Embed Size (px)
DESCRIPTION
over use injuries
Citation preview

Overuse Injuries in Pediatric and Adolescent Athletes
Heather W Harnly, M.D.

Overview
• Epidemiology • Unique pediatric anatomy • Upper and lower extremity overuse
injuries and “growing pains” • Sport specific injuries • Treatment
• Prevention of overuse injuries

Epidemiology of Youth Sports
• Participation increasing over the past 20 years
• Estimated 7,600,000 adolescents participating in high school sports
• Approximately 40 to 60,000,000 youth who participate in nonscholastic sports annually
National Council of Youth Sports, 2008 Report

Sports Injuries
• Estimated 4.3 million injuries per year
• Sports injuries account for 1/3 of all injuries in this age group
• Half of pediatric sports injuries are due to overuse

Paradigm Shift • Increasing participation in organized athletics among skeletally immature athletes
• Younger ages & increasing intensity of participation
• Specialization & Year-Round Focus
Shift in Etiology Macrotrauma • Fractures & Dislocations
Repetitive Microtrauma • Increasing Prevalence of Overuse injuries
Etiology

Why Do Overuse Injuries Occur?
• Longer seasons • Increased preseason training • Sports camps • “Select” teams • Rapid transition between sports • Emphasis on competition • Poor coaching
What is an Overuse Injury?
Chronic injuries related to constant high levels of physiologic stress without sufficient recovery time 1) rapidly increase level of activity 2) play w/ poor technique/ mechanics 3) fit/ good technique but over exposure
Overuse Injuries Seen In...
Previously Unfit Athlete
Extremely Fit Athlete
A condition caused by submaximal stress to previously normal tissues

Young Athletes
• The growing athlete is not merely a smaller version of the adult
• There are marked differences in coordination, strength, and stamina
• In young athletes, bone-tendon-muscle units, growth areas within bones, and ligaments experience uneven growth patterns, leaving them susceptible to injury.

Pediatric Anatomy
• Epiphysis: • bone between joint and
the growth plate
• Physis: • Growth plate: cartilage
layer which allows growth in length
• Apophysis: • attachment site for tendon
to bone

Pediatric Growth
• Puberty • Growth spurts begins
• Age 9 for girls with peak height velocity at 11-12 • Age 11 for boys, with peak height velocity at 13-14
• Growth accounts for 17-18% of final height • Boys double total muscle mass between ages 10-
17 • Often imbalance between strength and
flexibility in preadolescent/ adolescent years
Upper Extremity Overuse Injuries
• Distal Radius Physeal Stress syndrome • “Little Leaguer’s” Elbow and Shoulder • Stress Fractures • Swimmer’s shoulder • Osteochondritis Dessicans

Physeal Overuse Injuries • Distal radius physeal
stress syndrome • Seen in gymnasts • Wrist pain with weight
bearing • Usually no acute injury • Xrays show widening
of the growth plate, cysts, sclerosis
Roy et al, AJSM, 1985

Physeal Overuse Injuries
• May require a wrist brace for comfort, especially if pain with daily activities
• Usually resolves with 6-8 weeks of rest • Slow progressive return to activities if clinically
improved and radiographs resolve

Distal Radius Growth Arrest
• Serial radiographs showed • Stress-related changes
of the distal radial growth plate
• Progressed to closure of the distal radial growth plate before that of the ulna
9 cases of distal radial growth arrest in gymnasts
Difiori, AJSM, 2006

