Embed Size (px)
Citation preview

ia
Oncology
Outcomes and ClinicopathologicVariables Associated With LateRecurrence After Nephrectomyfor Localized Renal Cell CarcinomaSimon P. Kim, Christopher J. Weight, Bradley C. Leibovich, R. Houston Thompson,Brian A. Costello, John C. Cheville, Christine M. Lohse, and Stephen A. Boorjian
OBJECTIVE To characterize the incidence and clinicopathologic factors associated with late recurrence aftersurgical resection for renal cell carcinoma (RCC) because the recurrence patterns �5 years afternephrectomy have been poorly described.
METHODS We identified 1454 patients treated with nephrectomy for localized RCC from 1970 to 2000 whohad remained free of disease for 5 years. Subsequent tumor recurrence was classified as renalrecurrence and distant metastasis. The incidence of recurrence �5 years from surgery wasestimated using the Kaplan-Meier method. The associations of clinicopathologic variables withlate recurrence were analyzed using Cox proportional hazard regression models.
RESULTS With a median postoperative follow-up of 13.9 years (range 5.1-38.9), 63 patients (4.3%)experienced late renal recurrence at a median of 9.3 years (range 5.1-25.3), and 172 patients(11.8%) developed late distant metastases at a median of 9.6 years (range 5.1-26.6) after surgery.The estimated recurrence-free survival rate at 10 and 15 years was 97.3% and 95.2% for renalrecurrence, and 93.1% and 85.9% for distant metastases, respectively. On multivariate analysis,increased tumor size (hazard ratio [HR] 1.12; P � .001) was associated with late renal tumorrecurrence, and increased tumor size (HR 1.07; P � .018), clear cell or collecting duct histologicfeatures (HR 3.76; P � .001), and tumor Stage pT1b (HR 2.8; P � .001), pT2a (HR 4.5; P �.001), pT2b (HR 3.4; P � .007), and pT3-pT4 (HR 5.1; P � .001) were associated with distantmetastasis.
CONCLUSION After an initial 5-year postoperative disease-free interval, approximately 5% and 15% of patientswill develop renal recurrence and distant metastases, respectively, during the next decade.Therefore, long-term surveillance remains necessary after nephrectomy. UROLOGY 78:
1101–1106, 2011. © 2011 Elsevier Inc.The annual incidence of renal cell carcinoma(RCC) has been increasing during the past 2decades.1,2 In 2010, it was estimated that 58 240
ncident cases were diagnosed and 8210 deaths werettributable to RCC in the United States.3 The increased
use of cross-sectional imaging and the concurrent down-ward migration in clinical stage and primary tumor sizehave resulted in most incident cases now presenting assmall incidental renal masses, for which the 5-year sur-vival rates after surgical resection have been excellent.4-6
Funding Support: Healthcare Delivery Research Scholars Program, Mayo Clinic,Rochester, Minnesota
From the Departments of Urology, Oncology, and Pathology, and Health SciencesResearch, Mayo Clinic, Rochester, Minnesota
Reprint requests: Stephen A. Boorjian, M.D., Department of Urology, Mayo Clinic,200 First Street Southwest, Rochester, MN 55905. E-mail: Boorjian.Stephen@
mayo.eduSubmitted: January 24, 2011, accepted (with revisions): May 10, 2011
© 2011 Elsevier Inc.All Rights Reserved
Nevertheless, although surgical extirpation remains thereference standard for the treatment of localized renaltumors, approximately 30%-40% of patients with organ-confined RCC will experience local or distant recurrenceafter surgery.7-9
Characterizing the timing and patterns of RCC recur-rence after nephrectomy is critical for patient counseling,the development of evidence-based surveillance proto-cols, and the appropriate selection of patients for adju-vant therapy. As such, predictive models have been de-veloped and validated to assess the risk of diseaserecurrence and cancer-related mortality after radicalnephrectomy (RN) and nephron-sparing surgery(NSS).10-18 However, because most patients who expe-rience disease relapse do so within 3 years after nephrec-tomy for intermediate- or high-risk localized RCC, theincidence and clinicopathologic factors associated with
late RCC recurrence are poorly characterized.18,19 Thus,0090-4295/11/$36.00 1101doi:10.1016/j.urology.2011.05.012

we sought to determine the patterns of recurrence �5years after RN or NSS for localized RCC and to identifythe clinicopathologic factors associated with late recur-rence.
