Embed Size (px)
Citation preview

SCAN Audit Office, c/o Department of Clinical Oncology, Western General Hospital, Crewe Road, Edinburgh, EH4 2XU T: 0131 537 2266 F: 0131 537 2076 W: www.scan.scot.nhs.uk [email protected]
SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT
OVARIAN CANCER 2012
COMPARATIVE AUDIT REPORT Dr Melanie Mackean, NHS Lothian SCAN Lead Ovarian Cancer Clinician Dr Scott Fegan, NHS Fife & NHS Lothian Dr Adrian McCullough, NHS Dumfries and Galloway Dr Phillip Dutton, NHS Dumfries and Galloway Dr Queenie Menezes, NHS Borders Dr Graeme Walker, NHS Lothian Dr Lorna Bruce, NHS Lothian SCAN Ovarian Cancer Audit Facilitator Martin Keith, Cancer Audit Facilitator, NHS Dumfries and Galloway Alistair Meikle, Cancer Audit Facilitator, NHS Borders Jackie Stevenson, Cancer Audit Facilitator, NHS Fife
Report number SA Ov02/14

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02/14 2
Contents
Document History .................................................................................................................. 3
SCAN Chair Commentary...................................................................................................... 4
Change in practice................................................................................................................. 6
Action points from 2011 Audit................................................................................................ 7
Action points from 2012 Audit................................................................................................ 8
Attainment of Standards ........................................................................................................ 9
Introduction and Methods .................................................................................................... 12
1. Estimated Case ascertainment........................................................................................ 13
3. Referral Process .............................................................................................................. 15
3.1 Specialties into which patients were initially referred in SCAN 2012 ........................ 15
3.2 Time from referral to first treatment ........................................................................... 16
3.3 Time from Decision to Treat to First Treatment......................................................... 17
3.4 Time from definitive surgery to start of chemotherapy .............................................. 18
4. Investigations................................................................................................................... 19
5. Preoperative Preparations............................................................................................... 20
6. Surgical Treatment .......................................................................................................... 21
6.1 NHS QIS 6a ............................................................................................................... 21 6.1a SIGN 75 4.4: ........................................................................................................ 22
6.2 Fertility Preserving Surgery ....................................................................................... 23
6.4 Surgical Incision......................................................................................................... 24
6.5 Washings / ascitic fluid sampling............................................................................... 25
6.6 Primary cytoreductive surgery ................................................................................... 26 6.6.1 All patients having hysterectomy........................................................................ 26 6.6.2 Patients having unilateral or bilateral oophorectomy.......................................... 27
6.7 Omentectomy / omental biopsy ................................................................................. 27
6.8 Record of Residual disease....................................................................................... 28
6.9 Surgical Assessment FIGO ....................................................................................... 28
7. Post operative management: Pathology.......................................................................... 29
7.1 Type/Sub-Type .......................................................................................................... 29
7.2 Grade of Disease....................................................................................................... 29
7.3 Final FIGO on pathology report ................................................................................. 30
7.4 Final FIGO – All Patients ........................................................................................... 30
8. Chemotherapy management ........................................................................................... 31
9. Post Chemo surgery / Delayed primary surgery ............................................................. 32
10. Clinical Trials ................................................................................................................. 33
11. Outcomes ...................................................................................................................... 34
11.1 Thirty Day Mortality.................................................................................................. 34 11.1a Post Operative Deaths....................................................................................... 34 11.1b Post Chemotherapy Deaths .............................................................................. 34 11.1c Post Treatment deaths....................................................................................... 35
11.2 Residual Disease..................................................................................................... 36
11.3 Survival: ................................................................................................................... 38

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02/14 3
12. Multidisciplinary Meeting................................................................................................ 39
13. Quality Performance Indicators (QPI)............................................................................ 40
QPI 4................................................................................................................................ 40
QPI 5................................................................................................................................ 41
QPI 7................................................................................................................................ 42
QPI 8................................................................................................................................ 42
QPI 9................................................................................................................................ 43
Appendix 1........................................................................................................................... 44
Ovarian Cancer Glossary of Terms ..................................................................................... 49
Document History
v Date Events Actions
1 1/11/2013 Circulated to Lead clinicians prior to meeting.
2 8/11/2013 Discussed at clinical leads meeting
Some typos. QPIs required re-calculating. Published waiting times requested from ISD.
3 15/1/2014 Amended draft circulated to SCAN Group
Clarification required for Dumfries DPS patients – comments added. Fife QPI5 typo corrected
3 30/1/2014 Final draft circulated to SCAN Gynae group
4 18/02/2014
Final report circulated to the Health Board Clinical Governance Groups and to the RCPG. Also numbered and lodged on audit report index.
4w December 2014 Published to website

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02/14 4
SCAN Chair Commentary SCAN Audits are performed against nationally agreed standards. Up until 2013 for ovarian cancer these were the SIGN 75 guideline and the NHS Quality improvement Standards. However scientific knowledge, technical skills and medicines move forward and in 2013 these have been updated to the SIGN 135 guideline and the NHS Quality Performance Indicators (QPI) respectively. This audit follows the previous national audit data set but we have tried to also include some of the newer QPIs as a ‘benchmark’ for future audits which will be based on the data set for the QPIs. In 2015 the first full report on Ovarian cancer QPIs will be available. This SCAN 2012 audit shows an excellent compliance with both new and old standards. There is, however, always room for improvement and it is hoped that the development of both a standard operating form and a new dedicated theatre time for complex pelvic cancer surgery at the WGH will see improvements in future audits. The pathway to chemotherapy following surgery will also be subject to further analysis to see if any improvements can be made and unnecessary delays avoided. My personal thanks go to all the hardworking staff who treat these patients and the audit team for their dedicated approach in producing this report. Melanie Mackean SCAN gynae group chair Dec 2013

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02/14 5
RMI (Risk of Malignancy Index) and the difficulties to diagnose ovarian cancer on this index Every effort is made to diagnose ovarian cancer before an operation, however roughly only one in every 3 ovarian cysts will be cancer; the other 2 will be benign disease. To avoid overburdening cancer services with benign disease gynaecologists will calculate the RMI, using a combination of ultrasound and CA125 blood level. This again is not perfect but helps identify most patients very likely or very unlikely to have ovarian cancer. This tool is discussed well in the NICE guidelines on early detection of ovarian cancer published in 2011: ‘The evidence for this topic comprised one good quality systematic review of diagnostic studies (Geomini et al., 2009) in which the reviewers appraised 109 studies of eighty-three validated risk of malignancy models. By pooling data appropriately the authors concluded that the RMI I proposed by Jacobs et al., (1990) was superior in terms of sensitivity and specificity to the other comparators. With a cut-off score of 200, sensitivity = 78% [95%CI: 71-85%] and specificity = 87% [95%CI: 83-91%] and with a cut-off score of 50, sensitivity = 91% [95%CI: 85-97%] and specificity = 74% [95%CI: 69-80%]. A sensitivity of 78% means, using a cut off RMI score of greater than 200, 78% of women with ovarian cancer will be identified. Sadly it means 22% of ovary cancer patients will have a RMI score less than 200 and not be identified preoperatively.

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02/14 6
Change in practice - Neoadjuvant chemotherapy (NACT ) and delayed primary surgery.
Prior to 2009 it was routine for advanced ovarian cancer (stage IIIC and IV) to be treated with an initial operation and then 6 cycles of chemotherapy. Some patients have very advanced disease and surgery can be risky as well as unsuccessful. There have been studies to see if it is better to have chemotherapy first to shrink the cancer (NACT) then surgery after 3 cycles of chemotherapy (‘interval debulking’ or ‘delayed primary surgery’) followed by 3 further cycles of chemotherapy. The EORTC/NCIC 55971 trial randomly assigned people with advanced ovarian cancer to either of these approaches (surgery first or surgery after chemotherapy-NACT). They showed no difference in overall survival to either approach but a reduction in surgical mortality in the group receiving chemotherapy first (NACT). There has been a move throughout the UK to offer neoadjuvant chemotherapy then surgery in advanced ovarian cancer. In September 2009 a subgroup of the SCAN Gynae group met and formalised a protocol to offer neoadjuvant chemotherapy and delayed primary surgery. This means many more patients are having chemotherapy before surgery since 2009 in SCAN. The SCAN ovarian cancer protocol was updated in 2010 accordingly. This will have some effects on some of the criteria being examined in this audit.
It is now likely that less fit patients will receive chemotherapy rather than surgery as their first treatment. This is likely to increase the post chemotherapy mortality and reduce the post surgical mortality rates.
Current ovarian cancer patient pathway 2012
Follow up only
Adjuvant chemotherapy
x6
Palliative primary
chemotherapy
Adjuvant chemotherapy
x3
Patient diagnosis
Biopsy
Decision for therapy
Best supportive
care
Staginglaparotomy/laparoscopy
Neoadjuvantchemotherapy
Delayed primary surgery
Ca125 / cytology / scan(n = 178)
(n = 21) (n = 117)
(n = 38)(n = 51)
(n = 58)
SCAN Comparative Ovarian Cancer Report 2012 SA Ov02/14 7
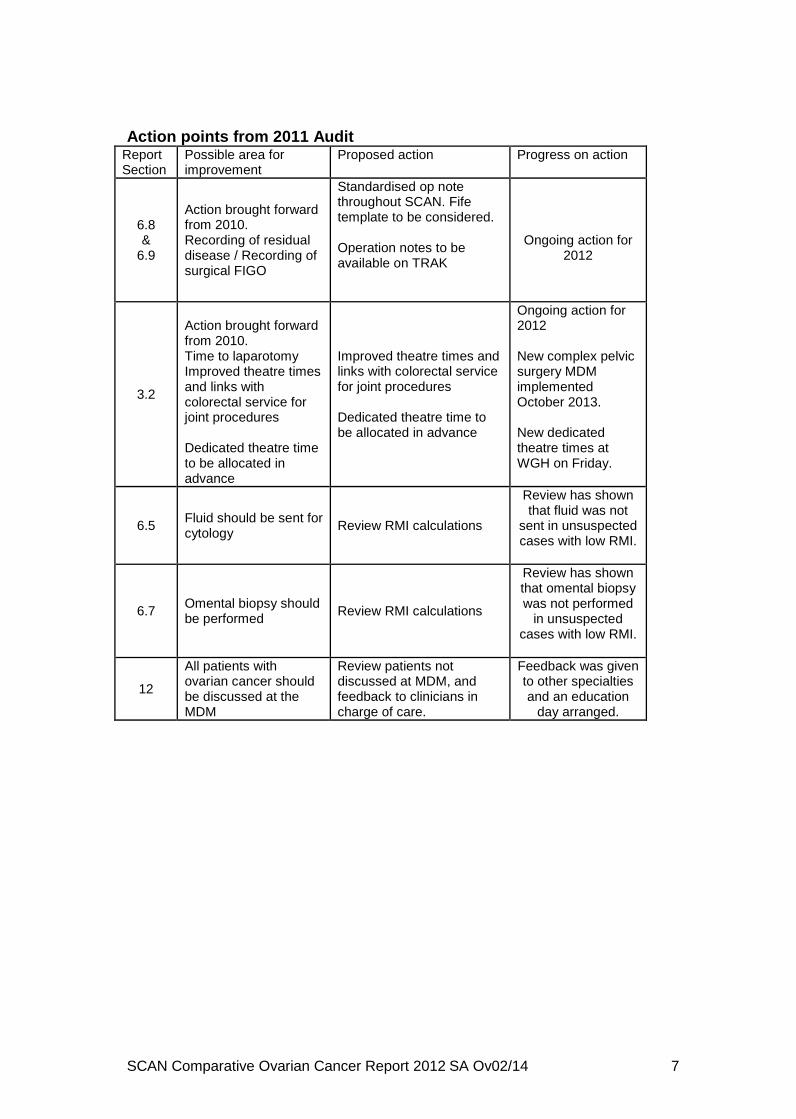
Action points from 2011 Audit
Report Section
Possible area for improvement
Proposed action Progress on action
6.8 &
6.9
Action brought forward from 2010. Recording of residual disease / Recording of surgical FIGO
Standardised op note throughout SCAN. Fife template to be considered. Operation notes to be available on TRAK
Ongoing action for
2012
3.2
Action brought forward from 2010. Time to laparotomy Improved theatre times and links with colorectal service for joint procedures Dedicated theatre time to be allocated in advance
Improved theatre times and links with colorectal service for joint procedures Dedicated theatre time to be allocated in advance
Ongoing action for 2012 New complex pelvic surgery MDM implemented October 2013.
New dedicated theatre times at WGH on Friday.
6.5 Fluid should be sent for cytology
Review RMI calculations
Review has shown that fluid was not
sent in unsuspected cases with low RMI.
6.7 Omental biopsy should be performed
Review RMI calculations
Review has shown that omental biopsy was not performed
in unsuspected cases with low RMI.
12
All patients with ovarian cancer should be discussed at the MDM
Review patients not discussed at MDM, and feedback to clinicians in charge of care.
Feedback was given to other specialties and an education
day arranged.

