Embed Size (px)
Citation preview

Paediatric NAFLD
Prof. Alastair Baker
Paediatric Liver Centre
King’s College Hospital
Potential Conflict: Unrestricted educational grant from Mirum Pharma

Fatty Liver Disease - the New Epidemic
0
8
15
23
30
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
NAFLD Age at referral
2002I992 19981994 2006 2010 2014 2018
NAFLD
New Referrals
To KCH 2015-16
Fatty liver disease in children. Aw M, Baker AJ, Dhawan A. Arch Dis Child. 2004 Jul;89(7):648-52.
118

• By 2030 the world population of obese children and adolescents
• is predicted to grow to 254 million – an increase of more than 60%
• There will be nearly 62 million obese children aged five to 19 in China by 2030,
• 27 million in India and 17 million in the US
• In the UK, 1.3 million children and adolescents will be obese by 2030
• “Governments are acting slowly or not at all, and there is strong resistance to
• intervening against commercial interests”
• “Multinational companies worldwide are making cheap food in bulk that has pushed out more nutritious foods from the market pl
World Obesity Federation, compiled data in the first Childhood Obesity Atlas

The highest rates of obesity are shown in red, followed by orange and yellow.
Green and blue means fewer than 5% of the young population is obese
Child and teen obesity spreading across the globe
World Obesity Federation, compiled data in the first Childhood Obesity Atlas

• Steatosis with or without inflammation and fibrosis, in the absence of a
known inherited metabolic defect or toxins and associated in the majority with
central obesity and insulin resistance
Definition - NAFLD/NASH