MATERIAL AND METHODS
After institutional review board approval, we identified 2228patients who had been treated with RN or NSS for unilateral,sporadic, Stage pNx-pN0M0 RCC from 1970 to 2000 using theMayo Clinic Nephrectomy Registry. Of these, 774 patients(34.7%), who had experienced local ipsilateral/contralateralrenal recurrence or distant metastases within 5 years of surgery,who had died within 5 years of surgery, or who were lost tofollow-up within 5 years of surgery were excluded, leaving 1454patients (65.3%) in our analytic cohort.
The clinical features studied included age at surgery, sex,symptoms at diagnosis, initial serum creatinine and glomerularfiltration rate (calculated using the abbreviated Modification ofDiet and Renal Disease equation), Eastern Cooperative Oncol-ogy Group performance status at surgery, Charlson score atsurgery, and surgery type (RN vs NSS). Patients with a palpablemass, abdominal discomfort, gross hematuria, acute-onset vari-cocele, or constitutional symptoms, including rash, sweats,weight loss, fatigue, early satiety, or anorexia, were consideredsymptomatic at diagnosis. The pathologic features studied in-cluded tumor size, the 2010 primary tumor classification, histo-logic subtype, nuclear grade, coagulative tumor necrosis, andsarcomatoid differentiation.20 A single urologic pathologist(J.C.C.) reviewed the microscopic slides from all tumor speci-mens to determine these pathologic features.
Tumor recurrence was recorded and classified as renal (ipsi-lateral or contralateral kidney or renal fossa) or distant (allother sites) metastases. The duration of follow-up was calcu-lated from the date of surgery to the date of recurrence for thosepatients who experienced disease relapse or to the date of deathor last follow-up otherwise. The disease status and vital statusfor patients in the Mayo Clinic Nephrectomy Registry areupdated yearly through a review of the medical records andcorrespondence with patients and their local physicians.
Recurrence-free survival, cancer-specific survival (CSS), andoverall survival (OS) were estimated using the Kaplan-Meiermethod. Univariate and multivariate associations with outcomewere evaluated using Cox proportional hazards regression mod-els and summarized with hazard ratios and 95% confidenceintervals (CIs). Multivariate models were developed using astepwise selection procedure, with the P value for a feature toenter or leave the model set to .05. Because many of the featuresstudied changed during the study period, particularly the symp-toms at diagnosis and surgery type, the surgery year group wasused as a stratification effect in the Cox models. Year groupswere chosen so that they contained approximately the samenumber of patients with the outcome of interest. Statisticalanalyses were performed using the SAS software package (SASInstitute, Cary, NC). All tests were 2-sided and P � .05 wasconsidered statistically significant.
RESULTSThe clinical and pathologic features of the cohort studiedare summarized in Table 1. The mean age was 61.5 years
(range 21-92), the mean preoperative serum creatinine1102
was 1.2 mg/dL (range 0.3-14.0), and the mean primarytumor size was 5.7 cm (range 0.2-24.0). A total of 777patients (53.4%) had died at a median of 11.6 years aftersurgery (range 5.1-37.0). For the 677 patients (46.4%)still alive at the last follow-up visit, the median durationof follow-up was 13.9 years (range 5.1-38.9).