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02/14 8
Action points from 2012 Audit
Report Section
Possible area for improvement
Proposed action Which clinical standard will this meet?
6.8 &
6.9
Action brought forward from 2010. Recording of residual disease / Recording of surgical FIGO
Standardised op note throughout SCAN. Fife template to be considered. Operation notes to be available on TRAK
NHS QIS 6c5 NHS QIS 6c7
QPI 5
3.2
Action brought forward from 2010. Time to laparotomy Improved theatre times and links with colorectal service for joint procedures Dedicated theatre time to be allocated in advance
New complex pelvic surgery MDM implemented October 2013.
New dedicated theatre times at WGH on Friday.
NHS QIS standard 2a5
3.5 Time from surgery to start of chemotherapy
Audit patient delays and pathways Time from 1st appointment with oncologist to start of chemo will be audited in a separate report.
SIGN 75 Guideline 5.2
13 Agree designated gynae oncologists
SCAN gynae group to agree on which gynaecologists are to be designated in SCAN
QPI 4

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 9
Attainment of Standards Ref Standard Lothian Fife BGH D&G SCAN
3.5 SIGN 75 Guideline 5.2 : Chemotherapy should be started no later than eight weeks after surgery 85.7% 61.5% 75.0% 85.7% 78.6%
NHS QIS 2a1 Minimum investigation: CA125 level to be organised 95.5% 97.2% 87.5% 93.8% 94.9%
4.0 NHS QIS 2a1
Minimum investigation: abdominal and pelvic ultrasound and/or CT scan 100.0% 100.0% 93.8% 100.0% 99.4%
6.1 NHS QIS 6a: All patients with a suspected diagnosis of ovarian cancer are operated on by a designated and trained gynaecological surgeon
100.0% 85.7% 100.0% 100.0% 100.0%
6.1a SIGN 75 4.4: All patients with (FIGO) stage 3 disease should be operated on by a gynaecological oncologist rather than a general gynaecologist or general surgeon. (Surgery as first treatment, excluding delayed primary surgery patients) 100.0% 100.0% 100.0% 100.0% 100.0%
6.2 NHS QIS 6b3: In young women, aged 30 or less, the possibility of germ cell tumours is considered. Fertility conserving surgery is planned and performed at laparotomy. 100.0% 100.0% 100.0% NA 100%
6.4 NHS QIS 6c1: Vertical incision is made 94.0% 95.2% 71.4% 88.9% 92.0%
Less than 75% 75 to 95% Over 95%

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 10
Attainment of Standards
Ref Standard Lothian Fife BGH D&G SCAN
6.5 NHS QIS 6c2: Washings or ascitic fluid should be sent for cytology 80.7% 95.5% 85.7% 100.0% 86.3%
NHS QIS 6c3: Primary cytoreductive surgery to be attempted and to include a total or subtotal hysterectomy 73.6% 76.2% 71.4% 87.5% 75.3%
6.6 NHS QIS 6c3: Primary cytoreductive surgery to be attempted and to include salpingo-oophorectomy 98.2% 100.0% 100.0% 100.0% 98.9%
6.7 NHS QIS 6c4: Omentectomy and/or omental biopsy performed 82.5% 100.0% 85.7% 100.0% 88.4%
6.8 NHS QIS 6c5: Record of residual disease to be made 70.2% 100.0% 100.0% 77.8% 80.0%
6.9 NHS QIS 6c7: FIGO surgical stage is recorded in case notes 50.9% 100.0% 90.0% 33.3% 64.3%
7.2 NHS QIS 8a3: Histological type, sub-type and grade of disease are recorded. 100.0% 100.0% 87.5% 100.0% 94.9%
7.3 NHS QIS 6c8: Final FIGO surgical pathological stage is recorded 100.0% 100.0% 100.0% 100.0% 100.0%
8.1 SIGN 75: 5.5.1A: First line chemotherapy of epithelial ovarian cancer should include a platinum agent either in combination or as a single agent, unless specifically contraindicated.
100.0% 100.0% 100.0% 100.0% 100.0%
12 NHS QIS 3a4: All patients confirmed to have ovarian cancer after surgery are discussed at the MDT meeting and follow up treatment organised. 98.2% 100.0% 93.8% 100.0% 98.3%
Less than 75% 75 to 95% Over 95%

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 11
Draft QPIs Lothian Fife BGH D&G SCAN
QPI 4 i) Percentage of early stage (FIGO Stage 1) epithelial ovarian cancer patients having primary surgery involving TAH, BSO, omentectomy and washings. Target 95%
85.7 77.8 33.3 100.0 75.0
QPI 4 ii) Percentage of early stage (FIGO Stage 1) epithelial ovarian cancer patients having primary surgery involving TAH, BSO, omentectomy and washings operated on by a gynaecological oncologist. Target 95%
100.0 71.4 100.0 100.0 88.9
QPI 5 i) Percentage of patients with advanced epithelial ovarian cancer (FIGO Stage 2 or higher) with no macroscopic residual disease following surgery. Target 30%
72.2 71.4 100.0 50.0 72.7
QPI 5 ii) Percentage of patients with advanced epithelial ovarian cancer (FIGO Stage 2 or higher) undergoing surgery with macroscopic residual disease < 1cm. Target 60%
88.9 71.4 100.0 50.0 63.6
QPI 7. Percentage of patients who have a diagnosis of epithelial ovarian cancer confirmed by histology prior to starting chemotherapy. Target 80%
80.8 100.0 100.0 100.0 87.5
QPI 8 i) Percentage of patients with advanced epithelial ovarian cancer (FIGO Stage 3c or 4) undergoing delayed primary surgery after neo-adjuvant chemotherapy. Target 75%
66.7 90.0 100.0 40.0 70.4
QPI 8 ii) Percentage of patients with advanced epithelial ovarian cancer (FIGO Stage 3c or 4) undergoing delayed primary surgery with residual disease <1cm. Target 65%
79.2 33.3 66.7 50.0 65.8
QPI 9. Percentage of epithelial ovarian cancer patients who receive chemotherapy involving either Paclitaxel in combination with a platinum-based compound or carboplatin only. Target 90%
85.0 100.0 66.7 100.0 87.3

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 12
Introduction and Methods
SCAN Ovarian Cancer Audit Overview This report relates to patients diagnosed with ovarian cancer (including primary peritoneal and Borderline tumours) between 1st January 2012 and 31st December 2012 within the SCAN region of NHS Borders, Fife, D&G and Lothian. Audit Process Identification of patients for audit, plus capture of some data items, is primarily from the regional Multi-disciplinary Meeting held at the Western General Hospital, Edinburgh. Other data is collected from the clinical record (casenotes and electronic systems), GRO (death) lists and pathology lists. Data Capture Data is recorded on Access databases by Audit Facilitators. Datasets and Definitions The Minimum Core Data Set (published September 2001) developed by the Scottish Cancer Therapy Network under the direction of the Scottish Programme for Clinical Effectiveness in Reproductive Health continues to be collected. SIGN Guidelines (75) for Epithelial ovarian cancer were published in October 2003. Nationally agreed general fields for waiting times were added from 1st January 2004. Measures, Analysis and Reporting Data has been analysed in line with national standards set by the NHS Quality Improvement Scotland (NHS QIS) in 2008, and by the Scottish Government Health Department, and is also in line with aspects of the SIGN Guidelines. Clinical Effectiveness Measures are as agreed by Lead Clinicians and approved by the SCAN Gynaecology Group. QPI measures are included where it’s possible using the current dataset. Actual figures for graphs are available by contacting: Lorna Bruce, SCAN Cancer Audit Manager SCAN Audit Office, Western General Hospital. Tel: 0131 537 3570 email: [email protected]. Data and Reporting Quality
• Clinical Sign-Off: This report compares data from reports prepared for individual health board areas and signed off as accurate following review by the lead clinicians from each service. Additionally, the collated SCAN results are reviewed jointly at a meeting of lead clinicians to assess variances and provide comments on results.
• External Quality Assurance of data is carried out by ISD and was performed on the 2010 data with the following percent accuracies recorded: Lothian 95.8%, Fife 97.3%, Borders 86.6% and Dumfries 90.5%.
Case ascertainment for the current reporting period is compared with the latest Scottish Cancer Registration 5 year average.
Actions for Improvement After final sign off, the process is for the report to be sent to the Clinical Governance groups within the four health boards and to the Regional Cancer Planning Group. Action plans and progress with plans will be highlighted to the groups. The report will be placed on the SCAN website once it has been fully signed-off and checked for any disclosive material. Action points for 2012: as part of clinical sign-off areas for improvement are highlighted in the Action Plan 2012. Action points from 2011 results: information is provided on progress with Action Plans for 2011.

