Embed Size (px)
Citation preview

OUR NSQIP JOURNEY Drilling Down NSQIP Data
Nanaimo Regional General Hospital Kelli Jennison-Gustafson RN SCR CNE

NRGH
Acute Care Facility and Trauma Center 292 Beds
56 Surgical BedsBusiest ER on Vancouver Island
We employ over 1,700 individuals locally

In the beginning…
July 2011 1st day on the job – NSQIP conference in Boston
August 2011 Office set-up: get the word out to staff and surgeons
SCR training, “CPT and ICD-9 codes “ Sept 2011
Ramp-up: start of chart reviewing and data collection Goal: 40 charts per 8 day cycle


Benefits of Participation
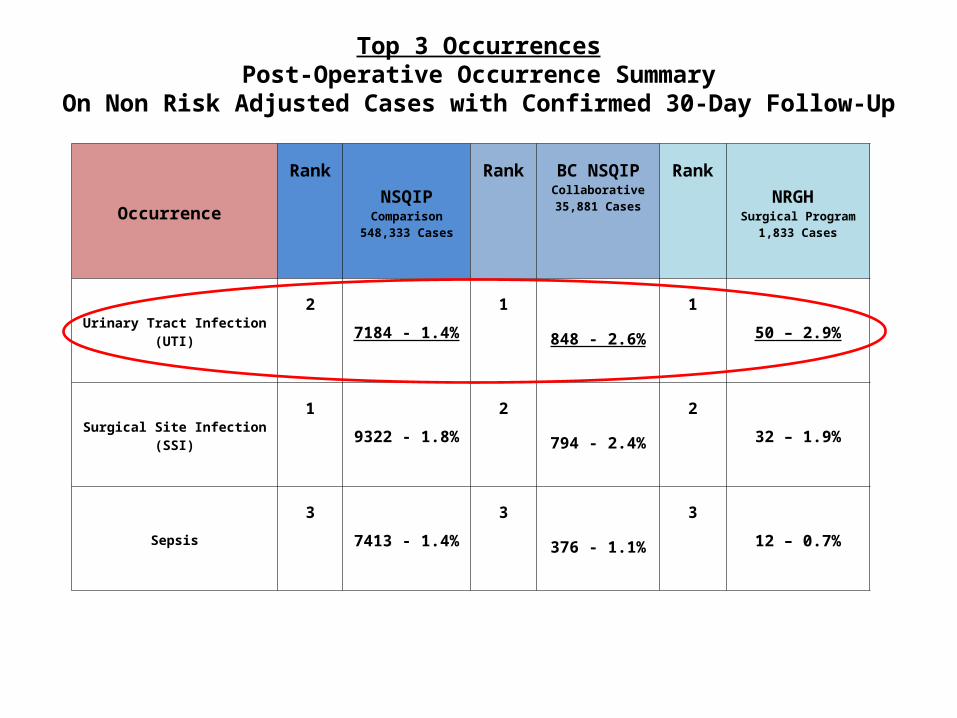
Occurrence
Rank
NSQIPComparison
548,333 Cases
Rank BC NSQIPCollaborative35,881 Cases
Rank
NRGH Surgical Program
1,833 Cases
Urinary Tract Infection(UTI)
2
7184 - 1.4%
1
848 - 2.6%
1
50 – 2.9%
Surgical Site Infection(SSI)
1
9322 - 1.8%
2
794 - 2.4%
2
32 – 1.9%
Sepsis
3
7413 - 1.4%
3
376 - 1.1%
3
12 – 0.7%
Top 3 OccurrencesPost-Operative Occurrence Summary
On Non Risk Adjusted Cases with Confirmed 30-Day Follow-Up


