Embed Size (px)
Citation preview

Drug allergy
Dean TeyPaediatric Allergist & Immunologist
Monday 17 May 2010

Drug challengeDrug challenge• Gold standard for determining if a patient isGold standard for determining if a patient is
tolerant or allergic to a particular drug• Patient is admitted to hospital for 4 hoursp• Graded doses of the index drug is
administered, starting typically at 1/100th of the final treatment dose
• Patient then completes the medication course t hat home
• Contraindications: SJS, TEN, DRESS
Khan DA and Solensky R. Drug allergy. JACI 2010;125:s126-37.

Drug Allergy: Talk OutlineDrug Allergy: Talk Outline
1 Background: adverse drug reactions1. Background: adverse drug reactions2. Epidemiology3 M h i f ti3. Mechanism of action4. Assessment on history5. Investigations6 Drug desensitisation6. Drug desensitisation7. Specific drugs

Drug desensitisationDrug desensitisation• New term is ‘drug tolerance induction’, asNew term is drug tolerance induction , as
procedure is used for both IgE and non-IgEmediated drug allergies
• Indicated where there is an absolute need for a particular drug and no suitable alternative
i texists• Aim is to allow the patient to temporarily
tolerate the drug in a safe manner (throughtolerate the drug in a safe manner (through immunologic or other non-immunologic mechanisms))
Khan et al. JACI 2010;125:S126-37.

Drug desensitisationDrug desensitisation
• General principlesGeneral principles– The amount of drug tolerated by patient during
the skin test determines a safe initial dose (usually 1/10,000th of the final treatment dose)
– Double dose every 15 minutes until final dose– Mild reactions occur in about 1/3 of patients, but
no fatal reactions have been reportedI d f ti t t i d iti d it i– In order for patient to remain desensitised, it is necessary to continually administer medication
Solensky R. Drug Hypersensitivity. Med Clin N Am 2006;90:233-260.


Drug Allergy: Talk OutlineDrug Allergy: Talk Outline
1 Background: adverse drug reactions1. Background: adverse drug reactions2. Epidemiology3 M h i f ti3. Mechanism of action4. Assessment on history5. Investigations6 Drug desensitisation6. Drug desensitisation7. Specific drugs

Specific drugsSpecific drugs
1 Beta-lactams1. Beta lactams– Penicillins
Cephalopsorins– Cephalopsorins2. Sulfonamides3. Local anaesthestics4. Radiocontrast media5. Aspirin & NSAIDs

Specific drugsSpecific drugs
1 Beta-lactams1. Beta lactams– Penicillins
Cephalopsorins– Cephalopsorins2. Sulfonamides3. Local anaesthestics4. Radiocontrast media5. Aspirin & NSAIDs

How do we approach allergy testing for a child with
suspected penicillin allergy?suspected penicillin allergy?

Beta-lactams: PenicillinsBeta lactams: Penicillins
Beta-lactam ring
1. Solensky, R. (2006). Medical Clinics of North America 90(1): 233‐60.2. Gruchalla, R. S., M. Pirmohamed, et al. (2006). New England Journal of Medicine 354(6): 601‐9.

Beta-lactams: PenicillinsBeta lactams: Penicillins
Thiazolidine ring
1. Solensky, R. (2006). Medical Clinics of North America 90(1): 233‐60.2. Gruchalla, R. S., M. Pirmohamed, et al. (2006). New England Journal of Medicine 354(6): 601‐9.

Beta-lactams: PenicillinsBeta lactams: Penicillins
R1 side chain
1. Solensky, R. (2006). Medical Clinics of North America 90(1): 233‐60.2. Gruchalla, R. S., M. Pirmohamed, et al. (2006). New England Journal of Medicine 354(6): 601‐9.

Structural similarities and differences of penicillin side-chainschains
Baldo BA. Penicillins and cephalosporins as allergens –structural aspects of recognition andstructural aspects of recognition and cross-reactions. Clinical and Experimental Allergy 199;29:744-749

Beta-lactams: PenicillinsBeta lactams: Penicillins
~ 95 %~ 95 %
1. Solensky, R. (2006). Medical Clinics of North America 90(1): 233‐60.2. Gruchalla, R. S., M. Pirmohamed, et al. (2006). New England Journal of Medicine 354(6): 601‐9.3. Khan et al. (2010). Journal of Allergy and Clinical Immunology 125:S126‐37.