Goh and McCullough. Dig Dis Sci 2016
7
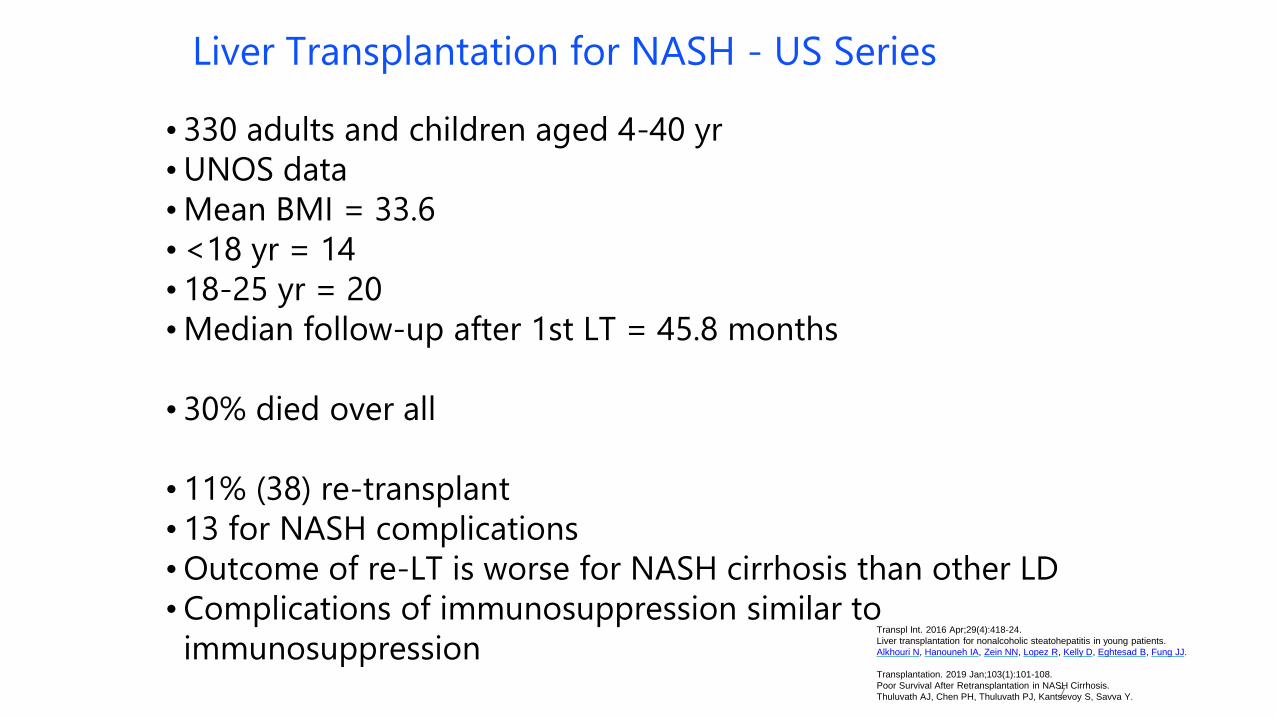
Liver Transplantation for NASH - US Series
• 330 adults and children aged 4-40 yr
• UNOS data
• Mean BMI = 33.6
• <18 yr = 14
• 18-25 yr = 20
• Median follow-up after 1st LT = 45.8 months
• 30% died over all
• 11% (38) re-transplant
• 13 for NASH complications
• Outcome of re-LT is worse for NASH cirrhosis than other LD
• Complications of immunosuppression similar to
immunosuppressionTranspl Int. 2016 Apr;29(4):418-24.
Liver transplantation for nonalcoholic steatohepatitis in young patients.
Alkhouri N, Hanouneh IA, Zein NN, Lopez R, Kelly D, Eghtesad B, Fung JJ.
Transplantation. 2019 Jan;103(1):101-108.
Poor Survival After Retransplantation in NASH Cirrhosis.
Thuluvath AJ, Chen PH, Thuluvath PJ, Kantsevoy S, Savva Y.
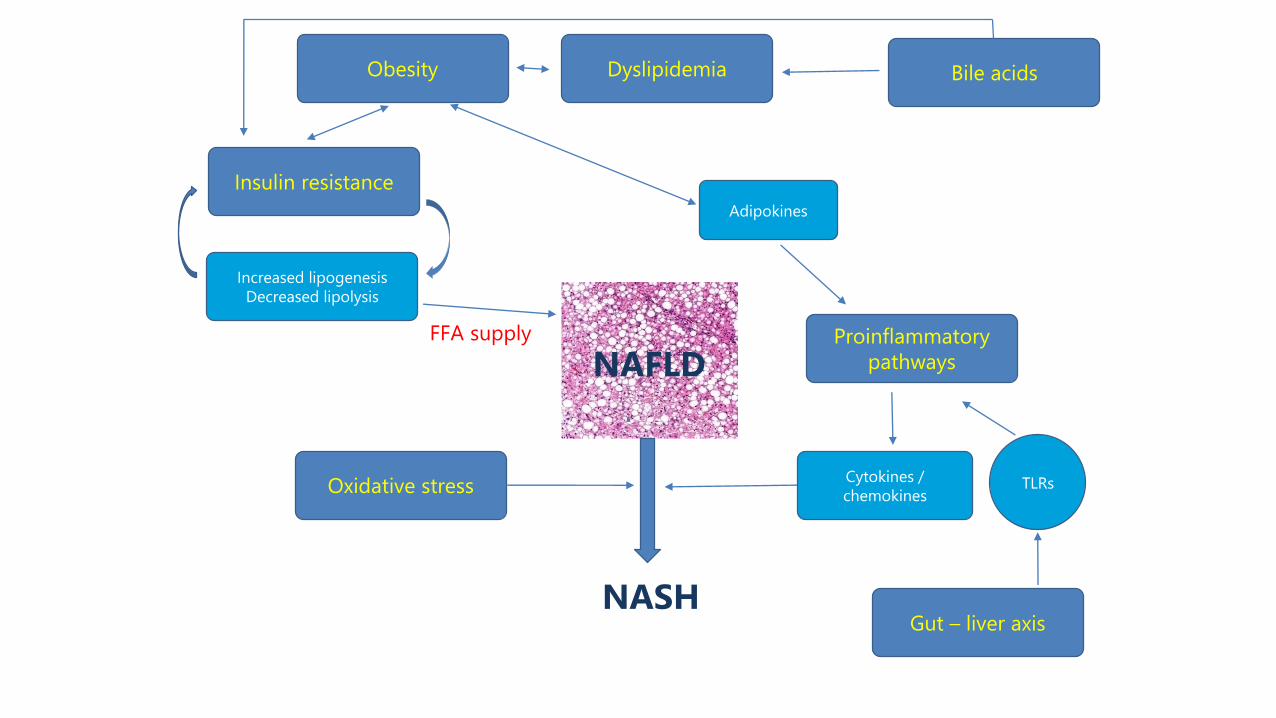
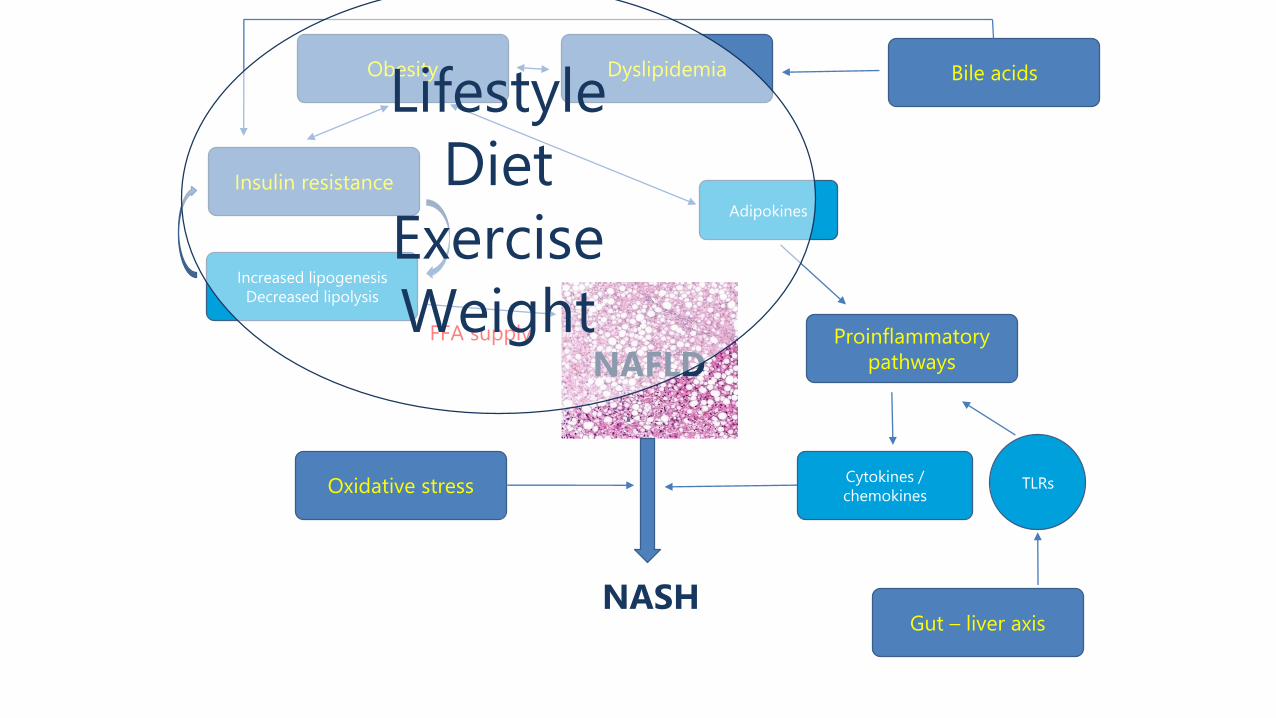
Proinflammatory
pathways
Insulin resistance
Bile acidsDyslipidemiaObesity
Adipokines
Cytokines /
chemokinesOxidative stress
Increased lipogenesis
Decreased lipolysis
FFA supply
NAFLD
NASHGut – liver axis
TLRs

