Embed Size (px)
Citation preview

Oxidative stress and ferritin expression in theskin of patients with rosacea
Vesna Sredoja Tisma, MD, MSc,a Aleksandra Basta-Juzbasic, MD, PhD,b Morana Jaganjac, BSc,c
Luka Brcic, MD, PhD,d Ivan Dobric, MD, PhD,b Jasna Lipozencic, MD, PhD,b Franz Tatzber, MD, PhD,e
Neven Zarkovic, MD, PhD,c and Marija Poljak-Blazi, BSc, PhDc
Zagreb, Croatia, and Vienna, Austria
Background: Rosacea is a common chronic light-sensitive inflammatory skin disease of unknown origin.The purpose of this work was to determine the parameters of oxidative stress, antioxidative capacity, andthe pathophysiologic role of ferritin expression in skin cells of patients with rosacea.
Objectives: The investigation consisted of measurements of serum peroxide levels, serum totalantioxidative potential levels, and immunohistochemical analyses of ferritin in skin tissue samples.
Results: Serum peroxide levels were significantly higher and serum total antioxidative potential levelswere significantly lower in patients with rosacea than in healthy control subjects (P \ .05). Compared withcontrol subjects, the number of ferritin-positive cells was significantly higher (P \ .001) in skin samplesfrom patients with rosacea, especially those with severe disease.
Limitations: Patients with rosacea in the study were aged 30 to 70 years (average age was 56 years).Younger patients with flushing only were not included according to the request of the ethics committee,limiting the use of diagnostic biopsies only to the necessary cases.
Conclusion: The statistically significant differences in the expression of ferritin, higher peroxide levels, andlower antioxidative potential support the onset of systemic oxidative stress in patients with rosacea. ( J AmAcad Dermatol 2009;60:270-6.)
Rosacea is a common chronic inflammatorydermatosis, characterized by various combi-nations of cutaneous signs such as flushing,
erythema, telangiectasia, edema, papules, papulo-pustules, ocular lesions, and phymas. Women areaffected at a younger age and more often than men,although more extreme cases with rhinophyma aremainly seen in men.1,2
From the Polyclinic Department of Dermatology and Venereology,
Dubrava University Hospital, Zagreba; Department of Derma-
tology and Venereology, Zagreb University Hospital Centerb;
Division of Molecular Medicine, Rudjer Boskovic Institute,
Zagrebc; Institute of Pathology, Medical School University of
Zagrebd; and KEG Co. Vienna.e
Supported by Croatian Ministry of Science, Education, and Sports
and by COST Action B35.
Conflicts of interest: None declared.
Accepted for publication June 26, 2008.
Reprint requests: Neven Zarkovic, MD, PhD, Laboratory for
Oxidative Stress, Division of Molecular Medicine, Rudjer
Boskovic Institute, Bijenicka 54, HR-10002 Zagreb, Croatia.
E-mail: [email protected].
Published online November 25, 2008.
0190-9622/$36.00
ª 2008 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2008.10.014
270
Although the pathogenesis of rosacea remainsunknown, inflammation is a central process in thisdisorder. Recent evidence suggests that in rosaceainflammation is associated with production of reac-tive oxygen species (ROS) by inflammatory cellssuch as neutrophils.3
ROS themselves do not necessarily have to lead todevelopment of pathological processes; however, inthe presence of transition metals, such as copper andiron, they easily generate harmful hydroxyl radicals.Iron has the capacity to accept and donate electronsreadily, which makes it physiologically essential as auseful component of cytochromes and oxygen-bind-ing molecules. However, iron is also biochemicallydangerous; it can damage tissues by catalyzing theconversion of hydrogen peroxide to free radicals thatattack cellular membranes, proteins, and DNA. Ironoverload may amplify the damaging effects of su-peroxide and peroxide overproduction in a broadspectrum of acute and chronic inflammatory condi-tions.4 In cells, most of the iron that is not metabo-lized is sequestered in ferritin as a crystalline core offerric (Fe31) ions. To catalyze oxidative reactions,the iron must first be released from the core. Thus,ferritin is able to restrict the availability of iron to

J AM ACAD DERMATOL
VOLUME 60, NUMBER 2
Sredoja Tisma et al 271
participate in oxidative reactions.5 In mammaliancells, the level of ferritin is tightly controlled by theiron-regulatory protein-1 at the posttranscriptionallevel. This regulation prevents iron from acting as acatalyst in reactions between ROS and biomolecules.Ultraviolet (UV) A radiation (320-400 nm) has beenshown to be a source of oxidative stress to skin viageneration of ROS.6 Pourzand et al6 reported that theexposure of human primary skin fibroblasts FEK4 toUVA radiation causes an immediate release of ‘‘free’’iron in the cells via proteolysis of ferritin, and thismight be a major factor in UVA-induced damage tothe skin.