A total of 63 patients (4.3%) developed late renaltumor recurrence at a median of 9.3 years (range 5.1-25.3) after nephrectomy. The most common sites werethe contralateral kidney (n � 42) followed by the renalfossa (n � 8) and ipsilateral kidney (n � 5). The esti-mated renal recurrence-free survival rate for these pa-tients with an initial 5-year postoperative disease-free
Table 1. Patient clinical and pathologic features
Feature Patients (n)
SexFemale 487 (33)Male 967 (67)
Symptoms at diagnosis(n � 1450)
877 (60)
Constitutional symptoms atdiagnosis (n � 1450)
300 (21)
Solitary kidney 32 (2)ECOG at surgery
(n � 1037)0 953 (92)�0 84 (8)
Charlson score at surgery(n � 1033)
0 554 (54)�0 479 (46)
Surgery typeOpen radical 1185 (82)Open nephron-sparing 256 (18)Laparoscopic radical 8 (�1)Laparoscopic nephron-
sparing5 (�1)
2010 Primary tumorclassification
pT1a 576 (40)pT1b 418 (29)pT2a 176 (12)pT2b 81 (6)pT3a 170 (12)pT3b 27 (2)pT3c 3 (�1)pT4 3 (�1)
Histologic subtypeClear cell RCC 1106 (76)Papillary RCC 256 (18)Chromophobe RCC 84 (6)Collecting duct RCC 1 (�1)RCC, NOS 7 (�1)
Nuclear grade1 186 (13)2 878 (60)3 371 (26)4 19 (1)
Coagulative tumor necrosis 267 (18)Sarcomatoid differentiation 9 (�1)
ECOG, Eastern Cooperative Oncology Group; RCC, renal cell car-cinoma; NOS, not otherwise specified.
Data in parentheses are percentages.
interval was 99% (95% CI 99%-100%; number still at
UROLOGY 78 (5), 2011

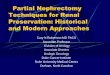
risk 1388), 97% (95%% CI 96%-98%; number still at risk1012), and 95% (95% CI 94%-97%; number still at risk514) at 6, 10, and 15 years after nephrectomy, respec-tively (Fig. 1). The univariate associations with late renalrecurrence and distant metastasis are summarized in Ta-ble 2. After adjusting for tumor size, no other clinico-pathologic feature was significantly associated with anincreased risk of late renal recurrence. Specifically, each1-cm increase in tumor size was associated with a 12%increased risk of late renal recurrence (hazard ratio 1.12;95% CI 1.05-1.19; P � .001).
Of the patients who experienced late renal recurrence,33 (52.4%) had died at a median of 2.8 years (range0.0-10.6) after recurrence, including 23 (36.5%) whodied of RCC. Thirty patients (47.6%) were still alive atthe last follow-up visit, with a median duration fromrecurrence to the last follow-up visit of 5.4 years (range0.2-19.3). The estimated CSS rate at 1, 5, and 10 yearsafter renal recurrence was 87% (95% CI 79%-96%; num-ber still at risk 51), 66% (95% CI 54%-81%; number stillat risk 25), and 50% (95% CI 36%-69%; number still atrisk 11), respectively. The estimated OS after renal re-currence at 1, 5, and 10 years was 86% (95% CI 77%-95%; number still at risk 51), 56% (95% CI 45%-72%;number still at risk 25), and 36% (95% CI 24%-53%;number still at risk 11), respectively.
A total of 172 patients (11.8%) developed late distantmetastases �5 years (median 9.6, range 5.1-26.6) afternephrectomy. The estimated late distant metastasis-freesurvival rate at 6, 10, and 15 years after nephrectomy was99% (95% CI 98%-99%; number still at risk 1381), 93%(95% CI 92%-96%; number still at risk 994), and 86%(95% CI 84%-88%; number still at risk 498), respectively(Fig. 1). Although the most common site of solitarydistant metastases was the lung (n � 59) followed bybone (n � 18), pancreas (n � 13), brain (n � 8), andadrenal glands (n � 7), another 22 patients who devel-oped late distant metastasis in the lung also presented
Figure 1. Late renal recurrence-free survival and distantmetastasis-free survival for patients with initial 5-year post-operative disease-free interval after nephrectomy.
with a synchronous metastatic lesion to other organ sites.
UROLOGY 78 (5), 2011
Tumor size, the 2010 primary tumor classification, andhistologic subtype were significantly associated with latedistant metastases on multivariate analysis (Table 3). Inparticular, each 1-cm increase in tumor size was associ-ated with a 7% increased risk of late distant metastases(hazard ratio 1.07; P � .018), and patients with 2010Stage pT1b, pT2a, pT2b, or pT3-pT4 tumors were 2.8 (P� .001), 4.5 (P � .001), 3.4 (P � .007), and 5.1 (P �.001) times more likely to develop late distant metastasesthan were patients with Stage pT1a, respectively. More-over, patients with clear cell RCC, collecting duct RCC,or RCC not otherwise specified were 4.0 times morelikely to develop late distant metastases than were pa-tients with papillary or chromophobe RCC (P � .001).Although patients who underwent RN were more likelyto experience late distant metastasis on univariate anal-ysis, this difference was not seen after adjusting for tumorsize, primary tumor classification, and histologic subtype.
