-
8/12/2019 Overlap Bis
1/39
Daniela Opris
Oana Sacu
Sf. Maria Hospital, Carol Davila University of Medicine and
Pharmacy,
Research Centr e on the Pathology and Treatment of the Systemic
Rheumatic DiseasesBucharest, Romania
Universita di Studi di F irenze, Azienda Ospedal iero
Universitari a Careggi,
F irenze, I taly
-
8/12/2019 Overlap Bis
2/39
-
8/12/2019 Overlap Bis
3/39
Female, 40 ys, DS
Never smoked
: -pulmonary TB, bK +
-6 months treatment
-bilateral wrists, 2-5 MCF, 2-5 PIP
Knees arthritis
-3hs morning stiffness
CRP 77 mg/l (N
-
8/12/2019 Overlap Bis
4/39
1
0
1
001
0
1
0 0
00
22
0
0 0
mRodnans score: 8
DAS 28= 7.65
-
8/12/2019 Overlap Bis
5/39
Hands X-ray -Acro-osteolysis of 2,3,4,5 distal phalanges
-Flexion contractures
-Periarticular osteoporosis-Bilateral carpitis
-
8/12/2019 Overlap Bis
6/39
Laboratory evaluation:
CT-scan -cavitary immages right
VIth segment
Barium radiography:
Esophageal dismotility
SCL70-, U1 RNP(ELISA)
ACA-, ANA + homogenous pattern (IIF on HEp2 cells)
RF 5500 IU (N
-
8/12/2019 Overlap Bis
7/39
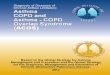
Capillaroscopic patternLATE Scleroderma pattern:
few or absent capillaries and microbleeding, architectural
derangement(angiogenesis), ramified/bushy capillaries
-
8/12/2019 Overlap Bis
8/39
Joint involvement in SS
arthralgias (early-common)
Frank arthritis (rarely)
ContracturesTendon fricture rubs
X-Ray: joint space narrowing 28%, flexioncontractures 27%,
erosions 21%, arthritis 18%Radiological hand involvement in
Systemic Sclerosis. J Avouac, H Guerini, J Wipff, A Kahn, Y
Allanore. Ann Rheum Dis 2006:65
-
8/12/2019 Overlap Bis
9/39
Particularities:
-RF = 5500 IU/ml
(x 550 H normal level)
-anti CCP = 520 IU/ml(x 25 H normal level)
-ANA +
-anti SCL-
-ACA
-U1RNP-
Hands
X-ray
Joint
involvement
Acro-
osteolysis
-
8/12/2019 Overlap Bis
10/39
Problems
Positive diagnosis
Worsening of joint involvement after TB
High titers of anti CCP
Positive ANA-homogenous pattern
Treatment
-
8/12/2019 Overlap Bis
11/39
OVERLAP Syndrome
Positive diagnosis:
-
8/12/2019 Overlap Bis
12/39
Diagnosis: characteristics of thetwo diseases
Clinical features+ or specific
autoantibodies
Thickening of the skin proximal to the fingers (SSc)
Articular erosions (RA)
-
8/12/2019 Overlap Bis
13/39
Overlap Syndrome SSc-ARbecause
Raynauds phenomenon
Diffuse skin involvement
ANA positive, RF highly positive, anti CCPhighly positive
Arthritis of hand joints: MCF, IFP, wrist
Arthritis of 3 joints: MCF, IFP, knee, foot
Symmetric arthritis
Imaging: hand x-ray changes typical of RAmust include
erosions
-
8/12/2019 Overlap Bis
14/39
Anti-cyclic citrullinated peptide antibody in systemic
sclerosis.Morita Y, Clin ExpRheumatol. 2008 Jul-Aug;26(4):542-7
OBJECTIVES: To determine if anti-cyclic citrullinated peptide
(anti-CCP) antibody titers can distinguish the overlap syndrome
of
systemic sclerosis and rheumatoid arthritis (SSc-RA) in
patientswith systemic sclerosis (SSc) and to investigate the
clinical
significance of anti-CCP antibodies in SSc
Elevated serum levels of anti-CCP antibodies wereobserved in 3
of 114 patients (2.6%) with SS, 9 of 14patients (64%) with RA, 6 of
7 patients (86%) with
SS/RA.