Bissett et al7 reported a 3-fold increase in the ironcontent of human epidermis from sun-exposed areasas compared with nonexposed body sites. Thepresence of excess iron has also been demonstratedin a variety of skin disorders such as psoriasis,8
venous ulceration,9 and atopic eczema,10 but there isno study of iron content in the skin cells of patientswith rosacea.
We hypothesized that increased release of freeiron in the skin cells via proteolysis of ferritin andconsequent oxidative damage to the skin, possiblyinduced by UV light or other exogenous stressorssuch as high temperature and inflammation, mighthave a pathogenic role in rosacea. Therefore, in thisstudy, measurements of serum peroxide levels, se-rum total antioxidative potential levels, and immu-nohistochemical analyses of ferritin expression inskin cells of patients with different forms of rosaceawere assessed.
METHODSParticipants
Sixty patients aged 30 to 76 years with rosacea and11 healthy control subjects were included in thisstudy. None of the patients had any treatment (drugor sun blocks) for 3 months. Skin samples, sera, andclinical and histopathologic data were obtained fromour department of dermatology and venereology.
Rosacea was diagnosed by clinical findings andhistologic examination. According to the standardclassification of rosacea proposed in 2002,1 thedisease is classified into 4 different subtypes: eryth-ematotelangiectatic rosacea (subtype 1; character-ized by persistent erythema of the central portion ofthe face lasting for at least 3 months with telangiec-tasia); papulopustular rosacea (subtype 2; character-ized by persistent erythema, telangiectasia, andpapules); and phymatous rosacea (subtype 3; char-acterized by thickened skin, surface nodularities,patulous follicles, and telangiectasia). Patients withocular rosacea (subtype 4) were not included in thestudy because they are treated by ophthalmologists.
Healthy persons with skin phototypes II and III (4male and 7 female) who had no history of skindisease were recruited as a control group.
Neither patients nor control subjects had historyof any topical or systemic drug therapy for at least 6months before the skin biopsy specimen and bloodcollection, and none had any systemic disease. Therewas no difference between patients and controlsubjects regarding age, smoking, medicaments, oralcohol intake.
Samples, data collection, and protection ofhuman participants
Forty skin samples and data used in this studywere collected and evaluated retrospectively fromthe existing database. Prospectively, 20 skin samplesand 20 serum samples from patients with rosaceawere collected on the same day. In patients withrosacea, biopsy specimens were taken from thenose, cheeks, central aspect of the forehead, andchin. The serum samples from the patients withrosacea and control subjects were taken on the sameday as the biopsy specimens. The biopsy specimensfrom control subjects (nonrosacea skin samples)were taken from the face during the excision ofbenign, noninflammatory facial disorders in which 4mm of healthy skin was taken from the edge of thelesion. Control sera were collected from the healthyvolunteers. Thus, the control skin and sera weretaken from different volunteers.
The use of the data for this investigational purposewas reviewed and approved by our department ofdermatology and venereology university hospitalcenter review board.
The study was approved by our university hospi-tal ethics committee and written informed consentwas obtained from each person involved. All proce-dures were in accordance with the recommenda-tions in the Helsinki Declaration of 1975.