Proinflammatory
pathways
Insulin resistance
Bile acidsDyslipidemiaObesity
Adipokines
Cytokines /
chemokinesOxidative stress
Increased lipogenesis
Decreased lipolysis
FFA supply
NAFLD
NASHGut – liver axis
TLRs
Genes
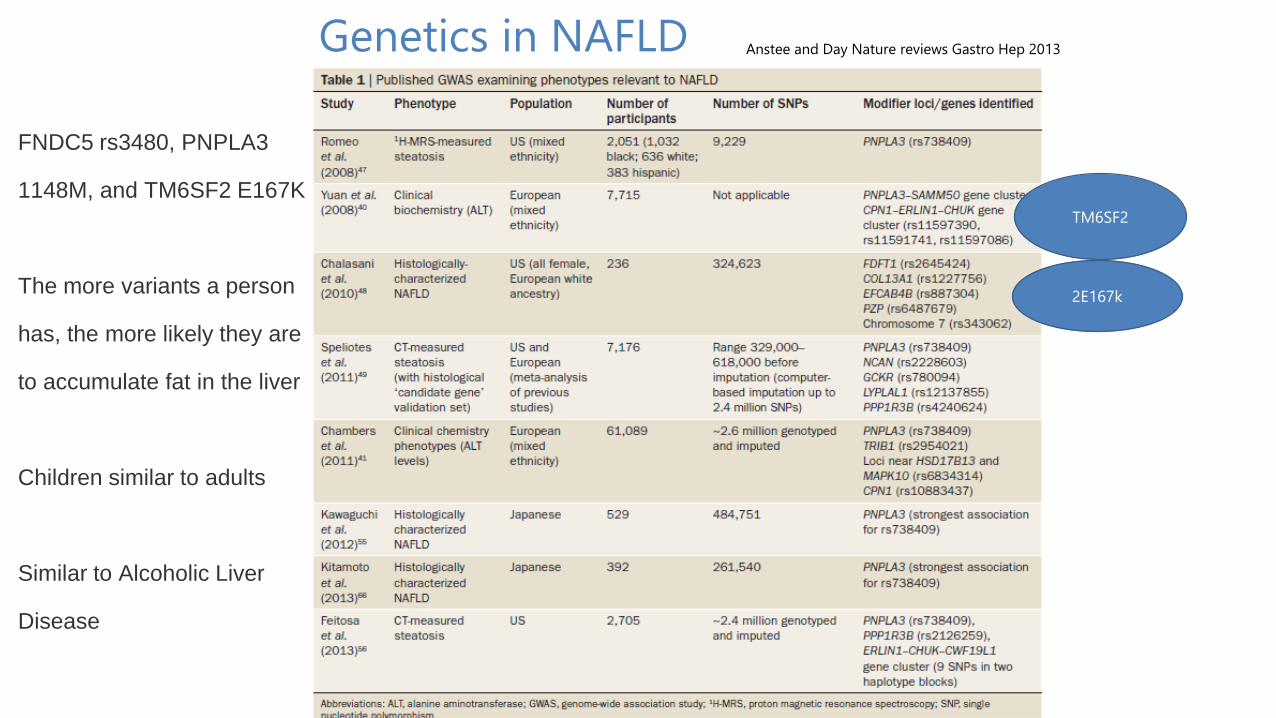
FNDC5 rs3480, PNPLA3
1148M, and TM6SF2 E167K
The more variants a person
has, the more likely they are
to accumulate fat in the liver
Children similar to adults
Similar to Alcoholic Liver
Disease
Genetics in NAFLD Anstee and Day Nature reviews Gastro Hep 2013
TM6SF2
2E167k
Proinflammatory
pathways
Insulin resistance
Bile acidsDyslipidemiaObesity
Adipokines
Cytokines /
chemokinesOxidative stress
Increased lipogenesis
Decreased lipolysis
FFA supply
NAFLD
NASHGut – liver axis
TLRs
Lifestyle
Diet
Exercise
Weight

Dietary intake as a risk factor for NAFLD
Fan et al 2014
‘Autistic’ dietary preferences seem to be a factor in children

Protocol at KCH
Investigation of a child of young person with fatty liver
• NAFLD is a diagnosis of exclusion
• KCH Protocol based on ESPGHAN Guidelines
• Often in presence of other features: metabolic syndrome (overweight, insulin resistance, hypertension, hyperlipidemia)
• FH of complications of metabolic syndrome
• Essential to exclude other treatable causes
• Even in childhood patients may have two conditions

Table 1
TABLE 2. Causes of fatty liver disease in childrenGeneral or systemic Genetic-metabolic causes Other rare hereditary causes Drugs’ hepatotoxicity
Acute systemic disease CF Alstrom syndrome Ethanol
Acute starvation Swachmann Sy Bardet-Biedl syndrome Ecstasy, cocaine
Protein-energy malnutrition Wilson D Prader-Willi syndromeNifedipine
Total parenteral nutrition A-1-ATD Cohen syndrome Diltiazem
METABOLIC SYNDROME Galactosaemia Cantu syndrome (1p36 deletion)Estrogens
Polycystic ovary syndrome Fructosaemia Weber-Christian disease Corticosteroids
Obstructive Sleep apnoea Wolman/LALD Citrin deficiency Amiodarone
Rapid weight loss GSD 1 & 1V Dorfmann- Chanarin SyndromePerhexiline
Anorexia Nervosa FAOD - Mitochondrial and peroxisomal Coralgil
Cachexia Madelung Lipomatosis Tamoxifen
IBD LipodystrophiesMethotrexate
Coeliac disease Abeta or hypobetalipoproteinemia Prednisolone
Nephrotic syndrome Organic acidaemias Valproate
Type 1 DM a- and b-oxidation defects L-asparaginase
Mauriac Syndrome Porphyria cutanea tarda Zidovudine
Bacetrial overgrowth Homocystinuria HIV treatments
Thyroid disorders Familial hyperlipoproteinemias Solvents
Endocrine disorders - adrenal eg. Tyrosinemia type 1 Pesticides
Bile acid synthesis defects
Congenital disorders of glycosylation
Turner syndrome
HFE (hemochromatosis)
Causes of fatty liver in children - ESPGHAN Guidelines