Testing for penicillin allergyTesting for penicillin allergy
1. A panel of reagents are suggested:1. A panel of reagents are suggested:– Classical penicillin reagents: PPL, MDM and
benzylpenicillin– Semi-synthetic penicillins: Amoxycillin and
ampicillin2. Start with SPT if negative proceed to
IDT3. If IDT negative proceed to drug
challenge

NPV of penicillin IDTs?NPV of penicillin IDTs?• Generally considered to be very highGenerally considered to be very high• Large scale studies show that only 1-3% of
skin test-negative patients develop a mild, g p p ,self-limiting reaction when challenged to the drug
G ( )– Gadde et al. JAMA 1993; 270: 2456-63 (n = 775)– Sogn et al. Arch Intern Med 1992; 152: 1025-32
(n = 726)(n 726)– Mendelson et al. JACI 1984; 73: 76-81 (n = 240)– Sullivan et al. JACI 1981; 68: 171-80 (n = 740)( )
Solensky, R. (2006). Medical Clinics of North America 90(1): 233‐60.

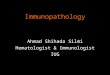
NPV of penicillin IDTs?NPV of penicillin IDTs?330 adults (mean age 38 yo) referred with a history of an
immediate reaction to penicillinimmediate reaction to penicillin
27% (89/330) CAP-FEIA and skin test negative to BPO, MDM, amoxycillin and
ampicillin
73% (241/330) positive to penicillin
CAP-FEIA or skin test
55% (49/89) had immediate allergic reactions to penicillin on drug challenge
• 45% (22/49) reacted to benzylpen• 55% (27/49) reacted selectively to
45% (40/89) were tolerant to both
benzylpenicillin and illi • 55% (27/49) reacted selectively to
amoxycillinamoxycillin
Torres et al. Clin Exp All 2002; 32: 270‐6

New vs old penicillin reagent kit?New vs old penicillin reagent kit?• Previously
– Pre-Pen (Hollister-Steer and Allergopharma)– Available commercially from 1974-2004
• Recentlyy– New kit from Diater Laboratories became available– Consists of
• PPL vial = Benzylpenicilloyl poly-L-lysine (and mannitol)y p y p y y ( )• MDM vial = Sodium benzylpenicillin, benzylpenicilloic acid,
sodium benzylpenicilloate (and mannitol)• Concordance
– Recent studies have indicated excellent concordance with the old kit for both benzylpenicilloyl major determinant (97.4%) and the minor determinants (100%)
1. Romano et al. Allergy 2007; 62: 53-58

What about cross-reactivity with cephalosporins?
Beta-lactam ring
1. Solensky, R. (2006). Medical Clinics of North America 90(1): 233-60.2. Gruchalla, R. S., M. Pirmohamed, et al. (2006). New England Journal of Medicine 354(6): 601-9.

What about cross-reactivity with cephalosporins?
Dihydrothiazine ringThiazolidine ring
1. Solensky, R. (2006). Medical Clinics of North America 90(1): 233-60.2. Gruchalla, R. S., M. Pirmohamed, et al. (2006). New England Journal of Medicine 354(6): 601-9.

What about cross-reactivity with cephalosporins?
R1 side chain: implicated in cross-reactivity1. Solensky, R. (2006). Medical Clinics of North America 90(1): 233-60.2. Gruchalla, R. S., M. Pirmohamed, et al. (2006). New England Journal of Medicine 354(6): 601-9.
R1 side chain: implicated in cross reactivity

What about cross-reactivity with cephalosporins?
R2 side chain: disappears after beta-lactam ring opens
1. Solensky, R. (2006). Medical Clinics of North America 90(1): 233-60.2. Gruchalla, R. S., M. Pirmohamed, et al. (2006). New England Journal of Medicine 354(6): 601-9.
lactam ring opens

What about cross-reactivity with cephalosporins?
• Historical “10% cross-reactivity”: a myth?Historical 10% cross reactivity : a myth?– 1st gen cephalosporins were introduced in
1960’s (cephaloridine cephalothin)1960 s (cephaloridine, cephalothin)– Soon after, several retrospective studies
reported increased frequency ofreported increased frequency of cephalosporin-allergy in penicillin-allergic subjects (8%), compared to those without (1-2%).1,2
1. Dash CH. J Antimicrob Chemother 1975;1(Suppl 3):107-18.2. Petz LD. J Infect Dis 1978;137(Suppl):S74-9.

