Embed Size (px)
Citation preview
Overall survival (OS) results from PARAMOUNT study of maintenance Pemetrexed plus best
supportive care (BSC) versus Placebo plus BSC, immediately after induction with Pemetrexed-
Cisplatin, in patients with advanced Nonsquamous Non-small Cell Lung Cancer (NS-NSCLC)
J. Corral1, 2 L. Paz-Ares1, 2, F. De Marinis3, M. Dediu4, M. Thomas5, J. L. Pujol6, P. Bidoli7, O. Molinier8, T. P. Sahoo9, C. Gridelli10 et al*
1Instituto de Biomedicina de Sevilla, 2University Hospital Virgen del Rocío, Seville, Spain; 3San Camillo–Forlanini Hospital,
Rome, Italy; 4Institute of Oncology Bucharest, Bucharest, Romania; 5Thoraxklinik, University of Heidelberg, Heidelberg, Germany; 6Montpellier CHRU Academic Hospital, Montpellier, France; 7Medical Oncology Unit, S. Gerardo Hospital, Monza,
Italy; 8Le Mans Regional Hospital, Le Mans, France; 9Jawaharlal Nehru Cancer Hospital and Research Center, Bhopal, India; 10San Giuseppe Moscati Hospital, Avellino, Italy
*M. Reck (Hospital Grosshansdorf, Grosshansdorf, Germany), E. Laack (University Medical Center Hamburg-Eppendorf, Hamburg, Germany) , S. A. Melemed, W. J. John, A. Zimmermann (Eli Lilly and Company, Indianapolis, IN, USA), N. Chouaki (Eli Lilly and Company, Suresnes, Hauts de Seine, France), and C. M. Visseren-Grul (Eli Lilly and Company,
Houten, The Netherlands) have participated as co-authors.

Background
Most patients have stage IIIB/IV NSCLC when diagnosed1
Platinum-based combinations are recommended for first-line
treatment2
Pemetrexed has demonstrated efficacy in advanced non-
squamous NSCLC (NS-NSCLC):
─ in combination with cisplatin as first-line doublet3
─ as maintenance agent following non-pemetrexed platinum doublet4
PARAMOUNT evaluated pemetrexed maintenance after
pemetrexed + cisplatin induction:
─ Primary endpoint was met: pemetrexed reduced risk of disease
progression over placebo (HR: 0.62 [0.49-0.79], Wald P<0.0001) 5
─ Final survival analysis occurred after ≥390 deaths;
log-rank test compared OS between arms, with α level of 0.0498
1 http://seer.cancer.gov/statfacts/html/lungb.html; 2Azzoli CG et al. J Clin Oncol. 2009; 3Scagliotti GV et al. J Clin Oncol. 2008; 4Ciuleanu T et al. Lancet 2009; 5Paz-Ares L et al. Lancet Oncol. 2012.