Skin biopsy specimen and histopathologicexamination
The 4-mm biopsy specimens were obtained un-der local anesthesia. The biopsy samples wereplaced in 10% buffered formalin and immediatelyprocessed in histopathologic laboratory. Histologicsections (5 �m) of paraffin-embedded tissue wereprepared. The sections were examined by a pathol-ogist well experienced in the histopathology ofrosacea.
Immunohistochemical detection of ferritinExpression of ferritin was analyzed using immu-
nohistochemical staining for ferritin. Briefly, 5-�mparaffin sections were deparaffinized, rehydrated,

J AM ACAD DERMATOL
FEBRUARY 2009
272 Sredoja Tisma et al
and subsequently quenched for endogenous perox-idase activity with a 3% hydrogen peroxide solutionin methanol at room temperature for 15 minutes.Nonspecific binding sites were blocked by incuba-tion in washing buffer containing 10% of normalswine serum (Dako, Glostrup, Denmark) at roomtemperature for 30 minutes. The sections were thenincubated for 2 hours at room temperature with aperoxidase-conjugated rabbit antihuman ferritin an-tibody (Dako) at a dilution of 1:150.
The 3,3’-diaminobenzidine tetrahydrochloride(Dako) was used as chromogen. The sections werecounterstained with hematoxylin. Negative controlslides, in which test antibody was omitted andreplaced by control diluents, were included in allexperiments.
Assessment of ferritin contentA total of 100 cells were counted 3 times, at 3
different areas of the histologic slide, for each sampleand the mean value was calculated. The results wereexpressed as a percentage of ferritin-positive(brown) cells.
The expression of ferritin was graded (blinded topatient outcome) using software (ISSA, Vamstec Co,Zagreb, Croatia) according to the percentage ofpositive cells as follows: 0 for less then 5%, 1 for6% to 35%, 11 for 36% to 70%, and 111 for morethan 70%.
Oxidative stress parametersTotal serum peroxides. Serum peroxide con-
centrations were determined by a rapid in vitrodiagnostic assay (peroxide-activity assay, LDN,Nordhorn, Germany) as previously described.11
The assay is based on a peroxide/peroxidase reac-tion using tetramethylbenzidine as chromogenicsubstrate. Peroxide levels are expressed as ‘‘�MH2O2 equivalents,’’ because of different contribu-tions of various peroxides to the reaction. Theinterassay and intra-assay variance was 4.5%. Toavoid a loss of total peroxide activity or antioxidativecapacity during prolonged storage, serum sampleswere stored for no more than 1 week at e28C aftercollection. In all, 10 �L of the serum samples wereplaced into 96-well plates in duplicates andincubated with a mixture of horseradish peroxidase,tetramethylbenzidine, and phosphate buffer for 30minutes, and absorbance was determined in a multi-well plate reader (Easy-Reader 400 FW, SLT LabInstruments GmbH, Salzburg, Austria) at 450 nm.
Total antioxidant capacity. The antioxidantcapacity of frozen serum samples was measured bya commercially available method (Antiox-Cap, LDN)through the consumption of antioxidants present in
serum after addition of hydrogen peroxide as de-scribed before.12 The assay is based on the con-sumption of antioxidants present in sample afterthe addition of hydrogen peroxide. Serial dilutionsof uric acid (2-, 6-, 8-trihydroxypurine, Sigma,Taufkirchen, Germany) were used as a standard.Results were expressed as mg/mL of uric acidequivalents.
Statistical analysis. Descriptive statistics wereshown as the mean 6 SE. The significance ofdifferences between groups was assessed using theStudent t test and Chi-square test. Differences with Pless than .05 were considered statistically significant.
RESULTSBetween 2003 and 2007, rosacea was diagnosed
histopathologically in 36 male and 24 female pa-tients. Patient evaluation included history, physicalexamination, pathology findings, and the appropri-ate imaging techniques.
Table I summarizes the characteristics of thepatients. The patients were aged 30 to 76 years(average age 56 years). Average duration of illness atthe time of diagnosis was less than 5 years (range 1-30). At the time of diagnosis 13 (22%) patients weresubtype 1, 36 (60%) were subtype 2, and 11 (18%)were subtype 3.