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22van%20der%20Veen%20MJ%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22van%20der%20Veen%20MJ%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
8/12/2019 Overlap Bis
15/39
Anti-CCP antibody titers are areliable marker of SSc-RA
facilitating its distinction fromSS alone.
-
8/12/2019 Overlap Bis
16/39
Problems
Positive diagnosis
Worsening of joint involvement after TB
High titers of anti CCP
Positive ANA-homogenous pattern
Treatment
-
8/12/2019 Overlap Bis
17/39
Worsening of joint involvement
TB arthritis- monoarticular
Poncetsdiseaseaseptic polyarthritis(70%) that occurs during
acute TB in whichno mycobacterial involvement can be found.
-self limited-no chronic arthritis reported
-no association reported with anti CCP
-diagnosis of exclusion
-
8/12/2019 Overlap Bis
18/39
Problems
Positive diagnosis
Worsening of joint involvement after TB
High titers of anti CCP & RF
Positive ANA-homogenous pattern
Treatment
-
8/12/2019 Overlap Bis
19/39
Anti-cyclic citrullinated peptide (CCP)antibodies
Relations with RA- sensitivity of 47-76% and specificity of
90-96% for RA
[Nishimura, k, Sugiyama, D, Kogata, Y et al. Meta-analysis:
Diagnostic accuracy of anti-CCp and RF for rheumatoid arthritis.
AnnIntern Med 2007: 146:797]
-when combined with high RF specificity for RA risefrom 90% to
98%
S. Bas, S. Genevay, O. Meyer1and C. Gabay Anti-cyclic
citrullinated peptide antibodies, IgM and IgA rheumatoid factors in
thediagnosis and prognosis of rheumatoid arthritis. Rheumatology,
Vol 42, No5
Relations with SS- positive results can occur in other
diseases:
(15% SLE, 14% SjogrensS, 23% PM, 6% scleroderma)
[Matsui, T, Shimada, K, Ozawa, N, et al. Diagnostic utility of
Anticitrullinated protein/peptide Ab in early rheumatoidarthritis,
J Rheumatol 2006; 33:2390]
-
8/12/2019 Overlap Bis
20/39
Increased prevalence in patients with active TB (32-39%)
32% (2.6% control, p=0.002)-no correlation found betweenanti
CCP+ and any rheumatologic symptoms
No association between anti CCP and RF+
False positivity of anti CCP in TB patients ?
Anti-CCP was inhibited by CCP peptide in sera from RApatients,
but not in sera from TB patients.
A slight increase in anti-CCP after initiating treatment for
TB,thereafter the anti-CCP level decreased in 1-2 months
A significant proportion of patients with TB present high titer
of anti CCP or Ig M RF. O Elkayan, R Segal, M Lidgi & D Caspi;
Ann Rheum Dis
doi:10.1136/ard.2005.045229
Patients with pulmonary tuberculosis are frequently positive for
anti-cyclic citrullinated peptide antibodies, but their sera also
react with unmodified arginine-containing peptide (p 1576-1581) P
Kakumanu, H Yamagata, E S. Sobel, W H. Reeves, Edward K. L. C May
31 2008 Arthritis and Rheumatism
Anti-cyclic citrullinated peptide (CCP)antibodies
Relation with TB
-
8/12/2019 Overlap Bis
21/39
Problems
Positive diagnosis
Worsening of joint involvement after TB
High titers of anti CCPPositive ANA-homogenous pattern
Treatment
-
8/12/2019 Overlap Bis
22/39
Positive ANA-homogenous pattern
SCL70-, anti centromere-
Anti U1 RNP-
2000ANA-!Drug induced lupus (isoniaside)-Ab anti
histone? (pattern homogenous)
-
8/12/2019 Overlap Bis
23/39
Problems
Positive diagnosis
Worsening of joint involvement after TB
High titers of anti CCPPositive ANA-homogenous pattern
Treatment
-
8/12/2019 Overlap Bis
24/39
Treatment
MTX10mg QW sc
SSZ 2g QD
Medrol 8 mg QD
Aspirin 100mg QD
Nifedipin 20 mg QD
Omeprazole+Metoclopramid
Pulmonary fibrosis Risk of infections/recent TB
Vascular problems
(Raynaud, SRC); ATS
Esophageal dismotility
-
8/12/2019 Overlap Bis
25/39
Last EUSTAR recommendationsfor SSc related skin involvement
Two RCT have shown that methotrexate
improves skin score in early diffuse SSc.Positive effects on
other organ manifestationshave not been established.