What about cross-reactivity with cephalosporins?
• These reviews likely overestimated true rate of ycross reactivity– Until 1982, compounds related to penicillin had been
produced by using a cephalosporium mould and theproduced by using a cephalosporium mould and the cephalosporins included in the analyses were contaminated with penicillin1
P ti t t t b i illi ll i– Patients were not proven to be penicillin-allergic (either through diagnostic testing or drug challenge)4
– Most 1st gen cephalosporins have similar R-group g p p g pside chains to benzylpenicillin, and this factor (rather than beta-lactam ring) may have led to cross-reactivity2y
1. Preger S and Healy B. BMJ 2007;335:9912. Solensky R. Med Clin N Am 90 2006;90:233-260.

What about cross-reactivity with cephalosporins?
• In a recent meta-analysis– 6 studies of 2387 patients with penicillin allergy and 44,897
without– Cross-reactivity was found to be related to cephalosporin
tigeneration• 1st generation – OR 4.79 (95%CI 3.71-6.17)• 2nd generation – OR 1.13 (95%CI 0.61-2.12)• 3rd generation – OR 0 45 (95%CI 0 18-1 13)• 3 generation – OR 0.45 (95%CI 0.18-1.13)
• Implications– For life-threatening conditions where it is optimal to use a
cephalosporin antibiotic in a penicillin-allergic patientcephalosporin antibiotic in a penicillin allergic patient– Consider use of a 2nd or 3rd generation cephalosporin with
a different side chain under suspicion
1. Preger S and Healy B. BMJ 2007;335:991.

What about cross-reactivity with h l i ?cephalosporins?
128 adults with immediate reaction to penicillin and +ve skin test.All skin tested to cephalothin (1st gen), cefamandole (2nd gen), cefuroximep ( g ) ( g )
(2nd gen), ceftriaxone (3rd gen), cefotaxime (3rd gen), ceftazidime (3rd gen).
96% (123/128) patients had negative skin tests to cefuroxime (2nd gen), ceftazidime (3rd gen),
3.9% had positive skin tests to cefuroxime (2nd
ceftriaxone (3rd gen) and cefotaxime (3rd gen)tests to cefuroxime (2gen), ceftazidime (3rd
gen), ceftriaxone (3rd
gen) or cefotaxime (3rd gen)
22 declined22 declinedcefotaxime (3rd gen)
NOT ELIGIBLE FOR CHALLENGE
challengechallenge
100% (101/101) who accepted challenge100% (101/101) who accepted challenge tolerated single dose cefuroxime axetil and
ceftriaxone (single IM dose) Romano et al. Ann Intern Med2004; 141: 16‐22

Pichichero ME. Journal of Family Practice 2006; 55 (2): 106-12.

Pichichero ME. Journal of Family Practice 2006; 55 (2): 106-12.

Specific drugsSpecific drugs
1 Beta-lactams1. Beta lactams– Penicillins
Cephalopsorins– Cephalopsorins2. Sulfonamides3. Local anaesthestics4. Radiocontrast media5. Aspirin & NSAIDs

SulfonamidesSulfonamides• Pathogenesisg
– Likely T-cell-mediated mechanism (rather than specific IgE or IgG antibodies)1
Increased risk in HIV positive patients due to:– Increased risk in HIV-positive patients, due to: altered drug metabolism (slow acetylation), relative glutathione deficiency and viral stimulation of cytochrome p450 and gamma-stimulation of cytochrome p450 and gamma-interferon2
• Clinical2– Mostly causes delayed generalised
maculopapular eruptions, associated with fever and pruritus
1. Choquet-Kastylevsky et al. Curr Alelrgy Asthma Rep 2002;2:16-25.2. Solensky R. Med Clin N Am 2006;90:233-260

Solensky R. Med Clin N Am 2006;90:233-260
Strom et al. NEJM 2003;349:1628-35

Specific drugsSpecific drugs
1 Beta-lactams1. Beta lactams– Penicillins
Cephalopsorins– Cephalopsorins2. Sulfonamides3. Local anaesthestics4. Radiocontrast media5. Aspirin & NSAIDs

Local anaestheticsLocal anaestheticsBenzoate esters AmidesBenzocaine BupivacaineChloroprocaine LevobupivacaineCocaine Lidocaine (lignocaine)Cocaine Lidocaine (lignocaine)Procaine MepivacaineProparacaine RopivacaineTetracaine (amethocaine) Prilocaine
• Cross-react with other esters• Does not cross-react with
amides.
• Does not cross-react with either other amides or esters.
Khan DA and Solensky R. Drug allergy. Journal of Allergy and Clinical Immunology 2010;125:S1256-37.

