Embed Size (px)
Citation preview

2010 Courses AANEM 57th Annual Meeting
Québec City, Québec, Canada
2010 Course AANEM 57th Annual MeetingQuébec City, Québec, Canada
Carpal Tunnel Syndrome From A To ZOther AANEM Learning Opportunities
Course Books
Lecture Series
Workshop Handouts
Educational CD/DVDs
Monographs
Case Reports
EDXSAEs/NMSAEs
Podcasts
Coding Resources
Invited Reviews
Case Studies
Practice Guidelines
Over 160 educational resources available at www.aanem.org
American Association of Neuromuscular & Electrodiagnostic MedicineAdvancing neuromuscular, musculoskeletal, & electrodiagnostic medicine
10YZ

Carrie E. Ford, R.NCS.T., R.EP T. Janet K. James, R. EEG T., R.NCS.T.
Jim Lewis, R.NCS.T.Lawrence R. Robinson, MD
Carpal Tunnel Syndrome From A to Z
AANEM 57th Annual Meeting Québec City, Québec, Canada
Copyright © October 2010 American Association of Neuromuscular
& Electrodiagnostic Medicine 2621 Superior Drive NW
Rochester, MN 55901
Printed by Johnson Printing Company, Inc.

AANEM Course Neuroanatomy for Nerve Conduction Studies iii
Neuroanatomy for Nerve Conduction Studies
Contents
CME Information iv
Faculty v
The Spinal Accessory Nerve and the Less Commonly Studied Nerves of the Limbs 1Zachary Simmons, MD
Ulnar and Radial Nerves 13Kevin R. Scott, MD
The Tibial and the Common Peroneal Nerves 21Kimberley B. Butler, R.NCS.T., R. EP T., CNIM
Median Nerves and Nerves of the Face 27Jerry Morris, MS, R.NCS.T.
iii
Course Description This course is designed to provide an introduction to anatomy of the major nerves used for nerve conduction studies, with emphasis on the surface land-marks used for the performance of such studies. Location and pathophysiology of common lesions of these nerves are reviewed, and electrodiagnostic methods for localization are discussed. This course is designed to be useful for technologists, but also useful and informative for physicians who perform their own nerve conduction studies, or who supervise technologists in the performance of such studies and who perform needle EMG examinations..
Intended Audience This course is intended for Neurologists, Physiatrists, and others who practice neuromuscular, musculoskeletal, and electrodiagnostic medicine with the intent to improve the quality of medical care to patients with muscle and nerve disorders.
Learning Objectives Upon conclusion of this program, participants should be able to: (1) describe anatomy as it pertains to common sites of entrapment.(2) improve their ability to perform nerve conduction studies.
Activity Profile This enduring material activity is a reproduction of the printed materials from a course at the AANEM Annual Meeting (October 6-9, 2010). Physician participation in this activity consists of reading the manuscript(s) in the book and completing the clinical and CME questions.
Release Date: January 10, 2011 Expiration Date: January 10, 2014. Your request to receive AMA PRA Category 1 Credits™ must be submitted on or before the credit expiration date. Duration/Completion Time: 2 hours
Accreditation and Designation Statements The American Association of Neuromuscular and Electrodiagnostic Medicine (AANEM) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The AANEM designates this enduring material for a maximum of 2.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit com-mensurate with the extent of their participation in the activity.
iv

AANEM Course Neuroanatomy for Nerve Conduction Studies v
Neuroanatomy for Nerve Conduction Studies
Faculty
v
Kimberley B. Butler, R.NCS.T, R. EP T., CNIMElectroneurodiagnostic TechnologistHartford Health CareWillimantic , ConnecticutMs. Butler has 30 years experience working in medicine. Originally a cardiac technologist and cardiac monitor technician, she has gone on to perform electroencephalograms (EEGs), long-term monitoring (LTM), intraoperative monitoring (IOM), evoked potentials (EPs), and now nerve conduction studies (NCSs). She has served on many boards and at one time was chair of the American Association of Electrodiagnostic Technologists (AAET) Examination Committee. She speaks and teaches regularly on board review courses, as well as a host of other topics. She has been published many times, including articles in Muscle & Nerve. Currently, she is branching into a new area, video urodynamics and pelvic floor neurophysiology.
Course Chair: Zachary Simmons, MD
The ideas and opinions expressed in this publication are solely those of the specific authors and do not necessarily represent those of the AANEM.
Jerry Morris, MS, R.NCS.T.Electrodiagnostic TechnologistNeurodiagnostic LaboratoryWillis-Knighton Medical CenterShreveport, LouisianaMr. Morris has more than 25 years of experience teaching at various electrodiagnosis seminars and as a guest speaker for engagements across the United States and Canada. Topics have included neuromuscular junction disease, entrapment and generalized neuropathies, late responses (F waves and H reflexes), blink reflexes, myopathies, basic to advanced nerve conduction study (NCS) electrode placement, and anatomy and physiology of the nervous system. He is currently a member of the American Association of Neuromuscular & Electrodiagnostic Medine (AANEM), the American Society of Electroneurodiagnostic Technologists (ASET), and the American Association of Electrodiagnostic Technologists (AAET). His past positions in these organizations include: AAET—past president, past member of the Board of Directors, and past member of the Examination Committee; ASET—past member of the Board of Directors, Program Chair of the 2009 Annual Meeting, and member of the Membership Committee. He is currently developing online an NCS course for ASET to be published in 2010. He was the ASET Theda Sannit Educational Award recipient for 2008.
Dr. Simmons is a consultant for Neuralstem, Inc. Any conflict of interest was resolved according to ACCME Standards.
All other authors/faculty have nothing to disclose.