Medial Epicondyle Apophysitis or Little Leaguer’s Elbow
Classic Presentation
• Insidious onset of medial elbow pain • Progressively worsening • Exacerbated w/ throwing • Triad of Symptoms:
• Localized Pain in Late Cocking & Early Acceleration Phases • Loss of Velocity & Distance • Diminished Throwing Effectiveness
Classic Physical Exam: • Point tenderness @ medial epicondyle • 5-8 degree flexion contracture • Pain w/ valgus stress, but No frank instability • +/- Swelling
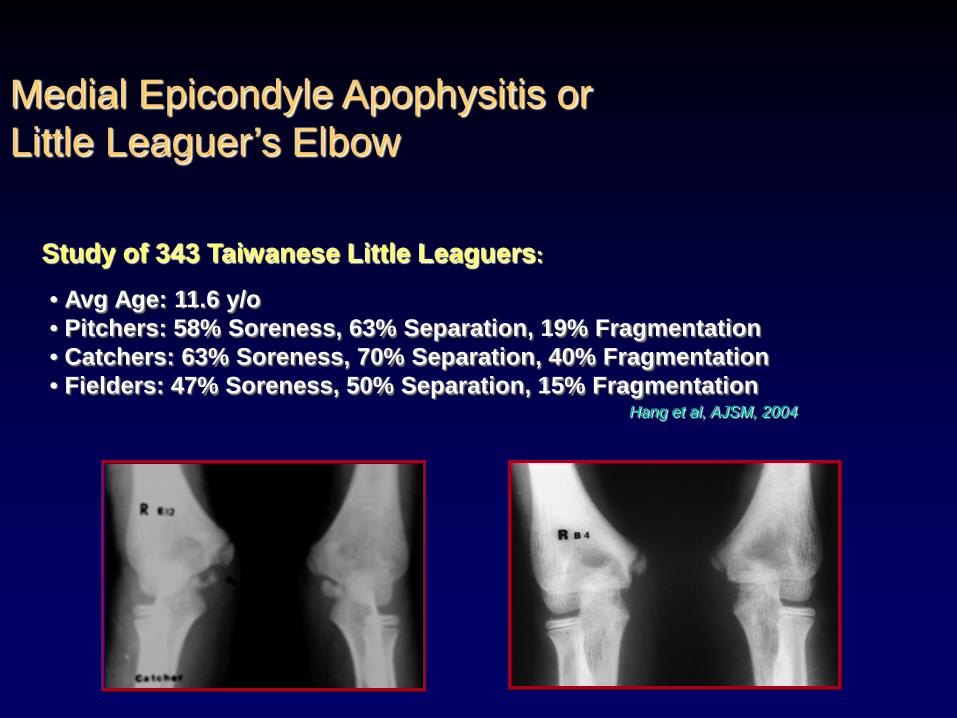
Medial Epicondyle Apophysitis or Little Leaguer’s Elbow
Study of 343 Taiwanese Little Leaguers:
• Avg Age: 11.6 y/o • Pitchers: 58% Soreness, 63% Separation, 19% Fragmentation • Catchers: 63% Soreness, 70% Separation, 40% Fragmentation • Fielders: 47% Soreness, 50% Separation, 15% Fragmentation Hang et al, AJSM, 2004

Medial Epicondyle Apophysitis
Treatment
Treatment: • Focuses on elimination of repetitive stress • Requires stopping all throwing activities - Recommended minimum 6-week restriction from throwing • Ice, NSAIDs for symptomatic relief •Physical Therapy can help with loss of range of motion
• Predicated on: • complete resolution of symptoms & • absence of tenderness on physical examination
• Documented radiographic healing is not essential for return to athletics • Gradual return = Critical → Strict throwing program emphasizing proper mechanics
Return to Throwing:

Little Leaguer’s Shoulder • Affects proximal humerus
growth plate at the shoulder
• Related to torsional stress during cocking and early acceleration phase of overhand throw
• Radiographs may demonstrate widening of the growth plate
Delee & Drez’s Orthopedic Sports Medicine, ©2003

Little Leaguer’s Shoulder
• Management: • Rest the throwing arm • May require complete
cessation of throwing, or switching to another position that requires less throwing
• Usually requires minimum of 6 weeks

Swimmer’s Shoulder
• Repetitive motion of swimming can cause rotator cuff impingement • Pressure on the rotator cuff from part of the
shoulder blade or scapula as the arm is lifted • Can result from fatigue and weakness of the
rotator cuff and muscles surrounding the shoulder blade
• Treated with physical therapy, strengthening exercises

