Embed Size (px)
Citation preview

Jacob Johnson, MD
Partner, San Francisco Otolaryngology Medical Group
Assistant Clinical Professor, UCSF
Medical Advisor, Phonak
Otoscopy: What Every Audiologist Should Know

Today’s Presentation
Visualizing the Ear
Medical Considerations
Common Ear Diseases
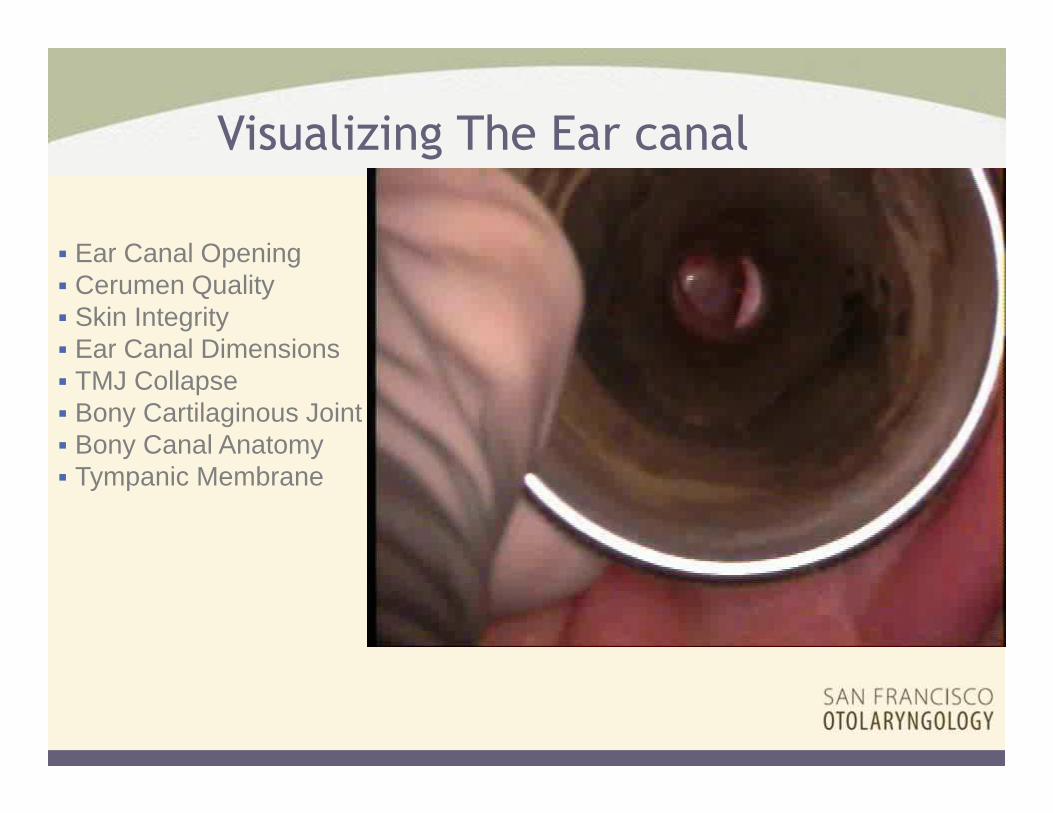
Visualizing The Ear canal
� Ear Canal Opening� Cerumen Quality� Skin Integrity� Ear Canal Dimensions� TMJ Collapse� Bony Cartilaginous Joint� Bony Canal Anatomy� Tympanic Membrane

� Tools for visualization: � Otoscope� Headlight� Magnified Headlight� Video-otoscope� Microscope
Visualizing the ear and tympanic membrane
Medical Considerations:
Tools & Techniques

� Techniques for visualization:� Equipment� Positioning
� Patient� Practioner� Ear canal anatomy
� Talking to the patient� Pre, during & post� Following trauma
Visualizing the ear and tympanic membrane
Medical Considerations:
Tools & Techniques