vi
Kevin R. Scott, MD, MAAssociate Professor of NeurologyDepartment of NeurologyPennsylvania State College of MedicineMilton S. Hershey Medical CenterHershey, PennsylvaniaDr. Scott received his medical degree from Wake Forest University School of Medicine. He completed a neurology residency and a neurophysiology fellowship training at Pennsylvania State College of Medicine. He is cur-rently an associate professor of neurology specializing in neuromuscular medicine and clinical neurophysiology. He is the program director of the Clinical Neurophysiology and Clinical Neuromuscular Fellowship pro-grams at Pennsylvania State College of Medicine. Dr. Scott in an American Board of Electrodiagnostic Medicine Diplomate.
Zachary Simmons, MDProfessor of NeurologyDepartment of NeurologyPennsylvania State College of MedicineMilton S. Hershey Medical CenterHershey, PennsylvaniaDr. Simmons received his medical degree from the University of Florida, and then trained in neurology at the University of Iowa and in neuro-muscular diseases and electromyography at the University of Michigan. He now serves as professor of neurology at Pennsylvania State Hershey Medical Center, where he is the director of the Neuromuscular Program and the Clinical Neurophysiology Laboratory. He founded and directs the Hershey Medical Center ALS Clinic. Active research programs under his supervision include studies of quality of life, cognitive function, and the development of evidence-based practice protocols for patients with amyo-trophic lateral sclerosis. Dr. Simmons has served on the AANEM Training Program, Workshop, and Program Committees, has been chair of the ABEM Maintenance of Certification Committee, and currently is chair of the ABEM Examination Committee. Dr. Simmons is an American Board of Electrodiagnostic Medicine Diplomate.

AANEM Course Neuroanatomy for Nerve Conduction Studies viivii
Please be aware that some of the medical devices or pharmaceuticals discussed in this handout may not be cleared by the FDA or cleared by the FDA for the specific use described by the authors and are “off-label” (i.e., a use not described on the product’s label). “Off-label” devices or pharmaceuticals may be used if, in the judgement of the treating physician, such use is medically indi-cated to treat a patient’s condition. Information regarding the FDA clearance status of a particular device or pharmaceutical may be obtained by reading the product’s package labeling, by contacting a sales representative or legal counsel of the manufacturer of the device or pharmaceutical, or by contacting the FDA at 1-800-638-2041.

AANEM Course Carpal Tunnel Syndrome From A to Z 1
FALSE POSITIVES (SPECIFICITY) AND FALSE NEGATIVES (SENSITIVITY) IN CARPAL TUNNEL SYNDROME
When performing electrodiagnostic (EDX) evaluation for carpal tunnel syndrome (CTS), it is important to avoid false positive results (low specificity) and false negative results (low sensitivity). Specificity is the likelihood of a normal result in healthy people without disease, and sensitivity is the likelihood of an abnormal results in the presence of the disease or disorder.
These concepts are particularly applicable to sensory nerve conduc-tion studies (NCSs) for CTS. There are many approaches to evaluat-ing median sensory conduction across the wrist. It is critical to think through these alternative approaches before seeing the patient. In particular, avoid the approach of doing one test and, upon finding a normal result, doing one test after another until an abnormality is found. While this approach is tempting, it is risky for the patient.
Each test, if well designed and studied in an appropriate healthy group, would include the mean ±2 standard deviations within the reference range. This means that 2.5% of healthy asymptomatic controls would be classified as abnormal (i.e., false positives). As each test is performed and analyzed, one roughly adds a 2.5% false positive rate. Thus, performing two tests, allowing an abnormality in either one to make a diagnosis, theoretically carries a 4.9% false positive rate.1 These theoretical calculations are shown in Table 1 and Figure 1.
In the setting of CTS, empirical measures have in part confirmed these theoretical calculations. In one study examining the effect of performing three tests in CTS, it was found that allowing one abnormal measure to make a diagnosis carried an 8% false positive rate (predicted 7.3% as in Table 1), while requiring two abnormal
measures of three tests carried only a 2% false positive rate (predicted 0.2%).2
There are several options to avoid false positives associated with doing multiple tests. The practioner could perform just one test for all patients coming to the laboratory; this however carries several risks including missing subtle disease affecting only some nerve fascicles, being misled by technical errors on a single test, and perhaps not picking the best test. Another possibility is to require multiple tests to be abnormal to make a diagnosis. The latter approach is not a bad one and effectively reduces the chances of false positive results. However, sensitivity will be lower as only more severe cases will
Bringing Together the Electrodiagnostic and Clinical
Information
Lawrence R. Robinson, MDProfessor
Rehabilitation MedicineUniversity of Washington
Seattle, Washington
1
Figure 1 The chance of having one abnormal test out of a number of tests performed. This calculation assumes a 2.5% false positive rate for each test (use of mean ± 2 standard deviation) and independence of the tests.