PARAMOUNT: Study Design
Induction Therapy 4 cycles, q21d
Continuation Maintenance Therapy q21d until PD
Pemetrexed + BSC
Placebo + BSC
Pemetrexed
+ Cisplatin
CR/PR/SD per
RECIST
R 2:1
Stratified for:
• PS (0 vs 1)
• Disease stage (IIIB vs IV) prior to induction
• Response to induction (CR/PR vs SD)
Randomized, placebo-controlled, double-blind phase III study
Pemetrexed 500 mg/m2; Cisplatin 75 mg/m2
Folic acid and vitamin B12 administered to both arms
• Previously
untreated
• PS 0/1
• Stage IIIB-IV
NS-NSCLC
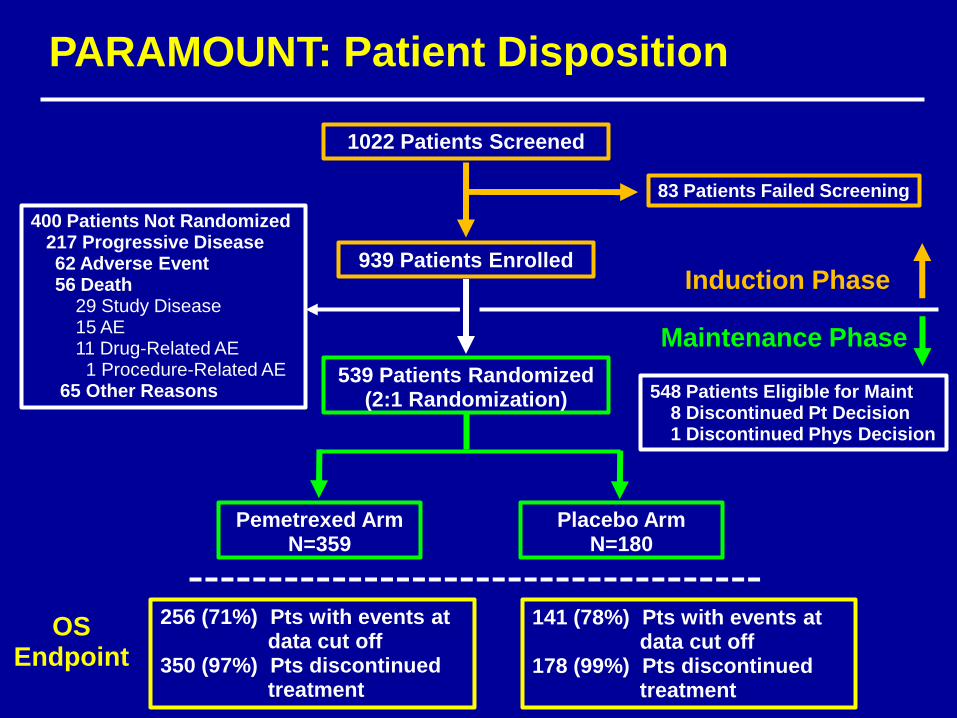
400 Patients Not Randomized 217 Progressive Disease
62 Adverse Event 56 Death 29 Study Disease 15 AE 11 Drug-Related AE 1 Procedure-Related AE 65 Other Reasons
1022 Patients Screened
939 Patients Enrolled
539 Patients Randomized (2:1 Randomization)
Pemetrexed Arm N=359
Placebo Arm N=180
83 Patients Failed Screening
Induction Phase
Maintenance Phase
256 (71%) Pts with events at data cut off 350 (97%) Pts discontinued treatment
141 (78%) Pts with events at data cut off 178 (99%) Pts discontinued treatment
PARAMOUNT: Patient Disposition
