Embed Size (px)
Citation preview

1
Andrew Dunn, MD, MPHProfessor of Medicine
Chief, Division of Hospital MedicineMount Sinai Health System, NY
Outpatient Management of PE
Case-based Discussion of Essential Issues in
Anticoagulant ManagementMarch 8, 2016
DISCLOSURES
Pfizer / BMS Pharmaceuticals – Grant funding

2
PROGRESS!
CASE - PE
A 62 year old man presents to the ED with severe SOB for 6 hours. There is associated right-sided pleuritic chest pain and cough. There is no hemoptysis or dizziness. The patient has a history of htn, DM, and systolic CHF (EF 38%).
Exam is significant for appearing mildly uncomfortable, HR 102, RR 18, BP 148/84. O2 sat (RA) 93%. Chest exam reveals crackles at the right base. The heart exam is normal. There is no edema of either leg.

3
CASE - PE
Labs are significant for WBC 10.1, Hb 13.8. Renal function is normal.
A CTA reveals a PE in a right segmental artery.
The patient lives with his wife. He has Medicare health insurance and has the means to pay for the co-pay for his medications.
CASE - PE
What management strategy would you choose?
A. Admission, start treatment with LMWH + warfarin; discharge after ≥5 days overlap and INR therapeutic
B. Admission, start treatment with DOAC; discharge after ≥5 days
C. Admission, start treatment with DOAC; discharge if status improves in 1-2 days
D. Discharge home from ED on LMWH + warfarin
E. Discharge home from ED on DOAC

4
DOACs vs NOACs
RivaroxabanPE TREATMENT - EINSTEIN
Rivaroxaban 15mg twice daily x 3 weeks then 20mg daily compared with LMWH/warfarin
Open label, noninferiority trial
N = 4,832
EINSTEIN PE Investigators. N Engl J Med .2012;366:1287-97.

5
EINSTEIN PE Investigators. N Engl J Med .2012;366:1287-97.
RECURRENT VTE:2.1% vs 1.8%, p=NS
MAJOR BLEEDING:2.2% vs 1.1%, p=0.003
ApixabanVTE TREATMENT - AMPLIFY
Agnelli G, et al. NEJM. 2013;369:1799-808.
Apixaban 10mg bid x 7 days followed by 5mg BID x 6 months compared with SC LMWH / warfarin
5,244 total patients; 1,836 with PE
Primary endpoint:Recurrent sx VTE or VTE related death

6
AMPLIFYRESULTS
DOACs for the Treatment of VTE
Van der Hulle, et al. J Thromb Haem. 2014;12:320-8.
Meta-analysis comparing DTIs with VKA
Lumpers: DTI (dabigatran) and anti-Xa agents (rivaroxaban, apixaban, edoxaban)
Included: 5 studies (24,455 participants)

7
Van der Hulle, et al. J Thromb Haem. 2014;12:320-8.
EFFICACY OUTCOMES
SAFETY OUTCOMES
Castellucci LA. JAMA. 2014;312(11):1122-1135.
Evidence Network for Recurrent Venous Thromboembolism and Major BleedingThe width of the lines for each connection in the evidence network is proportional to the number of randomized controlled trials comparing each pair of treatments. The size of each treatment node is proportional to the patient-years of follow-up. LMWH indicates low-molecular-weight heparin; RCT, randomized clinical trial; UFH, unfractionated heparin.
Figure Legend:

8
Figure Legend:
For VTE and no cancer, as long-term anticoagulant therapy, we suggest dabigatran (Grade 2B), rivaroxaban (Grade 2B), apixaban (Grade 2B) or edoxaban (Grade 2B) over VKA therapy, and suggest VKA therapy over LMWH (Grade 2C).
AT10 - GuidelineVTE Treatment
Kearon C, et al. CHEST Guideline, Chest. 2016.

9
Outpatient PE Treatment
Aujesky D. Lancet. 2011;378:41-8.
Acute PE with low-risk PESI score
Randomized to home vs hospital-based acute care
Received LMWH plus VKA
Primary outcome: Recurrence at 90 days
RCT - 19 hospitals in Europe and US, N = 344
Aujesky D. Lancet. 2011;378:41-8.
Age +1 per yearMale sex +10Cancer +30CHF +10Chronic lung disease +10Pulse ≥110 +20SBP<100 +30RR ≥30 +20Temperature <36°C +20Altered mental status +60O2 saturation <90% +20
Pulmonary Embolism Severity Index
SCORE<66 I66–85 II86–105 III106–125 IV>125 V

10
Fang MC, et al. JAMA Intern Med. 2015;175:1060-2.
Collaboration of 4 integrated health care delivery systems
5927 patients with acute PE presenting to ED
Anticoagulants - warfarin, LMWH, fondaparinux
PESI Class III or higher: 23%
Outpatient PE TreatmentCardiovascular Research Network Venous
Thromboembolism Study

11
Discharge from ED was uncommon - 8.3%
Discharge from ED increased from 2004 to 2011 (5.6% to 11.1% ).
Most patients did well: Return to ED 18.6% Hospitalized 7.9% Mortality (7 days) 0% Mortality (90 days) 0.4%
Fang MC, et al. JAMA Intern Med. 2015;175:1060-2.
Outpatient PE Treatment - Outcomes
Suitable for outpatient treatment:
1. No contraindications (recent bleeding, severe renal/liver disease, or severe thrombocytopenia)
2. Expected to be compliant with treatment
3. Feels well enough to be treated at home
AT10 - Outpatient PE Treatment
Clinical prediction rules such as PESI (<85 or simplified score 0) can identify low-risk patients
A predefined CPR score is not required Echo and biomarkers not routinely recommended If noted, RV dysfunction or increased biomarker levels should
discourage home treatment
Kearon C, et al. CHEST Guideline, Chest. 2016.

12
Hakemi EU, et al. Chest. 2015;147(3):685-694.
Troponins and PE Prognosis:The Power of the Negative Test
Retrospective study – 298 patients with PE Primary outcomes: Death, CPR, or Thrombolysis Highly sensitive Troponin I used
161 (55%) trop positive 137 (45%) trop negative
Primary Outcome: 0/137 (0%) vs 15/161 (9%), p<0.001
Cho JH, et al. BMC Cardiovascular Disorders. 2014;14:64.
Echocardiogram and PE Prognosis
Meta-analysis - RV dysfunction as a prognostic factor in stable patients with PE
12 trials, 3283 hemodynamically stable patients with acute PE 1223 patients (37.3%) RVD+ 2060 patients (62.7%) RVD-
167/1223 (13.7%)
134/2060 (6.5%)
MORTALITY
13
The Other 50%
Insurance status - DOAC coverage, pre-authorization
Ability to afford co-pay
History of compliance issues
Domiciled
Willing and able - Understand the gravity
Follow-up arranged
Ensure social / logistical issues are fully addressed!
Take Home Points
Use the PESI score to help identify patients who can be treated safely at home - Treat the patient, not the score.
F-Xa inhibitors are as efficacious and safer than LMWH/warfarin.
Troponin and echo are useful tools to help further guide risk stratification when prognosis is uncertain.
Give equal consideration to the other 50%! Ensure all social and logistical aspects are arranged.

14
Direct Oral Anticoagulant (DOAC) Related Bleeding
Case-based Discussion of Essential Issues in
Anticoagulant Management
Hospital Medicine 2016
San Diego
8 March 2016
Scott Kaatz, DO, MSc, FACP, SFHM
Chief Medical Officer
Hurley Medical Center
Associate Professor of Medicine
Michigan State University

15
• Speaker honorarium– Janssen– Boehringer-Ingelheim– Bristol Myer Squibb/Pfizer– CSL Behring– Daiichi Sankyo
• Consultant– Boehringer Ingelheim– Bristol Myer Squibb/Pfizer– Janssen– Daiichi Sankyo– Portola
• Board membership (non-profit)– Thrombosis and Hemostasis Societies of North America– AC Forum– National Certification Board of Anticoagulation Providers– National Blood Clot Alliance Medical and Scientific
Advisory Board
Full Disclosure
Case
• 74 yo admitted with GI bleed and melena
• AF, CHA2DS2-VASc = 6
• On rivaroxaban (Xarleto), CrCL = 40 ml/min
• Hemoglobin drops 6 hours after admission with mild hypotension
• What would you do in addition to usual support?A. Wait for rivaroxaban to wane, half-life relatively short
B. Give FFP
C. Give PCC
D. Turf to hematology