demonstrate multiple abnormalities. In a study using this approach, CTS sensitivity was reduced from 85% (requiring only one of three tests to be abnormal) to 74% if one required two tests to be abnor-mal.2 Requiring three of three tests to be abnormal further reduced sensitivity to 56%.
A preferred approach is similar to that used for standardized tests that everyone has all taken (board certification, admissions test, etc.). Ask multiple questions to assess different areas and summarize the results into a single summary score. While there are advanced statis-tical methods to perform this process such as discriminant analysis or factor analysis3,4 this process can be approximated quite well with simple addition.2
To achieve such a summary score, rely upon the three sensory NCSs (see Fig. 2, on page 3) that have literature support for a high degree of sensitivity and specificity in CTS. These include: comparison of the median and ulnar sensory antidromic conduction to the ring finger at 14 cm (ringdiff ), comparison of the median and radial sensory antidromic conduction to the thumb at 10 cm (thumbdiff ), and comparison of median and ulnar orthodromic conduction across the wrist with palmar stimulation at 8 cm (palmdiff ).5,6
The strategy is to simply add the results from these three tests into a single number. The combined sensory index (CSI) is calculated as the sum of the three latency differences (median peak latency minus ulnar or radial peak latency):
CSI = ringdiff + thumbdiff + palmdiff
An example is given in Figure 2 (on page 3), where the CSI is cal-culated as:
CSI = (3.8 – 3.2) + (3.2 – 2.7) + (2.2 – 1.9)
= 0.6 + 0.5 + 0.3
= 1.4 ms
Studies in subjects without CTS indicate that a reference value of up to 0.9 ms is normal, i.e., 1 ms or over is abnormal. When median latency is less than the comparable ulnar or radial nerve latency, a negative number is entered in the equation.
Although this technique was described in 1998 as the combined sensory index, or CSI,2 the advent of the television series CSI (Crime Scene Investigation) in 2000 has caused some to rename this tech-nique to the “Robinson index.” This author thinks the alternative name is fine.
This method carries the advantages of performing multiple tests (assessing multiple areas of nerve, enhancing reproducibility of find-ings, etc.) but does not create the problem of multiple comparisons and the consequent increase in false positives. Thus, as long as one performs three tests but only “looks at” the summated result from all three tests, one does not run into the problem of an additive false-positive rate. Using this approach, sensitivity is improved with specificity still remaining acceptable at 95%.2
While this approach represents an improvement over single tests, it has also been noted that it might not be necessary to perform all three tests for the CSI when the first test results are toward the ex-tremes of the normal or abnormal range.7 Figure 3 demonstrates the likelihood of finding an abnormal CSI as the median minus ulnar latency difference to the ring finger increases. Note that when there is no latency difference, or when the median nerve is faster than the ulnar nerve, there is a very low chance of finding an abnormal CSI (≥ 1.0). Similarly, when latency differences are 0.5 ms or more, almost all subjects will have an abnormal CSI. A conclusion with one test
2 Electrophysiologic Testing in Generalized Weakness AANEM Course
Table 1 Chances of abnormal results as the number of independent measures increases
Number of measures At least one At least two abnormal result abnormal results 1 2.5% - 2 4.9% 0.1% 3 7.3% 0.2% 5 11.9% 0.6% 10 22.4% 2.5% 20 39.5% 8.5%
Table 2 Sensitivity of the combined sensory index for detecting carpal tunnel syndrome, compared to individual tests
Test Reference value Sensitivity Midpalm < 0.3 70% Ring < 0.4 74% Thumb < 0.5 76% CSI < 0.9 83%
Specificity was 95-97% for all tests.2
CSI = combined sensory index
Figure 3 The chance of an abnormal combined sensory index (CSI) plotted against the median minus ulnar latency difference at the ring finger. Note that when latency differences are 0.5 ms or more, essentially all such patients will have an abnormal CSI. When the median latency is the same or less than the ulnar nerve latency, essentially all such patients will have a normal CSI.