548 Patients Eligible for Maint 8 Discontinued Pt Decision 1 Discontinued Phys Decision
OS Endpoint

PARAMOUNT: Patient Characteristics
*Protocol violations.
Pemetrexed
(N=359)
Placebo
(N=180)
Age
Median Age, yrs 61 62
< 65 yrs, % 66 62
Male, % 56 62
Caucasian, % 94 95
Smoker, %
Ever Smoker 76 80
Never Smoker 23 19
ECOG PS, %
0 32 33
1 68 66
2/3* 0.3 1
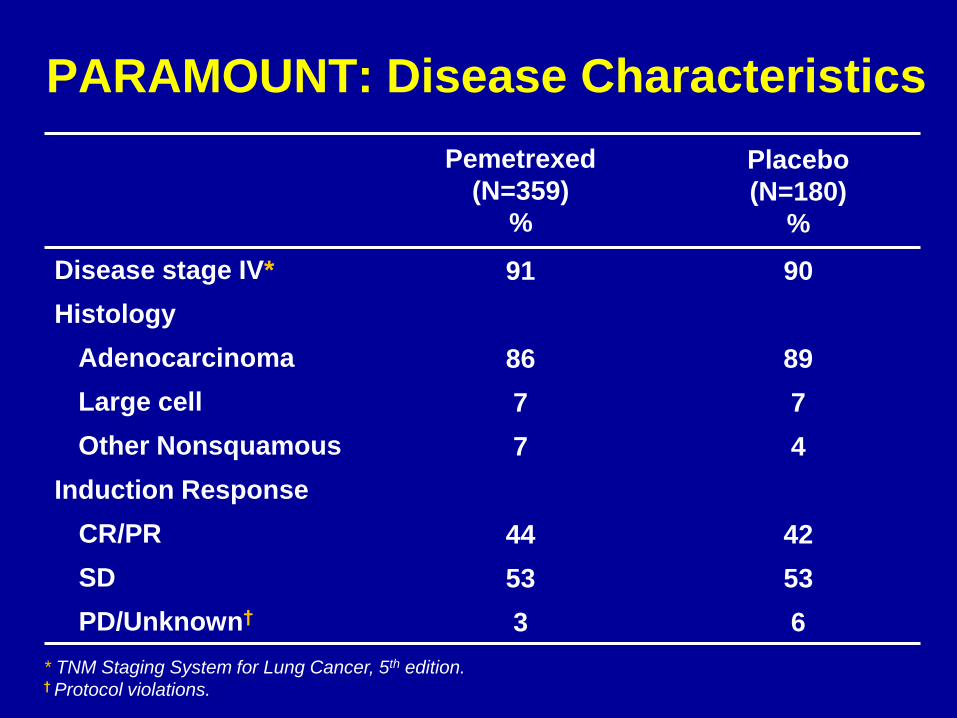
PARAMOUNT: Disease Characteristics
Pemetrexed
(N=359)
%
Placebo
(N=180)
%
Disease stage IV* 91 90
Histology
Adenocarcinoma 86 89
Large cell 7 7
Other Nonsquamous 7 4
Induction Response
CR/PR 44 42
SD 53 53
PD/Unknown† 3 6
* TNM Staging System for Lung Cancer, 5th edition. † Protocol violations.
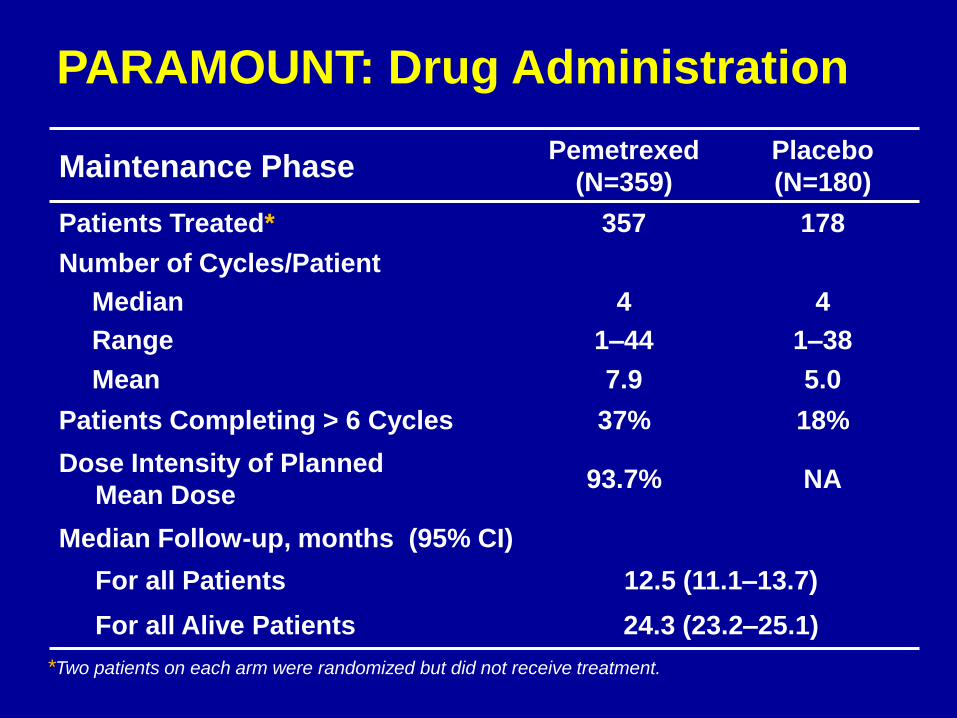
PARAMOUNT: Drug Administration
Maintenance Phase Pemetrexed
(N=359)
Placebo
(N=180)
Patients Treated* 357 178
Number of Cycles/Patient
Median 4 4
Range 1–44 1–38
Mean 7.9 5.0
Patients Completing > 6 Cycles 37% 18%
Dose Intensity of Planned
Mean Dose 93.7% NA
Median Follow-up, months (95% CI)
For all Patients 12.5 (11.1–13.7)
For all Alive Patients 24.3 (23.2–25.1)
*Two patients on each arm were randomized but did not receive treatment.