Of the patients who experienced distant metastases,135 (78.5%) had died at a median of 1.4 years (range0.0-14.5) after metastases, including 113 (65.7%) whodied of RCC. Thirty-seven patients (21.5%) were stillalive at the last follow-up visit, with a median durationfrom metastases to the last follow-up visit of 4.1 years(range 0.2-16.7). The estimated CSS rate at 1, 5, and 10years after the development of distant metastases was69% (95% CI 62%-76%; number still at risk 112), 35%(95% CI 28%-44%; number still at risk 33), and 20%(95% CI 13%-30%; number still at risk 8), respectively.The estimated OS at 1, 5, and 10 years after the devel-opment of distant metastases was 67% (95% CI 61%-75%; number still at risk 112), 27% (95% CI 21%-35%;number still at risk 33), and 15% (95% CI 9%-23%;number still at risk 8), respectively.
COMMENTWe found that even those patients who experienced aninitial 5-year recurrence-free interval after RN or NSS forlocalized RCC were at continued risk of late tumor re-currence, both in the remaining renal units and at distantsites. Specifically, we noted that 15% of these patientswill develop distant metastasis during the ensuing 10years, most commonly in the lung. We also determinedthat the clinicopathologic characteristics at presentationassociated with late renal recurrence and distant metas-tasis on multivariate analysis included tumor size, primarytumor stage, and histologic subtype. Our results are sim-ilar to the data from 2 recent single-institution series,which also noted a late recurrence rate of 6%-20% afternephrectomy for RCC and found that most recurrenceswere distant rather than local.21,22
Our results provide important information about the in-creasing risks of late recurrence and could help guide thedevelopment of extended postoperative surveillance proto-cols for patients with RCC after nephrectomy. Several stud-ies to date have outlined follow-up regimens with varying
degrees of intensity, although none have included recom-1103

isof
c
pare
mendations for �10 years after nephrectomy.9-12,16-19,23,24
For example, the Kattan nomogram reports a predictive
Table 2. Univariate analysis of factors associated with lmetastasis after nephrectomy
Feature Renal Recurren
Age at surgery (10-y increase) 1.10 (0.88-1.37Sex
Female 1.0 (ReferenceMale 1.22 (0.71-2.09
Symptoms at diagnosis 0.68 (0.41-1.12Solitary kidney NASerum creatinine at diagnosis
(1-unit increase)1.07 (0.77-1.47
GFR at diagnosis (10-unit increase) 0.89 (0.77-1.03ECOG at surgery
0 1.0 (Reference�0 1.10 (0.34-3.54
Charlson score at surgery0 1.0 (Reference�0 0.78 (0.44-1.38
Surgery typeNephron-sparing 1.0 (ReferenceRadical 1.37 (0.66-2.84
Tumor size (1-cm increase) 1.12 (1.05-1.192010 Primary tumor classification
pT1a 1.0 (ReferencepT1b 1.68 (0.84-3.38pT2a 2.66 (1.24-5.71pT2b 2.60 (0.94-7.17pT3a 2.83 (1.28-6.25pT3b, pT2c, pT4 4.21 (1.22-14.5
Histologic subtypePapillary, chromophobe 1.0 (ReferenceClear cell, collecting duct, NOS 1.05 (0.58-1.87
Nuclear grade1, 2 1.0 (Reference3, 4 1.08 (0.61-1.88
Coagulative tumor necrosis 0.37 (0.15-0.91Sarcomatoid differentiation NA
NA, not available (hazard ratio could not be estimated because nometastases; GFR, glomerular filtration rate; other abbreviations a
Data presented as hazard ratio, with 95% confidence interval in* Log-rank test.