16
Reversal of DOACs
Camm AJ. Eur Heart J. 2013 Sep;34(36):2850-1. PMID: 23903774.
Anti-Xa Reversal
• PCC human studies
– Only in healthy volunteers
– Improve lab test or punch bx bleeding
• No approved specific reversal agent
– Andexanet in late phase development
Siegal DM. J Thromb Thrombolysis. 2015 Apr;39(3):395-402. PMID: 25586208
17
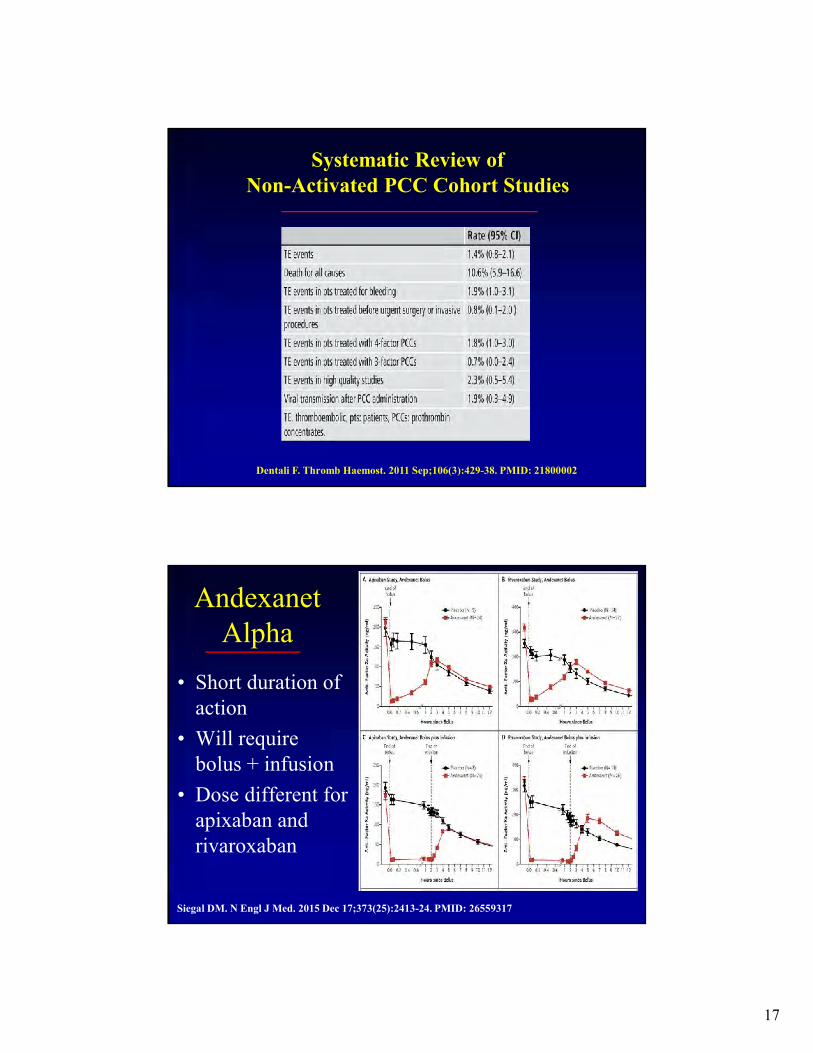
Systematic Review of Non-Activated PCC Cohort Studies
Dentali F. Thromb Haemost. 2011 Sep;106(3):429-38. PMID: 21800002
Andexanet Alpha
• Short duration of action
• Will require bolus + infusion
• Dose different for apixaban and rivaroxaban
Siegal DM. N Engl J Med. 2015 Dec 17;373(25):2413-24. PMID: 26559317

18
Case
• 74 yo admitted with GI bleed and melena
• AF, CHA2DS2-VASc = 6
• On dabigatran (Pradaxa), CrCL = 40 ml/min
• Hemoglobin drops 6 hours after admission with mild hypotension
• What would you do in addition to usual support?A. Wait for dabigatran to wane, half-life relatively short
B. Give FFP
C. Give PCC
D. Give idarucizumab (Praxbind)
E. Turf to hematology
RE-VERSE AD Study• Question: Can idarucizumab reverse
dabigatran?• Design: cohort study• Patients: 90 who received dabigatran
who needed reversal– 51 with bleeding– 39 with need for invasive
procedure/surgery
• Intervention: Two 50 ml boluses of 2.5 gm dabigatran within 15 min
• Outcome: maximum percentage of reversal of dilute thrombin time and ecarin clotting time at 4 hours
Pollack CV Jr. N Engl J Med. 2015 Aug 6;373(6):511-20. PMID: 26095746
19
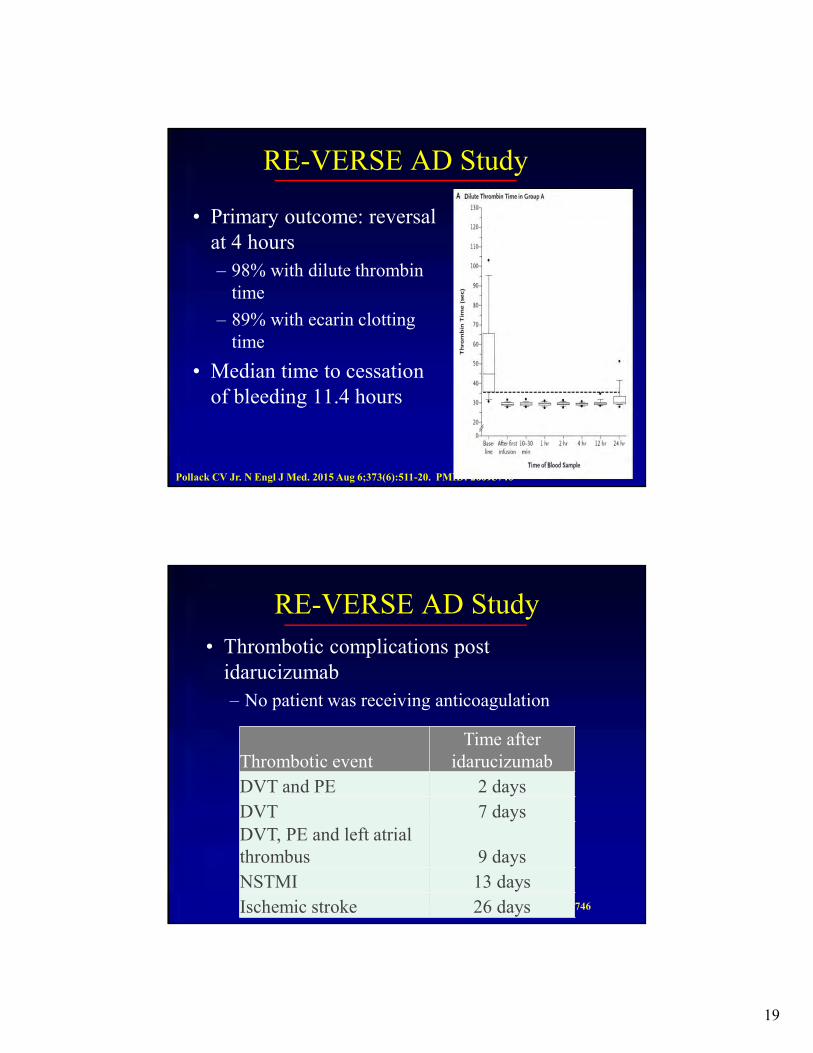
RE-VERSE AD Study
• Primary outcome: reversal at 4 hours
– 98% with dilute thrombin time
– 89% with ecarin clotting time
• Median time to cessation of bleeding 11.4 hours
Pollack CV Jr. N Engl J Med. 2015 Aug 6;373(6):511-20. PMID: 26095746
RE-VERSE AD Study
• Thrombotic complications post idarucizumab
– No patient was receiving anticoagulation
Pollack CV Jr. N Engl J Med. 2015 Aug 6;373(6):511-20. PMID: 26095746
Thrombotic eventTime after
idarucizumab
DVT and PE 2 days
DVT 7 daysDVT, PE and left atrial thrombus 9 days
NSTMI 13 days
Ischemic stroke 26 days

20
Protocol to Reverse Dabigatran with Idarucizumab
Eikelboom JW. Circulation. 2015 Dec 22;132(25):2412-22. PMID: 26700008
Ansell JE. N Engl J Med. 2014 Nov 27;371(22):2141-2. PMID: 25371966
Ciraparantag (PER977 or Aripazine)

21
Take Home Points
• Reversing anticoagulation puts the patient at risk for a clot
• Don’t forget to do all of the other things to stop bleeding
• Idarucizumab (Praxbind) is specific for dabigatran (Pradaxa) reversal
• 4 factor inactivated (Kcentra) or activated (FEIBA) PCC should be considered to reverse Anti-Xa drugs
• Restart anticoagulation after reversal when feasible

22
Andrew Dunn, MD, MPHProfessor of Medicine
Chief, Division of Hospital MedicineMount Sinai Health System, NY
Cost-effective Management of PE
Case-based Discussion of Essential Issues in
Anticoagulant ManagementMarch 8, 2016
CASE - PE
A 58 year-old man with htn and COPD is admitted with SOB for 1 day. He has a dry cough. There is no hemoptysis or chest pain. He was diagnosed with a DVT 4 years ago, for which he received 6 months of warfarin.
His medications are HCTZ, tiotropium MDI and fluticasone MDI.

23
CASE - PE
On exam, the patient appears comfortable. HR 92, RR 16, BP 136/90. O2 sat (RA) 93%. Chest exam is normal. There are no crackles or wheezes and airflow is normal. The heart exam is normal. The right leg is swollen.
Labs are significant for WBC 8.1, Hb 13.0. Renal function is normal. A CTA reveals a PE in a right segmental artery.
The patient lives with his wife. He has commercial health insurance. The hospitalist and PCP discuss the case. The plan is for indefinite anticoagulation.
Aujesky D. Lancet. 2011;378:41-8.
Age +58Male sex +10Cancer +30CHF +10Chronic lung disease +10Pulse ≥110 +20SBP<100 +30RR ≥30 +20Temperature <36°C +20Altered mental status +60O2 saturation <90% +20
Pulmonary Embolism Severity Index
SCORE<66 I66–85 II86–105 III106–125 IV>125 V

24
CASE - PE
From the perspective of society, the most cost-effective strategy would be:
A. Admission, start treatment with LMWH + warfarin; discharge after ≥5 days overlap and INR therapeutic
B. Admission, start treatment with DOAC; discharge after ≥5 days
C. Discharge home from ED on LMWH + warfarin
D. Discharge home from ED on DOAC
E. Thrombolysis, followed by thrombectomy and IVC filter placement, with lifelong LMWH
Imperative of providing high-value care
Hospitalists as stewards of finite resources
Perspective
Society Payer Hospital Patient
Health Care Costs