PARAMOUNT: Patient Discontinuation
Reasons for Discontinuation
Pemetrexed
(N=359)
%
Placebo
(N=180)
%
Progressive Disease 69 84
Adverse Event 18 7
Subject Decision 6 4
Investigator Decision 1 1
Death 2 2
Study Disease 0.8 0.6
Adverse Event/Toxicity 1 2

PARAMOUNT: Final OS from Randomization
Patients at Risk
Pem + BSC 359 333 272 235 200 166 138 105 79 43 15 2 0
Placebo + BSC 180 169 131 103 78 65 49 35 23 12 8 3 0
Time from Randomization (Months)
0 3 6 9 12 15 18 21 24 27 30 33 36
Su
rviv
al
Pro
bab
ilit
y
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Pem Placebo
OS Median (mo)
(95% CI)
13.9
(12.8-16.0)
11.0
(10.0-12.5)
Censoring (%) 28.7 21.7
Survival Rate (%) (95% CI)
1-year 58 (53-63) 45 (38-53)
2-year 32 (27-37) 21 (15-28)
Pemetrexed
Placebo
Log-rank P = 0.0195
Unadjusted HR: 0.78
(95% CI: 0.64–0.96)
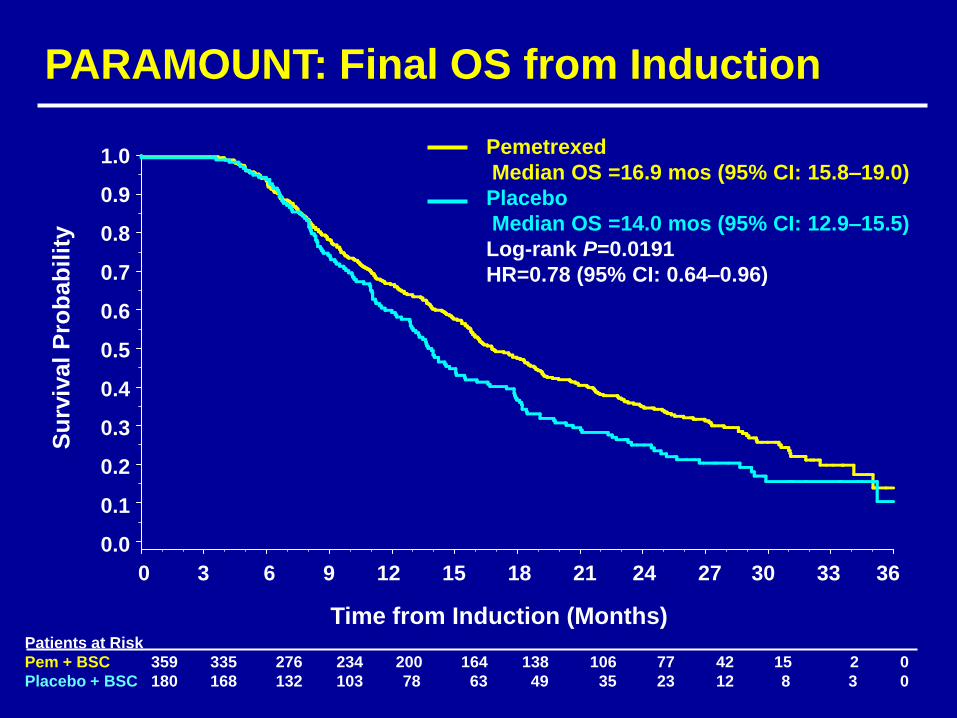
PARAMOUNT: Final OS from Induction S
urv
ival
Pro
bab
ilit
y
Time from Induction (Months)
0 3 6 9 12 15 18 21 24 27 30 33 36
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Pemetrexed
Median OS =16.9 mos (95% CI: 15.8–19.0)
Placebo
Median OS =14.0 mos (95% CI: 12.9–15.5)
Log-rank P=0.0191
HR=0.78 (95% CI: 0.64–0.96)
Patients at Risk
Pem + BSC 359 335 276 234 200 164 138 106 77 42 15 2 0
Placebo + BSC 180 168 132 103 78 63 49 35 23 12 8 3 0
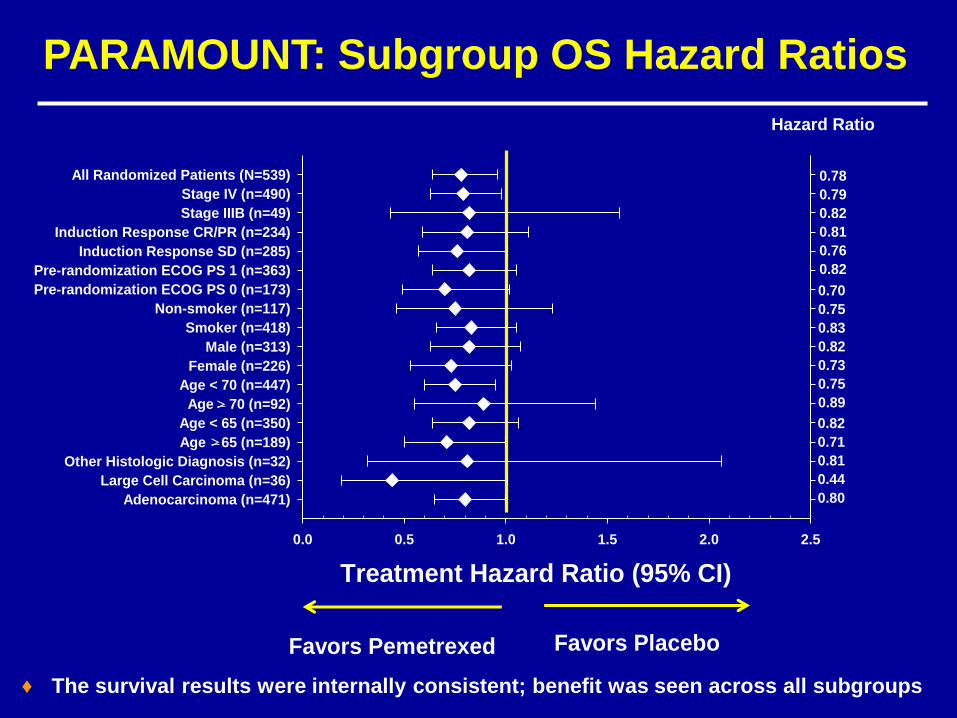