� 1983
� Looking in the canal
� 1993
� Academy responded with regional training� CIC deep fitting trainings
� Cerumen management workshops
� 2013
� As a field take responsibility for learning the ear canal � Position point for field
� Autonomy
� Cerumen management
� Microscope use
Everything old is new again
Audiologist Perspective

Medical Considerations: Assessment
� Differential diagnosis� Location� Type of Hearing Loss� Urgency/ Severity

Location
� Outer ear (TMJ)� Middle ear/ Mastoid� Inner ear� Face, Salivary glands, Neck� Central, Cranial Nerves� Systemic (Eyes, Thyroid, Heart, Kidney)

Type of Hearing Loss
� Conductive� Sensori-neural� Mixed Hearing Loss

�Hearing�Tinnitus�Vertigo�VII Cranial N.�TMJ/ Ear Pain�Skin Quality�CNS� Immune System�General Health �Motivation
Ear Assessment and Anatomy
““““Many look, few see””””
Medical Considerations: Management

Location
� Outer ear (TMJ)

� Description: keratin & oil material in ear canal
� Management: cerumen loop, irrigation, suction
� Deep fitting candidacy: moderate concern and needs active management
Identified as: Cerumen Impaction
Common Ear Diseases
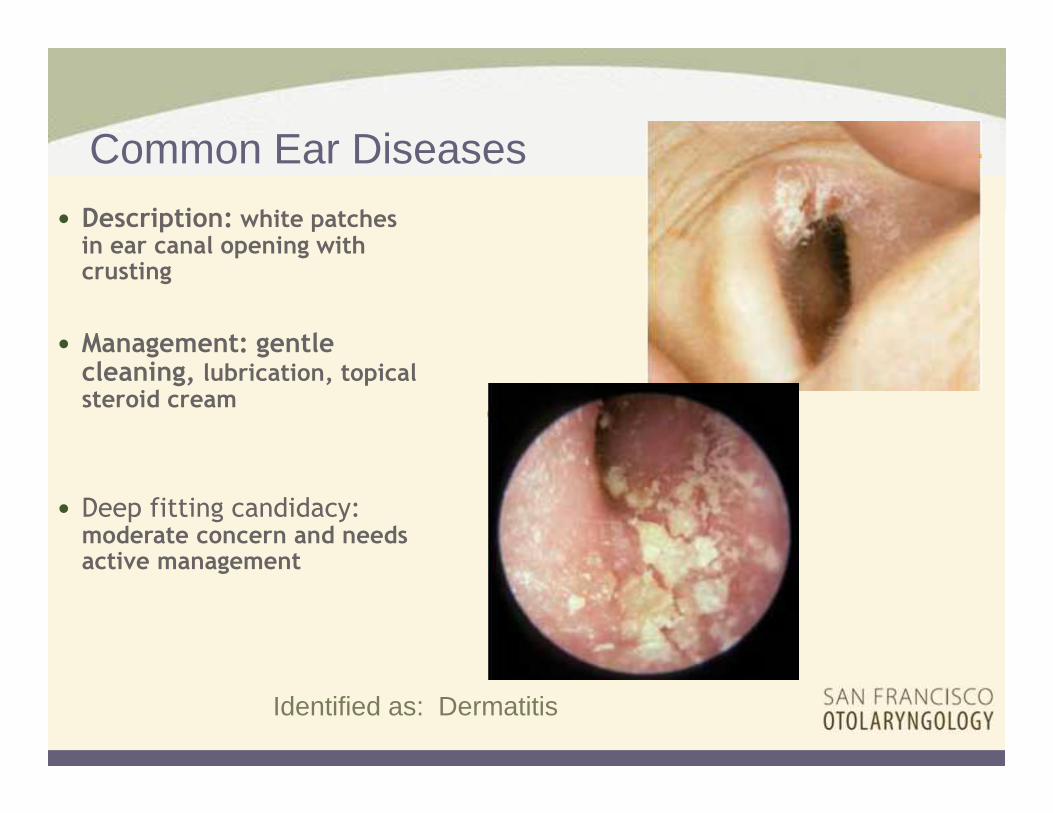
� Description: white patches in ear canal opening with crusting
� Management: gentle cleaning, lubrication, topical steroid cream
� Deep fitting candidacy: moderate concern and needs active management
Identified as: Dermatitis
Common Ear Diseases