Radiographic Findings • Persistence of olecranon apophysis +/- widening • Must compare to opposite elbow
Olecranon Stress Fracture
• Seen in older adolescent thrower • Persistent posterior elbow pain aggravated by
activity • Usually no history of acute injury • Posterior elbow pain in acceleration / follow-
through • Tenderness at Olecranon tip • Pain on resisted elbow extension

Conservative • Rest & avoidance of throwing • Splinting, ice, elevation
• Restrict throwing for minimum 6 wks
Treatment of Olecranon Stress Fracture
Operative • Indications
• Persistent symptoms > 3-6 months of conservative treatment • Radiographically documented failure of apophyseal closure despite conservative mgmt
• Single screw
Case #3

Osteochondritis Dessicans
• Can lead to fragmentation of the cartilage and formation of loose bodies
• Focal injury to subchondral bone resulting in loss of structural support for the overlying cartilage
OCD
Non-Surgical Treatment
• Stable Lesions: • STOP THROWING • NSAIDs • early splinting for acute symptoms • maintain range of motion • periodic radiographic follow-up • gradual return to activity when
asymptomatic and healed
OCD

Surgical Treatment
• Unstable Lesions may require surgery • Arthroscopic
• Drilling • Removal of loose bodies • Fixation
OCD

Lower Extremity Overuse Injuries
• Iliac Crest Apophysitis • Osgood-Schlatters • Sinding-Larsen-Johanssen • Patellofemoral Pain or “Runner’s Knee” • Shin Splints • Stress Fractures • Osteochondritis Dissecans

Pelvic Apophysitis • Occurs in runners 8-15 • Iliac crest apophysitis
• Pain at the top of the pelvis, occurs bilaterally with trunk rotation
• Ischial apophysitis • Pain localized to ischial
tuberosity or “sitting bone” • Onset insidious
• Treatment • Rest, ice, NSAIDS, stretching

Osgood-Schlatter Syndrome
• Traction apophysitis of tibial tubercle
• 1903: Osgood and Schlatter published independent papers on this clinical syndrome
• Athletes 10-15 years of age • Jumping sports • Boys > girls (? Historic sports
participation) • Bilateral 25-50% of cases
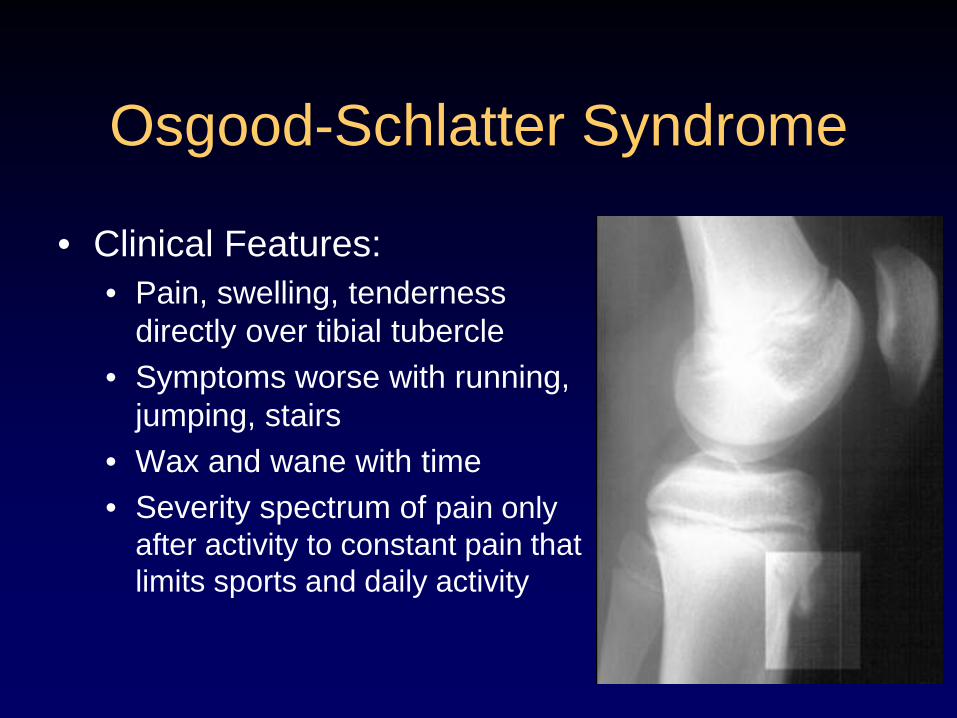
Osgood-Schlatter Syndrome
• Clinical Features: • Pain, swelling, tenderness
directly over tibial tubercle • Symptoms worse with running,
jumping, stairs • Wax and wane with time • Severity spectrum of pain only
after activity to constant pain that limits sports and daily activity