NAFLD management protocol
• Local liver work-up, anthropometry, social and diet history
• Referral to NAFLD specialist clinic
• Specific dietetic review and recommendations
• Local provision of lifestyle modification
• Insulin resistance and significant disease on biopsy or impaired glucose tolerance –trial of metformin in consultation with endocrinology team (1 – 2 years and repeat OGTT)
• Bariatric surgery MDT (BMI > 40 and ‘keen’)
• Ideally individual or family psychological support – this has only been possible on a research basis previously
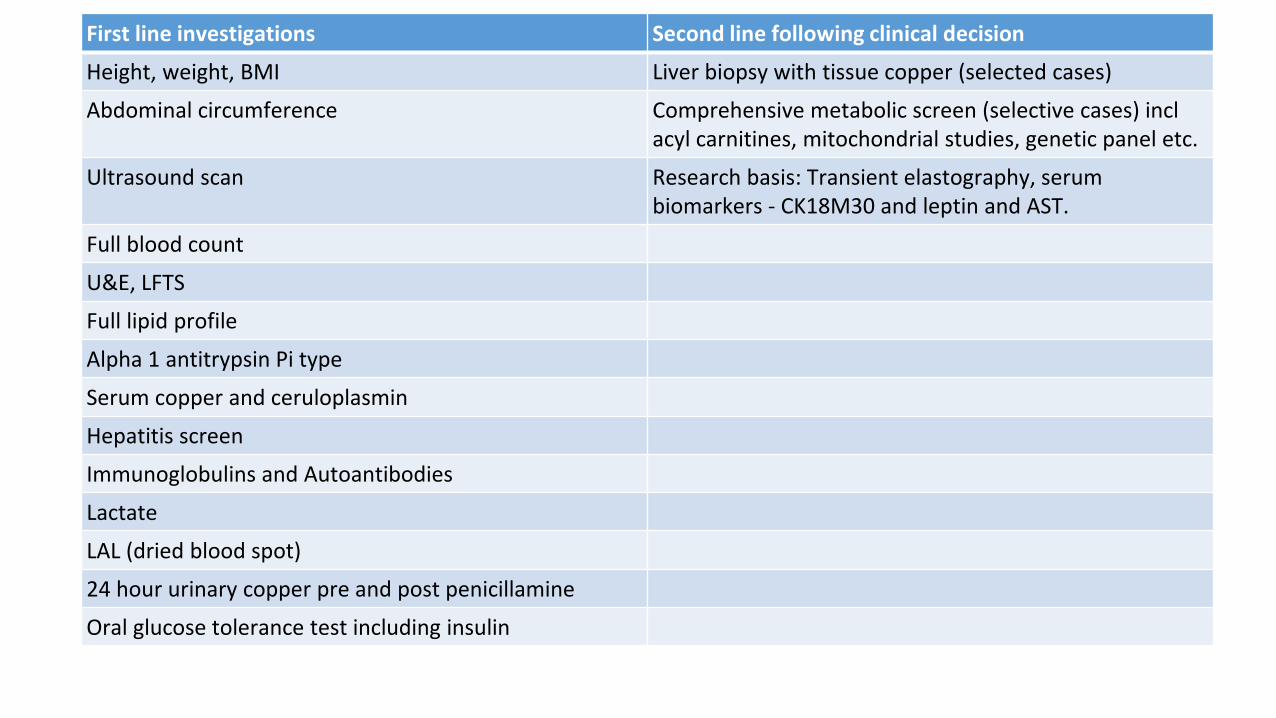
First line investigations Second line following clinical decision
Height, weight, BMI Liver biopsy with tissue copper (selected cases)
Abdominal circumference Comprehensive metabolic screen (selective cases) incl acyl carnitines, mitochondrial studies, genetic panel etc.
Ultrasound scan Research basis: Transient elastography, serum biomarkers - CK18M30 and leptin and AST.
Full blood count
U&E, LFTS
Full lipid profile
Alpha 1 antitrypsin Pi type
Serum copper and ceruloplasmin
Hepatitis screen
Immunoglobulins and Autoantibodies
Lactate
LAL (dried blood spot)
24 hour urinary copper pre and post penicillamine
Oral glucose tolerance test including insulin

KCH workload Jan 2015 – Dec 2016
NAFLD attendances 2015 2016
Number of visits total 300 354
- Number of patients 156 175
- Number of new patients 50 66
Number of visits OPD 174 192
Number of visits Day Case 115 128
Number of visits Inpatient 11 34
Number of attendances per pt. 2015 2016
Number of patients with 1 visit 64 78
Number of patients with 2 visits 60 70
Number of patients with 3 visits 23 21
Number of patients with 4 visits 9 6
Number of patients with 5 visits 1 0

Referral patterns - KCH Patients
Reason for referral Number of patients
Obese plus abnormal liver enzymes
6 (3%)
Obese plus steatosis on USS 7 (4%)
Abnormal liver enzymes 2 (1%)
Steatosis on US 72 (41%)
Abnormal liver enzymes plus steatosis on US
80 (45%)
Other 2 (1%)
Other plus steatosis on US 6 (3%)
Referral source Number of patients
Primary care 9 (5%)
Secondary care 166 (95%)
Presenting sx Number of patients
Abdominal pain 127 (73%)
Incidental 48 (27%)

Co-existing conditions and family history
Co-existing condition Number of patients
Turner syndrome 1
Sotos syndrome 1
Bardt Biedl 1
Becker MD (new) 1
ApoB (new) 1
Autism 8
AIH 1
Optic gliomas 2
Panhypopiituitarism 1
Anxiety / Depression 9
Alpha 1 AT deficiency 1
Family history Number of patients
Type 2 DM 66 (documented) 38%

Protocol – Investigations performed N (%) at 1st visit N (%) by subsequent visit
Height, weight, BMI 174 (99%) 173 (100%)
Abdominal circumference 38 (22%) 69 (40%)
Ultrasound scan 175 (100%) 173 (100%)
Full blood count 175 (100%) 173 (100%)
U and E, LFTS 175 (100%) 173 (100%)
Full lipid profile 175 (100%) 0
Alpha 1 antitrypsin Pi type 175 (100%) 0
Serum copper and ceruloplasmin 175 (100%) 0
Hepatitis screen 175 (100%) 0
Immunoglobulins and Autoantibodies 175 (100%) 0
LAL (dried blood spot) 20 (11%) 50 (29%)
24 hour urinary copper 0 170 (98%)
Oral glucose tolerance test 0 148 (85%) (3 scheduled)
Liver biopsy with tissue copper 0 71 (41%)
Comprehensive metabolic screen 0 5 (3%)
Fibroscan 0 3 (2%) * introduced
Non invasive markers 0 0 ** research

Results – ultrasound
100%
Degree of steatosis on Ultrasound
100%
Splenomegaly on ULtrasound

Glucose Intolerance - OGTT
Number of patients (%)
Insulin resistance (fasting insulin > 15mIU/l) 90/146 (62%)
Impaired fasting glucose (fasting BG > 6.7mmol/l) 1
Impaired glucose tolerance (2 our PP BG > 7.8 mmol/l)
25/146 (17%)