AANEM Course Carpal Tunnel Syndrome From A to Z 3
can be made when the latency difference is less than 0 or greater than 0.5 ms. The CSI is most useful when the difference at the ring finger is between 0.1 and 0.4 ms. This uncertain region is the range where performing additional tests will be most helpful. Figure 4 demonstrates similar ranges for each of the three tests.
Reliability is also an important consideration when designing elec-trodiagnostic (EDX) testing for CTS. It is preferable to use a testing protocol that provides a similar result if testing is repeated within a few days. Figure 5 shows a plot of test results from one day plotted against those from another in the same subjects. This figure shows that the CSI has a markedly higher degree of test–retest (intraob-server) reliability than single tests.8
The question occasionally arises as to what represents a sig-nificant difference between two different examinations. This is an important question when looking for either im-provement (e.g., after treatment) or worsening (e.g., after passage of time). An analysis of the same data using methods of Bland and Altman9 yields the graph in Figure 6. This plot indicates that a difference in CSI between two different tests of more than 0.3 ms is greater than that expected by chance alone. Thus, if one measures a change in CSI over time exceed-ing 0.3 ms, this likely represents a significant improvement or worsening; changes of 0.3 ms or less are not significant.
Figure 2 Three sensory nerve conduction studies commonly used to evaluate for carpal tunnel syndrome. These are (from top to bottom): median and ulnar comparison to the ring finger at 14 cm, median and radial comparison to the thumb at 10 cm, and median and ulnar comparison across the wrist with palmar stimulation at 8 cm.

NEEDLE ELECTROMYOGRAPHY IN DIAGNOSING CARPAL TUNNEL SYNDROME
There is some debate regarding the utility of needle electromyography (EMG) in the diagnosis of CTS. Some have reported that needle EMG of thenar muscles (or of the upper limb in general) is useful to look for evidence of axon loss or to diagnose cervical radiculopathy. Others, however, have reported that needle EMG of thenar muscles adds little to NCSs in the diagnosis of CTS.10 A recent literature review11 has summarized the state of the literature at present and concludes that needle EMG studies are not as sensitive or specific as NCSs to diagnose CTS although they are useful to document axonal nerve pathology.
Given lack of scientific data to guide the approach to needle EMG this author usually performs needle EMG in those in whom the yield is likely to be greatest or those in whom unique information can be provided. This includes three groups:
1. Patients in whom the median motor response is abnormal
2. Those patients with a history of trauma (where axon loss is more likely)
3. Patients with a clinical presentation that suggests another possible diagnosis (e.g., cervical radiculopathy or brachial plexopathy).
4 Electrophysiologic Testing in Generalized Weakness AANEM Course
Figure 4 Each of the three tests that comprise the combined sensory index (CSI) has a range of results that suggest the CSI will be normal (normal range), a region where the CSI is very likely to be abnormal, and a range where there is uncertainty and where the CSI will clarify the diagnosis.
Figure 5 Plots of test results from 2 different days for the median minus ulnar palmar stimulation comparison and the combined sensory index (CSI). The Spearman ρ (rho) coefficient is a nonparametric correlation coefficient Perfect correlation would have a value of 1. The Spearman ρ was 0.75 for midpalmar studies, 0.67 for studies to the ring finger, and 0.75 for studies to the thumb. The Spearman ρ for the CSI was 0.95 indicating a higher test–retest reliability.
Figure 6 Plot of the combined sensory index (CSI) obtained on 2 different days according to the methods of Bland and Altman. The average of the two values is plotted against the difference between the two values. This finding suggests that a difference in CSI of greater than 0.3 ms is significant and demonstrates either significant improvement or worsening.