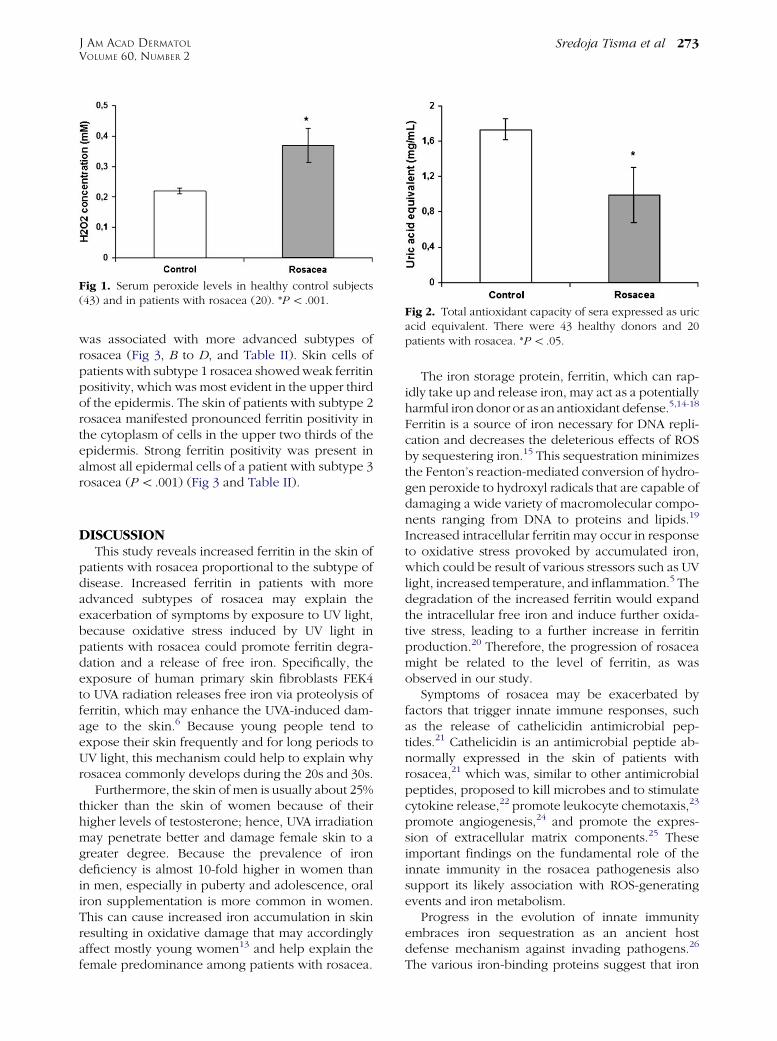
Serum peroxide levels were significantly higher inpatients with rosacea than in healthy control subjects(P \.05) (Fig 1). In contrast, serum total antioxidantcapacity was significantly lower in the sera of pa-tients with rosacea than in healthy control subjects(P \ .05) (Fig 2).
In the skin of healthy donors almost no ferritin-positive cells were present in the epidermis (Fig 3,A). The number of ferritin-positive cells was signif-icantly higher (P \ .001) in the skin samples ofpatients with rosacea and higher ferritin positivity
Table I. Patient characteristics
Parameters N (%)
All patients 60 (100)Male 36 (60)Female 24 (40)
Age at diagnosis, yAverage 56Range 30-76
Illness duration at diagnosis, yAverage 4.7Range 1-30
Subtype of disease1 - erythematotelangiectatic rosacea 13 (21)2 - papulopustular rosacea 36 (60)3 - pustules and phymatous rosacea 11 (18)
J AM ACAD DERMATOL
VOLUME 60, NUMBER 2
Sredoja Tisma et al 273
was associated with more advanced subtypes ofrosacea (Fig 3, B to D, and Table II). Skin cells ofpatients with subtype 1 rosacea showed weak ferritinpositivity, which was most evident in the upper thirdof the epidermis. The skin of patients with subtype 2rosacea manifested pronounced ferritin positivity inthe cytoplasm of cells in the upper two thirds of theepidermis. Strong ferritin positivity was present inalmost all epidermal cells of a patient with subtype 3rosacea (P \ .001) (Fig 3 and Table II).