25
EINSTEIN PE TrialDischarge with LOS <5 days increased in rivaroxaban group compared with LMWH/VKA (45% vs 33%)
Early Discharge with DOACs
Van Bellen B, et al. Current Medical Research and Opinion. 2014;30:829-37.
Lefebvre P, et al. J Med Econ. 2014;17:52-64.
Markov model - Based on EINSTEIN RCT
Calculated cost, quality-adjusted life-years (QALYs)
Compared to LMWH/VKA
Duration - 3, 6, or 12 months
Probabilities obtained from EINSTEIN trials during treatment and
published literature after treatment
US payer perspective
Cost-effectiveness Analysis
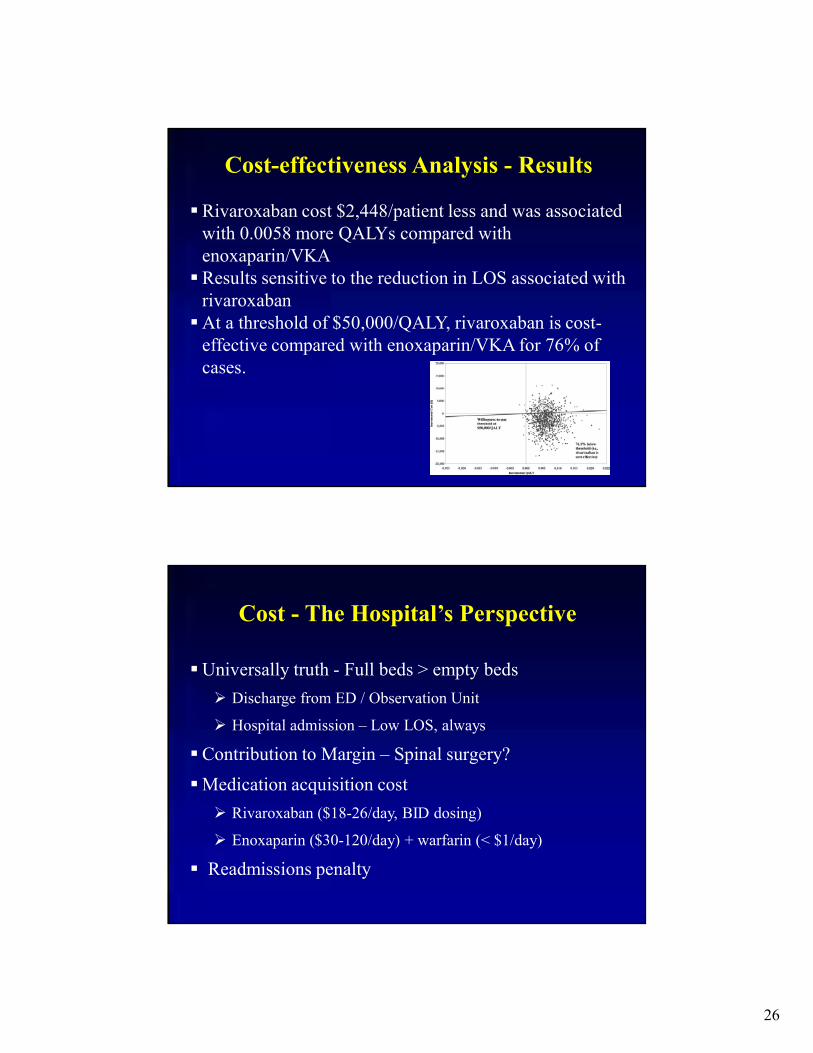
26
Rivaroxaban cost $2,448/patient less and was associated with 0.0058 more QALYs compared with enoxaparin/VKA
Results sensitive to the reduction in LOS associated with rivaroxaban
At a threshold of $50,000/QALY, rivaroxaban is cost-effective compared with enoxaparin/VKA for 76% of cases.
Cost-effectiveness Analysis - Results
Universally truth - Full beds > empty beds
Discharge from ED / Observation Unit
Hospital admission – Low LOS, always
Contribution to Margin – Spinal surgery?
Medication acquisition cost
Rivaroxaban ($18-26/day, BID dosing)
Enoxaparin ($30-120/day) + warfarin (< $1/day)
Readmissions penalty
Cost - The Hospital’s Perspective

27
Health insurance – none, some, plenty Co-pay Duration of Treatment
Cost - The Patient’s Perspective
Take Home Points
Appropriate selection of patients with PE who can be treated primarily at home is a high-value practice
Hospitalists are stewards of limited healthcare resources
Treat the patient, not the disease or score – Address all clinical, social, and logistical concerns
Cost-analyses demonstrate Anti-Xa inhibitors are cost-effective relative to LMWH/warfarin

28
Impact of CKD on Afib Management
Case-based Discussion of Essential Issues in
Anticoagulant Management
Hospital Medicine 2016
San Diego
8 March 2016
Steve Deitelzweig, MD, MMM, SFHM, FACP
System Chairman – Hospital Medicine
Medical Director – Regional Medical Director
Associate Professor of Medicine – Univ of Queensland
Ochsner Health System
29
• Speaker honorarium– Janssen– Bristol Myer Squibb/Pfizer– Daiichi Sankyo
• Consultant– Bristol Myer Squibb/Pfizer– Janssen– Daiichi Sankyo– Portola
• Board membership (non-profit)– Society of Cardiovascular Patient Care
Disclosure
AF Patients Often Managed by Hospitalists
Study of >55,000 patients aged ≥65 y with AF
• >50% admitted to the hospital for AF within 24 mo – 43.7% for readmissions and comorbidities
• Hypertension (80.5%)• Structural heart disease (32.9%)• Coronary artery disease (23.1%)• Diabetes (19%)
– 60% of patients were receiving warfarin
≈75% of the total direct and indirect costs of AF are hospitalization costs—clinical strategies to optimize care
by improving outcomes are critical58
Deitelzweig S. Ochsner J. 2013;13:2005-419-427.

30
Balancing Stroke and Bleeding Risk: Tools for Assessing Stroke Risk
59
CHADS2 Score1 CHA2DS2-VASc Score*2
Risk Factor Score
Congestive heart failurea 1
Hypertensionb 1
Age ≥75 y 2
Diabetes 1
Stroke/TIA/TE history 2
Vascular diseasec 1
Age 65-74 years 1
Sex category, female 1
MAXIMUM 9
Risk Factor Score
Congestive heart failure 1
Hypertensionb 1
Age ≥75 y 1
Diabetes 1
Stroke or TIA history 2
MAXIMUM 6
1. Gage BF et al. JAMA. 2001;285:2864-2870. 2. Lip GY et al. Chest. 2010;137:263-272. Reproduced with permission of the American College of Chest Physicians. 2. January CT et al. Circulation.2014. Mar 28. pii: S0735-1097(14)01740-9.
*In patients with NVAF, the CHA2DS2-VASc Score is recommended for assessment of stroke risk due to higher sensitivity in patients with CHADS2 Score = 12
Adjusted Risk for Stroke for CHADS2
and CHA2DS2-VASC Scores1,2
Score CHADS2
(%/y)1
CHA2DS2-VASc (%/y)2
0 1.9 0
1 2.8 1.3
2 4 2.2
3 5.9 3.2
4 8.5 4.0
5 12.5 6.7
6 18.2 9.8
7 9.6
8 6.7
9 15.2
1. Gage BF et al. JAMA. 2001;285:2864-2870. 2. Lip GY et al. Chest. 2010;137:263-272.
60
31
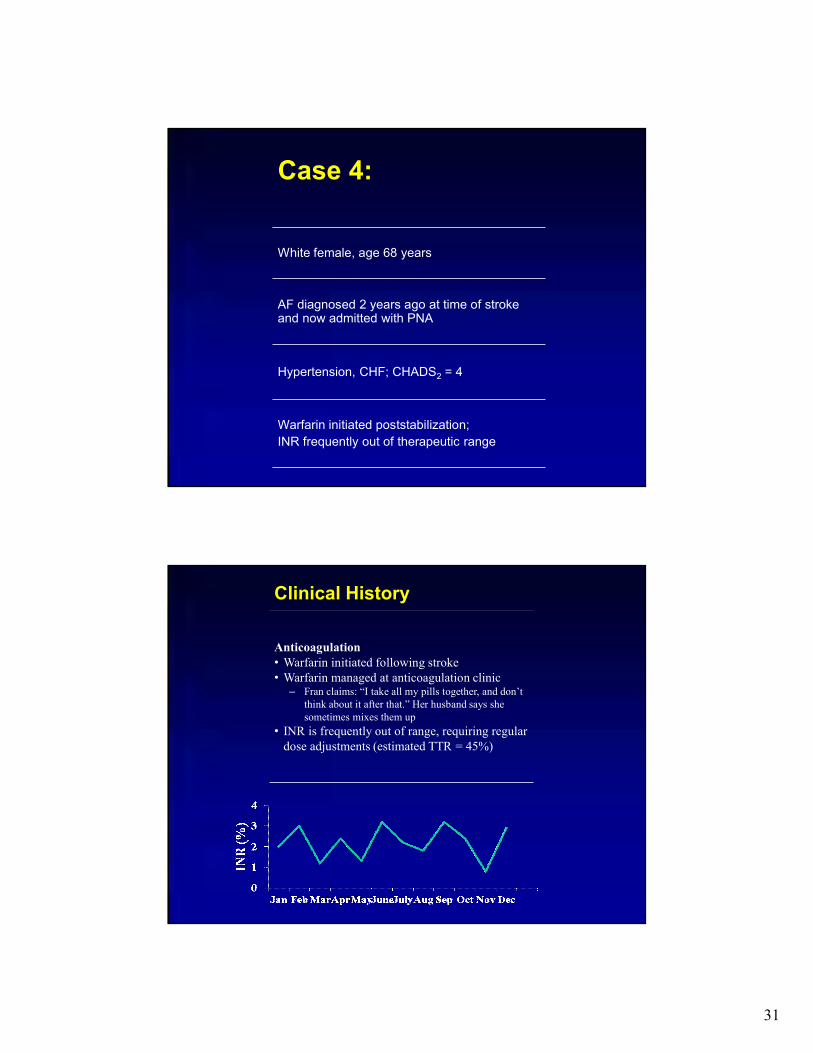
Case 4:
White female, age 68 years
AF diagnosed 2 years ago at time of stroke and now admitted with PNA
Hypertension, CHF; CHADS2 = 4
Warfarin initiated poststabilization;
INR frequently out of therapeutic range
Clinical History
Anticoagulation• Warfarin initiated following stroke • Warfarin managed at anticoagulation clinic
– Fran claims: “I take all my pills together, and don’t think about it after that.” Her husband says she sometimes mixes them up
• INR is frequently out of range, requiring regular dose adjustments (estimated TTR = 45%)
Month 2010

