3, 529-543. Kelso, J.A.S. and K.G. Holt, 1980. Exploring a vibratory systems analysis of human movement
production. Journal of Neurophysiology 43, 1183-1196. Kelso, J.A.S., G.E. Stelmach and W.M. Wanamaker, 1974. Behavioral and neurological parame-
ters of the nerve compression block. Journal of Motor Behaviour 6, 179-190. Kelso, J.A.S., S.A. Wallace, G.E. Stelmach and G.A. Weitz, 1975. Sensory and motor impairment
in the nerve compression block. Quarterly Journal of Experimental Psychology 27, 1233129.

36 K. Grew, N. Harvey / Incomplete and masked effects of nerue block
Laszlo, J.I., 1966. The performance of a simple motor task with kinaesthetic sense loss. Quarterly
Journal of Experimental Psychology 18, 1-8.
Laszlo, J.I., 1967. Training of fast tapping with reduction of kinaesthetic, tactile, visual and
auditory sensations. Quarterly Journal of Experimental Psychology 19, 344-349.
Laszlo, J.I. and P.J. Bairstow, 1971a. Accuracy of movement, peripheral feedback and efference
copy. Journal of Motor Behaviour 3, 241-252.
La&o, J.I. and P.J. Bairstow, 1971b. The compression block technique: a note on procedure.
Journal of Motor Behaviour 3, 313-317.
Malow, R.M., L. Grimm and R.E. Olsen, 1980. Differences in pain perception between myofascial
pain dysfunction patients and normal subjects: a signal detection analysis. Journal of Psycho-
somatic Research 24, 303-309.
Marsden, C.D., P.M. Merton and H.B. Morton, 1972. Servo action in human voluntary move-
ment. Nature 238, 140-143.
Meddis, R., 1984. Statistics using ranks: a unified approach. Oxford: Blackwell.
Melzack, R. and P.D. Wall, 1965. Pain mechanisms: a new theory. Science 150, 971-979.
Merton, P.A., 1964. Human position sense and sense of effort. Symposium of the Society of
Experimental Biology 18, 387-400. Roy, E.A. and I. Williams, 1979. ‘Memory for location and extent: the influence of reduction of
joint feedback information’. In: G.C. Roberts and K.M. Newell (eds.), Psychology of motor
behaviour and sport - 1978. Champaign, IL: Human Kinetics Publisher.
Shipley, E.F., 1959. Cueing as a determiner of apparent variability in sensitivity. Massachusetts
Institute of Technology: Research Laboratory of Electronics, Quarterly Progress Report No.
53; and Journal of the Acoustical Society of America 31, 834.
Sinclair, P.C. and J.R. Hinshaw, 1951. Sensory phenomena in experimental nerve block. Quarterly
Journal of Experimental Psychology 3, 49-72.
Smith, G.M., L.D. Egbert, R.A. Markowitz, F. Mosteller and H.K. Beecher, 1966. An experimen-
tal pain method sensitive to morphine in man: the submaximum effort tourniquet technique.
Journal of Pharmacology and Experimental Therapy 154, 324-332.
Sunderland, S.A., 1951. A classification of peripheral nerve injuries producing loss of function.
Brain 74, 491-516. Yerkes, R.M. and J.D. Dodson, 1908. The relation of strength of stimulus to rapidity of
habit-formation. Journal of Comparative Neurology and Psychology 18, 459-482.
Ylikorkala, 0. and M. Dawood, 1978. New concept in dysmenorrhea. American Journal of
Obstetrics and Gynecology 130, 833-847.