Embed Size (px)
Citation preview

Our senses provide us with wonderful capabilities. If you had to lose one, which would it be?
Neurological disorders take away sensation without a choice!
Chris Cohan, Ph.D.Dept. of Pathology/Anat SciUniversity at Buffalo
http://neuroscience.uth.tmc.edu/s2/chapter04.html

Objectives1. Describe the general characteristics of sensory pathways2. Understand the general organization and numbered areas of spinal cord
gray matter3. Understand dermatomes and be able to name them on the body surface.4. Understand the general characteristics of tactile sensory receptors.5. Understand how axon diameter relates to transmission of tactile
information.6. Describe the names and locations of the cell bodies and axons in the
pathway that transmits tactile information. Describe the cortical area involved.
7. Understand the concept of somatotopic orientation and describe it for tactile information at the level of the spinal cord, brainstem, and cortex.
8. Understand the term lesion and describe how lesions in the spinal cord, brainstem and cortex affect tactile sensibility.
9. Understand the effects of Tabes Dorsalis and use of Romberg test

What are we Doing• How is sensory info transmitted from body to brain?
Or when I poke you, why do you feel it
• How are neurons specialized to transmit sensory info?
• Where are the neurons that transmit tactile sensation?
• How do diseases impair sensory function/touch?

A 24-year-old man was brought to the ED after he was shot during an argument outside a bar. On exam, he had the following symptoms:
Sensation
R L
•Loss of touch, vibration senseand ability to tell position of his leg passively moved all on Left lower limb.•Tactile, vibration, position sense normal on Right•Pinprick sensation absent on Right lower limb but normal on Left.
•QUESTIONS: ••Which sensory systems involved
••Which areas of body affected.
••Why lost sensation on right and left
••Is there single location of damage (Lesion)

Body Sensation• Stimuli– touch, vibration, proprioception,
pain, temperature
• Sensory Receptors – modified nerve endings
Different types of neurons –specialized for different functions
How are stimuli transmitted to the brain:• encoding by receptor• pathway to brain
• types of neurons -specialized
• locations – injury effects
• synapses - processing

Somatosensory Systems
sensationmovement
perception
Overall Plan:
•Pathways for reflexes and perception
Reflexes - clinical tools to assess pathways
Perception - how we experience the world?
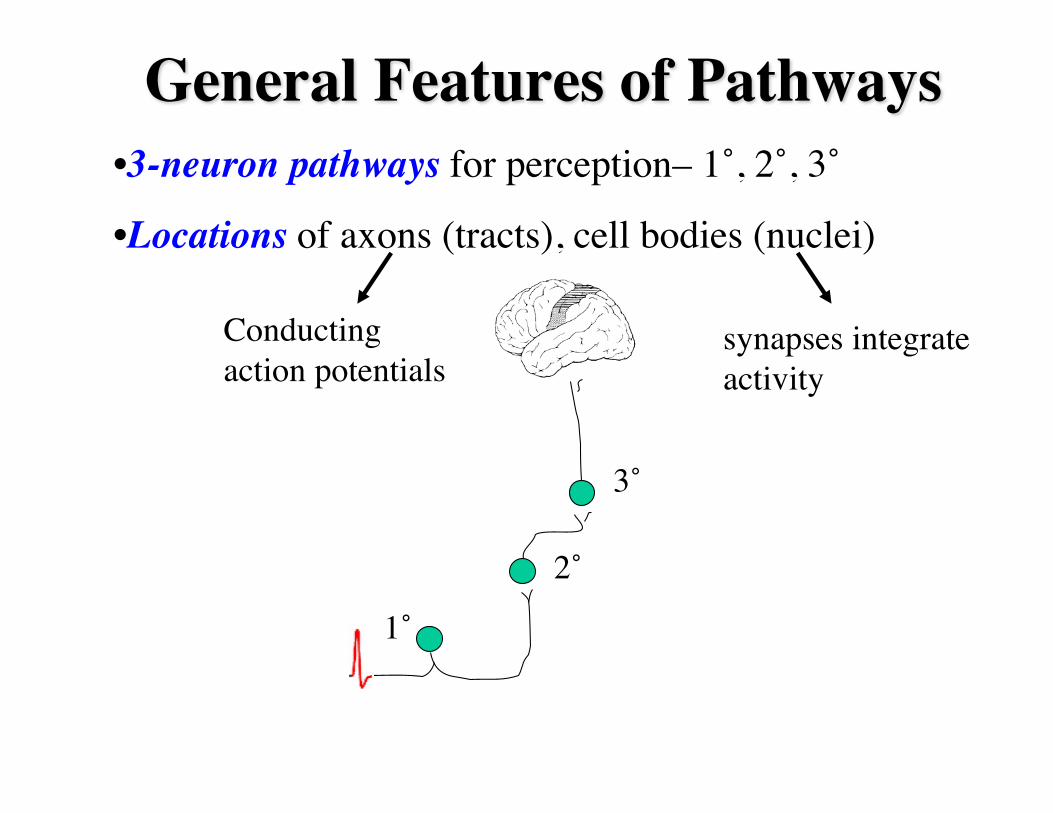
•3-neuron pathways for perception– 1˚, 2˚, 3˚
•Locations of axons (tracts), cell bodies (nuclei)
General Features of Pathways
1˚
2˚
3˚
synapses integrate activity
Conducting action potentials