Table 3. Multivariate analysis of factors associated withlate distant metastasis after nephrectomy for localizedRCC
Feature HR (95% CI) P Value
Tumor size (1-cm increase) 1.07 (1.01-1.14) .0182010 Primary tumor
classificationpT1a 1.0 (Reference) —pT1b 2.81 (1.61-4.91) �.001pT2a 4.45 (2.34-8.47) �.001pT2b 3.38 (1.39-8.23) .007pT3a, pT3b, pT2c, pT4 5.09 (2.68-9.67) �.001
Histologic subtype �.001Papillary, chromophobe 1.0 (Reference)Clear cell, collecting
duct, NOS3.76 (2.12-6.66)
HR, hazard ratio; CI, confidence interval; other abbreviations as inTable 1.
model for any type of recurrence (local or distant) in the first c
1104
5 years after nephrectomy.12 Other series studies have de-scribed multifactorial models according to the risk of devel-oping recurrence in varying sites (eg, abdomen, chest, bone,and brain), using the histologic findings as a guide fortailoring surveillance according to risk stratification.9,11,23
Again, however, the surveillance recommendations weredetailed for �10 years after surgery. Likewise, Lam et al24
used the University of California-Los Angeles IntegratedStaging System to risk stratify patients into 3 groups ofrecurrence at 9 years of follow-up.
Our results, documenting the continued renal and distanttumor recurrence for �15 years after nephrectomy after annitial 5-year disease-free interval, suggest that long-termurveillance in some capacity should continue. We previ-usly reported that CSS improves for patients as the disease-ree interval after surgery increases.25 Nevertheless, the sur-
vival for patients who develop metastatic RCC, althoughimproving with targeted therapies, remains relatively lim-ited.26 A potential benefit to extended surveillance in RCCould be the earlier detection of recurrence, allowing for
renal recurrence (ipsilateral or contralateral) and distant
P Value* Distant Metastasis P Value*
.42 1.13 (0.99-1.29) .08
.47 .771.0 (Reference)
0.95 (0.70-1.31).12 1.64 (1.17-2.31) .005.26 1.82 (0.81-4.13) .15.69 0.98 (0.74-1.30) .87
.13 0.94 (0.86-1.02) .15
.88 .461.0 (Reference)
1.28 (0.67-2.44).39 .032
1.0 (Reference)0.69 (0.49-0.97)
.40 �.0011.0 (Reference)
3.08 (1.61-5.88)�.001 1.16 (1.12-1.20) �.001
— 1.0 (Reference) —.15 3.47 (2.03-5.94) �.001.012 6.42 (3.70-11.14) �.001.07 6.20 (3.15-12.22) �.001.010 9.40 (5.51-16.05) �.001.023 4.57 (1.55-13.43) .006.88 �.001
1.0 (Reference)4.00 (2.27-7.05)
.80 �.0011.0 (Reference)
1.87 (1.36-2.56).031 1.23 (0.85-1.77) .27.52 1.67 (0.41-6.77) .47
nt with feature listed experienced late renal recurrence or distantable 1.ntheses.
ate
ce
)
)))
)
)
))
))
)))
)))))6)
))
)))
paties in T
onsideration of surgical resection. Surgical resection of
UROLOGY 78 (5), 2011

osgfptfpfathcorretpf
RCC metastasis has been associated with improved survivalamong patients with advanced disease and represents theonly reasonable potential for long-term cure.27,28 Thus, al-though the optimal surveillance regimen after surgery forRCC has not been defined, and the associations betweenthe intensity of RCC surveillance and improved survivalhave not been established, it is plausible that early identi-fication of RCC recurrence could facilitate improved out-comes.