AANEM Course Carpal Tunnel Syndrome From A to Z 5
EVALUATING FOR CARPAL TUNNEL SYNDROME IN THE PRESENCE OF AN UNDERLYING POLYNEUROPATHY
Diagnosing CTS in the presence of an underlying polyneuropathy presents special challenges. While it would seem that one could simply measure the difference in slowing in the median nerve versus other nearby nerves, it is not clear that all nerves are equally affected by diffuse neuropathies. It is quite possible that due to vascular supply or fascicular anatomy the median nerve is more severely af-fected than other nearby nerves in the upper limbs. Thus use caution in using the same diagnostic criteria for CTS in patients with diabetic or other polyneuropathies, and be sure that EDX findings are consis-tent with the clinical picture.
DESCRIBING SEVERITY OF CARPAL TUNNEL SYNDROME
There have been a number of proposed schemes to describe the sever-ity of CTS based on EDX findings. There are some conceptual prob-lems, however, with assigning disease severity based upon median nerve latency. First, a number of studies have shown that there is not a strong correlation between latency and symptoms in CTS.12 This finding is not surprising since a delay in latency of a few mil-liseconds is not likely to cause sensory or motor symptoms. Rather symptoms are more likely caused by ectopic nerve excitation, con-duction block, and axon loss, none of which are directly measured by latency.
A second problem with using nerve conduction data to assign sever-ity is the arbitrary nature of the assignment. Authors have proposed various categories for mild, moderate, and severe CTS, but these categories are arbitrary and have not been devised by correlation with outcomes, symptoms, or other independent measures.
It is therefore not possible to accurately define the severity of CTS with electrophysiologic studies. The degree of nerve conduction abnormalities can be described, but this is different from disease severity. An exception to this position is when there is evidence of denervation in thenar muscles. In that case, evidence of motor axon loss suggests a more severe lesion and suggests the need for surgical release more urgently.
PROGNOSIS OF CARPAL TUNNEL SYNDROME
There is growing information that NCSs can offer guidance as to outcome of carpal tunnel release (CTR) in patients with CTS. This is best summarized in Figure 7, which is the information provided to the author’s referral physicians.
CARPAL TUNNEL RELEASE POSTOPERATIVE ELECTRODIAGNOSTIC STUDIES
Take special care in evaluating the patient with persistent symptoms after CTR. Improvement in latencies usually occurs after success-ful release, with maximal improvement usually present within 6 months of surgery. However, latencies often do not return to the
normal range13 despite successful release. Thus, it is critical in these cases to compare post-operative latencies with pre-operative latencies to look for improvement or worsening. In the event there are no pre-operative studies for comparison, one should consider studying the patient twice over several months time, looking for change.
TREATMENT OF CARPAL TUNNEL SYNDROME
Reproduced from Labor and Industries CTS Guidelines, Washington State: http://lni.wa.gov/ClaimsIns/Files/OMD/MedTreat/CarpalTunnel.pdf. See also: http://www.aaos.org/Research/guide-lines/CTSSummaryofRecommendations.pdf for American Academy of Orthopaedic Surgeons guidelines.
Figure 7 Prognostic information provided to referral physicians by the author.
Above are the reported frequencies of complete symptom resolution after carpal tunnel release according to EDX criteria. These outcomes are only reported for EDX criteria and should not be used as the only predictive findings. Other factors may have strong influences on outcomes.
EDX criteria Frequency of symptom resolution1. Normal study 40%2. CSI 1.0-2.5 50%3. CSI 2.5-4.6 63%4. CSI > 4.6, Sensory responses present 55%5. Sensory responses absent, motor latency < 6.5 ms 45%6. Motor latency > 6.5 ms 42%7. Absent motor and sensory responses 23%The combined sensory index (CSI) is calculated as: (median − radial latency to thumb) + (median − ulnar latency to ring finger) + (median − ulnar latency across the palm)
References Bland JD. Do nerve conduction studies predict the outcome of carpal tunnel de-compression? Muscle Nerve 2001 Jul;24(7):935-940. Malladi N, Micklesen PJ, Hou J, Robinson LR. Carpal tunnel syndrome: a retro-spective review of the correlation between the combined sensory index and clinical outcome after carpal tunnel decompression. Muscle Nerve 2010 Apr;41(4):453-457.
EDX = electrodiagnostic