32
Clinical History
Anticoagulation (cont)• To investigate the cause of Fran’s fluctuating INR,
the physician asks:– Are you taking any OTC medication?– Have you been treated intermittently with any
antibiotics?– Does your diet/alcohol consumption vary
significantly from week to week?
• answers no to all questions
• inquires about new agent her husband heard about
Current Clinical Assessment
• BP = 122/78 mm Hg; pulse rate = 84 bpm, irregularly irregular
• CBC/SMAC-20 = unremarkable; estimated CrCl = 58 mL/min; HbA1C = 5.6%
• ECG AF rate = 76, indicating left ventricular hypertrophy
• CHADS2 = 4

33
Which Options for Stroke Prevention Would You Endorse?
A. ASA 81 mg po daily and Clopidogrel 75 mg po daily
B. Continue Warfarin with a target INR of 2-3
C. ASA 81 mg po qd
D. DOAC like Dabigatran 150 mg po bid
E. Use another brand for Warfarin like Coumadin
Case Study: Discussion

34
Overview of Phase 3 Clinical Trials in AF: DOACs vs Warfarin
67
1. Connolly SJ et al. N Engl J Med. 2009;361:1139-1151. 2. Connolly SJ et al. N Engl J Med. 2010;363;1875-1876. 3. Patel MR et al. N Engl J Med. 2011;365:883-891.4. Granger CB et al. N Engl J Med. 2011;365:981-992.5. Giugliano RP et al. N Engl J Med. 2013; 369:2093-2104.
RE-LY1,2
N=18,113 (3 arms)ROCKET-AF3
N=14,264ARISTOTLE4
N=18,201ENGAGE AF-TIMI 485
N=14,264
Drug, doseDabigatran
110 or 150 mg BIDRivaroxaban 20 mg QDay
Apixaban 5 mg BID
Edoxaban30 or 60 mg QDay
Adjusted dose?a NoYes: 15 mg QDay if CrCl 30-49 mL/min
Yes: 2.5 mg BID if 2 of: age ≥80 y, weight <60 kg,
SCr ≥1.5 mg/dL
Yes: Both doses halved if: CrCl 30-50 mL/min, weight
≤60 kg, use of verapamil, quinidine, or dronederone
DesignRandomized open-label
Randomized double-blind, double-dummy
Randomized double-blind, double-dummy
Randomized double-blind, double-dummy
Mean age, y 71.5 73 70 72
Prior stroke/TIA/SE
20% 55% 19% 28.5%
Mean CHADS2 2.1 3.5 2.1 2.8
Warfarin naïve 50.4% 37.6% 43% 41%
Comparator Warfarin INR 2-3
64% TTR (mean) 55% TTR (mean) 62% TTR (mean) 65% (mean)
aPatients with the following CrCl (mL/min) excluded: ARISTOTLE: <25 or SCr >2.5 mg/dL; RE-LY: <30; ROCKET-AF: <30; ENGAGE AF-TIMI 48 <30
Dabigatran1 Rivaroxaban2 Apixaban3 Edoxaban4
Drug classDirect factor IIa
inhibitorDirect factor Xa inhibitor
Direct factor Xa inhibitor
Direct factor Xa inhibitor
Time to Cmax 1 h 2-4 h 3-4 h 1-2 h
CYP metabolism NoneCYP3A4/5, CYP2J2, and
hydrolysis are the major means of biotransformation
Mainly by CYP3A4 Minimal
Renal excretion(unchanged drug)
80% of absorbed dose
66% of total dose; 36% of absorbed dose
27% 50%
Protein binding 35% 92-95% 85% 55%
Half-life 12-17 h 5-9 h ≈12 h 9-11 h
Dosing frequency NVAF
BID QDay BID QDay
1. Pradaxa (dabigatran etexilate mesylate) [prescribing information]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals Inc.; 9/2014. 2. Xarelto (rivaroxaban) [prescribing information]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; 9/2014. 3. Eliquis (apixaban) [prescribing information]. Princeton, NJ: Bristol-Myers Squibb Company; 8/2014. 4. Savaysa (edoxaban) [prescribing information]. Parsippany, NJ: Daiichi Sankyo, Inc; 1/2015.
Pharmacology of DOACs: PK/PD
68
Cmax, time to maximum concentration; PK/PD, pharmacokinetics/pharmacodynamics