Osgood-Schlatter Syndrome
• Radiographic Features: • X-rays not required, usually are
normal • X-rays can show fragmentation
of tubercle or loose ossicle separate from tuberosity

Osgood-Schlatter Syndrome
• Natural History: • Self-limited over a period of 12-
24 months • Pain usually remits at skeletal
maturity • Prominence of tibial tubercle
persists • Small percentage of patients
have painful ossicle : surgical excision very successful

Management of Osgood-Schlatters
• Reassurance and teaching of natural history • Patients can play sports as tolerated • Treat symptomatically: relative rest , ice, hamstring
and quad stretching, neoprene knee sleeves, NSAIDS
• Corticosteroid injections are not recommended • Rarely, 2-4 week course of immobilization is
indicated for severe cases that resists simple activity modification
• Temporarily improves symptoms, does not alter natural history
Sinding-Larsen-Johansson Lesion
• Closely related to Osgood-Schlatter • Occurs at the opposite end of the
patella tendon at attachment to patella • No apophysis is involved, tendon
attaches to patella directly • With repetitive tension, periosteum
becomes inflamed and lays down more bone

Sinding-Larsen-Johansson Lesion
• Similar complaints of activity related pain but located at the end of the patella • Slightly younger patient
population ages 8-12
• Treatment • Rest, ice, analgesia • Usually self-limiting
No evidence that having had OS or SLJ as a child predisposes adults to patella or quad tendinopathy

Patellofemoral Pain Syndrome • Pain in front of the knee • Cause unclear, usually
overuse • Pain with sitting, climbing,
running
• Diffuse peripatellar tenderness
• Normal knee mechanics • No joint swelling • Normal gait • Normal radiographs
Examination

Patellofemoral Pain Syndrome
• Relative rest
• NSAIDS
• Icing
• Quadriceps strengthening
• Avoidance of bent knee activities
• Graduated return to activities
Treatment
No role for surgery!
“Shin Splints”
• Medial Tibial Stress Syndrome • Shin pain that produces pain
and discomfort due to repetitive running
• Pain along posteromedial border of the tibia
• Treatment: rest/ ice/ NSAIDS/ stretching
• Recurrence common if return to activity too quickly

Stress Fractures
• Stress Fractures • Increasing incidence in pediatric pts • Tibial shaft most common location (50%) • Fibula (20%) • Spine (15%) • Femur (3%) • Tarsal Navicular (2%) • Metatarsals

The Stress of Running
Force = 1.5 - 5x body weight Stride length of 4.5 ft = 1175 steps
150 lb runner absorbs
110 tons / foot
Running 1 mile:

Stress Fractures
• Occasionally occur in prepubescent pediatric athletes
• More common in adolescent or high school age athletes
• Running sports higher risk: • Cross country, soccer,
basketball