Favors Pemetrexed Favors Placebo
Hazard Ratio
0.78
0.79
0.82
0.81
0.76
0.82
0.70
0.75
0.83
0.82
0.73
0.75
0.89
0.82
0.71
0.81
0.44
0.80
Treatment Hazard Ratio (95% CI)
0.0 0.5 1.0 1.5 2.0 2.5
Adenocarcinoma (n=471)
Large Cell Carcinoma (n=36)
Other Histologic Diagnosis (n=32)
Age 65 (n=189)
Age < 65 (n=350)
Age 70 (n=92)
Age < 70 (n=447)
Female (n=226)
Male (n=313)
Smoker (n=418)
Non-smoker (n=117)
Pre-randomization ECOG PS 0 (n=173)
Pre-randomization ECOG PS 1 (n=363)
Induction Response SD (n=285)
Induction Response CR/PR (n=234)
Stage IIIB (n=49)
Stage IV (n=490)
All Randomized Patients (N=539)
PARAMOUNT: Subgroup OS Hazard Ratios
♦ The survival results were internally consistent; benefit was seen across all subgroups

PARAMOUNT: Induction Response Subgroups OS Hazard Ratios
♦ The survival results were consistent across both induction response subgroups
CR/PR HR = 0.81
SD HR = 0.76
Time from Randomization (Months)
Su
rviv
al p
rob
ab
ility
S
urv
iva
l p
rob
ab
ility
0 9 18 27 36
0 9 18 27 36 0.70
0.75
0.83
0.82
0.73
0.75
0.89
0.82
0.71
0.81
0.44
0.80
0.0 0.5 1.0 1.5 2.0
All Randomized Patients (N=539)
Stage IV (n=490)
Stage IIIB (n=49)
Induction Response CR/PR (n=234)
Induction Response SD (n=285)
Pre-randomization ECOG PS 1 (n=363)
Pre-randomization ECOG PS 0 (n=173)
Non-smoker (n=117)
Smoker )n=418)
Male (n=313)