35
Drug Dosea
Dabigatran1
• CrCl >30 mL/min, 150 mg orally BID
• CrCl 15-30 mL/min, 75 mg orally BID
• CrCl <15 mL/min or on dialysis, dosing recommendations cannot be provided
Rivaroxaban2
• Take 15 mg and 20 mg tablets with food; take 10 mg tablets with or without food
• CrCl >50 mL/min, 20 mg orally QDay with the evening meal
• CrCl 15-50 mL/min, 15 mg orally QDay with the evening meal
• CrCl <15 mL/min, avoid use since drug exposure is increased
Apixaban3
• 5 mg orally BID• 5 mg orally BID in patients with NVAF and ESRD maintained on hemodialysis• 2.5 mg orally BID in patients with at least 2 of the following characteristics: age ≥80 y, body
weight ≤60 kg or serum Cr ≥1.5 mg/dL
Edoxaban4b• High dose: 60 mg orally QDay• Low dose: 30 mg orally QDay• Both doses halved if CrCl 30-50 mL/min, low body weight ≤60 kg, or taking concomitant verapamil,
quinidine or dronedarone
DOAC Dosing by Indication:Atrial Fibrillation
69
ESRD, end-stage renal disease aPatients with with CrCl < 30 for apixaban and dabigatran and <25 for rivaroxaban excluded from clinical trials . bNot currently approved by the US FDA for this indication1. Pradaxa (dabigatran etexilate mesylate) [prescribing information]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals Inc.; 9/2014.2. Xarelto (rivaroxaban) [prescribing information]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; 9/2014. 3. Eliquis (apixaban) [prescribing information]. Princeton, NJ: Bristol-Myers Squibb Company; 8/2014. 4. Giugliano RP et al. N Engl J Med. 2013; 369:2093-2104.
Recommendations COR LOE
Antithrombotic therapy based on shared decision making, discussion of risks of stroke and bleeding and patients preferences
I C
Antithrombotic therapy selection based on risk for thromboembolism I B
CHA2DS2-VASc score recommended to assess stroke risk I B
Warfarin recommended with mechanical heart valves; target INR based on type/location of prosthesis I B
With prior stroke, TIA, or CHA2DS2-VASc score ≥2, OACs recommended; options include:
• Warfarin I A
• Dabigatran, rivaroxaban, or apixaban I B
With warfarin, determine INR at least weekly and monthly when stable I A
Direct thrombin inhibitor or factor Xa inhibitor recommended if unable to maintain therapeutic INR I C
Reevaluate need for anticoagulation at periodic intervals I C
Evaluate renal function prior to initiation of direct thrombin inhibitor or factor Xa inhibitors, and re-evaluate when clinically indicated and at least annually
I B
70
AHA/ACC/HRS Recommendations for Prevention of Thromboembolism in AF
ACC, American College of Cardiology; AHA, American Heart Association; COR, category of recommendation; HRS, Heart Rhythm Society; LOE, level of evidence January CT et al. J Am Coll Cardiol. 2014 ;64(21):e1-e76.
36
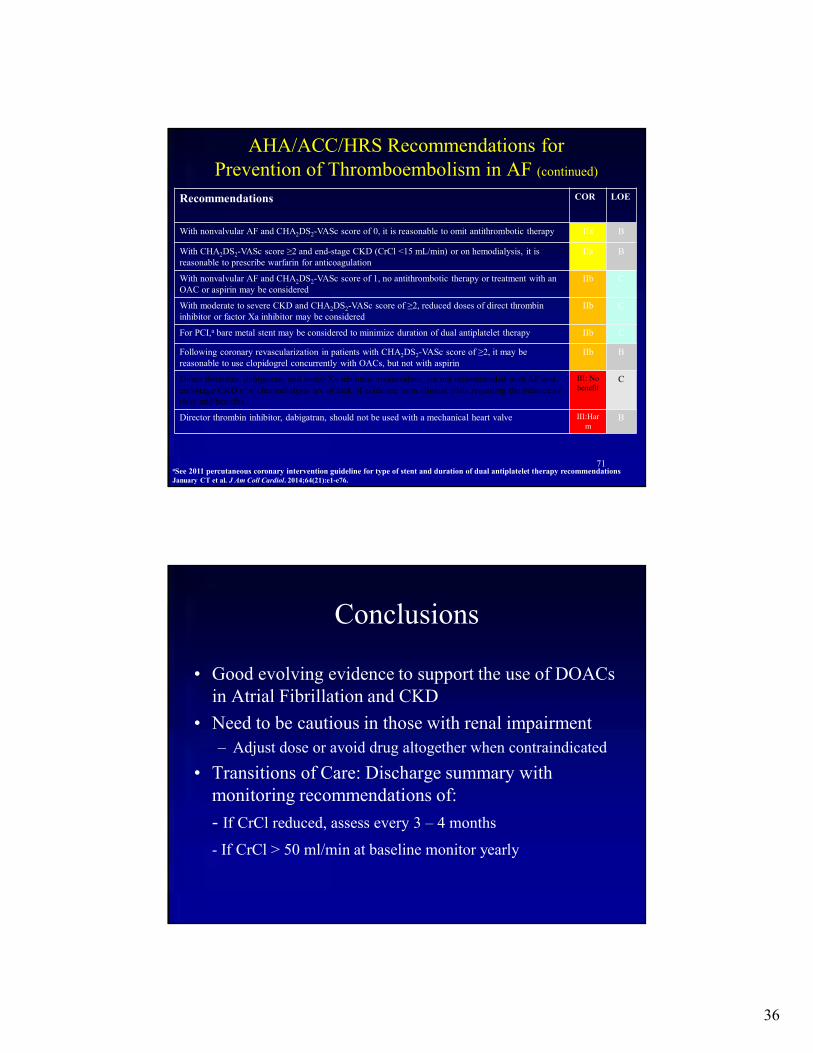
Recommendations COR LOE
With nonvalvular AF and CHA2DS2-VASc score of 0, it is reasonable to omit antithrombotic therapy IIa B
With CHA2DS2-VASc score ≥2 and end-stage CKD (CrCl <15 mL/min) or on hemodialysis, it is reasonable to prescribe warfarin for anticoagulation
IIa B
With nonvalvular AF and CHA2DS2-VASc score of 1, no antithrombotic therapy or treatment with an OAC or aspirin may be considered
IIb C
With moderate to severe CKD and CHA2DS2-VASc score of ≥2, reduced doses of direct thrombin inhibitor or factor Xa inhibitor may be considered
IIb C
For PCI,a bare metal stent may be considered to minimize duration of dual antiplatelet therapy IIb C
Following coronary revascularization in patients with CHA2DS2-VASc score of ≥2, it may be reasonable to use clopidogrel concurrently with OACs, but not with aspirin
IIb B
Direct thrombin, dabigatran, and factor Xa inhibitor, rivaroxaban, are not recommended with AF and end-stage CKD or on hemodialysis b/c of lack of evidence from clinical trials regarding the balance of risks and benefits
III: No benefit
C
Director thrombin inhibitor, dabigatran, should not be used with a mechanical heart valve III:Harm
B
71
AHA/ACC/HRS Recommendations for Prevention of Thromboembolism in AF (continued)
aSee 2011 percutaneous coronary intervention guideline for type of stent and duration of dual antiplatelet therapy recommendationsJanuary CT et al. J Am Coll Cardiol. 2014;64(21):e1-e76.
Conclusions
• Good evolving evidence to support the use of DOACs in Atrial Fibrillation and CKD
• Need to be cautious in those with renal impairment
– Adjust dose or avoid drug altogether when contraindicated
• Transitions of Care: Discharge summary with monitoring recommendations of:
- If CrCl reduced, assess every 3 – 4 months
- If CrCl > 50 ml/min at baseline monitor yearly
37
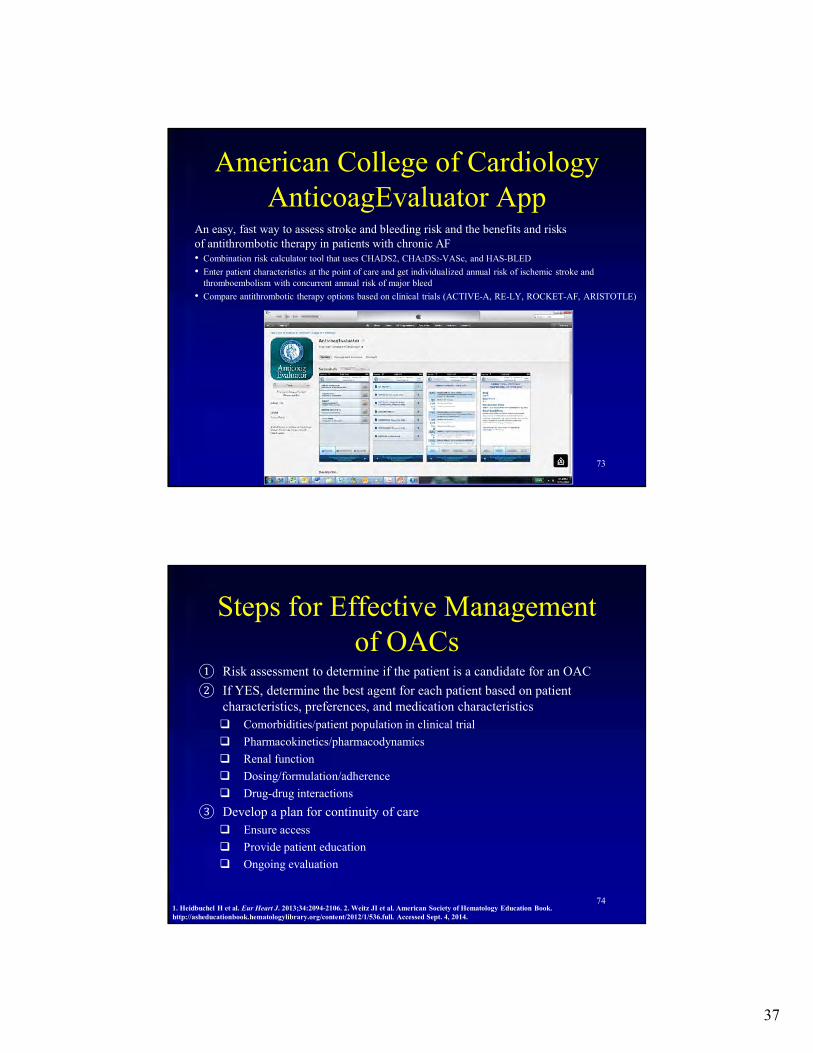
American College of Cardiology AnticoagEvaluator App
73
An easy, fast way to assess stroke and bleeding risk and the benefits and risks of antithrombotic therapy in patients with chronic AF• Combination risk calculator tool that uses CHADS2, CHA2DS2-VASc, and HAS-BLED
• Enter patient characteristics at the point of care and get individualized annual risk of ischemic stroke and thromboembolism with concurrent annual risk of major bleed
• Compare antithrombotic therapy options based on clinical trials (ACTIVE-A, RE-LY, ROCKET-AF, ARISTOTLE)
Steps for Effective Management of OACs
① Risk assessment to determine if the patient is a candidate for an OAC
② If YES, determine the best agent for each patient based on patient characteristics, preferences, and medication characteristics
Comorbidities/patient population in clinical trial
Pharmacokinetics/pharmacodynamics
Renal function
Dosing/formulation/adherence
Drug-drug interactions
③ Develop a plan for continuity of care
Ensure access
Provide patient education
Ongoing evaluation
741. Heidbuchel H et al. Eur Heart J. 2013;34:2094-2106. 2. Weitz JI et al. American Society of Hematology Education Book. http://asheducationbook.hematologylibrary.org/content/2012/1/536.full. Accessed Sept. 4, 2014.

38
Perioperative Management ofDirect oral Anticoagulants
(DOACs)
Amir K Jaffer, MD, MBA, SFHMProfessor of Medicine
Associate Chief Medical OfficerVice Chair, Patient Safety and QualityDivision Director, Hospital Medicine
Department of Internal Medicine