DISCUSSIONThis study reveals increased ferritin in the skin of
patients with rosacea proportional to the subtype ofdisease. Increased ferritin in patients with moreadvanced subtypes of rosacea may explain theexacerbation of symptoms by exposure to UV light,because oxidative stress induced by UV light inpatients with rosacea could promote ferritin degra-dation and a release of free iron. Specifically, theexposure of human primary skin fibroblasts FEK4to UVA radiation releases free iron via proteolysis offerritin, which may enhance the UVA-induced dam-age to the skin.6 Because young people tend toexpose their skin frequently and for long periods toUV light, this mechanism could help to explain whyrosacea commonly develops during the 20s and 30s.
Furthermore, the skin of men is usually about 25%thicker than the skin of women because of theirhigher levels of testosterone; hence, UVA irradiationmay penetrate better and damage female skin to agreater degree. Because the prevalence of irondeficiency is almost 10-fold higher in women thanin men, especially in puberty and adolescence, oraliron supplementation is more common in women.This can cause increased iron accumulation in skinresulting in oxidative damage that may accordinglyaffect mostly young women13 and help explain thefemale predominance among patients with rosacea.
Fig 1. Serum peroxide levels in healthy control subjects(43) and in patients with rosacea (20). *P \ .001.
The iron storage protein, ferritin, which can rap-idly take up and release iron, may act as a potentiallyharmful iron donor or as an antioxidant defense.5,14-18
Ferritin is a source of iron necessary for DNA repli-cation and decreases the deleterious effects of ROSby sequestering iron.15 This sequestration minimizesthe Fenton’s reaction-mediated conversion of hydro-gen peroxide to hydroxyl radicals that are capable ofdamaging a wide variety of macromolecular compo-nents ranging from DNA to proteins and lipids.19
Increased intracellular ferritin may occur in responseto oxidative stress provoked by accumulated iron,which could be result of various stressors such as UVlight, increased temperature, and inflammation.5 Thedegradation of the increased ferritin would expandthe intracellular free iron and induce further oxida-tive stress, leading to a further increase in ferritinproduction.20 Therefore, the progression of rosaceamight be related to the level of ferritin, as wasobserved in our study.
Symptoms of rosacea may be exacerbated byfactors that trigger innate immune responses, suchas the release of cathelicidin antimicrobial pep-tides.21 Cathelicidin is an antimicrobial peptide ab-normally expressed in the skin of patients withrosacea,21 which was, similar to other antimicrobialpeptides, proposed to kill microbes and to stimulatecytokine release,22 promote leukocyte chemotaxis,23
promote angiogenesis,24 and promote the expres-sion of extracellular matrix components.25 Theseimportant findings on the fundamental role of theinnate immunity in the rosacea pathogenesis alsosupport its likely association with ROS-generatingevents and iron metabolism.
Progress in the evolution of innate immunityembraces iron sequestration as an ancient hostdefense mechanism against invading pathogens.26
The various iron-binding proteins suggest that iron
Fig 2. Total antioxidant capacity of sera expressed as uricacid equivalent. There were 43 healthy donors and 20patients with rosacea. *P \ .05.

J AM ACAD DERMATOL
FEBRUARY 2009
274 Sredoja Tisma et al
Fig 3. Ferritin immunohistochemistry in normal-appearing skin of donor without rosacea(obtained during excision of benign facial lesions) (A) and skin of patients with subtype 1 (B), 2(C), and 3 (D) rosacea. (Original magnification: 340.)
withholding may be important to defend cellsagainst invading bacteria,27 while the skin of patientswith rosacea may be a target for the microbialinfiltration because these microbes might competefor host iron and could preferentially migrate intolocal environments where iron is abundant.