Methotrexate may be considered for thetreatment of skin
manifestationsof early
diffuse SSc.
-
8/12/2019 Overlap Bis
26/39
Using MTX for treating the erosive
arthritis
In the literature we found opposed dataregarding the pulmonary
fibrosis: There is no evidence to suggest clinically, from
HRCT assessment or serial pulmonary function
tests, that
low-dose methotrexate is associatedwith chronic interstitial
lung disease. J. K. DawsonRheumatology 2002; 41: 262-26 (Fifty-five
RA patients on methotrexate and 73control patientswith RA were
enrolled for the study. Mean doseof methotrexate was 10.7 mg/week
(S.D. 2.5mg/week) and meanduration of treatment at entry into the
study was 30 (20) months.Twentyper cent of patients with RA treated
with methotrexate had pulmonary fibrosis (PF) on initialHRCT
compared with 23% in the control group. When the patients with and
without PFwerecompared, there was no statistical difference in the
duration (mean difference -4.18 months,P=0.237) or dose (mean
difference -0.8 mg/week P=0.52) of methotrexate therapy.
Meanchanges after2 yr in forced expiratory volume, forced vital
capacity, diffusioncapacity for carbonmonoxide and residual volumes
were not differentin the methotrexate group compared with
thecontrol group.)
Fatal pulmonary fibrosis complicating low dosemethotrexate
therapy of 2 aged rheumatoidarthritis patients .van der Veen MJ,J
Rheumatol. 1995 Sep;22(9):1766-8
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Hirano%20Y%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Hirano%20Y%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Hirano%20Y%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Hirano%20Y%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Hirano%20Y%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Hirano%20Y%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Hirano%20Y%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Hirano%20Y%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
8/12/2019 Overlap Bis
27/39
TREATMENT?
Absence of large controlled trials
Recommendations are based on conventionaltreatment for
associated diseases
BIOLOGICS?
-
8/12/2019 Overlap Bis
28/39
The rationale for using TNFblockers in SSc
Clinical overlap of Ssc with other rheumaticdiseases in which
benefit is well established
Experimental models of lung fibrosis haveresponded to TNF
blockers
The inflammatory nature of skin disease inthe early stages of
diffuse cutaneous Ssc
The presence of a mononuclear cellinfiltrate including monocytes
in skin biopsyspecimens
-
8/12/2019 Overlap Bis
29/39
An open-label pilot study of infliximabtherapy in difuse
cutaneous SscCP Denton, Ann Rheum
Dis published online 9 Sep 2008
a 26 week open-label pilot study in which 16 cases ofdcSSc
received 5 infusions of infliximab (5mg/kg)
Clinical assessment included skin sclerosis score,
scleroderma-HAQ, self-reported functional score andphysician
global VAS. Collagen turnover, skin biopsyanalysis and full safety
evaluation was performed.
In dcSSc infliximab did not show clear benefit at 26 weeksbut
was associated with clinical stabilisation and fall in
twolaboratory markers of collagen synthesis.
The frequency of suspected infusion reactions maywarrant
additional immunosuppression in any futurestudies in SSc.
-
8/12/2019 Overlap Bis
30/39
High risk of TB reactivation using TNFblockers in patient with a
history of activeTB
ANA positive ( high risk of infusionreactions ) and for that the
necessity ofcombination therapy
Problems:
f
-
8/12/2019 Overlap Bis
31/39
A case of lung tuberculosis in a patient withrheumatoid
arthritis treated with infliximab after
antituberculosis chemoprophylaxis with
isoniazid. The patient was treated with methotrexate and
prednisolone, but the disease activity remained high.
Atuberculin skin test was positive. After antituberculosis
(TB) chemoprophylaxis with isoniazid for four weeks,infliximab
was administered. Chemoprophylaxis wascontinued for nine months.
Active lung TB was diagnosedat 17 months after the cessation of
isoniazid, namely at27 months after starting infliximab
treatment.