The interpretations of the results of our study have sev-eral limitations. First, inferences from the results of our studywere limited by the retrospective and single-institutionstudy design. Second, as a tertiary referral center, completefollow-up data for the patients in this cohort cannot beensured. Third, we acknowledge that the etiology of the laterenal recurrence in the ipsilateral or contralateral kidney, asclassified in the present study, might, in fact, have repre-sented a second primary tumor, not metastasis from theinitial lesion.29 Fourth, although defining a long-term post-perative surveillance protocol was not the intent of ourtudy, patients with the risk factors of larger renal tumor size,reater primary tumor stage, and adverse histologic subtypeor late recurrence could potentially be used to stratifyatients to higher intensity postoperative surveillance pro-ocols. Additional studies are needed to validate the riskactors for late recurrence after nephrectomy. Fifth, in theresent cohort of patients treated with RN or NSS for RCCrom 1970 to 2000, no patient received adjuvant treatmentfter surgery. Data regarding the potential effect of adjuvantherapy, in particular with targeted agents, for patients withigh-risk localized RCC, will be forthcoming from recentlyompleted, as well as active, ongoing clinical trials. Finally,ur study did not assess the effects of late renal and distantecurrence on CSS and OS in a multivariate model. Aetrospective multi-institution study noted that PN or RNliminated the risk of cancer-specific mortality, althoughhat study was limited by the inclusion of Stage pT1a andT1b renal tumors only and by a shorter mean postoperativeollow-up (just �3 years).30
Nevertheless, we found in the present study that patientsundergoing surgery for localized RCC remain at long-termrisk of disease recurrence. That is, even for those patientswho experience an initial 5-year postoperative disease-freeinterval, approximately 5% will experience renal recurrenceand 15% will develop distant metastases during the ensuingdecade. Although continued investigation to identify po-tential site-specific risk factors for late recurrence is neededto guide postoperative surveillance regimens, patientsshould be counseled regarding the continued need for long-term surveillance after nephrectomy.
CONCLUSIONSAfter an initial 5-year postoperative disease-free interval,approximately 5% and 15% of patients will develop renalrecurrence and distant metastases, respectively, duringthe ensuing 10 years. Primary tumor size, stage, and
histologic subtype were associated with late recurrence.UROLOGY 78 (5), 2011
Although continued investigation to identify potentialsite-specific risk factors for late recurrence is needed toguide postoperative surveillance regimens, patientsshould be counseled regarding the continued need forlong-term surveillance after RN or NSS for localizedRCC.
References1. Chow WH, Devesa SS, Warren JL, Fraumeni JF. Rising incidence
of renal cell cancer in the United States. JAMA. 1999;281:1628-1631.
2. Hollingsworth JM, Miller DC, Daignault S, Hollenbeck BK. Risingincidence of small renal masses: a need to reassess treatment effect.J Natl Cancer Inst. 2006;98:1331-1334.
3. Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA CancerJ Clin. 2010;60:277-300.
4. Bhargavan M, Sunshine JH. Utilization of radiology services in theUnited States: levels and trends in modalities, regions, and popu-lations. Radiology. 2005;234:824-832.
5. Jayson M, Sanders H. Increased incidence of serendipitously dis-covered renal cell carcinoma. Urology. 1998;51:203-205.
6. Kane CJ, Mallin K, Ritchey J, Cooperberg MR, Carroll PR. Renalcell cancer stage migration: analysis of the National Cancer DataBase. Cancer. 2008;113:78-83.
7. Hollingsworth JM, Miller DC, Daignault S, Hollenbeck BK. Five-year survival after surgical treatment for kidney cancer: a popula-tion-based competing risk analysis. Cancer. 2007;109:1763-1768.
8. Nguyen MM, Gill IS, Ellison LM. The evolving presentation ofrenal carcinoma in the United States: trends from the Surveillance,Epidemiology, and End Results program. J Urol. 2006;176:2397-2400.
9. Frank I, Blute ML, Cheville JC, et al. A multifactorial postopera-tive surveillance model for patients with surgically treated clear cellrenal cell carcinoma. J Urol. 2003;170:2225-2232.
10. Frank I, Blute ML, Cheville JC, et al. An outcome predictionmodel for patients with clear cell renal cell carcinoma treated withradical nephrectomy based on tumor stage, size, grade and necrosis:the SSIGN score. J Urol. 2002;168:2395-2400.
11. Frank I, Zincke H. Prediction of site-specific metastases in surgi-cally treated nonmetastatic renal cell cancer. Changes of follow-upprotocol. Urologe A. 2004;43(suppl 3):S125-S128.