Among environmental factors that could triggeroxidative stress in the skin, long-wavelength UVAlight, which is a strong oxidant, may play an impor-tant role. UVA radiation activates heme oxygenase-1 in dermal fibroblasts5,28 causing degradation ofheme and production of biliverdin, carbon monox-ide, and ferritin.29 Thus, potential induction of theheme oxygenase-1/ferritin system by UVA furthersupports the relevance of increased ferritin expres-sion in the skin of patients with rosacea as animportant factor in oxidative stress pathology asso-ciated with rosacea development based on theinflammatory stress response to exogenous factors(eg, UV and micro-organisms).
In accordance with other investigators30,31 ourstudy also shows a decrease in systemic antioxidantdefense system activity and consequential systemicoxidative stress in patients with rosacea. Our study
involved patients with rosacea who were aged 30 to76 years (average age 56 years), for whom weacknowledge that dysfunction of the antioxidantsystem might also be a consequence of aging. Wecould not include younger patients with transientflushing because relatively invasive diagnostic pro-cedures (eg, biopsy) necessary to establish the diag-nosis of rosacea in these patients was not approvedby the ethics committee. Therefore, further studieswith younger patients with flushing are desirable toevaluate in more detail a potential causative role ofoxidative stress and ferritin metabolism in rosacea.
Finally, it should also be mentioned that attenu-ation of oxidative stress might be a relevant approachfor the therapy of rosacea. A number of pharmaco-logic agents including metronidazole, tetracyclines,and azelaic acid, used in the treatment of the varioussubtypes of rosacea, appear to have antioxidantcapacities.32-34 In vitro studies have shown thatmetronidazole, an effective topical therapy for rosa-cea,35 interferes with neutrophil release of ROS thatcause injury at sites of inflammation.33 Some antiox-idant agents, such as topical vitamin C, vitamin E, andubiquinone, are already used in skin care products.

J AM ACAD DERMATOL
VOLUME 60, NUMBER 2
Sredoja Tisma et al 275
However, more research is necessary to validate theefficacy and safety of these antioxidant agents.Theoretically, antioxidants could be metabolizedalso into toxic free radicals, in particular in thepresence of pro-oxidant iron and peroxide; there-fore, careful monitoring of oxidative stress parame-ters in rosacea is advised. That is particularlyimportant because in our patients with rosaceasystemic oxidative stress was observed, as mani-fested by increased serum peroxide levels andreduced antioxidant capacities of serum. The resultsof our study support further investigations intodermal and systemic oxidative stress in patientswith rosacea. This may assist in the search for novelpharmacologic agents with antioxidant properties totreat affected patients.
REFERENCES
1. Wilkin J, Dahl M, Detmar M, Drake L, Feinstein A, Odom R, et al.
Standard classification of rosacea: report of the National
Rosacea Society expert committee on the classification and
staging of rosacea. J Am Acad Dermatol 2002;46:584-7.
2. Braun Falco O, Plewig G, Wolff HH, Burgdorf WHC. Diseases of the
sebaceous gland. In: Braun Falco O, Plewig G, Wolff HH, Burgdorf
WHC, editors. Dermatology. Second completely revised ed.
Berlin: Springer-Verlag; 2000. pp. 1071-9.
3. Jones D. Reactive oxygen species and rosacea. Cutis 2004;74:
17-20.
4. Emerit J, Beaumont C, Trivin F. Iron metabolism, free radicals,
and oxidative injury. Biomed Pharmacother 2001;55:333-9.
5. Vile GF, Tyrrell RM. Oxidative stress resulting from ultraviolet A
irradiation of human skin fibroblasts leads to heme oxygen-
ase-dependent increase in ferritin. J Biol Chem 1993;268:
14678-81.
6. Pourzand C, Watkin RD, Brown JE, Tyrrell RM. Ultraviolet A
radiation induces immediate release of iron in human primary
skin fibroblasts: the role of ferritin. Proc Natl Acad Sci U S A
1999;96:6751-6.