•3-neuron pathways for perception– 1˚, 2˚, 3˚
•Locations of axons (tracts), cell bodies (nuclei)
General Features of Pathways
1˚
2˚
3˚
What happens when a pathway is damaged
The brain experiences the deficit as a loss from the side where the stimulus originated.

General Features of PathwaysCell Body Axon
1° Dorsal Root Ganglion Dorsal Root
2° Spinal cord or Brainstem CROSSES CNS
3° Thalamus Internal CapsuleSynapses in cortex
1˚
2˚
3˚
Download template from web site

Spinal Cord Laminae

DermatomesDefine the relationship between body regions and the spinal cord segment innervating them.

Tactile Sensation•Sensory Stimuli: light touch, vibration, pressure,
proprioception
•The different qualities are due to the different nerve endings that encode physical deformation.
We call it touch, but it really has many qualities!

Tactile Receptors• What are they - modified nerve endings!
• mechanoreceptors – cutaneousmuscleskeletal
•Mechanoreceptors in skin differ in:1. Morphology
2. Depth in skin
3. Axon properties

Tactile Receptors•Different properties of mechanoreceptors produce the basic sensations of touch.
•Collectively, these properties allow us to discriminate the tactile qualities of objects.
• This information eventually arrives at the cortex where features of the stimulus are analyzed and perceived.

Pathway Overview
thalamus
midbrain
medulla
ponsCell Body Axon
1° Dorsal Root Ganglion Dorsal Root2° Brainstem CROSSES CNS3° Thalamus Internal Capsule
Synapses in cortex
spinal cord
(VPL)
Dorsal root gang
nuc gracilis, nuc cuneatus

Diameter of First-Order Axons
An action potential traveling from my finger to my spinal cord (1 meter) would require 8 ms for the fastest axon and 100 ms for the slowest mechanoreceptor axon.
Nerve Fiber Grp Axondiameter
ConductionVelocity
Function
Group A(myelinated)
α 10-20µm 60-120m/sec mechanorecep
β 5-15 µm 30-90 m/sec mechanorecep
γ 3-10 µm 10-50 m/sec mechanorecep
δ 1-5 µm 6-30 m/sec nociceptors,thermal r.
Grp C-unmyelinated 0.5-2 µm 0.5-2 m/sec nociceptors,thermal r.

Reflex Pathways• As sensory info enters spinal cord,
it immediately is used for reflexes.
• Basis of stretch reflexes
•1° axons make local connections in spinal cord onto motoneurons.
The presence and magnitude of reflexes provide a clinical tool to assess pathways. 0, 1+, 2+, 3+, 4+

Pathway
nucleus gracilisnucleus cuneatus
medial lemniscus
VPL
fasciculus gracilis
fasciculus cuneatus
midbrain
caudal medulla
pons

Pathway
Fasciculus gracilis and fasciculus cuneatus travel the length of the spinal cord on its dorsal (posterior) surface on each side of the midline. Consequently, these tracts are often called collectively the dorsal columns.