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 13
1. Estimated Case ascertainment Cancer Registration data for the 5 years from 2007 to 2011 indicates an annual average of 171 (range 161 – 185) new ovarian cancers diagnosed in SCAN. This compares to 178 patients (104%) recorded in audit during 2012 Scottish Cancer Registry
2007 2008 2009 2010 2011 Average
Lothian 101 93 72 109 103 96
Fife 54 43 38 42 28 41
BGH 13 13 18 11 7 12
D&G 20 13 16 22 18 18
SCAN 185 171 161 184 156 171 Source: Scottish Cancer Registry, ISD (15/10/2013) http://www.isdscotland.org/Health-Topics/Cancer/Cancer-Statistics/ Cancer Registration figures are based on the date the patient first attends hospital, rather than the date of definitive diagnosis and include patients diagnosed though post mortem only.
SCAN Audit registrations
2008 2009 2010 2011 2012 Average
Lothian 84 86 105 105 110 98
Fife 44 31 40 28 36 36
BGH 9 12 11 7 16 11
D&G 11 14 23 18 16 16
SCAN 148 143 179 158 178 161
SCAN Audit figures for 2012 compared with 5 year Cancer Registry average from 2007 - 2011
% Estimated Case Ascertainment.
Lothian 115
Fife 88
BGH 129
D&G 90
SCAN 104

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 14
2. Age at Diagnosis Age of patients at diagnosis: n = 178 All patients
Patient age Lothian Fife BGH D&G SCAN <40 12 3 2 0 17
40-59 15 2 0 1 18 50-59 17 7 3 3 30 60-69 28 11 2 5 46 70-79 23 9 4 4 40
>80 15 4 5 3 27 Total 110 36 16 16 178
Median age: 66 Range: (15-91)

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 15
3. Referral Process
3.1 Specialties into which patients were initially referred in SCAN 2012 .
Gynaecology(69%)
Non - Gynaecology
(31%)
Routes to diagnosis for ovarian cancer, England (2007) Ovarian cancer patients (n = 5012) %
Two Week Wait 26 GP referral 22
Other outpatient 15 Inpatient elective 1
Emergency presentation 29 Death Certificate Only 1
Unknown 6 Total 100
This concern about ovarian cancer presenting late and to emergency departments has led to the NICE guideline, ‘Ovarian cancer: the recognition and initial management of ovarian cancer’ being published in 2011’ with several key recommendations. There has been a Scottish wide initiative to ‘Detect cancer early’. As part of this initiative a new tumour markers bookmark has been developed in early 2012 for all GPs including guidance on CA125 testing. This is being disseminated through work in the Scottish Primary Care Cancer Group. In SCAN gynae group a protocol and pathway for raised CA125 has been developed for GPs in Lothian to aid in this initiative.

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 16
3.2 Time from referral to first treatment : All Referrals NHS QIS 2a5: Assessment, investigations, treatment planning and first treatment are completed within 62 days of first referral in accordance with Scottish Government Health Department guidelines. n = 170. All patients, excluding 3 that declined treatment and 3 that died before treatment and 2 Lothian patients with no referral date recorded.
Ovarian Cancer Patients - SCAN 2012 Time from referral to treatment
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
7 14 21 28 35 42 49 56 62 >62
Time (days)
% p
atie
nts
Lothian
Fife
BGH
DGRI
SCAN
2012 Lothian Fife BGH D&G SCAN n 105 35 15 15 170
Median (days) 42 50 39 42 43 Range 0-418*
0-125
4-90
14-151
0-418
*418 days: Patient was initially referred to gastroenterology and was diagnosed with a borderline ovarian tumour.
SCAN data 2007* 2008 2009 2010 2011 2012 n 150 140 120 174 154 170
Median (days) 36* 38.5 44 43 33 43 Range 0 - 435 0 - 179 0-229 0 - 297 0-351 0-418
*Excluding BGH data, which are not available 76.5% of patients were treated within 62 days of referral in SCAN.
SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 17
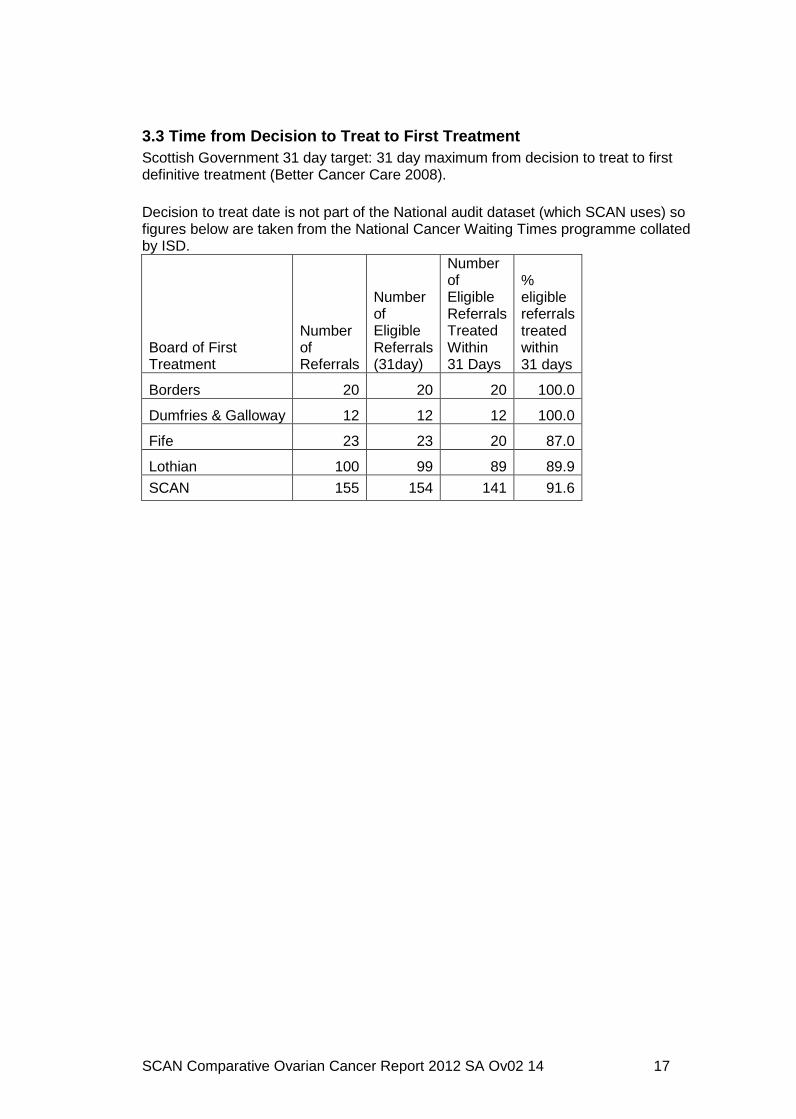
3.3 Time from Decision to Treat to First Treatment Scottish Government 31 day target: 31 day maximum from decision to treat to first definitive treatment (Better Cancer Care 2008). Decision to treat date is not part of the National audit dataset (which SCAN uses) so figures below are taken from the National Cancer Waiting Times programme collated by ISD.
Board of First Treatment
Number of Referrals
Number of Eligible Referrals (31day)
Number of Eligible Referrals Treated Within 31 Days
% eligible referrals treated within 31 days
Borders 20 20 20 100.0
Dumfries & Galloway 12 12 12 100.0
Fife 23 23 20 87.0
Lothian 100 99 89 89.9
SCAN 155 154 141 91.6

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 18
3.4 Time from definitive surgery to start of chemot herapy SIGN 75 Guideline 5.2 : Chemotherapy should be started no later than eight weeks after surgery Time from definitive surgery to start of chemotherapy n = 52. All patients who had surgery followed by chemotherapy
Ovarian Cancer Patients - SCAN 2012Time from surgery to chemotherapy
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
7 14 21 28 35 42 49 56 >56
Time (days)
% p
atie
nts
Lothian
Fife
BGH
DGRI
SCAN
2012 Lothian Fife BGH D&G SCAN n 28 13 4 7 52
Median (days) 39.5 49.0
46.5
40.0
41.0
Range 28-103
34-142*
35-85
20-60
20-142
% SIGN guideline compliance
85.7%
61.5%
75.0%
85.7%
78.6%
*142 days: Patient had post surgical complications.
SCAN data 2007 2008 2009 2010 2011 2012
n 78 65 31 43 25 52
Median (days) 34 34 41 37 42.0 41.0
Range 10-98 15-105 17-132 17-110 23- 93 20-142 % Compliance
SIGN 89.0 90.8 80.6 93.0 92.0 78.6
ACTION - Time from 1st appointment with oncologist to start of chemo will be audited in a separate report.