Patient ID sticker
Prevent the Bug Date (d/m/y): _______________ Initials (reviewer): ______________ MRN #: _______________ Postop Day: __________ Gender: M or F Reason for admit/Surgical Procedure: _________________________________________________________ Check all that apply: Type of Catheter: Foley Coude 3-way (CBI) Size: #12 #14 #16 #18 #_____ Statlock on? Yes No Drainage Bag? Name and date on <24 hr old >24 hr old Below the Bladder tubing free of loops Chart/Kardex; Catheter Inserted? Date: _____________________ Unit where inserted?_________________ # of attempts_________ Who inserted: (RN, DR, student?)________________________________________________ Pre Operatively Intraoperatively Post Operatively Reinserted x __________ Reason ______________________________________________ How many days has this catheter been in? 1 2 3 4 or more #?____________________ Date removed?___________ Is there a plan for removal? Yes, ________________________________________________________________________ No, _________________________________________________________________________ Epidural? Date removed?_____________________________________________________ More than 48 hours?______ Why?________________________________________________
Pre-Initiative Audit

NSQIP IDN: Case #: MRN:Sex:Age:Diabetes: Patients functional status pre-operatively:Did the patient have a catheter: Date inserted:Where was the catheter inserted: (ER, OR, Floor) Who inserted?( RN, student, resident)Documentation of insertion, was it a simple or complicated procedure?(# of attempts)What prep was used? (Poviodine or normal saline)Principal operation:Elective or emergency procedure:Was the patient transferred from another hospital?Surgeon:Temperature on admission to PARR:Did the patient have an epidural? Date Removed? PO day#?
Are there clinical orders sets for removal of Foley? (Ortho cases)What day was the Foley removed: If Foley remained in greater than 48 hours was there a reason:Type of catheter used:Is there documentation of patient symptoms of a UTI?What were the symptoms:Did the patient have a positive urinalysis or culture pre-operatively?If so, what organism was growing?Was there a positive urinalysis or culture post op:Type of bacteria growth in urine culture post op:Is there documentation of correct placement of drainage bag and tubing? Is there documentation of drainage bag changed every 24hours?Is the patient on antibiotics post op? Type of antibiotic and why?Was an antibiotic ordered prior to Foley removed?
Template for Drilling down UTI Cases

Reducing UTIsBack to Basics

Changes to be Implemented
• Nurse educationFoley Insertion Training + Regular skills assessment forCare providers
• Patient educationImproved education for careof Foley Catheter at home
• Application of GRIP-LOK on all patients with a urinary catheter

Catheter Associated Urinary Tract Infection Prevention Action Team Improvement Strategies
Urinary Catheter Insertion Practice Recommendations:
Two Clinician insertion technique is recommended. Wash hands and maintain aseptic technique. Prewash Meatal/Perineal area prior to performing catheter insertion. Make only one attempt at catheter insertion. If unsuccessful, repeat the entire procedure with new supplies. Secure safely with Grip-Lok (to unaffected leg) if not already done in PARR.
Documentation:
Document why the catheter is in place and give reason if >48 hrs. Document if the patient is exhibiting any signs and symptoms of a UTI? If UTI is suspected send C+S and
document all symptoms such as: fever (>38 degrees C), urgency, frequency, dysuria, or suprapubic tenderness. Document when catheter is inserted and removed including number of attempts and difficulty of insertion.
Urinary Catheter Management Guidelines:
No drooping or looping of tubing. Keep bag below the bladder and off the floor. Drain bag before transfers to prevent back flow. Label drainage container with name and date, rinse after every use and change every 24 hours (at 0600). Maintain closed system. Routine pericare and patient education on proper pericare. Always assess why the catheter is insitu? Two days is too long. Remove a urinary catheter at max postop day 2.
If catheter remains in place document reason and plan of care. Ask if there is a plan for catheter removal?
After catheter removal mobilize, hydrate patient and provide bowel care.