39
Disclosure Statement
• Consultant– Boehringer-Ingelheim, Janssen
Pharmaceuticals, Pfizer, BMS, Medtronic, Daiichi Sankyo, Astra Zeneca
• Research and Grant Support– NHLBI, Astra-Zeneca
• Board Member– Society of Perioperative Assessment and
Quality Improvement (SPAQI)
Anticoagulation in the Perioperative Period has Become More Challenging
Perioperative
Landscape
Warfarin (Coumadin)
Dabigatran(Pradaxa)
Rivaroxaban(Xarelto)
Apixaban
(Eliquis)
Edoxaban(Savaysa)
• Pharmacokinetics of the NOACs are different
• Lack of Level 1 evidence
• Varying Knowledge about DOACs amongst clinicians
• Litigation
40
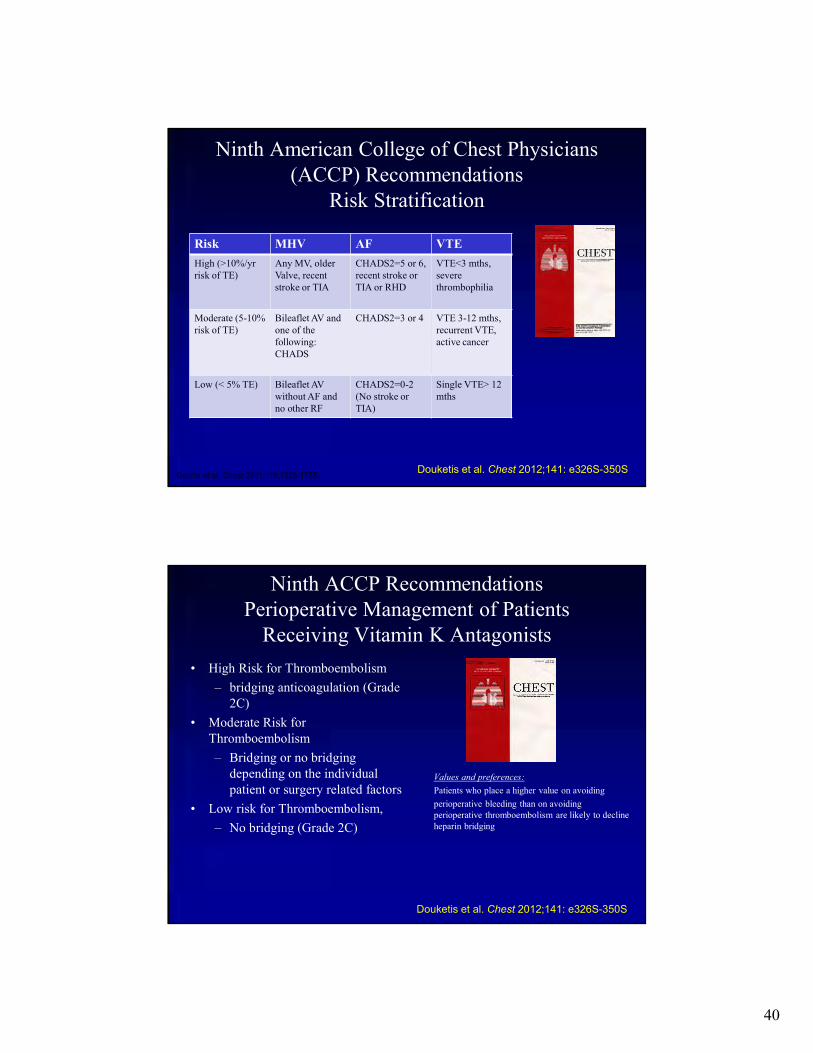
Ninth American College of Chest Physicians (ACCP) Recommendations
Risk Stratification
Geerts et al. Chest 2001;119:132S-175S. Douketis et al. Chest 2012;141: e326S-350S
Risk MHV AF VTE
High (>10%/yr risk of TE)
Any MV, older Valve, recent stroke or TIA
CHADS2=5 or 6, recent stroke or TIA or RHD
VTE<3 mths,severe thrombophilia
Moderate (5-10%risk of TE)
Bileaflet AV and one of the following: CHADS
CHADS2=3 or 4 VTE 3-12 mths, recurrent VTE, active cancer
Low (< 5% TE) Bileaflet AV without AF and no other RF
CHADS2=0-2 (No stroke or TIA)
Single VTE> 12 mths
Ninth ACCP RecommendationsPerioperative Management of Patients
Receiving Vitamin K Antagonists
• High Risk for Thromboembolism
– bridging anticoagulation (Grade 2C)
• Moderate Risk for Thromboembolism
– Bridging or no bridging depending on the individual patient or surgery related factors
• Low risk for Thromboembolism,
– No bridging (Grade 2C)
Values and preferences:
Patients who place a higher value on avoiding
perioperative bleeding than on avoiding perioperative thromboembolism are likely to decline heparin bridging
Douketis et al. Chest 2012;141: e326S-350S
41
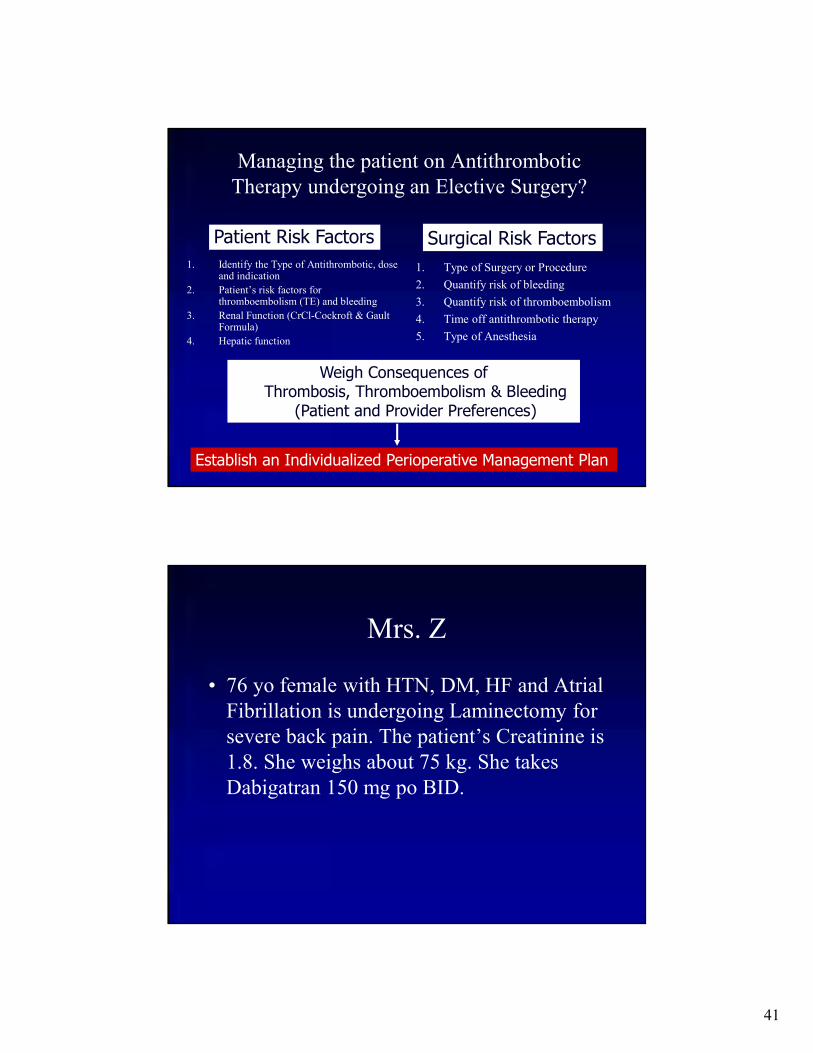
Managing the patient on Antithrombotic Therapy undergoing an Elective Surgery?
1. Identify the Type of Antithrombotic, dose and indication
2. Patient’s risk factors for thromboembolism (TE) and bleeding
3. Renal Function (CrCl-Cockroft & Gault Formula)
4. Hepatic function
1. Type of Surgery or Procedure
2. Quantify risk of bleeding
3. Quantify risk of thromboembolism
4. Time off antithrombotic therapy
5. Type of Anesthesia
Patient Risk Factors Surgical Risk Factors
Weigh Consequences of Thrombosis, Thromboembolism & Bleeding
(Patient and Provider Preferences)
Establish an Individualized Perioperative Management Plan
Mrs. Z
• 76 yo female with HTN, DM, HF and Atrial Fibrillation is undergoing Laminectomy for severe back pain. The patient’s Creatinine is 1.8. She weighs about 75 kg. She takes Dabigatran 150 mg po BID.

42
The last dose of Dabigatran should be taken when?
1. 5-days before surgery (8-doses)
2. 4-days before surgery (6-doses)
3. 3-days before surgery (4-doses)
4. 2-days before surgery (2-doses)
5. 1-day before surgery (hold only day of surgery doses)
Overview of Pharmacology of DOACs: Impact of PK/PD
Cmax, time to maximum concentration; PK/PD, pharmacokinetics/pharmacodynamics
1. Pradaxa (dabigatran) [prescribing information]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals Inc.; 9/2014. 2. Xarelto (rivaroxaban) [prescribing information]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; 9/2014. 3. Eliquis (apixaban) [prescribing information]. Princeton, NJ: Bristol-Myers Squibb Company; 8/2014. 4. Camm AJ et al. Drugs. 2011;71:1503-1526. 5. Ogata K et al. J Clin Pharmacol. 2010;50:743-753. 6. Eikelboom JW et al. Circulation. 2010;121:1523-1532. 7. Bathala M et al. Drug Metab Dispos. 2012;40:2250-55.
Dabigatran1 Rivaroxaban2 Apixaban3 Edoxaban4-7
Drug class Direct factor Direct factor Direct factor Direct factorIIa inhibitor Xa inhibitor Xa inhibitor Xa inhibitor
Time to Cmax 1 h 2-4 h 3-4 h 1-2 h
CYP metabolism None CYP3A4/5, CYP2J2, Mainly by 62%and hydrolysis are CYP3A4 fecal elimination
the major means ofbiotransformation
Renal excretion 80% of 66% of total dose; 27% 35% of total(unchanged drug) absorbed dose 36% of absorbed dose; 49% of
dose absorbed dose
Half-life 12-17 h 5-9 h ≈12 h 9-11 h
Dosing frequency BID QD BID QDfor NVAF
43
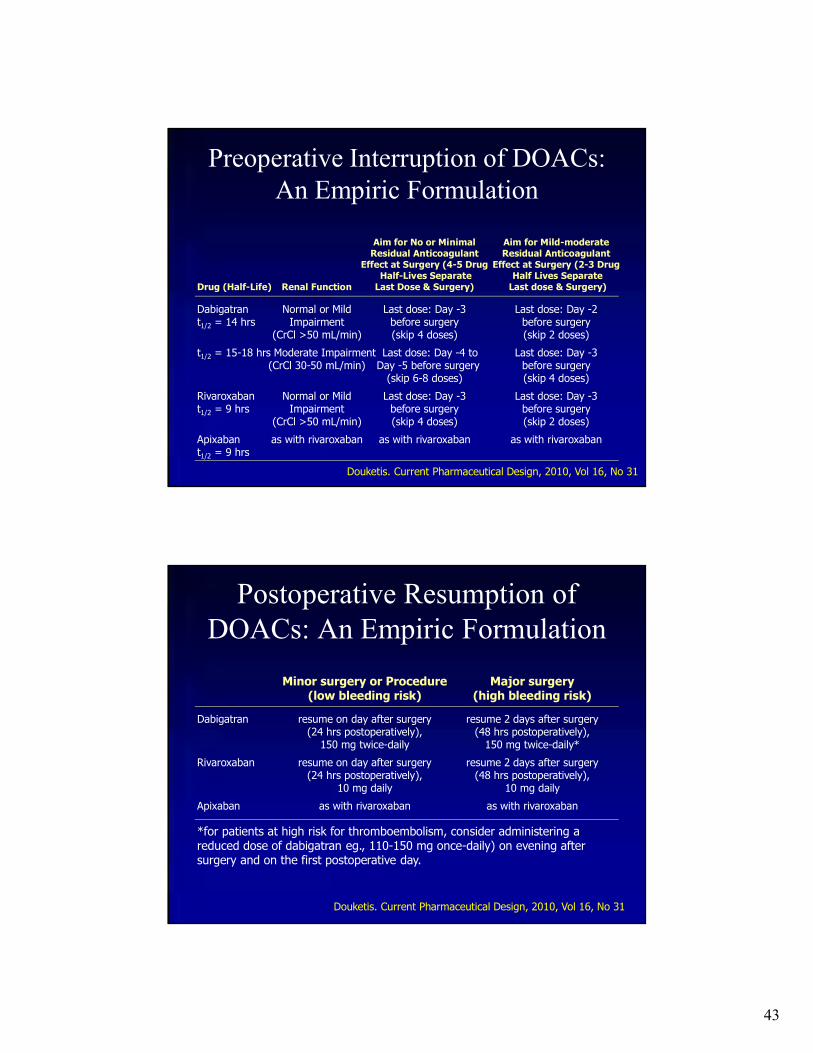
Preoperative Interruption of DOACs: An Empiric Formulation
Dabigatran Normal or Mild Last dose: Day -3 Last dose: Day -2t1/2 = 14 hrs Impairment before surgery before surgery
(CrCl >50 mL/min) (skip 4 doses) (skip 2 doses)
t1/2 = 15-18 hrs Moderate Impairment Last dose: Day -4 to Last dose: Day -3(CrCl 30-50 mL/min) Day -5 before surgery before surgery
(skip 6-8 doses) (skip 4 doses)
Rivaroxaban Normal or Mild Last dose: Day -3 Last dose: Day -3t1/2 = 9 hrs Impairment before surgery before surgery
(CrCl >50 mL/min) (skip 4 doses) (skip 2 doses)
Apixaban as with rivaroxaban as with rivaroxaban as with rivaroxabant1/2 = 9 hrs
Aim for No or Minimal Aim for Mild-moderateResidual Anticoagulant Residual Anticoagulant
Effect at Surgery (4-5 Drug Effect at Surgery (2-3 DrugHalf-Lives Separate Half Lives Separate
Drug (Half-Life) Renal Function Last Dose & Surgery) Last dose & Surgery)
Douketis. Current Pharmaceutical Design, 2010, Vol 16, No 31
Postoperative Resumption of DOACs: An Empiric Formulation
Dabigatran resume on day after surgery resume 2 days after surgery(24 hrs postoperatively), (48 hrs postoperatively),
150 mg twice-daily 150 mg twice-daily*
Rivaroxaban resume on day after surgery resume 2 days after surgery(24 hrs postoperatively), (48 hrs postoperatively),
10 mg daily 10 mg daily
Apixaban as with rivaroxaban as with rivaroxaban
Douketis. Current Pharmaceutical Design, 2010, Vol 16, No 31
Minor surgery or Procedure Major surgery(low bleeding risk) (high bleeding risk)
*for patients at high risk for thromboembolism, consider administering a reduced dose of dabigatran eg., 110-150 mg once-daily) on evening after surgery and on the first postoperative day.