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 19
4. Investigations NHS QIS 2a1: The following basic investigations are to be organised once ovarian cancer is suspected or a mass detected: CA125 level; abdominal and pelvic ultrasound and/or CT scan. n = 178. All patients
Lothian Fife BGH D&G SCAN CA 125 n % n % n % n % n %
Performed 105 95.5 35 97.2 14 87.5 15 93.8 169 94.9
Not performed 5 4.5 1 2.8 2 12.5 1 6.3 9 5.1
Not recorded
0 0.0 0 0.0 0 0.0 0 0.0 0 0.0
Total 110 100 36 100 16 100 16 100 178 100
Comment: This is an excellent result. There will always be emergency cases and unexpected surprise diagnoses. % Performed in previous years
Year Lothian Fife BGH D&G SCAN 2006 97.4 96.4 92.9 100 96.9 2007 95.9 96.2 87.5 100 96.0 2008 97.6 93.2 88.9 100 95.9 2009 97.7 100 91.7 No data 97.7 2010 95.2 97.5 90.9 100 96.1 2011 95.2 100 100 94.4 96.2 2012 95.5 97.2 87.5 93.8 94.9
n = 159. All patients, excluding 19 patients with stage 1 Borderline tumours
Lothian Fife BGH D&G SCAN Imaging n % n % n % n % n %
Performed 95 100.0 33 100.0 15 93.8 15 93.8 158 99.4
Not performed
0 0.0 0 0.0 1 6.3 0 0.0 1 0.6
Not recorded
0 0.0 0 0.0 0.0 0 0.0 0 -
Total 95 100.0 33 100.0 16 100.0 15 93.8 159 100
% Performed in previous years (All patients excl. stage 1 borderline after 2009)
Year Lothian Fife BGH D&G SCAN 2006 89.6 100 92.9 90.9 92.3 2007 82.4 100 100 100 91.3 2008 100 100 100 100 100 2009 100 100 83.3 - 98.4 2010 100 100 100 100 100 2011 100 100 100 100 100 2012 100 100 93.8 93.8 99.4

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 20
Patients with Stage 1 Borderline (n = 19)
Lothian Fife BGH D&G SCAN Imaging n % n % n % n % n %
Performed 14 93.3 3 100.0 0 - 1 100.0 18 94.7
Not performed
1 6.7 0 - 0 - 0 - 1 5.3
Not recorded
0 0.0 0 - 0 - 0 - 0 -
Total 15 100.0 3 100.0 0 1 100.0 19 100
5. Preoperative Preparations 5.1 NHS QIS 5a1: All patients considered suitable for surgery will have appropriate pre-operative preparation. Preparation to include: Chest x-ray, DVT prophylaxis and antibiotic prophylaxis. Bowel preparation and Pre-op chest imaging are no longer current practice, so are not documented. DVT and antibiotic prophylaxis are standard practice and results are now routinely documented.

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 21
6. Surgical Treatment 6.1 NHS QIS 6a: All patients with suspected ovarian cancer to be operated on only by a designated gynaecological surgeon or referred to a gynaecological oncologist. In 2012 SCAN had 4 trained sub-specialty consultant gynaecological oncologists and 3 gynaecologists with special interest in oncology. n = 74. All patients with suspected ovarian cancer having surgery as first treatment
Surgical patients with suspected ovarian cancer Lothian Fife BGH D&G SCAN Clinician n % n % n % n % n %
Sub-specialty trained 43 100 16 76.2 3 100 4 57.1 66 89.2 Gynaecology surgeon with special interest 0 - 2 9.5 0 - 3 42.9 5 6.8
General Gynaecologist 0 3 14.3 0 0 3 4.1 Total 43 100 21 100 3 100 7 100 74 100
95.9% of suspected ovarian cancer patients in SCAN were operated on by sub-specialty consultant gynaecological oncologists or a gynaecologist with special interest in oncology. There have been specific staffing problems in Fife which have now been addressed. n = 95. All patients having surgery as first treatment (includes 21 patients where cancer was not suspected pre-op)
All surgical patients Lothian Fife BGH D&G SCAN Clinician n % n % n % n % n %
Sub-specialty trained 51 89.5 17 77.3 4 57.1 4 44.4 76 80.0 Gynaecology surgeon with special interest 0 0.0 2 9.1 0 0.0 4 44.4 6 6.3
Gynaecologist 5 8.8 3 13.6 3 42.9 1 11.1 12 12.6 General surgeon 1 1.8 0 0.0 0 0.0 0 0.0 1 1.1
Total 57 100.0 22 100.0 7 100.0 9 100.0 95 100.0
Year Lothian Fife BGH D&G SCAN 2006 96.8 82.6 58.3 100 90.0 2007 88.3 86.1 100 80.0 88.0 2008 81.8 96.9 66.7 66.7 85.0 2009 90.5 82.4 66.7 No data 85.3 2010 89.8 88.9 66.7 33.3 81.7 2011 81.1 91.7 100 72.8 82.3
% Operated on by sub-specialty trained or special interest gynaecologists in previous years
for all patients (suspected & unsuspected)
2012 89.5 86.4 57.1 88.8 86.3

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 22
6.1a SIGN 75 4.4: All patients with (FIGO) stage 3 disease should be operated on by a gynaecological oncologist rather than a general gynaecologist or general surgeon. n = 20. All patients having surgery as first treatment with FIGO stage 3 disease.
Stage I Stage II Stage III Stage IV Total Clinician n % n % n % n % n %
Dr Busby - Earle 5 10.0 5 21.7 4 20.0 0 0.0 14 14.7
Dr Farquharson 3 6.0 3 13.0 0 0.0 0 0.0 6 6.3
Dr Martin 7 14.0 1 4.3 4 20.0 0 0.0 12 12.6
Dr Walker 11 22.0 8 34.8 8 40.0 0 0.0 27 28.4
Dr Fegan 8 16.0 3 13.0 3 15.0 0 0.0 14 14.7
Sub-specialty trained
gynaecologist
Dr Ghaoui 2 4.0 0 0.0 0 0.0 0 0.0 2 2.1
Dr McCullough 3 6.0 0 0.0 1 5.0 0 0.0 4 4.2 Special interest
gynaecologist Dr Macnab 2 4.0 0 0.0 0 0.0 0 0.0 2 2.1
Dr Abdel-Ali 1 2.0 0 0.0 0 0.0 0 0.0 1 1.1 Dr Atputhasingham 0 0.0 0 0.0 0 0.0 1 50.0 1 1.1
Dr Brady 3 6.0 0 0.0 0 0.0 0 0.0 3 3.2 Dr Brooks 0 0.0 1 4.3 0 0.0 0 0.0 1 1.1 Dr Cooper 1 2.0 0 0.0 0 0.0 0 0.0 1 1.1 Dr Hadoura 1 2.0 0 0.0 0 0.0 0 0.0 1 1.1 Dr Khalifa 0 0.0 1 4.3 0 0.0 0 0.0 1 1.1
Dr Magowan 2 4.0 0 0.0 0 0.0 0 0.0 2 2.1
General gynaecologist
Dr West 1 2.0 0 0.0 0 0.0 0 0.0 1 1.1 Other specialty General surgeon 0 0.0 1 4.3 0 0.0 1 50.0 2 2.1
Totals 50 100 23 100 20 100 2 100 95 100
Total sub-specialty trained / special interest 41 82.0 20 87.0 20 100 0 0.0 81 85.3
20 patients with surgery as first treatment in SCAN were staged with FIGO IIIA , IIIB or IIIC
95% of those were operated on by a sub-specialty trained gynaecologist.
5% were operated on by a gynaecologist with special interest in oncology.
100% compliance with the SIGN guideline

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 23
6.2 Fertility Preserving Surgery NHS QIS 6b3: In young women, the possibility of germ cell tumours is considered. Fertility preserving surgery to be performed in most cases. If germ cell tumour is confirmed, patient to be referred to regional oncology centre.
Lothian
Fife
BGH D&G
SCAN Fertility
preserving surgery in
women under 30 at
diagnosis % % % % %
Performed 100 100 100 - 100
Not performed - - - - -
Total under 30 100 100 100 - 100
% Performed in previous years Year Lothian Fife BGH D&G SCAN 2006 100 100 100 n/a 100 2007 100 100 100 n/a 100 2008 100 100 n/a n/a 100 2009 100 n/a 100 No data 100 2010 100 100 n/a n/a 100 2011 100 100 n/a 100 100 2012 100 100 100 n/a 100

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 24
6.4 Surgical Incision NHS QIS 6c1: Vertical incision is made. This is to ensure a good exposure of the upper abdomen to assess the full peritoneal cavity. n =95. All patients having surgery as first treatment, excluding 8 patients with laparoscopic surgery.
Lothian Fife BGH D&G SCAN Incision
n % n % n % n %
Midline (vertical)
47 94.0 17 81.0 5 71.4 6 66.7 75 86.2
Paramedian (vertical)
0 - 3 14.3 0 0 2 22.2 5 5.7
Low transverse
3 6.0 1 4.8 2 28.5 0 0 6 6.9
Transverse muscle cutting
0 - 0 - 0 - 0 - 0 -
Not recorded 0 - 0 - 0 0 1 11.1 1 1.1
Total 50 100 21 100 7 100 9 100 87 100
80 patients had a vertical incision, 94.4 % compliance with the CSBS standard.
% Vertical incisions performed in previous years
Year Lothian Fife BGH D&G SCAN 2006 NA 91.3 83.3 44.4 NA 2007 NA 92.7 100 53.5 NA 2008 89.4 90.7 100 33.4 86.9 2009 85.6 94.1 77.8 No data 86.8 2010 88.1 83.3 66.6 88.9 85.3 2011 93.5 91.7 100 100 94.4
Lothian figures for 2006 and 2007 are not available for comparison

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 25
6.5 Washings / ascitic fluid sampling NHS QIS 6c2: Washings or ascitic fluid should be sent for cytology
n = 95. All patients with surgery as first treatment (laparotomy / laparoscopy)
Lothian
Fife
BGH D&G
SCAN Washings/
Ascites Fluid n % n % n % n % n %
Sampled 47 82.5 21 95.5 6 85.7 9 100 83 87.4
Not Sampled 10 17.5 0 0.0 1 14.3 0 - 11 11.6
Not recorded 0 0.0 1 4.5 0 0.0 0 - 1 1.1
Total 57 100 22 100 7 100 9 100 95 100
Lothian: 8 patients were not suspected cancer pre-operatively due to low RMI. 1
patient had an exenteration and 1 had fluid sampled but sent to microbiology in error.
Lothian
Fife
BGH D&G
SCAN Washings/
Ascites Result
n % n % n % n % n %
Positive 19 41.3 18 85.7 3 50 5 55.6 45 54.9
Negative 27 58.6 3 14.3 3 50 4 44.4 37 45.1
Total 46 100 21 100 6 100 9 100 82 100
% Performed in previous years
Year Lothian Fife BGH D&G SCAN 2006 91.6 84.6 92.9 63.6 87.7 2007 87.1 36.6 100 37.5 66.7 2008 92.5 87.5 100 100 91.7 2009 85.7 82.4 100 No data 86.8 2010 77.6 100 83.3 100 85.4 2011 67.6 100 100 72.7 75.8 2012 82.5 95.5 85.7 100 87.4