� Description: conchal bowl cartilage protrudes toward tragus
� Management: surgical
� Deep fitting candidacy: mild to moderate concern
Identified as: Collapsing Ear Canal
Common Ear Diseases

� Description: underdeveloped ear and no ear canal
� Management: surgical, prosthetic, stem cells, BAHA
� Deep fitting candidacy: contraindicated
Identified as: Microtia and Atresia
Common Ear Diseases
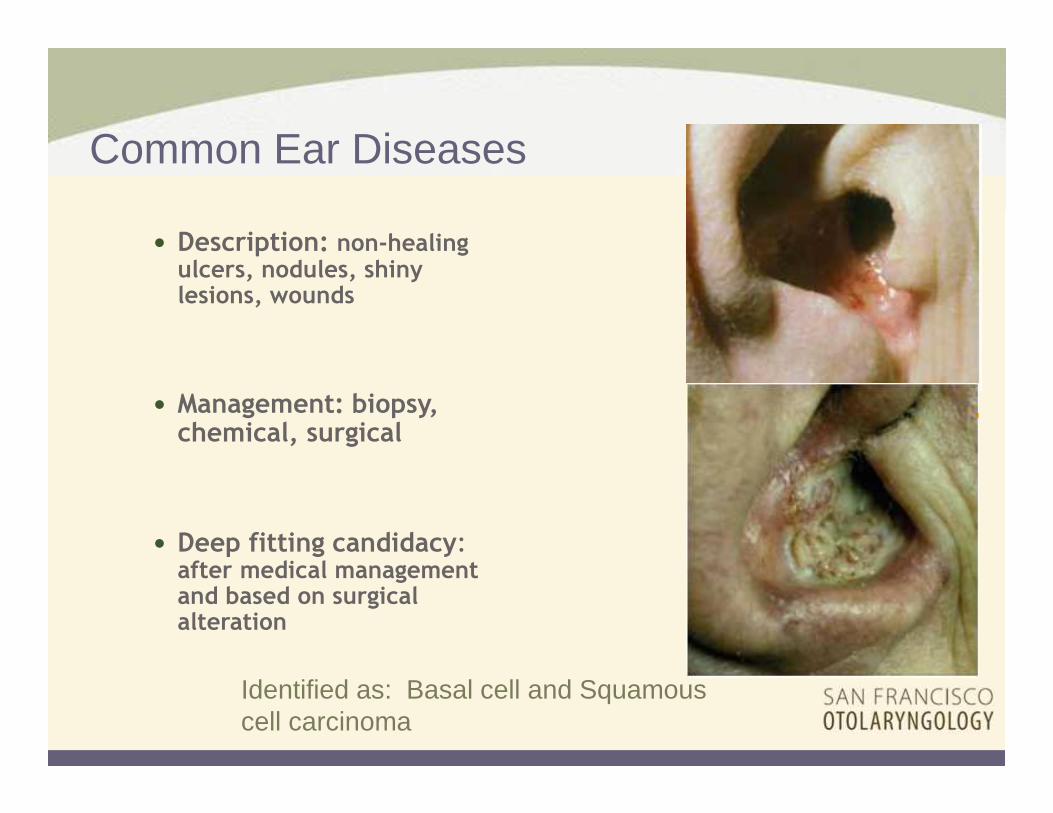
� Description: non-healing ulcers, nodules, shiny lesions, wounds
� Management: biopsy, chemical, surgical
� Deep fitting candidacy: after medical management and based on surgical alteration
Identified as: Basal cell and Squamous cell carcinoma
Common Ear Diseases

� Description: line of blisters along concha bowl, ear canal onto TM
� Management: Acyclovir/ Valtrex, prednisone
� Deep fitting candidacy: medical clearance (pain issues)
Identified as: Shingles
Common Ear Diseases