Sport Specific Stress Fractures
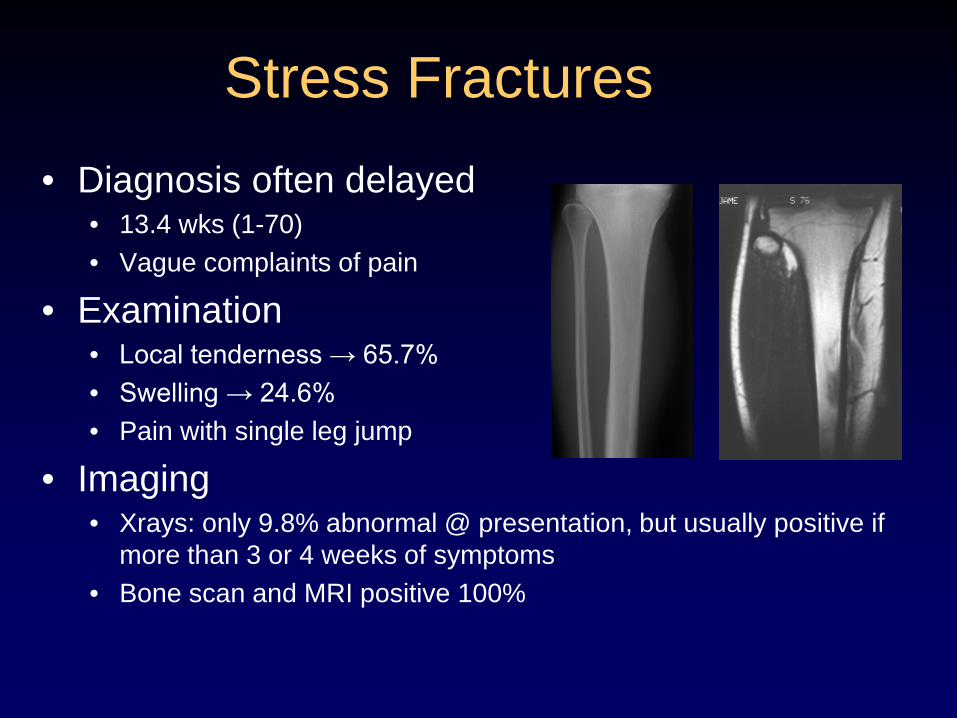
• Diagnosis often delayed • 13.4 wks (1-70) • Vague complaints of pain
• Examination • Local tenderness → 65.7% • Swelling → 24.6% • Pain with single leg jump
• Imaging • Xrays: only 9.8% abnormal @ presentation, but usually positive if
more than 3 or 4 weeks of symptoms • Bone scan and MRI positive 100%
Stress Fractures


Stress Fracture
• Usually heals with 6-12 weeks of rest
• Some require crutches/ brace treatment
• Usually means missing that season
2 weeks 8 weeks
Stress Fractures
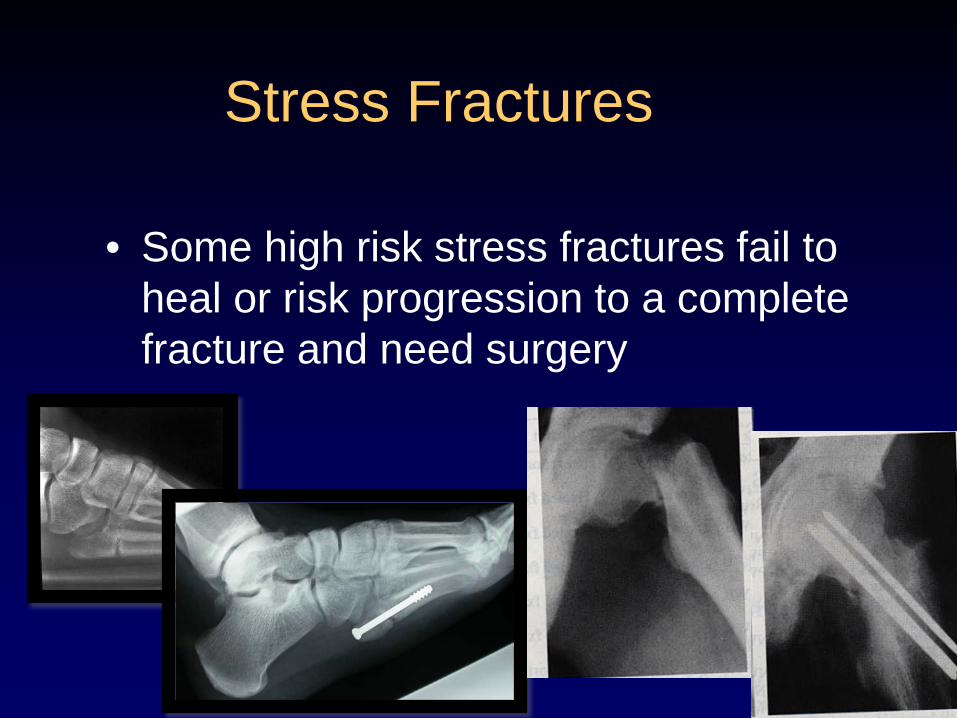
• Some high risk stress fractures fail to heal or risk progression to a complete fracture and need surgery