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 26
6.6 Primary cytoreductive surgery NHS QIS 6c3: Primary cytoreductive surgery to be attempted and to include a total or subtotal hysterectomy and bilateral salpingo-oophorectomy 6.6.1 All patients having hysterectomy
n = 95 All patients having surgery as first treatment
Lothian Fife BGH D&G SCAN
n % n % n % n % n %
No uterus present pre-operatively
4 7.0 1 4.5 0 - 1 11.1 6 6.3
Uterus present pre-operatively
53 93.0 21 95.5 7 100 8 88.9 89 93.7
Total surgical patients
57 100 22 100 7 - 9 100 95 100
Lothian Fife BGH D&G SCAN
n % n % n % n % n %
Total hysterectomy
38 71.7 15 71.4 5 71.4 5 62.5 63 70.8
Sub total hysterectomy
1 1.9 1 4.8 0
- 2 25.0 4 4.5
No hysterectomy
4 7.5 3 14.3
0
- 1 12.5 8 9.0
Fertility preserving
surgery 10 18.9 2 9.5 2 28.6 0 0 14 15.7
Total with uterus recorded as present pre-
operatively
53 100 21 100 7 100 8 100 89 100
NB: 7 Lothian patients over 30 yrs old had fertility preserving surgery
% Performed in previous years (total + sub-total hysterectomy) Year Lothian Fife BGH D&G SCAN 2006 77.8 50.0 83.3 60.0 70.1 2007 73.4 75.0 75.0 58.3 72.4 2008 79.3 79.3 100 66.7 78.9 2009 74.3 68.8 88.9 No data 75.0 2010 65.9 83.3 80.0 55.6 69.7 2011 77.1 87.5 100 66.7 77.8 2012 73.6 76.2 71.4 87.5 75.3

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 27
6.6.2 Patients having unilateral or bilateral oophorectomy
n = 95. All patients with ovaries recorded as present pre-operatively
Lothian Fife BGH D&G SCAN
n % n % n % n % n %
Unilateral 13 22.8 8 36.4 3 42.9 1 11.1 25 26.3
Bilateral 43 75.4 14 63.6 4 57.1 8 88.9 69 72.6
No oophorectomy
1 1.8 0 0.0 0 0.0 0 0.0 1 1.1
Not recorded 0 0.0 0 0.0 0 0.0 0 0.0 0 0.0
Total with ovaries recorded as present pre-op
57 100 22 100 7 100 9 100 95 100
% Performed in previous years (bilateral + unilateral) Year Lothian Fife BGH D&G SCAN 2006 93.6 73.9 100 100 91.3 2007 78.4 87.8 100 76.9 82.1 2008 87.7 90.7 100 71.4 87.8 2009 97.7 94.1 100 No data 95.6 2010 97.9 100 100 100 98.8 2011 100 100 100 100 100
6.7 Omentectomy / omental biopsy
NHS QIS 6c4: Omentectomy and/or omental biopsy performed n = 95. All surgical patients having surgery as first treatment
Lothian Fife BGH D&G SCAN
n % n % n % n % n %
Omentectomy 40 70.2 12 54.5 4 57.1 4 44.4 60 63.2
Omental biopsy 7 12.3 10 45.5 2 28.6 5 55.6 24 25.3
No omental tissue taken
10 17.5 0 0.0 1 14.3 0 0.0 11 11.6
Total surgical patients
57 100 22 100 7 100 9 100 95 100
Lothian: 8 were not suspected cancer pre-op due to low RMI % Performed in previous years (omentectomy + omental biopsy)
Year Lothian Fife BGH D&G SCAN 2006 88.9 82.6 100 50.0 87.4 2007 92.3 78.1 75.0 77.0 85.4 2008 91.0 96.9 100 71.4 91.7 2009 88.1 88.2 100 No data 89.7 2010 75.5 88.9 100 66.7 79.3 2011 78.4 91.7 100 72.7 80.6

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 28
6.8 Record of Residual disease NHS QIS 6c5: Record of residual disease to be made
n= 95. All patients having surgery as first treatment
Lothian Fife BGH D&G SCAN Residual disease
n % n % n % n % n %
Recorded 40 70.2 22 100 7 100 7 77.8 76 80.0
Not recorded 17 29.8 0 - 0 - 2 22.2 19 20.0
Total surgical patients
57 100 22 100 7 100 9 100 95 100
Lothian: 12 had stage 1 tumours. Introduction of a standardised operation note is required to address this.
% Recorded in previous years Year Lothian Fife BGH D&G SCAN 2006 96.8 95.7 66.7 100 93.2 2007 98.3 90.2 75.0 84.6 93.2 2008 95.5 96.9 100 100 96.3 2009 76.1 100 100 No data 85.2 2010 75.5 88.9 100 55.6 78.0 2011 64.9 100 100 63.6 72.6 2012 70.2 100 100 77.8 80.0
6.9 Surgical Assessment FIGO NHS QIS 6c7: Surgical pathological stage is recorded in case notes n = 117. All surgically assessed patients, includes laparoscopy, and laparotomy where treatment was not possible.
Lothian Fife BGH D&G SCAN FIGO
n % n % n % n % n %
Recorded 31 40.8 22 100 9 90 3 33.3 65 55.6
Not recorded 45 59.2 0 - 1 10 6 66.7 52 44.4
Total patients 76 100 22 100 10 100 9 100 117 100
% Recorded in previous years Year Lothian Fife BGH D&G SCAN 2006 83.9 95.7 41.7 100 82.2 2007 75.4 92.7 100 100 81.3 2008 83.3 100 100 85.7 89.0 2009 70.9 100 90.0 No data 78.7 2010 75.8 100 100 58.3 80.2 2011 58.9 100 100 18.2 61.9 2012 40.8 100 90 33.3 55.6

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 29
7. Post operative management: Pathology NHS QIS 8a3: Type, sub-type and grade of disease are recorded.
7.1 Type/Sub-Type
n = 169. All patients with histology, or cytology samples
Lothian Fife BGH D&G SCAN
n % n % n % n % n %
Recorded 103 100 36 100 14 100 16 100 169 100
Not recorded 0 - 0 - 0 - 0 - 0 -
Total 103 100 36 100 14 100 16 100 169 100
% Recorded in previous years
Year Lothian Fife BGH D&G SCAN 2006 100 95.7 100 66.7 96.5 2007 100 89.4 83.3 100 96.3 2008 100 100 100 100 98.5 2009 100 100 100 No data 100 2010 100 100 100 100 100 2011 100 100 100 100 100 2012 100 100 100 100 100
7.2 Grade of Disease
n = 178. All patients with histology / cytology samples, where grading is applicable
Lothian Fife BGH D&G SCAN
n % n % n % n % n %
Grading applicable 75 68.2 33 91.7 14 87.5 9 56.2 133 74.7
Grading inapplicable*
35 31.8 3 8.3 2 12.5 7 43.8 45 25.2
Total 110 100 36 100 16 100 16 100 178 100
*Not applicable to grade (e.g. germ cell tumours), or not possible to grade (e.g., cytology or no histology sample)
Lothian Fife BGH D&G SCAN
n % n % n % n % n %
Recorded 75 100 33 100 13 92.9 9 100 130 97.7
Not recorded 0 - 0 - 1 7.1 0 - 3 2.3
Total with histology /cytology applicable to grade
75 100 33 100 14 100 9 100 133 100
% Recorded in previous years Year Lothian Fife BGH D&G SCAN 2006 94.0 100 85.7 66.7 96.5 2007 95.6 97.9 83.3 68.8 92.7 2008 83.3 91.9 100 40.0 83.5 2009 96.5 100 100 No data 97.8 2010 100 100 100 100 100 2011 100 100 100 100 100

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 30
2012 100 100 92.9 100 97.7
7.3 Final FIGO on pathology report - Surgical patients
NHS QIS 6c8: Final surgical pathological stage is recorded
n = 117. All patients having surgical assessment, includes laparoscopy, and laparotomy where treatment was not possible.
Lothian Fife BGH D&G SCAN
n % n % n % n % n %
Recorded 76 100 22 100 10 100 9 100 117 100
Not recorded 0 - 0 - 0 - 0 - 0 -
Total surgically assessed
76 100 22 100 10 100 9 100 117 100
% Recorded in previous years
Year Lothian Fife BGH D&G SCAN 2006 96.8 95.7 91.7 81.8 96.3 2007 83.1 92.7 66.7 81.3 88.6 2008 92.5 100 100 85.7 94.5 2009 91.9 100 90.0 No data 93.3 2010 100 100 100 100 100 2011 98.2 100 100 100 98.8 2012 100 100 100 100 100
7.4 Final FIGO – All Patients n = 178. All patients (including diagnoses where FIGO is not applicable, so this is an estimate of stage)
Lothian Fife BGH D&G SCAN
n % n % n % n % n %
Recorded 105 95.5 33 91.7 10 62.5 16 100 164 92.1
Not recorded 5 4.5 3 8.3 6 37.5 0 - 14 7.9
Total 110 100 36 100 16 100 16 100 178 100
Data not recorded prior to 2010 (Not National dataset). Year Lothian Fife BGH D&G SCAN 2010 87.6 92.5 63.6 100 88.8 2011 86.7 96.4 100 94.4 89.9 2012 95.5 91.7 62.5 100 92.1