� Description: swollen ear canal opening with wetness and white debris in bony canal
� Management: keep ear dry for 6 weeks, clean debris, antibiotics/steroid drops, possible ear wick, possible oral antibiotics for immuno-compromised patients
� Deep fitting candidacy: contraindicate if recurrent
Identified as: Otitis Externa
(Swimmer’s ear)
Common Ear Diseases
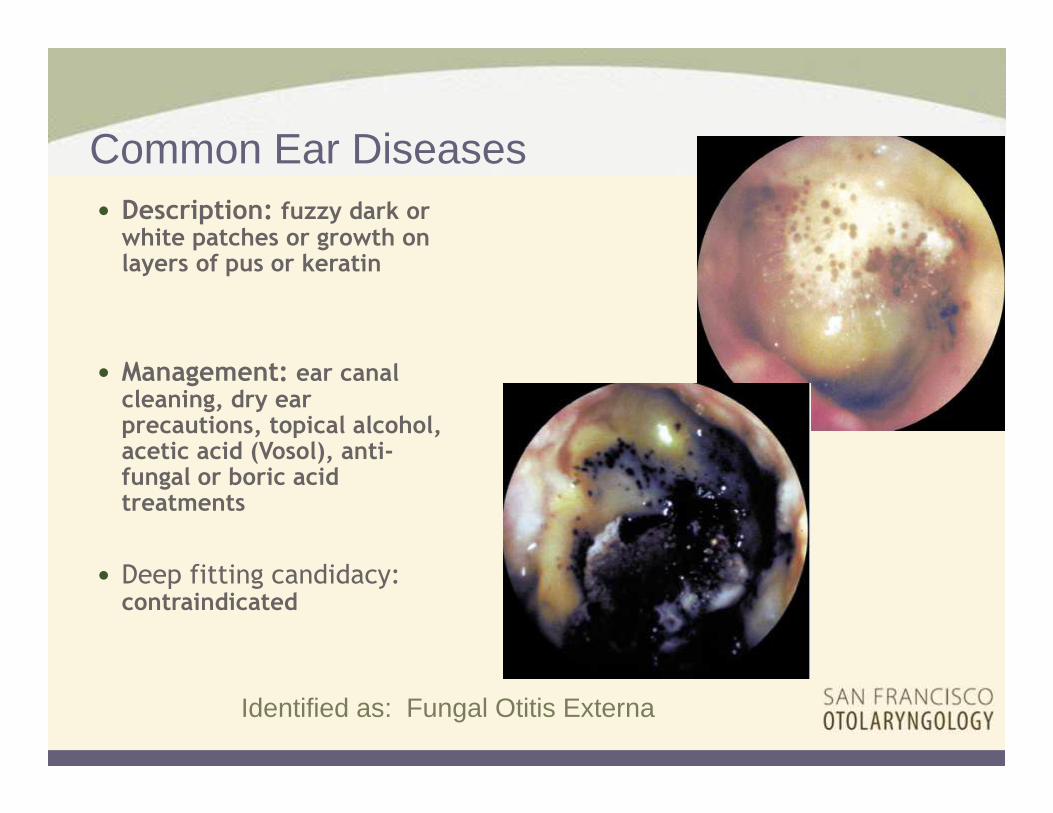
� Description: fuzzy dark or white patches or growth on layers of pus or keratin