Conservative Treatment
Conservative management may be helpful and may include:
1. Splinting of the wrist. (May be more useful at night).
2. Anti-inflammatory medication including nonsteroidal.
3. Steroid injections. Although this form of treatment is favored by some physicians, it may not have longterm benefits and may itself cause nerve injury. No more than two steroid injections over a 3-month period will be authorized.
The duration of conservative treatment will depend primarily on whether the patient can remain at work. Most patients will improve when off work, whether or not specific treatment is rendered. In some cases, job modification, along with conservative treatment, may improve symptoms and prevent worsening of occupational CTS (OCTS). If job modification is not possible, or if the claimant cannot continue working with conservative treatment, then surgery should be considered as a treatment option.
Surgery
Decompression of the transverse carpal ligament is the surgical pro-cedure of choice for OCTS. A second procedure, internal neurolysis, or freeing up of the nerve, is sometimes requested; however, there is no evidence to suggest that this procedure is necessary and, in most cases, requests for this procedure will be denied.
Return to Work
The vast majority of persons with work-related OCTS are expected to have dramatic relief of their symptoms after carpal tunnel decom-pression surgery and should return to their same job. Return to work, with or without job modification, should be tried in most people. If symptoms worsen or reappear after return to work, repeat nerve con-duction velocities (NCVs) will help to sort out if OCTS has recurred, and if surgery successfully removed the pressure on the median nerve (NCVs will improve with successful surgery, although they may not return completely to normal).
REFERENCES
1. Robinson LR, Temkin NR, Fujimoto WY, Stolov WC. Impact of statistical methodology on normal limits in nerve conduction studies. Muscle Nerve 1991;14:1084-1090.
2. Robinson LR, Micklesen P, Wang L. Strategies for analyzing nerve conduction data: superiority of a summary index over single yests. Muscle Nerve 1998;21:1166-1171.
3. Robinson LR, Rubner DE, Wahl PW, Fujimoto WY, Stolov WC. Factor analysis. A methodology for data reduction in nerve conduc-tion studies. Am J Phys Med Rehabil 1992;71(1):22-27.
4. Rondinelli RD, Robinson LR, Hassanein KM, Stolov WC, Fujimoto WY, Rubner DE. Further studies on the electrodiagnosis of diabetic peripheral polyneuropathy using discriminant function analysis. Am J Phys Med Rehabil 1994;73(2):116-123.
5. Jackson D, Clifford JC. Electrodiagnosis of mild carpal tunnel syn-drome. Arch Phys Med Rehabil 1989;70:199-204.
6. American Association of Electrodiagnostic Medicine. Literature review of the usefulness of nerve conduction studies in needle electromyography for the evaluation of patients with carpal tunnel syndrome. Muscle Nerve 1999;22 (supplement 8):S145-S167.
7. Robinson LR, Micklesen PJ, Wang L. Optimizing the number of tests for carpal tunnel syndrome. Muscle Nerve 2000;23:1880-1882.
8. Lew H, Wang L, Robinson LR. Test retest repeatability of the combined sensory index. Muscle Nerve Test-retest reliability of combined sensory index: implications for diagnosing carpal tunnel syndrome. Muscle Nerve 2000;23(8):1261-1264.
9. Bland JM, Altman DG. Statistical methods for assessing agree-ment between two methods of clinical measurement. Lancet 1986;1(8476):307-310.
10. Wee AS. Needle electromyography in carpal tunnel syndrome. Electromyogr Clin Neurophysiol 2002;42(4):253-256.
11. Jablecki et al., 2002b C.K. Jablecki, M.T. Andary, M.K. Floeter, R.G. Miller, C.A. Quartly, M.J. Vennix and J.R. Wilson, Second AAEM literature review of the usefulness of nerve conduction studies and needle electromyography for the evaluation of patients with carpal tunnel syndrome. Muscle Nerve 2002;26:S1-S53.
12. Schrijver HM, Gerritsen AA, Strijers RL, et al. Correlating nerve conduction studies and clinical outcome measures on carpal tunnel syndrome: lessons from a randomized controlled trial. J Clin Neurophysiol 2005 Jun;22(3):216-221.
13. Melvin JL, Johnson EW, Duran R. Electrodiagnosis after surgery for the carpal tunnel syndrome. Arch Phys Med Rehabil 1968;49:502-507.
6 Electrophysiologic Testing in Generalized Weakness AANEM Course

AANEM Course Carpal Tunnel Syndrome From A to Z 7 7
For many electromyography (EMG) laboratories in North America the diagnosis of carpal tunnel syndrome (CTS) is the most common referral. Although CTS is thought of as the compression of the median nerve as it travels through the carpal tunnel it is better defined as the signs and symptoms resulting from that compression. Patients will complain of numbness or paresthesia, pain, and occa-sionally weakness in the median nerve distribution.
CLINICAL PRESENTATION OF CARPAL TUNNEL SYNDROME
Epidemiology and Risk Factors
CTS is a common disorder occurring in up to 5% of the general population.1,2 The ratio of CTS in women is 3:1 as compared to men.1,3
There has probably never been a good study to compare the fre-quency of CTS in the industrial setting to the general population, but as a general rule CTS is thought to have a higher incidence in the settings where there is excessive and forceful movements of the hands and wrists. Most of the occupational studies did not use nerve conduction testing and factors relating to secondary gain typically were not well controlled. In one report, 432 workers were followed for about 5 years and the incidence of CTS was 12.4 cases per 1000 workers per year, with an average annual incidence rate of 1.2%.4
Thus, the role of repetitive hand/wrist use and workplace factors in the development of CTS remains controversial.
A number of conditions have been found to predispose individuals to CTS:
1. Gender. As noted women are affected more than men. One pos-sible explanation for the female predominance is anatomic. The cross sectional area of the proximal carpal tunnel is smaller in women than in men. Furthermore, women with CTS may have smaller cross sectional areas than control women without CTS.5
2. Obesity. This is likely a risk factor. The prevalence of CTS appears to be highest in obese women, and lowest in thin and normal-sized men.6
3. Pregnancy. The increased frequency of CTS in pregnancy likely is due to the accumulation of fluid.7
4. Diabetes. The increased frequency of CTS in diabetes prob-ably is the result of swelling and pressure at the carpal tunnel. Anything that interferes with blood flow to the hands, causes nerve issues, or affects soft tissue increases the risk of developing CTS. Diabetes causes all of these effects.8
5. Rheumatoid arthritis. One study reported that up to one-third of patients with acromegaly have median nerve compression that is frequently bilateral.9 These findings probably are due to soft tissue enlargement (synovial edema and tendon hyperplasia).
6. Hypothyroidism. The increased frequency of CTS in hypothy-roidism probably is due to swelling of membranes that compress the median nerve.10
Carpal Tunnel Syndrome from A to Z
Jim Lewis, R.NCS.T.Nerve Conduction Technologist
Hennepin County Medical CenterMinneapolis, Minnesota
Carrie E. Ford, R.NCS.T., R. EP T.Electroneurodiagnostic Technologist
Neuroscience LaboratoryBirmingham, Alabama
Janet K. James, R. EEG T., R.NCS.T.EMG Laboratory Manager
White-Wilson Medical CenterNavarre, Florida