Female (n=226)
Age < 70 (n=447)
Age > 70 (n=92)
Age < 65 (n=350)
Age > 65 (n=189(
Other Histologic Diagnosis (n=32)
Large Cell Carcinoma (n=36)
Adenocarcinoma (n=471)
0.78
0.79
0.82
0.81
0.76
0.82
Hazard Ratio
Treatment Hazard Ratio (95%% CI)
Favors Pemetrexed Favors Placebo

Time (Months)
0 3 6 9 12 15
Su
rviv
al P
rob
ab
ilit
y
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
PFS: Primary Efficacy Endpoint
Pemetrexed
Placebo
Unadjusted HR: 0.62 (0.49-0.79)
Patients at Risk
Pem + BSC 359 132 57 21 4 0
Plac+ BSC 180 52 15 5 0 0
0 3 6 9 12 15 18 21 24 27 30 33
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
PFS: Reassessed at Time of Final OS
Pemetrexed
Placebo
Unadjusted HR: 0.60 (0.50-0.73)
Su
rviv
al
Pro
ba
bil
ity
Time (Months)
Patients at Risk
Pem +BSC 359 215 139 97 67 47 32 22 16 10 5 0
Plac + BSC 180 75 33 16 9 7 6 4 2 0 0 0
PARAMOUNT: PFS from Randomization

PARAMOUNT: Post-discontinuation Therapy
Pemetrexed
(N=359)
%*
Placebo
(N=180)
%*
Patients Receiving Post
Discontinuation Therapy 64 72
Erlotinib 40 43
Docetaxel† 32 43
Gemcitabine 10 8
Vinorelbine 8 6
Investigational drug 6 4
Carboplatin 5 4
Paclitaxel 3 3
Pemetrexed 2 4
Cisplatin 1 2 *Data expressed as % of randomized patients. Systemic therapies used in ≥2% of patients in either arm
are shown. †Only docetaxel usage differed significantly between arms (P=0.013).