Cortical Localization
•The 3º neuron terminates in the postcentral gyrus.
Paracentral lobule
Circle this
Lateral view Medial

Paracentral Lobule
The postcentral gyrus does not continue as a gyrus onto the medial surface of the hemisphere.
central sulcus

Somatotopic OrientationSPINAL CORD
Below T6-Lower body
only
Upper body
Above T6
Relationship between a part of the body and position in a pathway
FC
FG
FG
FGFG

Somatotopic OrientationBRAINSTEM – medial lemniscus
Upper bodyLower body
medulla pons

Somatotopic OrientationParacentral lobule
CORTEX
homonculus

Perception of the sensory stimulus occurs when activity reaches the cortex.
• You feel something touching your body. Postcentral gyrus analyzes simple tactile qualities: dull/sharp, light/heavy …
• Neighboring parietal cortex associates the stimulus with previous experiences (memory) to provide more complex features:
• stereognosis, graphesthesia, 2-point discrimination, etc.
Cortical Integration

• Damage to the Postcentral gyrus – loss of tactile sensation
• Damage to neighboring parietal cortex while postcentral gyrus is intact – the complex features are lost but tactile perception is retained (agnosia).
FEATURE DEFICIT (agnosia)
2-point discrimination loss of…Stereognosis AstereognosisGraphesthesia AgraphesthesiaDouble Simultaneous Stim Extinction on..
(Attention to stimulated area)
Loss of any of the complex features while tactile sensation is intact, indicates a (parietal) cortex lesion.
Cortical Integration
Sensation intact but inability to comprehend

Clinical Applications
LESION:•An area of localized dysfunction in the nervous system that may be caused by a variety of factors.
•Symptoms caused by lesion provide clues to its location in the nervous system.
tumor, trauma, infection, degenerative/metabolic/genetic disorder …

Clinical Applications•Tabes Dorsalis (advanced syphilis);
vitamin B12 deficiency
•Romberg Test• maintain balance - how(visual, tactile, vestibular info)
Vestibular system intactEyes closedBalance maintained by proprioception

1. Spinal cord2. Brainstem3. Thalamus4. Internal Capsule5. Postcentral gyrus
Level-Specific Deficits
Loss of tactile sense
Which side?
Parietal lobe damage may result in• Loss of 2 pt discrim• Astereognosis• Agraphesthesia• Extinction on double
simultaneous stimulationLabeled-line encoding:pathways are dedicated to specific sensory info.

Testing Intact PathwayOn returning home from shopping, a wife finds her 59 year-old husband unconscious on the floor. He has no pulse. After calling 911, she begins CPR. When Mr. T arrives in the ED, he is in ventricular fibrillation. Spontaneous circulation is eventually restored, but Mr. T remains comatose. After 3 days in coma, his wife asks about her husband’s condition and the probability of a good outcome.
• No clinical methods exist to assess cerebral cortex damage/function in unconscious patients.
• How can a physician assess the extent of CNS damage and chances for recovery?

Coma is caused by damage to the cerebral hemispheres and/or brainstem.
Brainstem involvement is much more serious condition and often life-threatening due to autonomic centers.
• Brainstem involvement can be assessed using knowledge of pathways and reflexes.
Testing Intact Pathway
1. Somatosensory Evoked Potential

A 24-year-old man was brought to the emergency room after he was shot during an argument outside a bar. On exam, he had the following symptoms:
•Loss of touch, vibration sense and ability to tell position of leg passively moved all in Left lower limb.
•Pinprick sensation absent in Right lower limb.
Case

•Which sensory systems were affected
•Why did he lose some senses on Leftside, but other senses on Right.
•What pathway
•Where is the damage (Lesion).
Case
R L

Check out tutorials on module web site:• Review tutorials – review each pathway and structure IDs.










![Welcome [] · UNIQUE BUILDING, WITH A SPECIAL CHARM THAT BREATHES ... your taste buds and awaken all your senses, while enjoying wonderful views over La Concha bay in](https://img.dokumen.tips/doc/110x75/5ae1253c7f8b9afd1a8eda65/welcome-building-with-a-special-charm-that-breathes-your-taste-buds-and.jpg)


