Follow up at KCH
Follow up interval Number of patients (%)
3 monthly 2 (1%)
6 monthly 126 (72%)
9 monthly 3 (2%)
12 monthly 17 (10%)
2 yearly 1 (0.5%)
Discharged (normalised, 1 DNA) 13 (7%)
Local follow up 1 (0.5%)
Transition KCH 6 (3%)
Transition locally 5 (3%)
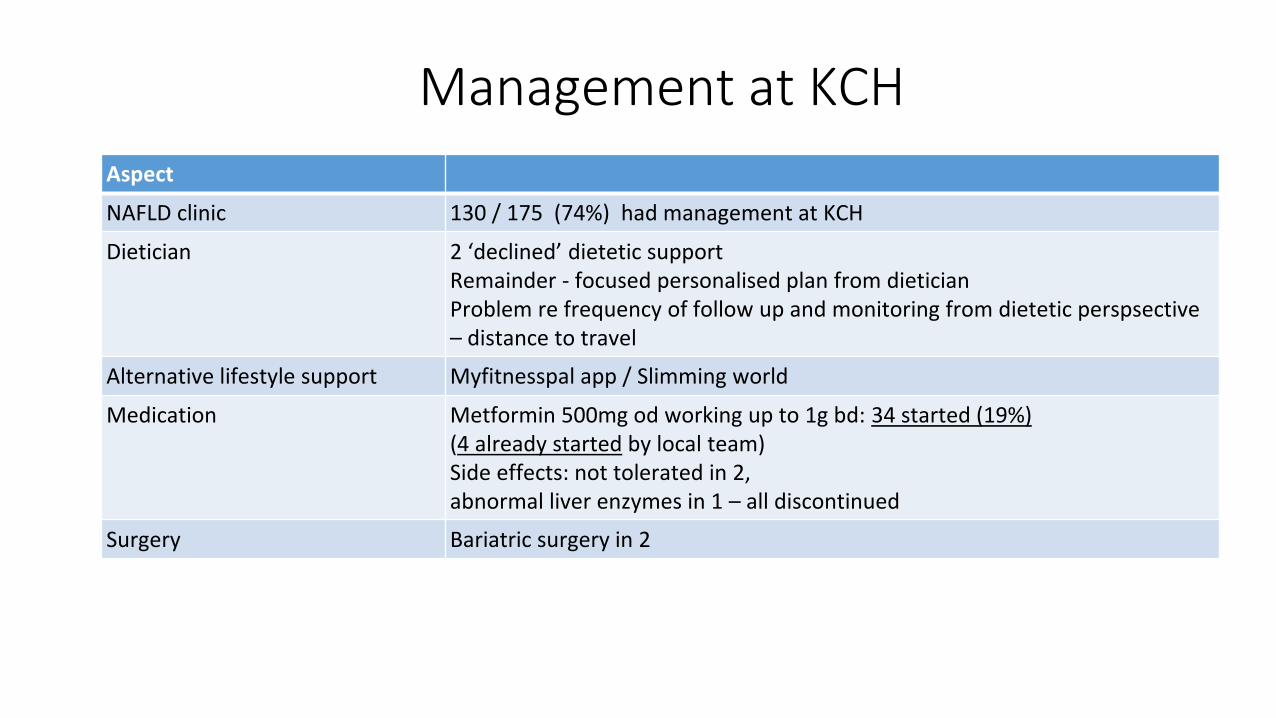
Management at KCH
Aspect
NAFLD clinic 130 / 175 (74%) had management at KCH
Dietician 2 ‘declined’ dietetic supportRemainder - focused personalised plan from dietician Problem re frequency of follow up and monitoring from dietetic perspsective – distance to travel
Alternative lifestyle support Myfitnesspal app / Slimming world
Medication Metformin 500mg od working up to 1g bd: 34 started (19%)(4 already started by local team) Side effects: not tolerated in 2, abnormal liver enzymes in 1 – all discontinued
Surgery Bariatric surgery in 2

Fatty Liver Investigation: Decision for Liver Biopsy

Liver biopsyIndication for liver biopsy• Persistently abnormal transaminases / persistent
splenomegaly
• Suspicion of severity
• Suspicion of alternative diagnosis - normal BMI
Fatty Liver Investigation: Decision for LiverBiopsy

Type 1 NAFLD- commoner in adults

Type 2 NAFLD-commoner in children
67% ≥F2
fibrosis

Differences: Adults vs. Children
• Antenatal priming: liver as a store for fat in obesogenic environment in utero
Brumbagh 2013
• Dietary differences: children are highest consumers of fructose Sluik 2014, Vos 2008
• Ductular reaction & the maturing liver Swiderska-Syn 2013
• Type 2 pattern implies more severe disease Brunt 2009
• Liver injury significant at diagnosis Fitzpatrick 2010, Molleston 2014, Alkhouri 2013

Liver biopsy: n=71
0
13
25
38
50
None Mild Moderate Severe No info
Steatosis on liver biopsy
0
8
15
23
30
None Mild F1Moderate F2Bridging F3 F4 no info
Fibrosis on liver biopsy
0
13
25
38
50
63
None Mild Moderate Severe No score
Inflammation on liver biopsy
71 / 175 (41%) underwent liver biopsy under IV sedation (68) or GA (3) One failed biopsy on first attempt - rebooked
No other complications reported in this cohort
Summary KCH
• NAFLD approx. 175 children in follow up annually, 2/3 in NAFLD clinic
• Protocol adhered to mostly, but abdominal circumference and full OGTT sometimes missed
• Liver biopsy undertaken in 41% of which 40% had bridging fibrosis
• High incidence of insulin resistance
• 66 new referrals in 2016; 118 in 2018, 25 transitioned or discharged
• Dietician support but lack of wider MDT available
• Local/community resources patchy/unfocussed in UK.