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 31
8. Chemotherapy management SIGN 75: 5.5.1A: First line chemotherapy of epithelial ovarian cancer should include a platinum agent either in combination or as a single agent, unless specifically contraindicated. n =131. All patients with epithelial ovarian cancer that received chemotherapy, excluding 22 patients with Borderline tumours, 21 patients with non-epithelial tumours or no histology, 2 patients with epithelial tumour that died before treatment and 2 that declined treatment.
Lothian Fife BGH D&G SCAN
n % n % n % n % n % Platinum
based 60 82.2 23 76.7 8 61.5 11 84.6 102 79.1
Platinum
alone 13 17.8 8 26.7 4 30.8 3 23.1 28 21.4
Platinum + taxane
47 64.4 15 50.0 4 30.8 8 61.5 74 56.5
Other Chemo
0 0.0 0 0.0 0 0.0 0 0.0 0 0
No chemo required
15 17.8 7 23.3 5 38.5 2 15.4 29 22.1
Total 73 100 30 100 13 100 13 100 131 100
100% of patients who received chemotherapy received a platinum based treatment
Reasons for no chemotherapy Lothian Fife BGH D&G SCAN
Died post surgery / biopsy 0 0 2 0 2 Early stage and low grade tumour 5 3 2 0 10 Too frail / comorbidities 8 1 0 1 10 Declined chemotherapy 2 3 1 1 7 Total 15 7 5 2 29
Reasons for no chemotherapy in SCAN in previous years
5
15
8
710
10
22
25
13
84
6
751 1
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2008 2009 2010 2011 2012
Not recorded
Declined chemotherapy
Too frail / comorbidities
Died post surgery/biopsy
Early stage tumour

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 32
9. Post Chemo surgery / Delayed primary surgery n = 178. All patients, includes patients with neoadjuvant and adjuvant chemo.
Lothian Fife BGH D&G SCAN Subsequent Surgery
n % n % n % n % n %
Delayed primary surgery
25 22.7 9 25.0 2 12.5 1 6.3 37 20.8
Post chemo surgery
0 0.0 0 0.0 1 6.3 0 0.0 1 0.6
Biopsy Only 1 0.9 0 0.0 0 0.0 1 6.3 2 1.1
Not performed*
41 37.3 15 41.7 5 31.3 10 62.5 71 39.9
Inapplicable (no chemo)
43 39.1 12 33.3 8 50.0 4 25.0 67 37.6
Total 110 100 36 100 16 100 16 100 178 100
* Includes patients with previous complete surgery, and those that were inoperable post chemotherapy.

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 33
10. Clinical Trials
CSBS Essential Criteria: Patients being offered clinical trials is recorded. Clinical trial entry is recorded. n = 178. All patients
Lothian Fife Borders D&G SCAN
Entered in trial 8 0 0 0 8
Not entered in trial 102 36 16 16 170
% Entered in trial 7.8 0 0 0 0
Total patients 110 36 16 16 178
Accrual figures for Surgical and Clinical Trials (offered and accepted) are regularly reported to the Scottish Executive by Scottish Cancer Research Network (SCRN).

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 34
11. Outcomes 11.1 Thirty Day Mortality Surgical mortality within 30 days is subject to automatic review. Following the NCEPOD report on chemotherapy 30 days mortality (2009) from chemotherapy is also now subject to close review and scrutiny. 11.1a Post Operative Deaths (30 days or less from date of primary surgery)
n = 95. All patients undergoing surgery Lothian Fife BGH D&G SCAN
n % n % n % n % n % Number of
post op deaths
0 - 0 - 0 - 0 - 0 -
Total surgical patients
57 100 22 100 7 100 9 100 95 100
% Post op deaths in previous years
Year Lothian Fife BGH D&G SCAN 2006 3.2 13 8.3 0 5.6 2007 1.5 0 0 0 0.8 2008 1.5 9.4 0 0 3.7 2009 0 0 0 No data 0 2010 0 0 0 0 0 2011 5.4 0 0 0 3.2 2012 0 0 0 0 0
Post operative deaths have decreased since the introduction of neoadjuvant chemotherapy and delayed primary surgery in 2009. 11.1b Post Chemotherapy Deaths (30 days or less from start date of chemotherapy) NB: National dataset currently only includes start date of first chemotherapy, not date of any chemotherapy e.g., second cycle.
n = 109. All patients undergoing chemotherapy Lothian Fife BGH D&G SCAN
n % n % n % n % n % Number of post chemo deaths
1 1.5 0 - 0 - 0 - 1 0.9
Total no patients
undergoing chemotherapy
66 100 24 100 8 100 11 100 109 100
Reports prior to 2008 included deaths within 60 days of 1st cycle of chemo % Post chemo deaths (30 days or less from start date of chemo)
Year Lothian Fife BGH D&G SCAN 2008 0 0 0 0 0 2009 10.2 6.25 0 0 8.6 2010 1.7 3.7 0 0 1.8 2011 0 0 0 0 0 2012 1.5 0 0 0 0.9

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 35
11.1c Post Treatment deaths (Within 30 days of first treatment date) (Treatment includes surgery, chemotherapy, no active treatment) n = 172. All patients undergoing treatment (excluding 3 patients that declined
treatment and 3 that died before treatment)
Lothian Fife BGH D&G SCAN n % n % n % n % n %
No of post treatment
deaths 5 4.7 0 - 1 6.7 0 - 6 3.5
Total no patients that
received treatment
107 100 35 100 15 100 15 100 172 100
% Post Treatment deaths in previous years (30 days or less from date of first treatment, or decision not to treat)
Year Lothian Fife BGH D&G SCAN 2006 6.7 23.1 7.1 0 9.7 2007 8.3 5.9 0 0 6.1 2008 4.9 15.0 33.3 0 9.3 2009 7.0 7.1 8.3 No data 7.5 2010 11.8 2.6 10.0 4.3 8.6 2011 12.6 3.8 0 5.6 9.7 2012 4.7 0 6.7 0 3.5

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 36
11.2 Residual Disease Survival in ovarian cancer is directly related to residual disease i.e. the amount of cancer left behind at the end of surgery. The less disease (under 1cm) the more likely 5 year survival without relapse. This is an indicator of the quality of surgery, but also dependent upon the amount of disease at the start of the operation. n = 95. All patients undergoing surgery as first treatment
Lothian Fife BGH D&G SCAN n % n % n % n % n %
No residual disease 32 56.1 18 81.8 6 85.7 5 55.6 61 64.2
< 1 cm 4 7.0 1 4.5 0 0.0 0 0.0 5 5.3
1 - 5 cm 2 3.5 3 13.6 1 14.3 1 11.1 7 7.4
> 5 cm 2 3.5 0 0.0 0 0.0 1 11.1 3 3.2
Residual disease size not recorded 17 29.8 0 0.0 0 0.0 2 22.2 19 20.0 Total surgical
patients 57 100 22 100 7 100 9 100 95 100
% No residual disease or <1cm in previous years.
Year Lothian Fife BGH D&G SCAN 2006 43.5 39.1 91.7 66.7 49.5 2007 20.0 56.7 75.0 70.0 37.5 2008 51.5 46.9 66.7 66.7 51.4 2009 59.5 58.8 88.9 No data 63.2 2010 61.2 66.7 100 55.6 64.6 2011 56.7 75.0 100 54.5 61.3 2012 63.1 86.0 85.7 55.6 69.5

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 37
Since 2009 practice has changed towards patients receiving neoadjuvant chemotherapy followed by delayed primary surgery (see page 5 for details). Residual disease after delayed primary surgery is shown below. n = 38. All patients undergoing delayed primary surgery (DPS)
Lothian Fife BGH D&G SCAN n % n % n % n % n %
No residual disease 13 52.0 4 44.4 2 66.7 1 100 20 52.6
< 1 cm 6 24.0 0 0.0 0 0.0 0 0.0 6 15.8
1 - 5 cm 5 20.0 3 33.3 0 0.0 0 0.0 8 21.1
> 5 cm 0 0.0 2 22.2 0 0.0 0 0.0 2 5.3
Residual disease size not recorded 1 4.0 0 0.0 1 33.3 0 0.0 2 5.3 Total surgical
patients 25 100 9 100 3 100 1* 100 38 100 * D&G 1 patient was inoperable at delayed primary surgery and is not included in this table. For SCAN no residual or <1cm disease is 68.4% % No residual disease or <1cm in previous years for DPS patients (data only available since 2010.
Year Lothian Fife BGH D&G SCAN 2010 57.9 40.0 100.0 63.6 56.1 2011 72.0 83.3 100.0 40.0 71.1 2012 76.0 44.4 66.7 100 68.4

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 - 38 -
11.3 Survival: NHS QIS 4a2: 1, 2, and 5-year survival rates are audited. Regular reporting of case mix and outcome. Survival figures are given below. They will vary from year to year given the small number of patients and the case mix (stage of disease at presentation). Cause of death is taken from the GRO data (death certificate). Over 93% of these are due to advanced ovarian cancer rather than other disease
Patients diagnosed 2006 – 2011. Patients with no known death date checked against dates last seen alive. D&G data is not available for 2006 – 2009. Exclusions: Patients with Borderline tumours, patients that declined treatment and patients that died before treatment.
SCAN Percentage survival Stage 1-2 1yr 2yr 3yr 4yr 5yr 2006 92.9 82.1 67.9 64.3 64.3 2007 94.6 89.2 83.8 75.7 67.6 2008 89.3 85.7 85.7 82.1 2009 100.0 100.0 90.3 2010 92.3 79.5 2011 100.0
SCAN Percentage survival Stage 3-4
1yr 2yr 3yr 4yr 5yr 2006 72.5 51.0 35.3 23.5 15.7 2007 69.6 50.0 26.8 19.6 2008 61.9 46.0 30.2 2009 67.4 44.2 2010 62.5 2011 85.1
SCAN Percentage survival No stage
1yr 2yr 3yr 4yr 5yr 2006 42.9 14.3 7.1 0 - 2007 52.6 42.1 10.5 10.5 2008 36.8 5.3 5.3 2009 31.0 10.3 2010 22.7 2011 90.5

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 - 39 -
12. Multidisciplinary Meeting NHS QIS 3a4: All patients confirmed to have ovarian cancer after surgery are discussed at the MDT meeting and follow up treatment organised.
Lothian Fife BGH D&G SCAN n % n % n % n % n %
Discussed at MDM 108 98.2 36 100 15 93.8 16 100 175 98.3
Not discussed at MDM 2 1.8 0 0.0 1 6.3 0 0.0 3 1.7
Not recorded 0 0.0 0 0.0 0 0.0 0 0.0 0 0.0
Total 110 100 36 100 16 1 16 100 178 100

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 - 40 -
13. Quality Performance Indicators (QPI) Quality Performance Indicators (QPI) for Ovarian cancer have been developed and published in 2013. Data collection with the new QPI dataset for these QPIs commences on 1/10/2013. There are 5 QPIs that are possible to measure with the existing national dataset and these are listed below. It must be noted that these are a close approximation for these measures and that the full QPI dataset will be reported in 2015 with the first full year of data.
QPI 4 Epithelial Ovarian cancers only Patients undergoing surgery for early stage epithelial ovarian cancer (FIGO Stage 1) have an adequate staging operation which includes Total Abdominal Hysterectomy (TAH), Bilateral Salpingo-Oophorectomy (BSO), omentectomy and washings. QPI target = 95% Lothian Fife Borders D&G SCAN
N1 Number of early stage (FIGO Stage 1) epithelial ovarian cancer patients having primary surgery involving TAH, BSO, omentectomy and washings.
6 7 2 3 18
D1 All early stage (FIGO Stage 1) epithelial ovarian cancer patients undergoing primary surgery.
7 9 3 3 24
N2 Number of early stage (FIGO Stage 1) epithelial ovarian cancer patients having
primary surgery involving TAH, BSO, omentectomy and washings operated on by a gynaecological oncologist.
6 5 2 3* 16
D2 All early stage (FIGO Stage 1) epithelial ovarian cancer patients operated on by a
gynaecological oncologist. .
6 7 2 3* 18
Exclusions: Emergency presentations or fertility sparing 2 4 2 0 8
QPI4 i) % achievement 85.7 77.8 33.3 100.0 75.0
QPI4 ii) %achievement 100.0 71.4 100.0 100.0 88.9
* Current QPI definitions don’t indicate if special interest is included. SCAN needs to agree which clinicians are designated for this measure.