This case report shows that TB can manifest
afterchemoprophylaxis in patients treated withantitumor necrosis
factor agents.
Hirano Y, Mod Rheumatol. 2009 Mar 6.
-
8/12/2019 Overlap Bis
32/39
Tuberculosis in patients receiving anti-
TNF agents despite chemoprophylaxis.
Anti-tuberculosischemoprophylaxis was only ofpartial preventive
success inthe pacients receiving TNF
agents.
Sichletidis L,Int J Tuberc Lung Dis. 2006 Oct
Long-term folow up of patients with TB as a
-
8/12/2019 Overlap Bis
33/39
Long term folow up of patients with TB as acomplication of TNF
alfa antagonist therapy: safere-initiation of TNF alfa blockers
after appropriate
anti TB treatmentDenis B, Clin. Microbiol. Infec.2008
21 TB cases complicating TNF alfa blocker
therapy
29 % patients had recommenced TNF alfaantagonist treatment after
appropriate anti
TB therapy, without reactivation
Conclusions: TNF alfa antagonist can berestarted in TB patients
provided thatadequate anti TB treatment has been
completed
-
8/12/2019 Overlap Bis
34/39
Other possibilities ?
In recent years, clinical trials with B cell
depleting agents, unveiled a role for Blymphocytes in the
pathogenesis of severalauto-immune diseases. Multiple elements
pointto a role for B cells in Ssc pathogenesis.
B ll d l i i h i i b i
-
8/12/2019 Overlap Bis
35/39
B cell depletion with rituximab inpatients with diffuse
cutaneous
systemic sclerosis (15 pz)
The treatment with rituximab appeared to be safeand well
tolerated among patients with dcSSc.Rituximab treatment resulted in
both depletion ofcirculating B cells and depletion of dermal B
cells buthad little effect on the levels of
SSc-associatedautoantibodies. Rituximab treatment did not appear
toresult in a significant beneficial effect on skin disease.The
potential efficacy of rituximab in other organssuch as the lung
could not be clearly evaluated in this
small open-label trial. The modest B cell infiltrates that were
present
in most skin biopsy specimens at baseline werecompletely
depleted at 6 months in most patientsLafyatis R, Arthritis Rheum.
2009 Feb
Rituximab in diffuse cutaneous systemic
-
8/12/2019 Overlap Bis
36/39
Rituximab in diffuse cutaneous systemic
sclerosis: an open-label clinical and
histopathological study
Vanessa P Smith,Ann Rheum Dis published online 22 Dec 2008
Ritixumab induced effective B cell depletion in all
patients(
-
8/12/2019 Overlap Bis
37/39
Rituximab for the treatment ofcutaneous involvement in
Systemic
sclerosis (10 pz)
Despite limitations of few patients, no
control group and short follow up period,
rituximab seems be a safe therapeuticoption for skin fibrosis
and to confirm therole of B cells and autoantibody mediated
fibroblast activation in systemic sclerosis.
P. Fraticelli,Ann. Rheum Dis 2007
-
8/12/2019 Overlap Bis
38/39
Systemic sclerosis-rheumatoid arthritis
overlap syndrome: literature
77% lcSSc, 23% dcSScThe diagnosis of RA followed that of SS
-86.4%
82% erosive poliartritis (xRay)
77% pulmonary fibrosis & 55% oesophageal involv.Genetics:
both SSc and RA- associated HLA-DR alleles
Systemic sclerosis-rheumatoid arthritis overlap syndrome: a
unique combination of features suggests s distinct
genetic, serological and clinical entity. G. Szcs1,*,Z.
Szekanecz1,*, E. Zilahi2, A. Kapitny2,3, S. Barth2, S.Szamosi1 A. V
vri1 Z. Szab1 S. Sznt1 L. Czir k4and C. G r Kiss4Rheumatolo 2007
46:989-993
ANA +: 100%Anti SCL70 +: 22.7%ACA +: 9.1%RF +: 72.7%Anti CCP +:
81.8%
P bl
-
8/12/2019 Overlap Bis
39/39
Problems
Positive diagnosis
Worsening of joint involvement after TB
High titers of anti CCPPositive ANA-homogenous pattern
Treatment
Opinions & Suggestions