Treatment Options
Copyright © 2015 American Medical Association.
All rights reserved.
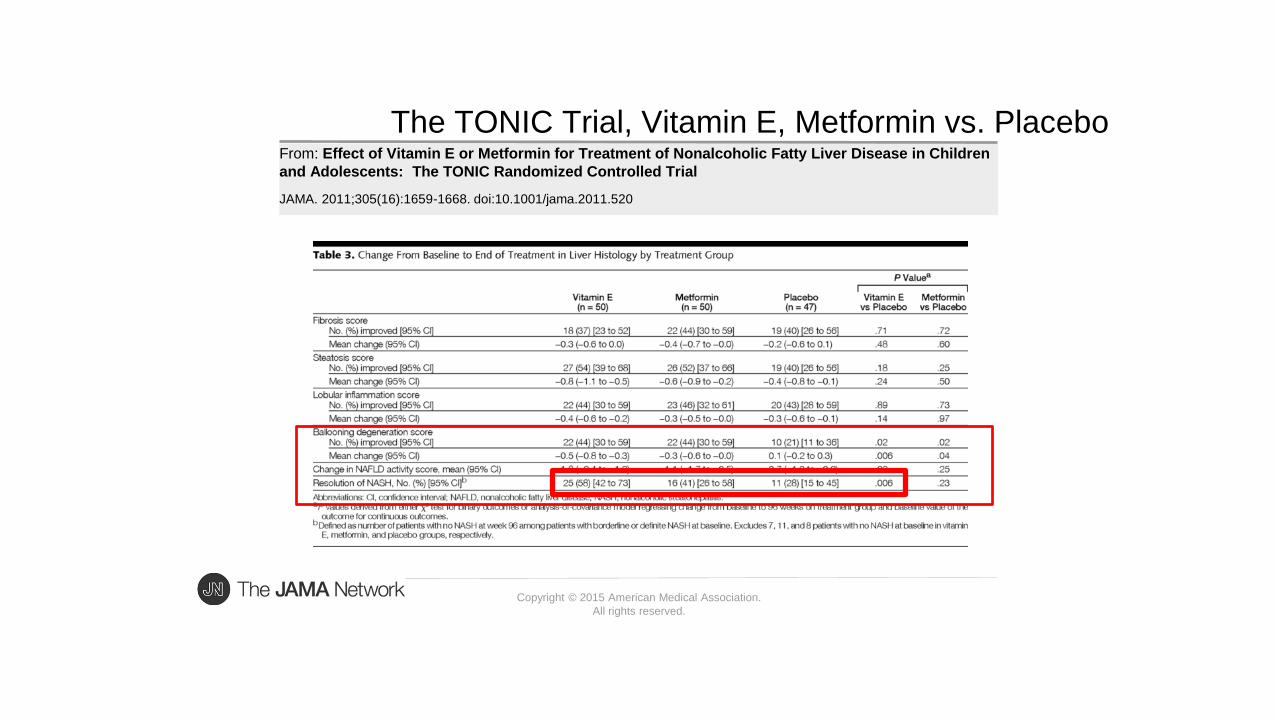
From: Effect of Vitamin E or Metformin for Treatment of Nonalcoholic Fatty Liver Disease in Children
and Adolescents: The TONIC Randomized Controlled Trial
JAMA. 2011;305(16):1659-1668. doi:10.1001/jama.2011.520
The TONIC Trial, Vitamin E, Metformin vs. Placebo

ELF test• Viral hepatitis B and C
• Type 2 Diabetes/Metabolic Syndrome
• Alcohol Abuse
The ELF Blood Test combines three serum biomarkers,
Fibrosis assigned a score based on the measurement of three substances:
• Hyaluronic acid (HA)
• Procollagen III amino terminal peptide (PIIINP)
• Tissue inhibitor of metalloproteinase 1 (TIMP-1)
An algorithm of these three markers creates an ELF Score.
NICE suggests only Vitamin E for NASH and mild/moderate fibrosis
Stopped with severe fibrosis
We evaluated it and found it did not correlate well with histology

36
» Microbial metabolites, such as short chain fatty acids (SCFAs), bind to conjugate receptors of G protein on intestinal epithelial cells by regulating energy from gut-derived
hormones, such as the intestinal peptide hormone, and controlling the inflammatory response of the host. The activation of Toll-like receptor-5) in the epithelia or myeloid cells
affects the structural composition of the intestinal microbiota, which regulates appetite, weight gain and insulin sensitivity
» It is suspected that the intestinal microbiota of obese individuals presents peculiarities that may induce chronic inflammation. The induction of endotoxemia in obesity,
diabetes mellitus and insulin resistance causes the expression of inflammatory factors that resemble those present in a diet rich in fat
Intestinal microbiota and NAFLD/NASH
Annals of Hepatology: 18,;3, May–June 2019, 416-421
Microbiota and nonalcoholic fatty liver disease/nonalcoholic steatohepatitis (NAFLD/NASH)
Sebastião M.B.DuarteabJose TadeuStefanoaClaudia P.Oliveiraab
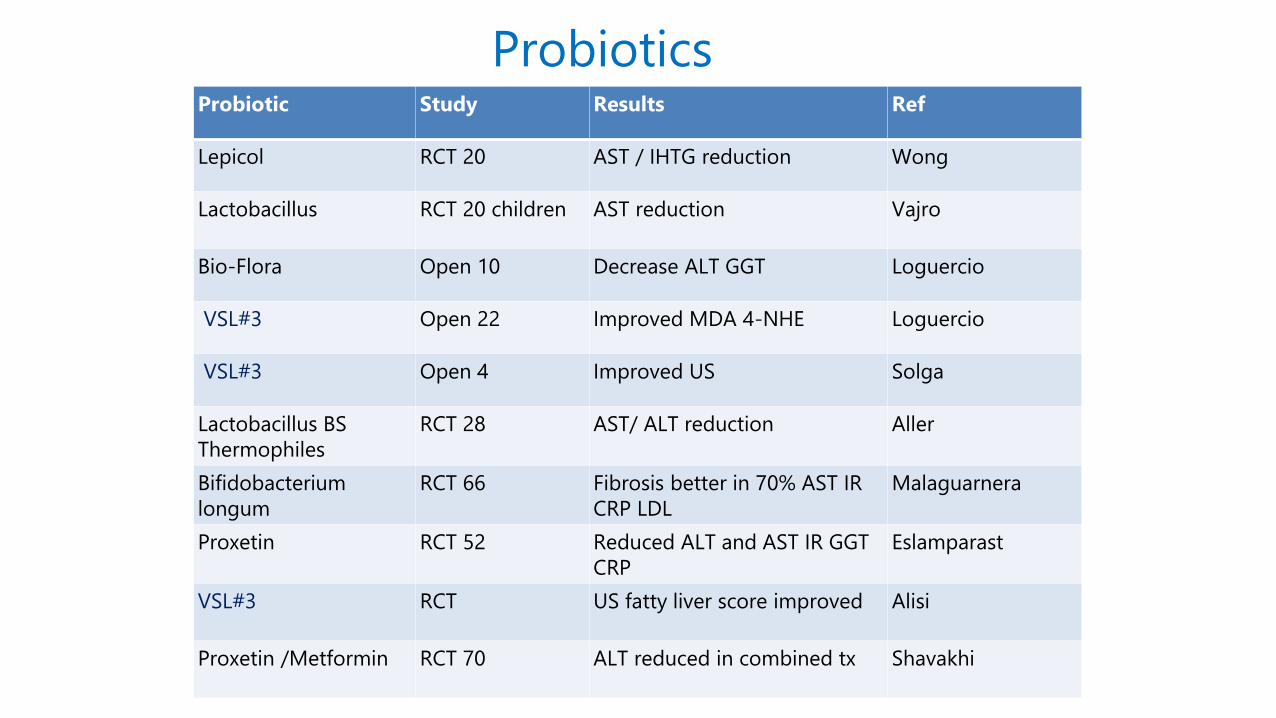
ProbioticsProbiotic Study Results Ref
Lepicol RCT 20 AST / IHTG reduction Wong
Lactobacillus RCT 20 children AST reduction Vajro
Bio-Flora Open 10 Decrease ALT GGT Loguercio
VSL#3 Open 22 Improved MDA 4-NHE Loguercio
VSL#3 Open 4 Improved US Solga
Lactobacillus BS
Thermophiles
RCT 28 AST/ ALT reduction Aller
Bifidobacterium
longum
RCT 66 Fibrosis better in 70% AST IR
CRP LDL
Malaguarnera
Proxetin RCT 52 Reduced ALT and AST IR GGT
CRP
Eslamparast
VSL#3 RCT US fatty liver score improved Alisi
Proxetin /Metformin RCT 70 ALT reduced in combined tx Shavakhi