12. Kattan MW, Reuter V, Motzer RJ, Katz J, Russo P. A postoperativeprognostic nomogram for renal cell carcinoma. J Urol. 2001;166:63-67.
13. Leibovich BC, Blute ML, Cheville JC, et al. Prediction of progres-sion after radical nephrectomy for patients with clear cell renal cellcarcinoma: a stratification tool for prospective clinical trials. Can-cer. 2003;97:1663-1671.
14. Motzer RJ, Mazumdar M, Bacik J, et al. Survival and prognosticstratification of 670 patients with advanced renal cell carcinoma.J Clin Oncol. 1999;17:2530-2540.
15. Sorbellini M, Kattan MW, Snyder ME, et al. A postoperativeprognostic nomogram predicting recurrence for patients with con-ventional clear cell renal cell carcinoma. J Urol. 2005;173:48-51.
16. Zisman A, Pantuck AJ, Dorey F, et al. Improved prognostication ofrenal cell carcinoma using an integrated staging system. J ClinOncol. 2001;19:1649-1657.
17. Zisman A, Pantuck AJ, Figlin RA, Belldegrun AS. Validation ofthe UCLA integrated staging system for patients with renal cellcarcinoma. J Clin Oncol. 2001;19:3792-3793.
18. Zisman A, Pantuck AJ, Wieder J, et al. Risk group assessment andclinical outcome algorithm to predict the natural history of patientswith surgically resected renal cell carcinoma. J Clin Oncol. 2002;20:4559-4566.
19. Eggener SE, Yossepowitch O, Pettus JA, et al. Renal cell carcinomarecurrence after nephrectomy for localized disease: predicting sur-
vival from time of recurrence. J Clin Oncol. 2006;24:3101-3106.1105

2
2
2
20. Edge SB, Byrd DR, Compton CC, et al. AJCC Cancer StagingManual, 7th ed. New York: 2010.
21. Adamy A, Chong KT, Chade D, et al. Clinical characteristics andoutcomes of patients with recurrence 5 years after nephrectomy forlocalized renal cell carcinoma. J Urol. 2011;185:433-438.
2. Miyao N, Naito S, Ozono S, et al. Late recurrence of renal cellcarcinoma: retrospective and collaborative study of the JapaneseSociety of Renal Cancer. Urology. 2011;77:379-384.
3. Siddiqui SA, Frank I, Cheville JC, et al. Postoperative surveillancefor renal cell carcinoma: a multifactorial histological subtype spe-cific protocol. BJU Int. 2009;104:778-785.
4. Lam JS, Shvarts O, Leppert JT, et al. Postoperative surveillanceprotocol for patients with localized and locally advanced renal cellcarcinoma based on a validated prognostic nomogram and riskgroup stratification system. J Urol. 2005;174:466-472; quiz: 801.
25. Thompson RH, Leibovich BC, Lohse CM, et al. Dynamic outcomeprediction in patients with clear cell renal cell carcinoma treated with
radical nephrectomy: the D-SSIGN score. J Urol. 2007;177:477-480.1106
26. Motzer RJ, Hutson TE, Tomczak P, et al. Overall survival andupdated results for sunitinib compared with interferon alfa inpatients with metastatic renal cell carcinoma. J Clin Oncol. 2009;27:3584-3590.
27. Boorjian SA, Crispen PL, Lohse CM, Leibovich BC, Blute ML.Surgical resection of isolated retroperitoneal lymph node recur-rence of renal cell carcinoma following nephrectomy. J Urol. 2008;180:99-103.
28. Alt AA, Boorjian SA, Lohse CM, et al. Survival after completesurgical resection of multiple metastases from renal cell carcinoma.Cancer. Epub Jan 10, 2011.
29. Boorjian SA, Crispen PL, Lohse CM, Leibovich BC, Blute ML.The impact of temporal presentation on clinical and pathologicaloutcomes for patients with sporadic bilateral renal masses. Eur Urol.2008;54:855-863.
30. Zini L, Patard JJ, Capitanio U, et al. Cancer-specific and non-cancer-related mortality rates in European patients with T1a and
T1b renal cell carcinoma. BJU Int. 2009;103:894-898.UROLOGY 78 (5), 2011