� Management: ear canal cleaning, dry ear precautions, topical alcohol, acetic acid (Vosol), anti-fungal or boric acid treatments
� Deep fitting candidacy: contraindicated
Identified as: Fungal Otitis Externa
Common Ear Diseases
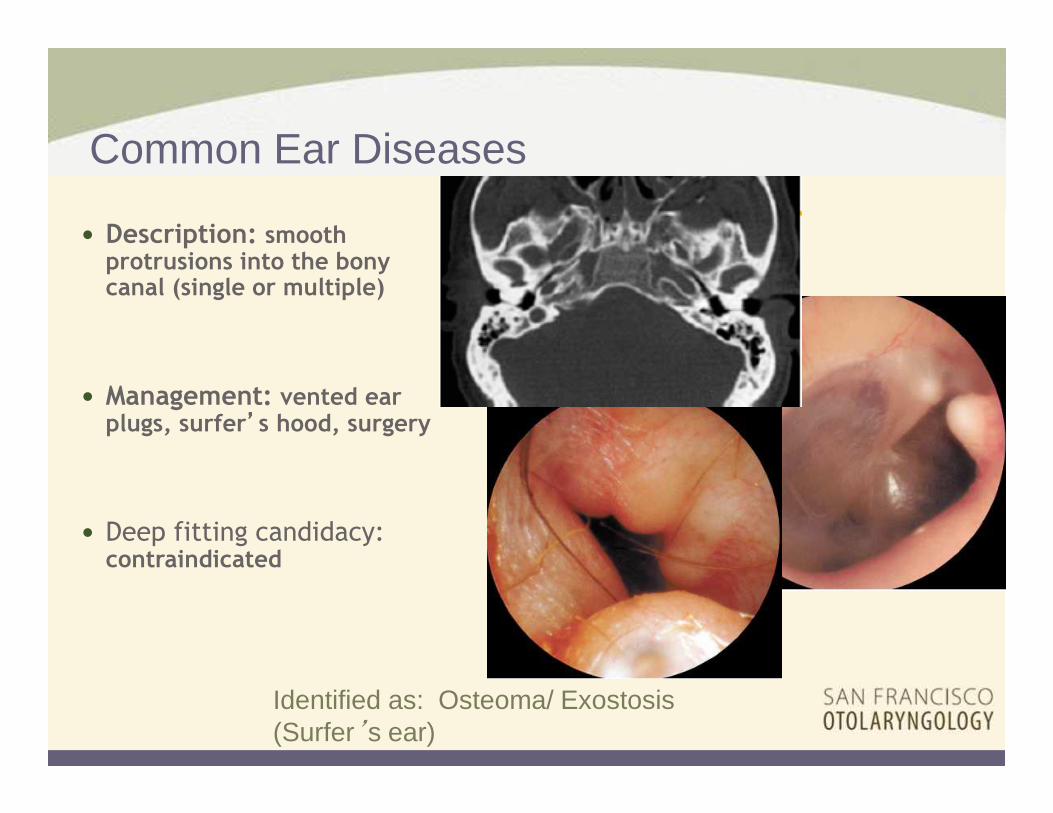
� Description: smooth protrusions into the bony canal (single or multiple)
� Management: vented ear plugs, surfer’’’’s hood, surgery
� Deep fitting candidacy: contraindicated
Identified as: Osteoma/ Exostosis (Surfer’s ear)
Common Ear Diseases