8 Carpal Tunnel Syndrome from A to Z AANEM Course
7. Connective tissue diseases. The increased frequency of CTS in con-nective tissue diseases (i.e., rheumatoid arthritis, lupus, sarcoidosis, and Sjogren’s syndrome) is, as with diabetes and hypothyroidism, due to soft tissue inflammation near or around the carpal tunnel.
8. Preexisting neuropathy. Individuals with a preexisting median mononeuropathy are more likely to develop CTS.4,11,12
9. Genetics. There is data to suggest that some patients have a genetic predisposition to CTS. A twin study conducted in the United Kingdom found that up to one-half of the liability for CTS in women was genetic.13 This may be because of inherited anatomic size of the carpal tunnel or familial predisposition to other medical conditions such as diabetes.
10. Occupation. As mentioned before, there is controversy regard-ing the role of workplace factors in the development of CTS. Sustained wrist or palm pressure, prolonged wrist extension and flexion, repetitive hand and wrist use, work with vibrating tools, and use of hands in cold temperatures are all possible causes or ag-gravating causes of CTS. However, there is no definitive evidence that these factors play a role in the development of CTS. One possible reason is that some patients have one or more risk factors (i.e., obesity and diabetes) in addition to the industrial factors so it is difficult to weigh the impact of the workplace in relation to the other factors. Most studies do not support computer use and/or clerical duties as a risk of developing CTS.4,12,14-16
11. Other factors. There are limited and conflicting data with regard to the potential association of age,12,14 estrogen-progestin oral contraceptive use,2,17-20 and smoking20-22 with CTS. For unclear reasons, studies of American workers consistently report higher risk estimates of CTS than studies published elsewhere.23
Pathophysiology
There are several functional changes that come with CTS. Certainly, increased pressure in the intracarpal canal plays a key role in the de-velopment of clinical CTS.24
It is not known exactly why the tunnel pressure increases in CTS, but experiments point to anatomic compression and/or inflamma-tion. The nerve can be injured as a result of this increased pressure, whether it is impairment of axonal transport or nerve ischemia as a result of compression of the vessels in the perineurium.25
Upper extremity posture also influences carpal tunnel pressure. The lowest carpal tunnel pressure is seen when the wrist is in a neutral or slightly flexed position, and it increases proportionately with devia-tion from this posture.26-30
The natural way humans curl their wrists in sleep, thus increasing the pressure in the carpal tunnel, may explain why patients wake at night with paresthesias.
A deformity which reflects the relative thinning of the nerve beneath the transverse carpal tunnel ligament and swelling of the nerve in
more distal and proximal segments (“hour glass” deformity) seen in surgical reports4 can be explained by the edema and thickening of vessel walls within the endoneurium and perineurium, myelin thin-ning, and nerve fiber degeneration and regeneration.26,31,32
Clinical Presentation
Pain and/or paresthesia (numbness and tingling) in a distribution that includes the median nerve territory, with involvement of the first three digits and the lateral half of the fourth digit are the predominant symptoms (see Fig. 1). Typically these symptoms are worse at night and often awaken patients from sleep. Some patients feel the need to shake or wring their hands or place them under warm running water to return to sleep.33
Although the sensory symptoms of CTS are usually limited to the median-innervated fingers, there are some subjective differences. The pain and paresthesia may be localized to the wrist or additionally involve the ulnar and radial portions of the hand. It is not uncom-mon for sensory symptoms to radiate proximally into the forearm, or even occasionally radiate above the elbow to the shoulder.33
Many daily activities that involve flexing or extending the wrist or raising the arms, such as driving, reading, typing, and holding a telephone exacerbate these symptoms.33,34
Figure 1 Pain and/or parethesia distribution in carpal tunnel syndrome.