FXR agonists
ALT ALP
gGTWtKg
Interrupt
FFA supply
Via BA
control of
uptake
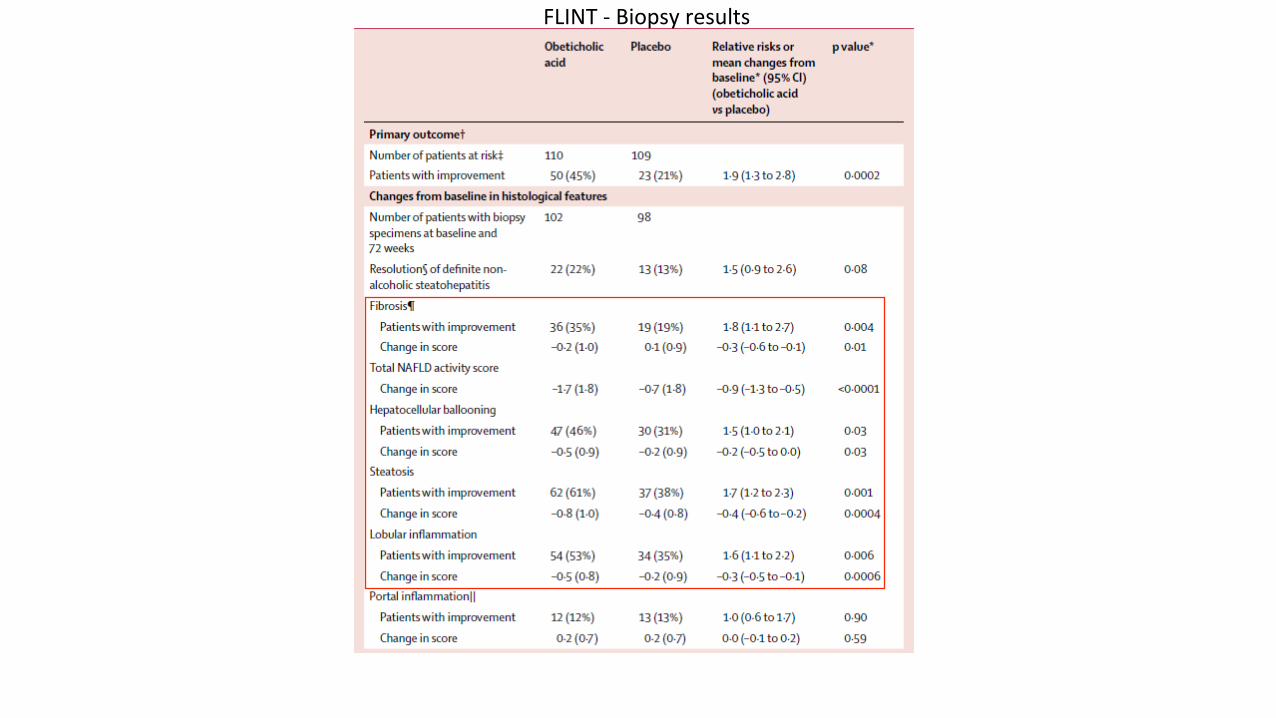
FLINT - Biopsy results

45% in OCA group had >2 point decrease in NAS with no worsening
of fibrosis compared to 21% in placebo group
Fibrosis was improved in 35% of OCA group versus 19% of placebo
BUT Increase in LDL in treatment group 25% in treatment group pruritis including 3 which were severe
FLINT - Biopsy results