� Description: foreign body
� Management: removal
� Deep fitting candidacy: check device each time it is removed
Identified as: Foreign body
Common Ear Diseases
Location
Middle ear/Mastoid

� Description: blister on TM
� Management: observation, lance
� Deep fitting candidacy: consider if device touched TM
Identified as: TM Bulla (Blister)
Common Ear Diseases

� Description: bubbles behind TM
� Management: observation, myringotomy if persistent
� Deep fitting candidacy: important to do tympanogram, medical clearance
Identified as: Serous Otitis Media
Common Ear Diseases

� Description: hazy, bulging, congested TM
� Management: oral antibiotics, myringotomy
� Deep fitting candidacy: remove device to evaluate TM, refit when well
Identified as: Acute Otitis Media
Common Ear Diseases
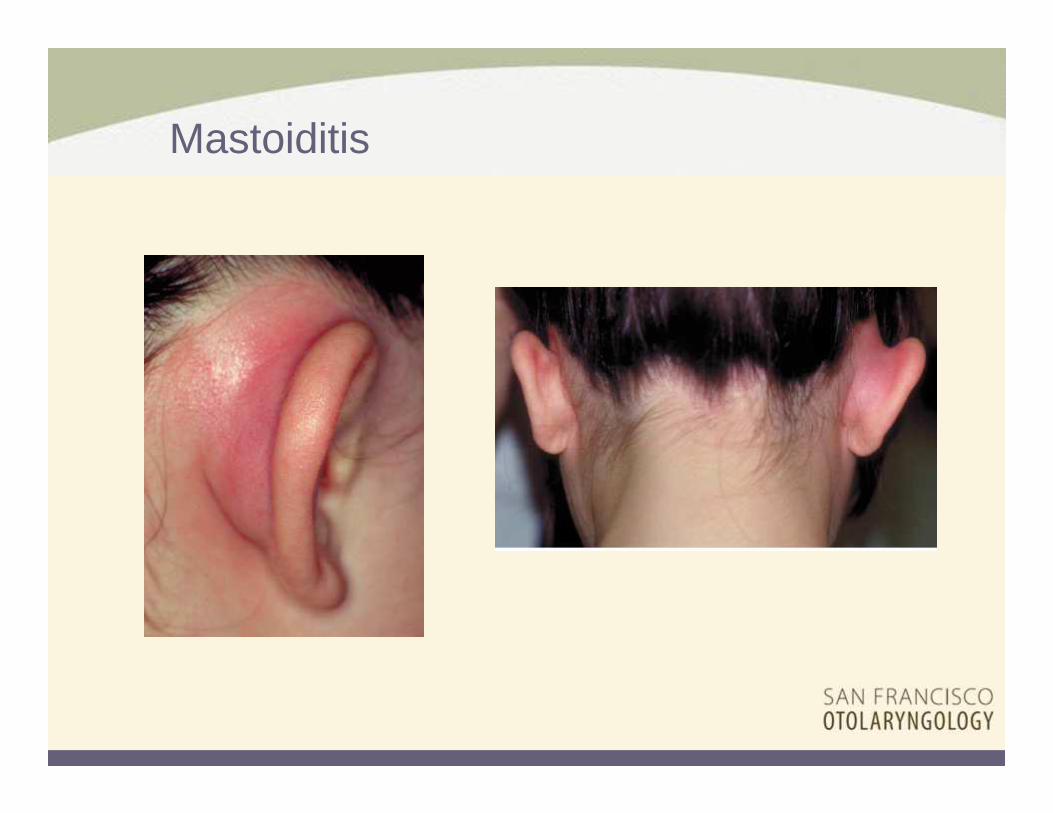
Mastoiditis

� Description: silver or colored hole in TM (standard vs. extended)
� Management: observation, treatment of underlying issue
� Deep fitting candidacy:contraindicated, concern with T-tube
Identified as: Ear Tubes
Common Ear Diseases

� Description: hole in TM, clear edge with no thin TM covering hole (““““monomeric”””” membrane)
� Management: observation, tympanoplasty
� Deep fitting candidacy: medical clearance (dry vs. wet)
Identified as: TM Perforation/
Myringosclerosis
Common Ear Diseases