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 -41 -
QPI 5 Epithelial Ovarian cancers only. Surgery, as first definitive treatment, for patients with advanced epithelial ovarian cancer (FIGO Stage 2 or higher) should achieve no macroscopic residual disease. QPI target 1 = 30%, QPI target 2 = 60% Lothian Fife Borders D&G SCAN
N1 Number of patients with advanced epithelial ovarian cancer (FIGO Stage 2 or higher) with no macroscopic residual disease following surgery. 13 5 3 2 23
N2 Number of patients with advanced epithelial ovarian cancer (FIGO Stage 2 or higher) undergoing surgery with macroscopic residual disease < 1cm. 16 5 3 2 26
D All patients with advanced epithelial ovarian cancer (FIGO Stage 2 or higher) undergoing surgery. 21 7 4 5 37
Residual disease not recorded (Exclusion for denominator) 3 0 1 1 5
QPI5 i) % achievement 72.2 71.4 100 50.0 72.7
QPI5 ii) %achievement 88.9 71.4 100 50.0 63.6

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 -42 -
QPI 7 Epithelial Ovarian cancers only. Patients with epithelial ovarian cancer should have a histo/cytological diagnosis of their cancer prior to starting neo-adjuvant chemotherapy. QPI target = 80% Lothian Fife Borders D&G SCAN
N Number of patients who have a diagnosis of epithelial ovarian cancer confirmed by histology prior to starting chemotherapy. 21 10 3 1 35
D All patients with epithelial ovarian cancer having neo-adjuvant chemotherapy 26 10 3 1 40
QPI7 i) % achievement 80.8 100 100 100 87.5
QPI 8 Epithelial Ovarian cancers only. Delayed primary surgery, after neo-adjuvant chemotherapy for advanced epithelial ovarian cancer (FIGO Stage 3c or 4), should achieve optimal cytoreduction (<1cm). QPI target = 65% Lothian Fife Borders D&G* SCAN
N1 Number of patients with advanced epithelial ovarian cancer (FIGO Stage 3c or 4) undergoing
delayed primary surgery after neo-adjuvant chemotherapy.
24 9 3 2† 38
N2 Number of patients with advanced epithelial ovarian cancer (FIGO Stage 3c or 4) undergoing
delayed primary surgery with residual disease <1cm.
19 3 2 1 25
D1 All patients with advanced epithelial ovarian cancer (FIGO Stage 3c or 4) having neo-adjuvant
chemotherapy.
36 10 3 5 54
D2 All patients with advanced epithelial ovarian cancer (FIGO Stage 3c or 4) undergoing delayed
primary surgery after neo-adjuvant chemotherapy.
24 9 3 2 38
QPI8 i) % achievement 66.7 90.0 100.0 40.0 70.4
QPI8 ii) % achievement 79.2 33.3 66.7 50.0 65.8 *Patients diagnosed in Dumfries and Galloway undergo delayed primary surgery in Lothian † Includes one patient with inoperable disease at delayed primary surgery.

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 -43 -
QPI 9 Epithelial Ovarian cancers only Chemotherapy treatment of epithelial ovarian cancer should include a platinum agent. Exclusions: Patients with low-grade serous disease; patients with FIGO stage 1a or 1b, low grade (G1) disease; patients with Stage 1a clear cell tumour; patients who decline chemotherapy treatment. QPI target = 90%
Lothian Fife Borders D&G SCAN
N Number of epithelial ovarian cancer patients who receive chemotherapy involving either Paclitaxel in combination with a platinum-based compound or carboplatin only 51 20 8 10 89
D All epithelial ovarian cancer patients 60 20 12 10 102
QPI9 % achievement 85 100 66.7 100 87.3
Lothian: 9 patients with no platinum based chemo; 8 were too frail 1 had an unusual tumour type (Brenner tumour) Borders: 4 patients were too frail

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 - 44 -
Appendix 1 Summary of Results All Patients Lothian Fife BGH D&G SCAN
Tested 105 35 14 15 169 Not Tested 5 1 2 1 9
Not Recorded 0 0 0 0 0 CA 125
Total 110 36 16 16 178
Surgery 63 21 8 5 97 Percutaneous Biopsy 25 13 5 7 50
Presumptive* 22 2 3 4 31 Mode of Diagnosis
Total 110 36 16 16 178 *Includes cytological and imaging only diagnoses
Laparotomy 53 21 8 9 91 Laparoscopy 23 1 2 0 26 No operation 34 14 6 7 61
Patient Declined 0 0 0 0 0
Surgical assessment
Total 110 36 16 16 178
Surgery 57 22 7 9 95 Chemotherapy 38 11 4 5 58
Patient Declined 1 1 0 1 3 No Treatment 10 0 4 1 15
Hormone therapy 2 2 0 0 4 Died before Tx 2 0 1 0 3
First Treatment
Total 0 0 0 0 0
Chemotherapy 66 24 8 11 109 No Chemotherapy 44 12 8 5 69 Chemotherapy
Total 110 36 16 16 178
Delayed primary surgery 25 9 2 1 37 Post chemo surgery 0 0 1 0 1
Biopsy Only 1 0 0 1 2 Not performed 41 15 5 10 71
Inapplicable (no chemo) 43 12 8 4 67
Subsequent Surgery (post chemo)
Total 110 36 16 16 178
Discussed at MDM 108 36 15 16 175 Not discussed at MDM 2 0 1 0 3
Not recorded 0 0 0 0 0 MDM Discussion
Total 110 36 16 16 178
Yes 42 21 3 7 73 No 15 1 4 2 22
Not recorded 0 0 0 0 0
Cancer suspected pre-operatively
Total 57 22 7 9 88

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 -45 -
All Patients Excluding Borderline Stage 1 Lothian Fife BGH D&G SCAN
Performed 95 33 15 15 158 Not Performed 0 0 1 0 1 Not Recorded 0 0 0 0 0
Imaging
Total 95 33 16 15 159 All Borderline Stage 1 Patients
Performed 14 3 0 1 18 Not Performed 1 0 0 0 1 Not Recorded 0 0 0 0 0
Imaging
Total 15 3 0 1 19 Patients with surgery as first treatment Lothian Fife BGH D&G SCAN
Elective 51 18 7 8 84 Emergency 6 4 0 1 11
Not Recorded 0 0 0 0 0 Type of List
Total surgical patients 57 22 7 9 95
Midline 47 17 5 6 75 Paramedian 0 3 0 2 5
Low Transverse 3 1 2 0 6 Transverse Muscle Cutting 0 0 0 0 0
Laparoscopy only 7 1 0 0 8 Not Recorded 0 0 0 1 1
Incision
Total surgical patients 57 22 7 9 95
Omentectomy 40 12 4 4 60 Omental Biopsy 7 10 2 5 24 Not Performed 10 0 1 0 11
Not recorded 57 22 7 9 95 Omentectomy
Total surgical patients 40 12 4 4 60
Both ovaries present 52 22 6 8 88 One ovary present 4 0 1 1 6 No ovaries pre-op 1 0 0 0 1
Not recorded 0 0 0 0 0
Pre-Op ovary status
Total surgical patients 57 22 7 9 95
Unilateral 13 8 3 1 25 Bilateral 43 14 4 8 69
Not Performed 1 0 0 0 1 Biopsy only 0 0 0 0 0
No ovaries pre-op 0 0 0 0 0 Not recorded 57 22 7 9 95
Oophorectomy
Total surgical patients 13 8 3 1 25

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 -46 -
Patients with surgery as first treatment Lothian Fife BGH D&G SCAN
Total hysterectomy 38 15 5 5 63 Subtotal hysterectomy 1 1 0 2 4
No hysterectomy (>30yrs) 3 3 0 1 7 No hysterectomy, fertility
preserving 11 2 2 0 15
No uterus present pre-op 4 1 0 1 6
Hysterectomy
Total surgical patients 57 22 7 9 95
None 32 18 6 5 61 <1 cm 4 1 0 0 5
1-5 cm 2 3 1 1 7 >5 cm 2 0 0 1 3
Not recorded 17 0 0 2 19
Residual disease
Total surgical patients 57 22 7 9 95
Positive for cancer 19 18 3 5 45 Negative for cancer 27 3 3 4 37
Not sent 11 0 1 0 12 Not recorded 0 1 0 0 1
Fluid sampled
Total surgical patients 57 22 7 9 95 All patients with tissue sampled Lothian Fife BGH D&G SCAN
Borderline 18 3 0 1 22 Serous 48 17 9 8 82 Mucinous 3 4 2 0 9 Endometrioid 9 5 1 2 17 Clear Cell 3 5 1 2 11 Epithelial cancer – Undifferentiated 1 0 0 0 1 Epithelial cancer – Mixed 5 0 1 1 7 Epithelial cancer – Unspecified 6 0 0 1 7 Epithelial - Brenner 1 0 0 0 1 Sex cord – Granulosa 1 1 0 0 2 Sex cord – Stromal tumour 0 0 0 0 0 Germ Cell (Dysgerminoma) 1 0 0 0 1 Germ Cell (Teratoma) 4 0 0 0 4 Germ Cell (mixed) 0 0 0 0 0 Struma ovarii (germ cell) 0 0 0 0 0 Mixed mullerian 2 1 0 1 4 Sertoli leydig sex cord 0 0 0 0 0 Other (inc Mixed Mesodermal) 1 0 0 0 1 No Histological Sample 7 0 2 0 9 Not recorded 0 0 0 0 0
Histo-pathological type
Total 110 36 16 16 178
Well Differentiated 16 6 3 1 26 Moderately Differentiated 2 1 1 0 4 Poorly Differentiated 39 23 9 7 78 Borderline 18 3 0 1 22 Not recorded 0 0 1 0 1 Inapplicable* 35 3 2 7 48
Differentiation
Total 110 36 16 16 178