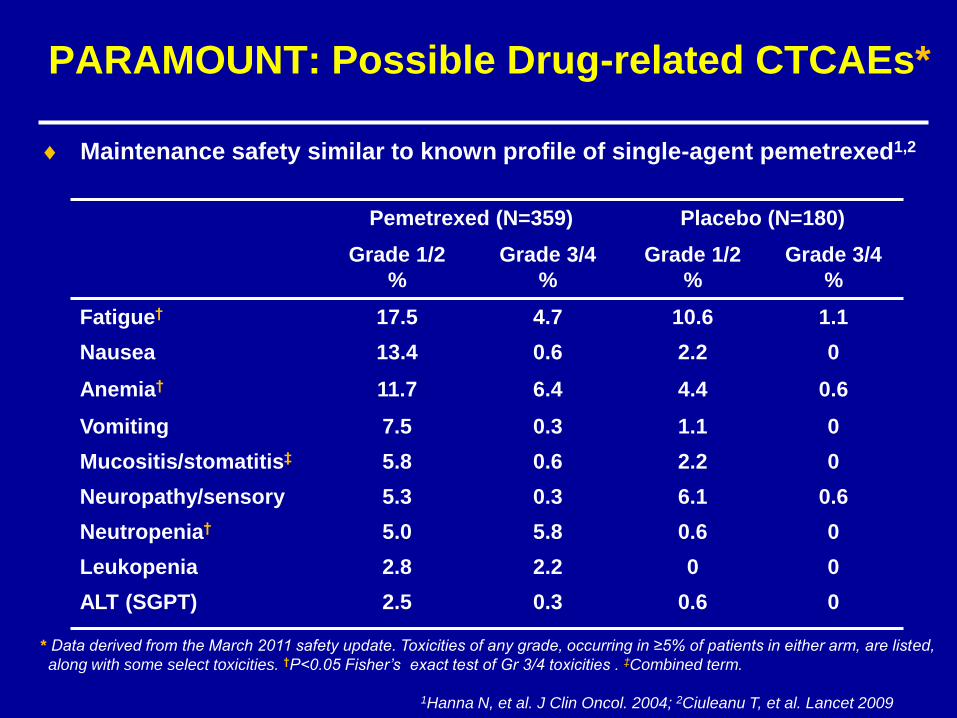
PARAMOUNT: Possible Drug-related CTCAEs*
Pemetrexed (N=359) Placebo (N=180)
Grade 1/2
%
Grade 3/4
%
Grade 1/2
%
Grade 3/4
%
Fatigue† 17.5 4.7 10.6 1.1
Nausea 13.4 0.6 2.2 0
Anemia† 11.7 6.4 4.4 0.6
Vomiting 7.5 0.3 1.1 0
Mucositis/stomatitis‡ 5.8 0.6 2.2 0
Neuropathy/sensory 5.3 0.3 6.1 0.6
Neutropenia† 5.0 5.8 0.6 0
Leukopenia 2.8 2.2 0 0
ALT (SGPT) 2.5 0.3 0.6 0
* Data derived from the March 2011 safety update. Toxicities of any grade, occurring in ≥5% of patients in either arm, are listed,
along with some select toxicities. †P<0.05 Fisher’s exact test of Gr 3/4 toxicities . ‡Combined term.
Maintenance safety similar to known profile of single-agent pemetrexed1,2
1Hanna N, et al. J Clin Oncol. 2004; 2Ciuleanu T, et al. Lancet 2009
PARAMOUNT: Conclusions
These final results show that survival is significantly
improved when patients are treated with pemetrexed
continuation maintenance therapy compared with
placebo (HR=0.78)
The survival results were internally consistent across
all subgroups, including response to induction
(complete/partial response versus stable disease)
PARAMOUNT is the first study to show continuation
maintenance has an impact on the disease course of
advanced NSCLC (including PFS and OS), supporting
a change in the treatment paradigm in this setting

Acknowledgements
We thank all of the patients and their caregivers for participating in this
trial. We also thank all the Investigators and their support staff who
generously participated in this work with a special mention to the Spanish
Investigators:
• D. Isla (Hospital Clínico Universitario Lozano Blesa, Zaragoza, España)
• Y. García (Hospital Universitari Parc Tauli, Sabadell, España)
• D. Almenar (Hospital Universitario Dr. Peset, Valencia, España)
• R. Bernabé (Hospital Universitario de Valme, Sevilla, España)
• M. Domenech (Hospital Althaia de Manresa, Barcelona, España)





