� Description: chronic ear drainage (wet ear canal) with TM perforation
� Management: medical, imaging and possible tympano-mastoidectomy
� Deep fitting candidacy: contraindicated
Identified as: Chronic otitis media (Draining ear)
Common Ear Diseases
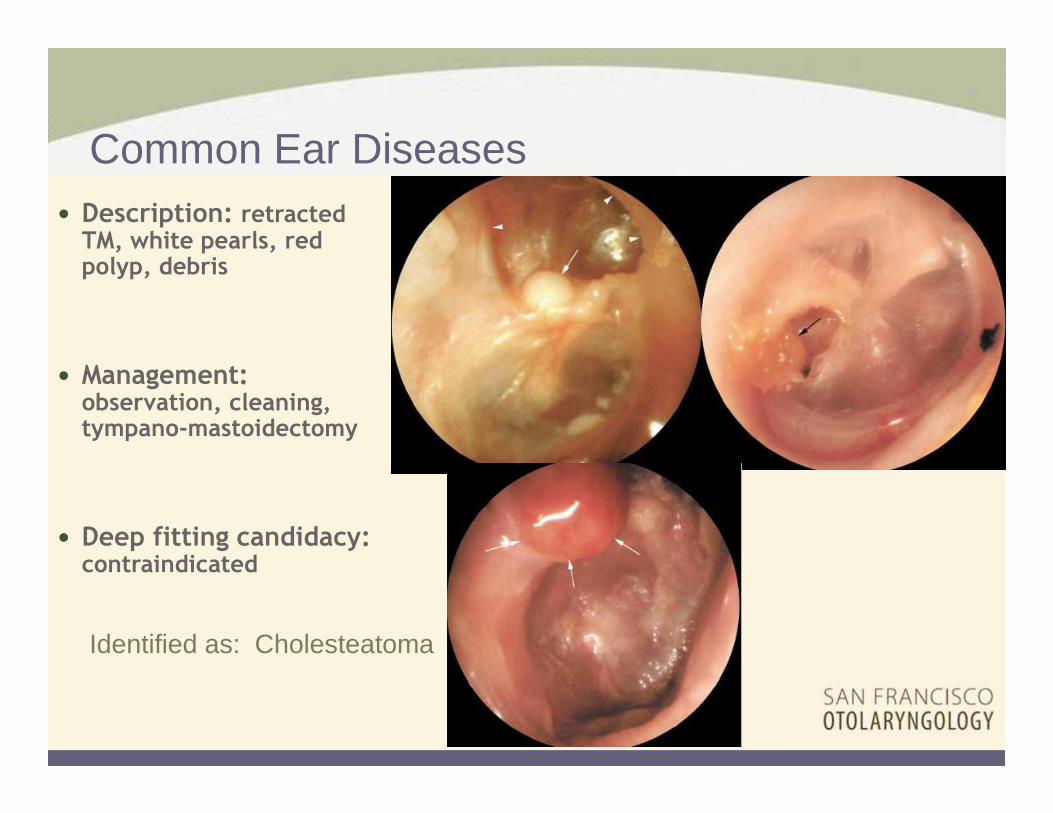
� Description: retracted TM, white pearls, red polyp, debris
� Management: observation, cleaning, tympano-mastoidectomy
� Deep fitting candidacy: contraindicated
Identified as: Cholesteatoma
Common Ear Diseases

Canal Wall Down Mastoidectomy

Location
� Inner Ear

� Description: red or blue lesions on or behind the TM
� Management: referral, imaging, surgical, observation
� Deep fitting candidacy: contraindicated until cleared
Identified as: Glomus tumor/
Hemotympanum
Common Ear Diseases

Temporal Bone Fractures
Longitudinal or otic capsule sparing Transverse or otic capsule violating

Within skeleton, matrix material properties are anatomically-distinct
- J.D. Currey, J. Exp. Biol 1999
*
*
*
*
*
*
*
Bone matrix material properties
- elastic modulus and hardness- independent of bone mass and geometry
*
6.7 GPa11.2 GPa18.5 GPa
21.8 GPa
25.4 GPa
34.1 GPa
***
*
**

Inner ear
Superior SCC Dehiscence Acoustic neuromaInner Ear Fistula
� Management versus referral
� Assessment
� Urgency
� Commitment to learning (practice)
Medical Considerations: Management

Day 0 Days 1-7 Days 8-14 Days 15-21 Days 22-30 Days Over 30
<=27 Insertions 9.47% 15.15% 32.14% 17.86% 6.82% 4.49%
Between 28 - 224 Insertions 5.51% 16.10% 11.74% 8.34% 5.42% 2.16%
Over 225 Insertions 5.84% 13.44% 8.68% 5.71% 4.47% 1.98%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
R
e
m
o
v
a
l
R
a
t
e
s
DOW
DOW for Ear Irritation Medical Removal Reasonfor All Lyrics US Subscriptions
Comparing Accounts by the Number of Insertion Experiencefrom 2012- 2013
As of December 16, 2013
<=27 Insertions Between 28 - 224 Insertions Over 225 Insertions

Expert- 10,000 hours