44
Periprocedural Management of DOACs: Postprocedure Timing of DOAC Resumption
• Depends solely on the postoperative risk for bleeding1,2
– Risk for major bleeding complications postsurgery clearly outweighs risk for thromboembolism1
• For major abdominal or urologic surgery: Delay DOACs until no drainage or signs of active bleeding
• For procedures with good hemostasis shortly afterwards: Resume NOACs a minimum of 4-6 h postsurgery
• In the case of bowel paralysis, bridging with a parenteral anticoagulant may be required
• Dabigatran, rivaroxaban, and apixaban should be resumed 24-48 h after minor procedure, or 48-72 h after major surgery, assuming that hemostasis achieved2
• Dabigatran, Rivaroxaban, Abixaban resume with half-dose for 1-3d depending on surgery, then resume usual maintenance dose1
1. Schulman S et al. Blood. 2012;119:3016-3023. 2. Nutescu EA. Am J Health-Syst Pharm. 2013;70(Suppl 1)S2-S11
Do you recommend Bridging with LMWH given a CHADS2
score of 4?
1. Yes
2. No

45
Peri-interventional Management of NOACs: Results from the Dresden Registry
• Evaluation of NOAC management in unselected patients from daily care
• 2179 Patients on NOACs
• 595 underwent 863 procedures, median age 74
• Outcomes adjudicated using standard event definitions
Minimal Procedures were procedures with little tissue traumaMinor procedures were procedures with little tissue trauma but relevant bleeding riskMajor procedures were procedures with relevant tissue trauma and high bleeding risk
Results
CI 0.5-2.0
CI 1.3-11.4
CI 3.3-15.9
CI 0.2-3.4
CI 0.9-5.0
N=863
46
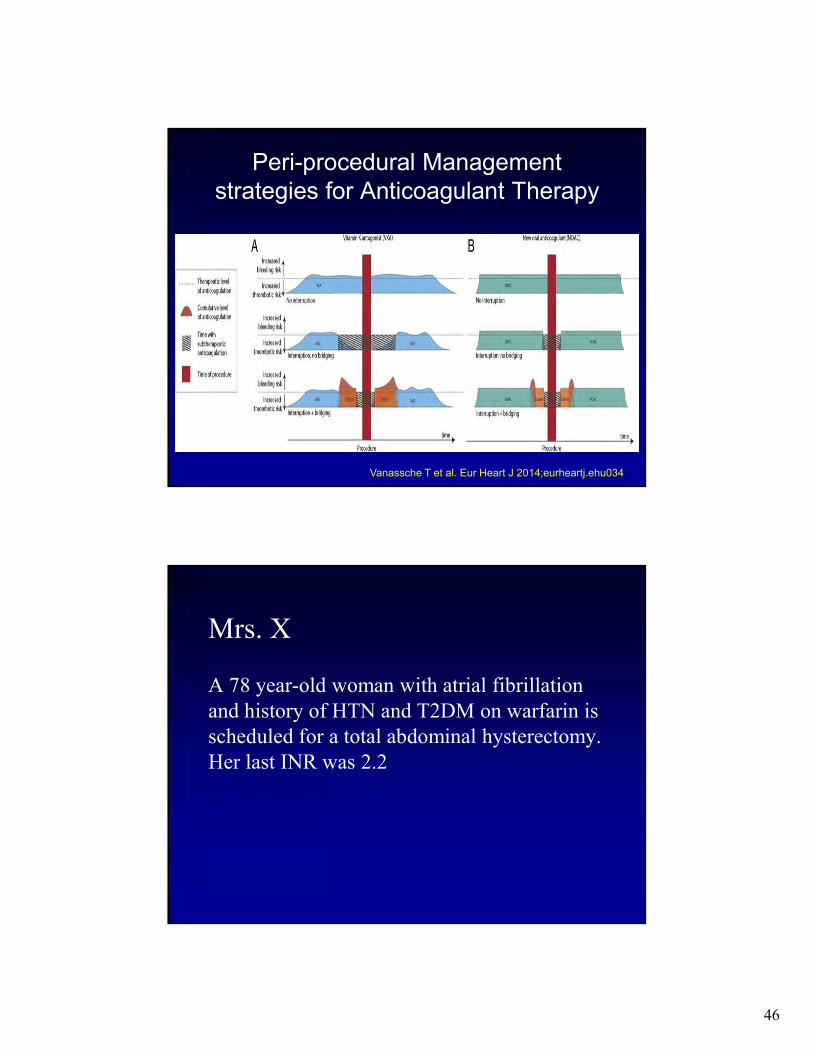
Peri-procedural Management strategies for Anticoagulant Therapy
Vanassche T et al. Eur Heart J 2014;eurheartj.ehu034
Mrs. X
A 78 year-old woman with atrial fibrillation and history of HTN and T2DM on warfarin is scheduled for a total abdominal hysterectomy. Her last INR was 2.2

47
What would you recommend for Perioperative Anticoagulation Management?
1. Stop warfarin 3 days preop and restart 1 day postop
2. Stop warfarin 5 days preop and restart 1 day postop
3. Stop warfarin 5 days preop, bridge with full dose LMWH preop, restart warfarin and full dose LMWH 1 day postop
4. Stop warfarin 5 days preop, admit for IV UFH, restart warfarin and UFH 1 day postop
BRIDGING ANTICOAGULATION IN PATIENTS WHO
REQUIRE TEMPORARY INTERRUPTION OF WARFARIN THERAPY FOR AN ELECTIVE
PROCEDURE OR SURGERY
Thomas L. Ortel, MD, PhD, on behalf of the BRIDGE Investigators and Committees
The BRIDGE trial was funded by the U.S. National Heart, Lung, and Blood Institute of the U.S. National Institutes of Health

48
Hypotheses
We hypothesized that:
1) Forgoing bridging anticoagulation in patients with atrial fibrillation (AF) who needed warfarin held for an operation or invasive procedure would be non-inferior to bridging with LMWH for the prevention of perioperative arterial thromboembolism (ATE)
- and –
2) Forgoing bridging anticoagulation would be superior to bridging with respect to major bleeding
Trial Design