Juvenile Osteochondritis Dissecans (JOCD)
• Acquired condition of the joint that affects the articular surface and subchondral bone in pts with open growth plates
• Most commonly presents w/ vague knee pain that is poorly localized, without history of recent trauma • 80% symptoms more than 15 months
Osteochondritis Dissecans
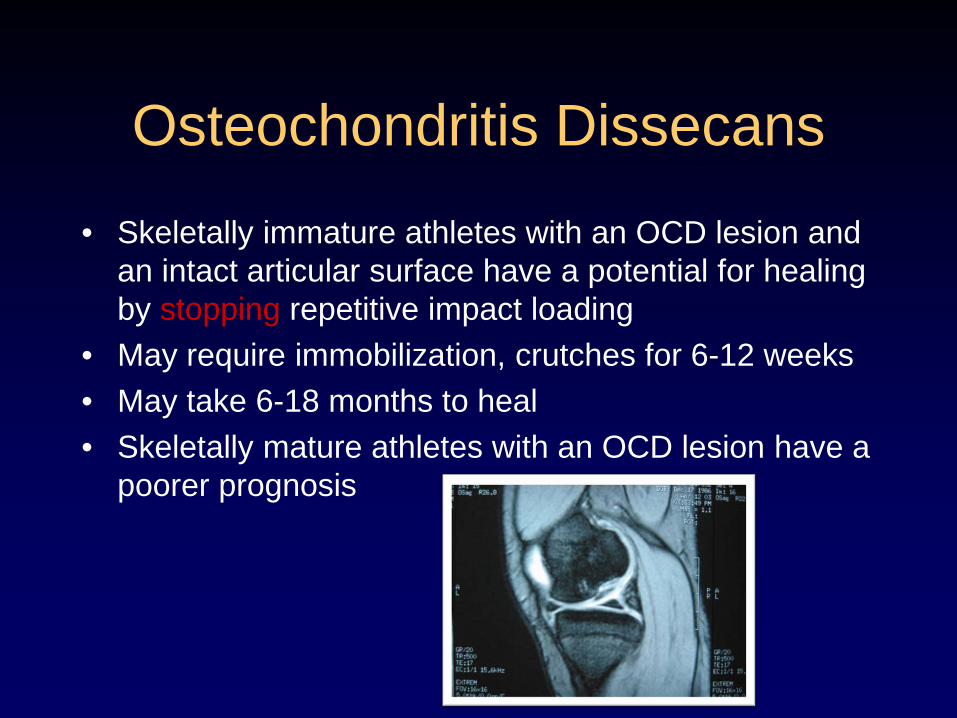
• Skeletally immature athletes with an OCD lesion and an intact articular surface have a potential for healing by stopping repetitive impact loading
• May require immobilization, crutches for 6-12 weeks • May take 6-18 months to heal • Skeletally mature athletes with an OCD lesion have a
poorer prognosis