Table II. Association of clinical subtype with ferritinstaining in study cases (n = 60)
Staining*
Rosacea subtype 0 1 11 111 No. of patients
1 2 8y 3 0 132 0 4 22z 10§ 363 0 0 3 8§ 11No. of patients 2 12 28 18 60
*Ferritin expression was semiquantitatively classified as is
described in ‘‘Methods.’’yP \ .05 mild-moderate erythematotelangiectatic rosacea
(subtype 1) vs severe pustules and phymatous rosacea (subtype 3).zP \ .001 moderate papulopustular rosacea (subtype 2) vs mild-
moderate erythematotelangiectatic rosacea (subtype 1) and severe
pustules and phymatous rosacea (subtype 3).§P \ .001 severe pustules and phymatous rosacea and moderate
papulopustular rosacea (subtype 3 and 2) vs mild-moderate
erythemato telangiectatic rosacea (subtype 1).
7. Bissett DL, Chatterjee R, Hannon DP. Chronic ultraviolet
radiation-induced increase in skin iron and the photoprotec-
tive effect of topically applied iron chelators. Photochem
Photobiol 1991;54:215-23.
8. Molin L, Wester PO. Iron content in normal and psoriatic
epidermis. Acta Derm Venereol 1973;53:473-6.
9. Ackerman Z, Seidenbaum M, Loewenthal E, Rubinow A.
Overload of iron in the skin of patients with varicose ulcers:
possible contributing role of iron accumulation in progression
of the disease. Arch Dermatol 1988;124:1376-8.
10. David TJ, Wells FE, Sharpe TC. Serum levels of trace metals
in children with atopic eczema. Br J Dermatol 1990;122:
485-9.
11. Tatzber F, Griebenow S, Wonisch W, Winkler R. Dual method
for the determination of peroxidase activity and total
peroxideseiodide leads to a significant increase of peroxi-
dase activity in human sera. Ann Biochem 2003;316:147-53.
12. Resch U, Tatzber F, Budinsky A, Sinzinger H. Reduction of
oxidative stress and modulation of auto antibodies against
modified low-density lipoprotein after rosuvastatin therapy. Br
J Clin Pharmacol 2005;61:262-74.
13. Gropper SS, Kerr S, Barksdale JM. Non-anemic iron deficiency,
oral iron supplementation, and oxidative damage in college-
aged females. J Nutr Biochem 2003;14:409-15.
14. Sakaida I, Kyle ME, Farber JL. Autophagic degradation of
protein generates a pool of ferric iron required for the killing
of cultured hepatocytes by an oxidative stress. Mol Pharmacol
1990;37:435-42.
15. Balla G, Jacob HS, Balla J, Rosenberg M, Nath K, Apple F, et al.
Ferritin: a cytoprotective antioxidant stratagem of endothe-
lium. J Biol Chem 1992;267:18148-53.
16. Nath KA, Balla G, Vercellotti GM, Balla J, Jacob HS, Levitt MD,
et al. Induction of heme oxygenase is a rapid, protective
response in rhabdomyolysis in the rat. J Clin Invest 1992;90:
267-70.
17. Balla J, Jacob HS, Balla G, Nath K, Eaton JW, Vercellotti GM.
Endothelial-cell heme uptake from heme proteins: induction
of sensitization and desensitization to oxidant damage. Proc
Natl Acad Sci U S A 1993;90:9285-9.
18. Vile GF, Basu-Modak S, Waltner C, Tyrrell RM. Heme
oxygenase 1 mediates an adaptive response to oxidative
stress in human skin fibroblasts. Proc Natl Acad Sci U S A
1994;91:2607-10.
19. Mello Filho AC, Hoffmann ME, Meneghini R. Cell killing and
DNA damage by hydrogen peroxide are mediated by intra-
cellular iron. Biochem J 1984;218:273-5.
20. Cairo G, Tacchini L, Pogliaghi G, Anzon E, Tomasi A, Bernelli-
Zazzera A. Induction of ferritin synthesis by oxidative stress:
transcriptional and post-transcriptional regulation by expan-
sion of the ‘‘free’’ iron pool. J Biol Chem 1995;270:700-3.