49
Inclusion Criteria• 18 years or older
• Chronic (permanent or paroxysmal) AF or atrial flutter, confirmed by electrocardiography or pacemaker interrogation
• AF associated with valvular disease, including mitral valve disease
• Received warfarin therapy for 3 months or longer, with a target INR therapeutic range of 2.0–3.0
• Undergoing an elective operation or invasive procedure requiring warfarin interruption
• At least one of the following CHADS2
stroke risk factors:
– Congestive heart failure or left ventricular dysfunction
– Hypertension
– 75 years or older
– Diabetes mellitus
– Previous ischemic stroke, systemic embolism, or transient ischemic attack (TIA)
Exclusion Criteria
• Mechanical heart valve
• Stroke, systemic embolism, or TIA within previous 12 weeks
• Major bleeding within previous 6 weeks
• Venous thromboembolism within the previous 12 weeks
• Creatinine clearance <30 mL/min
• Platelet count <100×103 per cubic millimeter
• Planned cardiac, intracranial, or intraspinal surgery
• Unable or unwilling to provide informed consent
50
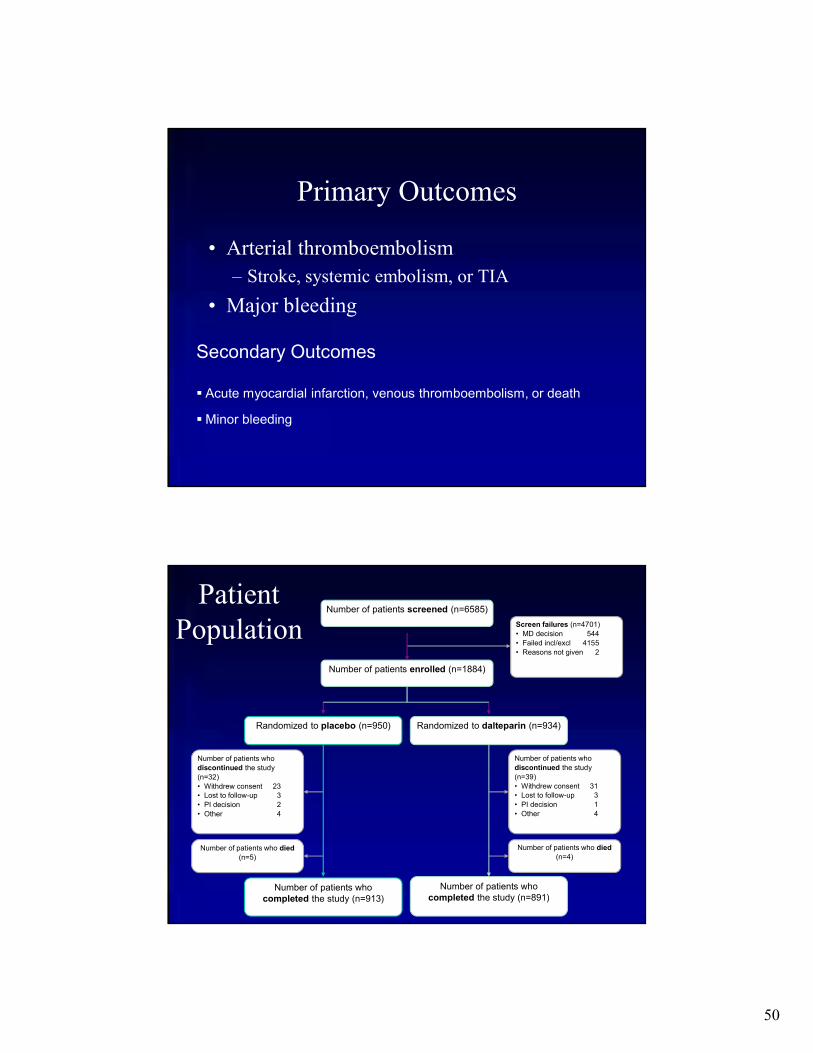
Primary Outcomes
• Arterial thromboembolism
– Stroke, systemic embolism, or TIA
• Major bleeding
Secondary Outcomes
Acute myocardial infarction, venous thromboembolism, or death
Minor bleeding
Number of patients who
discontinued the study
(n=32)
• Withdrew consent 23• Lost to follow-up 3
• PI decision 2
• Other 4
Number of patients who
discontinued the study
(n=39)
• Withdrew consent 31• Lost to follow-up 3
• PI decision 1
• Other 4
Screen failures (n=4701)
• MD decision 544
• Failed incl/excl 4155
• Reasons not given 2
Number of patients who died
(n=5)
Number of patients who died
(n=4)
Patient Population
Number of patients screened (n=6585)
Number of patients who completed the study (n=913)
Number of patients who completed the study (n=891)
Randomized to placebo (n=950) Randomized to dalteparin (n=934)
Number of patients enrolled (n=1884)

51
Patient Characteristics
Characteristic No Bridging(N=950)
Bridging(N=934)
Age, yr 71.8±8.74 71.6±8.88
Male sex, no. (%) 696 (73.3) 686 (73.4)
Race, no. (%)
White 860 (90.5) 849 (90.9)
Nonwhite 88 (9.3) 82 (8.8)
Unknown 2 (0.2) 3 (0.3)
Weight, kg 96.2±24.87 95.4±23.50
CHADS2 score
Mean 2.3±1.03 2.4±1.07
Distribution, no. (%)
0 1 (0.1) 1 (0.1)
1 216 (22.7) 212 (22.7)
2 382 (40.2) 351 (37.6)
3 229 (24.1) 232 (24.8)
4 96 (10.1) 106 (11.3)
5 23 (2.4) 27 (2.9)
6 3 (0.3) 5 (0.5)
CharacteristicNo Bridging
(N=950)Bridging(N=934)
CHF or left ventricular dysfunction, no. (%)
289 (30.4) 310 (33.2)
Hypertension, no. (%) 833 (87.7) 806 (86.3)
Diabetes mellitus, no. (%) 390 (41.1) 382 (40.9)
Stroke, no. (%) 79 (8.3) 99 (10.6)
TIA, no. (%) 79 (8.3) 77 (8.2)
Mitral valve disease, no. (%)
165 (17.4) 142 (15.2)
Stenosis 19 (2.0) 10 (1.1)
Regurgitation 142 (14.9) 133 (14.2)
Prolapse 13 (1.4) 5 (0.5)
Laboratory values
INR 2.4±0.57 2.4±0.57
Creatinine clearance, mL/min
88.1±39.50 87.6±40.14
Patient Characteristics

52
Surgeries andProcedures*
Surgery/Procedure Type
No Bridging Bridging
Minor, no. (%) (n=781) (n=758)
Gastrointestinal 391 (50.1) 357 (47.1)
Cardiothoracic 139 (17.8) 151 (19.9)
Orthopedic 54 (6.9) 47 (6.2)
Urologic 41 (5.3) 45 (5.9)
Other 156 (19.9) 158 (20.9)
Major, no. (%) (n=94) (n=89)
Orthopedic 29 (30.9) 29 (32.6)
Urologic 26 (27.7) 20 (22.5)
General surgery 16 (17.0) 14 (15.7)
Other 23 (24.5) 26 (29.2)
* Initial classification of surgery/procedure was not always aligned to post-procedure bleeding risk designation
Perioperative Anticoagulant Management
VariableNo Bridging
(N=950)Bridging(N=934)
P Value
Warfarin treatment
Preprocedure time not taking warfarin
Patients with data, no. 872 8390.28
Mean, days 5.2±1.4 5.3±1.8
Time to first postprocedurewarfarin dose
Patients with data, no. 735 6960.40
Mean, days 1.5 (1.3) 1.4 (1.0)
Aspirin treatment, no./total no. (%)
Interruption ≥7 days before procedure 92/324 (28.4) 92/329 (28.0)
0.53Interruption <7 days before procedure 41/324 (12.7) 33/329 (10.0)
No interruption 191/324 (59.0) 204/329 (62.0)

53
Perioperative Anticoagulant Management
VariableNo Bridging
(N=950)Bridging(N=934)
P Value
LMWH or placebo
Preprocedure dosePatients with data, no. 796 768
0.61Mean no. of doses 5.0±0.7 5.0±1.4
Patients in whom last dose was taken on the morning of the day before the procedure, no./total no.
778/796 (97.7) 734/768 (95.6) 0.01
Time to first postprocedure dose
Major surgery/procedure (high bleeding risk)
Patients with data, no. 235 2230.74
Mean, hr 53.3±31.6 51.3±27.9
Minor surgery/procedure (low bleeding risk)
Patients with data, no. 526 4970.74
Mean, hr 21.1±2.3 21.0±2.4
Postprocedure dosesPatients with data, no. 764 721
0.47Mean no. of doses 15.7±7.4 16.1±8.4
Primary Outcomes
OutcomeNo. (%)
No Bridging(N=918)
Bridging(N=895) P Value
ATE 4 (0.4) 3 (0.3)0.01 (non-inf)
0.73 (sup)
Stroke 2 (0.2) 3 (0.3)
TIA 2 (0.2) 0 (0)
Systemic embolism 0 (0) 0 (0)
Major bleeding 12 (1.3) 29 (3.2) 0.005 (sup)
* The mean CHADS2 score in patients who sustained a thromboembolic event was 2.6 (range, 1-4) The median time to an arterial thromboembolic event was 19.0 days (IQR, 6.0-23.0 days)The median time to a major bleeding event after a procedure was 7.0 days (IQR, 4.0-18.0 days)

54
Secondary Outcomes
OutcomeNo. (%)
No Bridging(N=918)
Bridging(N=895) P Value
Death 5 (0.5) 4 (0.4) 0.88 (sup)
Myocardial infarction 7 (0.8) 14 (1.6) 0.10 (sup)
Deep vein thrombosis 0 (0) 1 (0.1) 0.25 (sup)
Pulmonary embolism 0 (0) 1 (0.1) 0.25 (sup)
Minor bleeding 110 (12.0) 187 (20.9) <0.001 (sup)
Limitations
• Few patients had a high CHADS2 score (e.g., 5–6)
• Most patients underwent low-risk procedures, such as colonoscopy or ambulatory surgery
• Overall rate of ATE was lower than initial projections
• Findings should not be applied to patients with mechanical heart valves or venous thromboembolism
• Findings are not applicable to patients with AF treated with a direct oral anticoagulant

55
Conclusions
• For patients with AF who require temporary interruption of warfarin treatment for an elective operation or invasive procedure, a strategy of forgoing bridging anticoagulation was non-inferior to perioperative bridging with LMWH for prevention of arterial thromboembolism
• Forgoing bridging treatment also decreased the risk of major bleeding compared to perioperative bridging with LMWH
Conclusions
• Patients on DOACs require an individualized custom tailored approach during the perioperative period
• Timing of preoperative cessation for DOACs based on elimination half-life
• Patients with Atrial fibrillation and CHADS 2 < 4 are at increased risk of bleeding when using full dose LMWH for bridging
• Discussion of perioperative anticoagulation strategy with patient, anesthesiologist and surgeon is key

56
Questions





