Where are we now?•Continue to educate surgical staff in catheter
care; best practice•Follow up audit of practice changes to confirm
compliance and assess for improvements•Monitor our monthly post op occurrence rates
from NSQIP and compare this with our pre-initiative results
•Review and compare results with our risk adjusted SAR from NSQIP
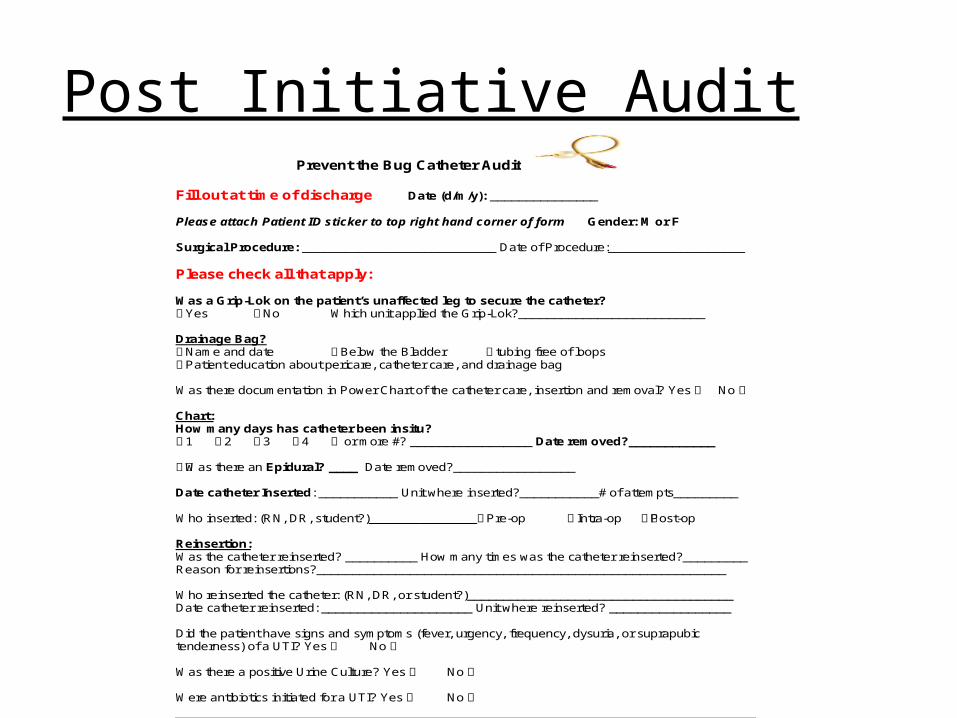
Patient ID sticker
Prevent the Bug Catheter Audit Fill out at time of discharge Date (d/m/y): _______________ Please attach Patient ID sticker to top right hand corner of form Gender: M or F Surgical Procedure: ___________________________ Date of Procedure:___________________ Please check all that apply: Was a Grip-Lok on the patient’s unaffected leg to secure the catheter? Yes No Which unit applied the Grip-Lok?__________________________ Drainage Bag? Name and date Below the Bladder tubing free of loops Patient education about pericare, catheter care, and drainage bag Was there documentation in Power Chart of the catheter care, insertion and removal? Yes No Chart: How many days has catheter been insitu? 1 2 3 4 or more #? _________________ Date removed?____________ Was there an Epidural? ____ Date removed?_________________ Date catheter Inserted: ___________ Unit where inserted?___________# of attempts_________ Who inserted: (RN, DR, student?)_______________Pre-op Intra-op Post-op Reinsertion: Was the catheter reinserted? __________ How many times was the catheter reinserted?_________ Reason for reinsertions?_________________________________________________________ Who reinserted the catheter: (RN, DR, or student?)_____________________________________ Date catheter reinserted: _____________________ Unit where reinserted? _________________ Did the patient have signs and symptoms (fever, urgency, frequency, dysuria, or suprapubic tenderness) of a UTI? Yes No Was there a positive Urine Culture? Yes No Were antibiotics initiated for a UTI? Yes No
Post Initiative Audit

OUR NSQIP TEAM AT NRGH
SURGEON CHAMPION: Dr. Blair Rudston-Brown and
Dr. Scott NeilsonSCR: Debera Coles and Judy Lekisch
QI Consultant: John KristiansenSURGICAL CNE: Kelli Jennison-Gustafson
and Tammy [email protected]

ACKNOWLEDGEMENTS
Angela Tecson- BC SCR SupportBC Patient Safety & Quality Council- NSQIP
Clinical Improvement SharePoint Centers for Disease Control- UTI Guidelines
Institute for Healthcare Improvement Surrey Memorial Hospital- Fraser Health- UTI
Reductions





