Child obesity for Year Six children fell in 2016-17, bucking the national trend
28% of all children aged two to 15 in England are overweight or obese
Over four years, obesity in Leeds has dropped from 11.5% to 10.5% during the study
The biggest decline in obesity in Leeds is 6.4% in the reception class
Most marked among families living in the most deprived areas
Approach = authoritative parenting, where parents make it clear they are in charge, but also respond to their children
Childhood obesity rates are rising in many parts of the world
in Amsterdam they are falling
2012 and 2015 the percentage of children who were overweight fell from 21% to 18.5%,
12% drop in overweight and obese children
A structured, interventionist approach integrated across various departments of local government
Managed by a city-level authority, and leverages the powers held by local governments
The healthy choice should be the easy choice - a “whole-systems approach.”
Eradicating overweight and obesity is a long term task that will take a generation
The programme, actions and activities must be sustainable
The programme is inclusive of all people and across all policy areas
Addressing childhood obesity is a matter of shared responsibility
The approach is evidence-based - ‘learning by doing, doing by learning’
Choices must be made to focus efforts
Prevention first, but do not forget children of the present
Curative components
How Amsterdam is reducing child obesityAmsterdam Healthy Weight Programme (AAGG)
• Recognise health as a long term priority• Nutrition must be taught in class• Birthday treats brought into school must be healthy (e.g. dried fruit, vegetables or fruit kebabs)• Only water or milk can be drunk and healthy snacks to be eaten during breaks• Fruit juice must not be brought into school• Meetings must be held with parents to discuss healthy lifestyles• Extra gym classes must be facilitated by trained teachers, attention given to children’s motor skills and development• Children must be encouraged to be active when outside school• Appointments must be organised with child health services to measure school children’s height andweight• Additional appointments to be organised if anything unusual is found
Amsterdam Healthy Weight Programme (AAGG)
OBESITY & NAFLD - A Public Health Problem!

Gweneth PaltrowTHANK YOU

Leptin was a good predictor of fibrosis: 29ng/ml in no / minimal fibrosis v 70ng/ml insignificant / severe fibrosis (p=0.037)Adiponectin did not meet statistical significance, leptin: adiponectin ratio trend towards significanceNeither leptin nor adiponectin could predict NAS
Lep
tin
ng/
ml
<F2 ≥F2
P=0.037
Adipocytokines
Lep
tin
:ad
ipo
ne
ctin
rat
io
<F2 ≥F2
P=0.052

Multivariate analysis
Logistic regression
• CK18M30 and leptin were independently associatedwith differentiation of fibrosis versus no fibrosis
• CK18M30 and AST were found to be significantdifferentiating simple steatosis from steatohepatitis
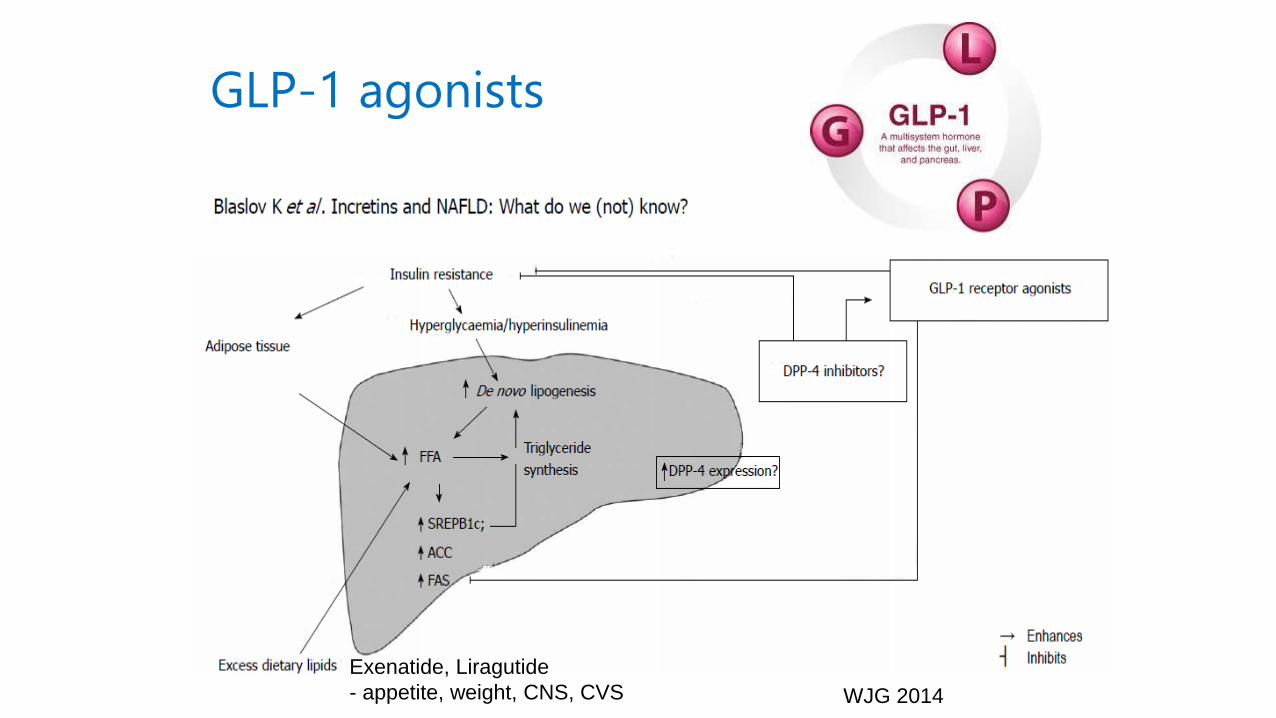
GLP-1 agonists
WJG 2014
Exenatide, Liragutide
- appetite, weight, CNS, CVS

Policies and action:A. Preventative:• Screening of infants for risk of obesity• Counselling for expectant mothers• Information provided to pregnant womenabout healthy diets• Mothers supported to breastfeed• Additional support for teenage parents andmore deprived mothers• Making primary schools healthier places• Cycle routes have been made safer• After-school activities have been arrangedfor children• Subsidies for sports club membership forlow income families
1. A 'first 1000 days' approach (from the start of pregnancy until age two)2. Schools approach (including pre-schools and primary schools)3. Neighbourhood and community approach4. Healthy environment approach (healthy urban design, healthy food environment)5. Focus on teens6. Focus on children with special needs
• Community health ambassadors assigned• Working with supermarkets and local foodsuppliers to: modify menus and reduce portion sizes; manage stock better; create healthier checkout environments; use traffic-light labelling posters• Banning unhealthy food and drinks sponsorship of city sports events• Reducing the advertising of unhealthy foods in council-owned locationsB. Curative:• Assigning youth healthcare nurses
• Drawing up care plans• Ensuring overweight and obese childrenreceive an appropriate level of care• Communicating behavioural insights7. Helping children who are overweight or obese to regain a healthier weightC. Facilitative:• Using an evidence-based approach• Observing interventions• Innovating digital tools• Introducing digital health coins• Exploring healthy sleep determinants, and assessing interventions8. Learning and research approach9. Use of digital facilities10. Use of communications and methodologies for behavioural insight