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 -47 -
All surgically assessed patients Lothian Fife BGH D&G SCAN
IA 5 6 3 0 14 IB 0 1 0 0 1 IC 4 7 1 0 12 IIA 1 1 0 0 2 IIB 0 1 0 0 1 IIC 13 3 0 1 17 IIIA 0 0 0 0 0 IIIB 2 1 2 0 5 IIIC 4 1 2 2 9
IV 0 1 1 0 2 Not recorded 28 0 1 6 35
Surgical pathological FIGO Stage
Total 57 22 10 9 98 All surgically assessed patients
IA 13 6 1 2 22 IB 0 1 0 1 2 IC 15 7 4 1 27 IIA 1 1 0 0 2 IIB 1 1 0 0 2 IIC 14 3 0 1 18 IIIA 2 0 0 1 3 IIIB 4 1 2 0 7 IIIC 7 1 2 3 13
IV 0 1 1 0 2 Not Recorded 0 0 0 0 0
Final FIGO stage (all surgically assessed patients)
Total 57 22 10 9 98 All patients
IA 13 6 1 2 22 IB 0 1 0 1 2 IC 15 6 4 1 26 IIA 1 2 0 0 3 IIB 1 1 0 0 2 IIC 15 3 0 1 19 IIIA 2 0 0 1 3 IIIB 5 1 2 0 8 IIIC 31 8 3 7 49
IV 22 7 0 3 32 Not Recorded 5 1 6 0 12
Final FIGO Stage † (all patients)
Total 110 36 16 16 178
†Technically FIGO is only calculated for patients that have been surgically assessed. Some of these patients have been assigned FIGO stages in the absence of surgical data through clinical and radiological assessment.

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 -48 -
Delayed Primary Surgery Data n = 38 Lothian Fife BGH D&G* SCAN
Elective 25 9 3 1 38 Emergency 0 0 0 0 0
Not Recorded 0 0 0 0 0 Type of List
Total surgical patients 25 9 3 1 38
Midline 25 9 3 1 38 Paramedian 0 0 0 0 0
Low Transverse 0 0 0 0 0 Transverse Muscle Cutting 0 0 0 0 0
Laparoscopy only 0 0 0 0 0 Not Recorded 0 0 0 0 0
Incision
Total surgical patients 25 9 3 1 38
Omentectomy 25 7 2 1 35 Omental Biopsy 0 1 0 0 1 Not Performed 0 1 1 0 2
Not recorded 0 0 0 0 0 Omentectomy
Total surgical patients 25 9 3 1 38
Both ovaries present 23 9 2 1 35 One ovary present 1 0 1 0 2 No ovaries pre-op 1 0 0 0 1
Not recorded 0 0 0 0 0
Pre-Op ovary status
Total surgical patients 25 9 3 1 38
Unilateral 1 0 1 0 2 Bilateral 23 6 2 1 32
Not Performed 0 3 0 0 3 Biopsy only 0 0 0 0 0
No ovaries pre-op 1 0 0 0 1 Not recorded 0 0 0 0 0
Oophorectomy
Total surgical patients 25 9 3 1 38
Total hysterectomy 18 6 1 1 26 Subtotal hysterectomy 4 1 0 0 5
No hysterectomy (>30yrs) 1 2 0 0 3 No uterus present pre-op 2 0 2 0 4
Hysterectomy
Total surgical patients 25 9 3 1 38
None 13 4 2 1 20 <1 cm 6 0 0 0 6
1-5 cm 5 3 0 0 8 >5 cm 0 2 0 0 2
Not recorded 1 0 1 0 2
Residual disease
Total surgical patients 25 9 3 1 38
Positive for cancer 6 4 1 0 11 Negative for cancer 4 4 1 0 9
Not sent 15 1 1 1 18 Not recorded 0 0 0 0 0
Fluid sampled
Total surgical patients 25 9 3 1 38
D&G patients were operated on in Lothian

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 49
Ovarian Cancer Glossary of Terms Adenocarcinoma A malignant growth of glandular tissue, adenocarcinoma can develop in any gynaecological organ. Adjuvant treatment Treatment used in addition to main treatment, usually chemotherapy given after surgery. Adnexal mass Mass of tissue on or in a structure associated with the uterus such as an ovary, fallopian tube, or uterine ligament. ARDS Acute Respiratory Distress Syndrome Ascites An accumulation of fluid in the abdominal (peritoneal) cavity. Audit A method by which those involved in providing services assess the quality of care. Results of a process or intervention are assessed, compared with a pre-existing standard, changed where necessary, then reassessed. BACiL Better Acute Care in Lothian Bevacizumab A drug that slows the growth of new blood vessels Biopsy Removal of a sample of tissue or cells from the body to assist in diagnosis of a disease. Borderline Tumour Tumours of low malignant potential based on the microscopic appearance of the cancer. They are expected to behave as very low grade cancers, i.e., to be very slow growing Carcinoma A cancerous growth. CA125 A substance which may be found in the blood of women who have ovarian cancer, used as a biochemical marker for the disease. Chemotherapy The use of drugs that kill cancer cells, or prevent or slow their growth. Cytology The study of the appearance of individual cells under a microscope. Cytotoxic Toxic to cells. This term is used to describe drugs which kill cancer cells or slow their growth.3 Debulking Removal by surgery of a substantial proportion of cancer tissue. Optimal debulking refers to the removal of the largest possible amount of cancer while limiting damage to normal tissue Delayed primary surgery (DPS) Previously referred (to in this report) as interval debulking, refers to surgical removal of tumour after chemotherapy aimed at further reducing its bulk. Differentiation The degree of morphological resemblance between cancer tissue and the tissue from which the cancer developed. Exenterative surgery Removal of the pelvic organs including the uterus, ovaries and associated organs and the bladder and/or large bowel.
SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 50
FIGO International Federation of Gynaecology and Obstetrics. FIGO defines staging in gynaecological cancer and collates information about treatment and survival from a group of collaborating European centres (including some in the UK). Gynaecology The branch of medicine which deals with the female reproductive organs. Histological grade Degree of malignancy of a tumour, usually judged from its histological features. Histological type The type of tissue found in a tumour. Histology Examination of the microscopic structure of tissue. Hysterectomy Surgical removal of the uterus. Lymph nodes Small organs which act as filters in the lymphatic system. Lymph nodes close to the primary tumour are often the first sites to which cancer spreads. Lymphadenectomy Surgical removal of lymph nodes. Lymphadenopathy Disease of the lymph nodes. Magnetic resonance imaging (MRI) A non-invasive method of imaging which allows the form and metabolism of tissues and organs to be visualised. Medical Oncologist A doctor who specialises in the treatment of cancer through the use of chemotherapy. Metastases Spread of cancer away from the primary site. mEOC A trial looking at chemotherapy with or without bevacizumab for mucinous ovarian cancer Multidisciplinary Team (MDT) A multiprofessional group of people consisting of several specialties and disciplines who work together to provide care for patients with a particular condition NCEPOD National Confidential Enquiry into Patient Outcome and Death Neo-adjuvant treatment Treatment given before the main treatment; usually chemotherapy given before surgery. Nodes See Lymph nodes. Non-neoplastic Tissue that does not contain tumour. Omentectomy Surgical removal of the omentum, a large fold of visceral peritoneum. Oncologist A doctor who specialises in treating cancer. Oncology The study of the biology and physical and chemical features of cancers. Also the study of the causes and treatment of cancers. Oophorectomy Removal of the ovaries. Palliative Anything which serves to alleviate symptoms due to the underlying cancer but is not expected to cure it. Hence palliative care, palliative chemotherapy. Peritoneal washings Fluid taken from the abdominal (peritoneal) cavity during surgery.

SCAN Comparative Ovarian Cancer Report 2012 SA Ov02 14 51
PETROC A trial comparing different combinations of chemotherapy after surgery for women with ovarian cancer who have already had chemotherapy before surgery Primary Peritoneal Cancer A tumour which shows similar morphological characteristics to ovarian cancer but which has no or minimal ovarian involvement Prophylaxis An intervention used to prevent an unwanted outcome. Protocol A policy or strategy which defines appropriate action. Resection The surgical removal of all or part of an organ. Risk of Malignancy Index (RMI) A measure of the risk of a harmful tumour, based on combining the results of transvaginal ultrasound examination, menopausal status and blood levels of the ovarian cancer marker CA125 (measured in U/ml) Staging The allocation of categories (stage I to IV) to tumours defined by internationally agreed criteria. Stage I tumours are localised, whilst stages II to IV refer to increasing degrees of spread through the body from the primary site. Tumour stage is an important determinant of treatment and prognosis. Surgical stages of ovarian cancer Stage I Limited to the ovaries IA One ovary involved IB Both ovaries involved IC One or both ovaries involved, but with cancer on the surface of an ovary, rupture of an ovarian cyst malignant ascites or positive abdominal washings Stage II Spread to adjacent pelvic structures IIA Spread to uterus or fallopian tubes IIB Spread to pelvic peritoneum IIC Confined to the pelvis, but with malignant ascites or positive abdominal washings Stage III Spread to the upper abdomen IIIA Microscopic spread to the upper abdomen IIIB Cancer nodules less than 2 cm in the abdomen IIIC Nodules more than 2 cm, or positive pelvic or aortic lymph nodes Stage IV Distant spread beyond the abdomen, liver, lung etc Total abdominal hysterectomy and bilateral salpingo -oophorectomy (TAH/BS0) Removal of the uterus with both fallopian tubes and ovaries through an incision in the abdomen. Ultrasound High-frequency sound waves used to create images of structures and organs within the body.