21. Yamasaki K, Di Nardo A, Bardan A, Murakami M, Ohtake T,
Coda A, et al. Increased serine protease activity and catheli-
cidin promotes skin inflammation in rosacea. Nat Med 2007;
13:975-80.
22. Braff MH, Hawkins MA, Di Nardo A, Lopez-Garcia B, Howell MD,
Wong C, et al. Structure-function relationships among human
cathelicidin peptides: dissociation of antimicrobial properties
from host immunostimulatory activities. J Immunol 2005;174:
4271-8.
23. Yang De, Chen Q, Schmidt AP, Anderson GM, Wang JM,
Wooters J, et al. LL-37, the neutrophil granule and epithelial
cell-derived cathelicidin, utilizes formyl peptide receptor-like1
(FPRL1) as a receptor to chemoattract human peripheral blood
neutrophil monocytes, and T cells. J Exp Med 2000;192:
1069-74.

J AM ACAD DERMATOL
FEBRUARY 2009
276 Sredoja Tisma et al
24. Koczulla R, von Degenfeld G, Kupatt C, Krotz F, Zahler S, Gloe
T, et al. An angiogenic role for the human peptide antibiotic
LL-37/hCAP-18. J Clin Invest 2003;111:1665-72.
25. Gallo RL, Ono M, Povsic T, Page C, Eriksson E, Klagsbrun M,
et al. Syndecans, cell surface heparan sulfate proteoglycans,
are induced by a proline-rich antimicrobial peptide from
wounds. Proc Natl Acad Sci U S A 1994;91:11035-9.
26. Beck G, Ellis TW, Habicht GS, Schluter SF, Marchalonis JJ. Evolution
of the acute phase response: iron release by echinoderm (Asterias
forbesi) Coelomocytes, and cloning of an echinoderm ferritin
molecule. Dev Comp Immunol 2002;26:11-26.
27. Ong ST, Ho JZ, Ho B, Ding JL. Iron-withholding strategy in
innate immunity. Immunobiology 2006;211:295-314.
28. Tyrrell RM. Oxidant, antioxidant status and photocarcino-
genesis: the role of gene activation. Photochem Photobiol
1996;63:380-3.
29. Eisenstein RS, Garcia-Mayol D, Pettingell W, Munro HN.
Regulation of ferritin and heme oxygenase synthesis in rat
fibroblasts by different forms of iron. Proc Natl Acad Sci U S A
1991;88:688-92.
30. Baz K, Cimen MY, Kokturk A, Aslan G, Ikizoglu G, Demirseren D,
et al. Plasma reactive oxygen species activity and antioxidant
potential levels in rosacea patients: correlation with seropos-
itivity to Helicobacter pylori. Int J Dermatol 2004;43:494-7.
31. Oztas MO, Balk M, Ogus E, Bozkurt M, Ogus IH, Ozer N. The
role of free oxygen radicals in the ethiopathogenesis of
rosacea. Clin Exp Dermatol 2003;28:188-92.
32. Miyachi Y, Yoshioka A, Imamura S, Niwa Y. Effect of antibiotics
on the generation of reactive oxygen species. J Invest
Dermatol 1986;86:449-53.
33. Miyachi Y, Imamura S, Niwa Y. Anti-oxidant action of metro-
nidazole: a possible mechanism of action in rosacea. Br J
Dermatol 1986;114:231-4.
34. Akamatsu H, Komura J, Asada Y, Miyachi Y, Niwa Y. Inhibitory
effect of azelaic acid on neutrophil functions: a possible cause
for its efficacy in treating pathogenetically unrelated diseases.
Arch Dermatol Res 1991;283:162-6.
35. Nielsen PG. Treatment of rosacea with 1% metronidazole
cream: a double-blind study. Br J Dermatol 1983;108:
327-32.





