Natural History
• If healing does not occur • Subchondral fracture • Fragmentation of
cartilage • Full thickness defect • Ultimately loss of
fragment stability and loose bodies

Operative Treatment
• Indications • Loose bodies • Failure to improve over 6
months • Unstable lesion • Approaching skeletal maturity
• Surgery • Drilling and or Fixation
Wright RW, McLean M, Matava MJ, Shively RA: “Osteochondritis dissecans of the knee: Long-term results of excision of the fragment. Clin Orthop 2004;424:2

Treatment of Overuse Injuries
• Most overuse injuries will heal with rest, occasional bracing or splints, and gradual return to activities
• Very rarely require surgery • Most overuse injuries can be prevented
with proper training and common sense • Teach kids to listen to their body,
remember that "no pain, no gain" does not apply
Recognizing Injuries
• Athletes should pay close attention to the physical limitations of their bodies by quickly responding to pain and allowing rest when needed
• It is important to recognize injuries at their earliest stages and to diagnose and treat them appropriately so that play is not impeded

Prevention of Overuse Injuries
• Baseball data has shown: • Excessive throwing, measured by number
of pitches per game or pitches per season, results in higher injury rates.
• Better pitchers throw a higher number of pitches and have higher injury rates.
• Year-round participation without rest results in higher injury rates.
• Specialty pitches such as curve balls and sliders may play a role.

Petty, et al., AJSM 2004
Recommended Maximum Number of Pitches
Age Max. Pitches / Game Max. Games / Week
8–10 50 2 11–12 65 2 13–14 75 2 15–16 90 2 17–18 105 2
recommendations were modified with permission from the USA Baseball Medical & Safety Advisory Committee in Petty et al. Ulnar Collateral Ligament Reconstruction in High-School Baseball Players AJSM, 2004.
Current Recommendations

Petty, et al., AJSM 2004
Recommended Rest Between Pitching
Age, y 1 Day of
Rest 2 Days of
Rest 3 Days of
Rest 4 Days of
Rest
8–10 20 35 45 50 11–12 25 35 55 60 13–14 30 35 55 70 15–16 30 40 60 80 17–18 30 40 60 90
aRecommendations were modified with permission from the USA Baseball Medical & Safety Advisory Committee in Petty et al. Ulnar Collateral Ligament Reconstruction in High-School Baseball Players AJSM, 2004.
Current Recommendations

Age to Learn Types of Pitches
Petty, et al., AJSM 2004
Pitch Age, y
Fastball 8 Change-up 10 Curveball 14 Knuckleball 15 Slider 16b Forkball 16b Splitter 16b Screwball 17b aReprinted with permission from the USA Baseball Medical & Safety Advisory Committee.1
bAges reflect results from a survey by the USA Baseball Medical & Safety Advisory Committee. Petty et al. believe that these pitches should not be thrown before the player is 18 years old.
Current Recommendations
Overuse Injuries In Baseball Pitchers
• Recent 10 year longitudinal study followed pitchers and documented injury rates
• Pitchers who pitched > 100 innings in at least one year were 3.5x more likely to be injured during the study
• Only 2.2 percent were still pitching by the 10th year of the study.
Prevention of Overuse Injuries
• Injury surveillance • Preparticipation Exams
• Identify potential risk factors • Proper adult supervision and coaching
• Teach correct technique • Teach stretching, warming up • Promote proper safety gear
• Healthy diet • Calcium, vitamin D

Prevention of Overuse Injuries
• Training Programs • Gradual progression: 10% rule • Varied practice • Planned rest • Cross-Training • Avoid excessive training volumes
• Delaying sport specialization • One team of the same sport per season • Keep sports fun, keep perspective

www.STOPSportsInjuries.org
STOP Sports Injuries — Keeping Kids in the Game for Life





