Specific drugsSpecific drugs
1 Beta-lactams1. Beta lactams– Penicillins
Cephalopsorins– Cephalopsorins2. Sulfonamides3. Local anaesthestics4. Radiocontrast media5. Aspirin & NSAIDs

Radiocontrast media (RCM)Radiocontrast media (RCM)
• PrevalencePrevalence – Anaphylactoid reactions1
• 1-3% of patients receiving ionic RCM• 1-3% of patients receiving ionic RCM• <0.5% of patients receiving non-ionic RCM
– Severe life-threatening reactions2Severe life threatening reactions• 0.22% of patients receiving ionic RCM• 0.04% of patients receiving non-ionic RCMp g
– Fatality rate is 1-2 per 100,000 procedures3
1 Wolf et al Invest Radiol 1991;26:404-101. Wolf et al. Invest Radiol 1991;26:404 102. Katayama et al. Radiology 1990;175:621-83. Caro et al. AJR Am J Roentgenol 1991;156:825-32

Radiocontrast media (RCM)Radiocontrast media (RCM)
• Anaphylactoid versus anaphylaxisAnaphylactoid versus anaphylaxis– Reaction not mediated by specific IgE
antibodiesantibodies– RCM likely has direct effects on mast cells
and basophils leads to direct degranulationand basophils leads to direct degranulation and systemic mediator release
– Complement activation may also account for p ysome reactions
Solensky R. Med Clin N Am 2006;90:233-260

Radiocontrast media (RCM)Radiocontrast media (RCM)
• ManagementManagement1. Determine if the study is essential2 Explain risks to patient2. Explain risks to patient3. Ensure proper hydration4 Use a non ionic iso osmolar RCM4. Use a non-ionic, iso-osmolar RCM5. Pretreatment with corticosteroid and
antihistamineantihistamine
Solensky R. Med Clin N Am 2006;90:233-260

Specific drugsSpecific drugs
1 Beta-lactams1. Beta lactams– Penicillins
Cephalopsorins– Cephalopsorins2. Sulfonamides3. Local anaesthestics4. Radiocontrast media5. Aspirin & NSAIDs

Type of reaction
Notes
Aspirin-exacerbated respiratory
• Occurs in up to 20% of adult asthmatic patients, more common in women, has an average onset of around 30 yo1
disease (AERD) • Usually starts with rhinitis, progressing to sinusitis and nasal polyposis1
• Pathogenesis: aspirin leads to inhibition of COX-1 decrease PGE2 levels reduced inhibition of 5decrease PGE2 levels reduced inhibition of 5-lipoxygenase increased cysteinyl leukotrienes2
• Management: avoid both aspirin and NSAIDs; aggressive management of asthma and rhinitis2aggressive management of asthma and rhinitis
Exacerbation of chronic urticaria & angiodema
• Ingestion of NSAIDs that inhibit COX-1 can exacerbate chronic urticaria & angioedema2
• Most patients tolerate COX 2 inhibitors2angiodema • Most patients tolerate COX-2 inhibitors2
Anaphylaxis • Typically drug-specific and able to tolerate other NSAIDs3
1. Stevenson DD. JACI 2006;118:773-88.2. Khan et al. JACI 2010;125:S126-37.3. Quiralte et al. J Investig Allergol Clin Immunol 2007;17:182-8.

Summary pointsSummary points
1 Severe cutaneous drug reactions1. Severe cutaneous drug reactions – SJS, TEN, AGEP, HSS (DRESS)
Can cause significant morbidity and mortality– Can cause significant morbidity and mortality– Important to exclude these conditions as
they present as contraindications for IDT andthey present as contraindications for IDT and drug challenge

Summary pointsSummary points
2. Penicillin allergy2. Penicillin allergy– Majority (90%) of self-reported penicillin
allergic patients are actually tolerant following evaluation and drug challenge
– IDT should be performed toM j d t i t b l i ill l• Major determinant: benzylpenicilloyl
• Minor determinant• Side chains: amoxycillin and ampicillinSide chains: amoxycillin and ampicillin
– NPV for intradermal skin testing is good (1-3%)

Summary pointsSummary points
3 Penicillin and cross-reactivity with3. Penicillin and cross reactivity with cephalosporins
– Previous reports of 10% cross-reactivity are aPrevious reports of 10% cross reactivity are a likely overestimated
– Cross-reactivity with cephalosporins are most likely due to similarities of R1-side chains (rather than sensitisation to beta-lactam ring)If ki t ti i ti ti t h hi h– If skin testing is negative, patients have a high likelihood of tolerating a 3rd generation cephalosporincephalosporin