AANEM Course Carpal Tunnel Syndrome From A to Z 9
Sixty-five percent of patients have CTS bilaterally. Symptoms begin-ning in the dominant hand are most common and some patients do not even realize they have CTS in both hands.33
The clinical course of CTS may follow an alternating pattern with periods of remission and exacerbation.35 In some cases, there is progression from intermittent to persistent sensory complaints in the hand as CTS worsens, and later to the development of motor symptoms in the hand.
In more severe cases of CTS, motor involvement leads to complaints of weakness or clumsiness when using the hands, such as difficulty holding objects, turning keys or doorknobs, buttoning clothing, or opening jar lids.33 Clinical signs may include weakness of thumb abduction and opposition and atrophy of the thenar eminence.
Sensation over the thenar eminence is spared in CTS. This pattern occurs because the palmar sensory cutaneous nerve arises proximal to the wrist and passes over, rather than through, the carpal tunnel.
DIFFERENTIAL DIAGNOSIS OF HAND NUMBNESS AND WEAKNESS
Cervical Radiculopathy
Cervical radiculopathy is a dysfunction of the nerve root(s) in the cervical spine. Disc hernination or injuries are the most common causes in the younger population. Foraminal narrowing from osteo-phyte formation and degenerative changes are the most common causes of radiculopathy in the older population. There are seven cer-vical vertebra and eight cervical roots. Roots one through seven exit above their corresponding vertebra and the eighth cervical root exits below the seventh cervical vertebra. The seventh cervical root is the most common radiculopathy with C6 as second most common.
The sensory innervations of the median nerve in the hand originate from C6 and C7, while the motor innervations in the hand originate from C8 and T1 nerve roots. A patient may have subjective sensory changes in the thumb and index from either a C6 radiculopathy or CTS, while sensory changes in the long and ring fingers could be signs of a C7 radiculopathy or CTS. Muscle weakness or atrophy can be a result of CTS or could be a C8 or T1 radiculopathy.
While a thorough clinical examination will differentiate between cer-vical radiculopathies and CTS, the nerve conduction study (NCS)/needle EMG is the gold standard. Some differences between cervical radiculopathy and CTS include:
Cervical radiculopathy does not present with nocturnal pain •and paresthesias.In C6-C7 radiculopathy the sensory NCSs are normal; sensory •NCSs of the digits is abnormal in CTS. In cervical radiculopa-thy of C6-C7, the intrinsic hand muscles are not affected due to C8-T1 innervations.Cervical radiculopathy usually causes neck and shoulder pain •and restricted neck movements in acute radiculopathy.
In cervical radiculopathy, paresthesias are usually limited to one •side, whereas in CTS they are often bilateral. Root compression maneuvers may elicit paresthesias in radiculopathy.
Brachial Plexus Lesions
The brachial plexus is located between the neck and axilla and is an anatomic structure formed by the anterior (ventral) rami of the lower cervical and upper thoracic nerve roots. The various fascicles from these nerve roots are intermixed and eventually separate again into the nerves into the arm.36 The brachial plexus is formed by five roots (C5, C6, C7, C8, and T1) divided into three trunks (upper, middle, and lower), two divisions (anterior and posterior), three cords (lateral, posterior, and medial), and finally five nerves (muscu-locutaneous, axillary, radial, median, and ulnar).
In lesions of the upper or middle trunk and lateral cord, sensation to the thumb through the ring finger can be altered. In lesions of the lower trunk and medial cord atrophy of the thenar muscles can be seen. There is not, however, a single lesion in the brachial plexus that can cause paresthesias to the lateral four fingers and weakness in the thenar muscles.
While a thorough clinical examination will differentiate between brachial plexus lesions and CTS, the NCS/needle EMG is the gold standard. Some differences between brachial plexus lesions and CTS include:
In upper trunk and lateral cord plexopathies there can be numb-•ness in the lateral hand and thumb, but additional numbness in the lateral forearm is not seen in CTS. Additionally, muscle weakness in upper trunk plexopathies is seen in several muscles including proximal muscles that would not be seen in CTS. Sensory studies would likely be abnormal to the thumb and index in upper trunk plexopathies, but spared in the long finger, whereas in CTS the long finger, because of fascicular involve-ment, is often the most affected.37
Middle trunk plexopathies are rare. Muscle weakness would be •apparent in the triceps and numbness would be confined to the third digit. In CTS numbness would be more widespread to the lateral four digits.37
Posterior cord plexopathies can have hand numbness in the •radial dorsum of the hand, which could look like CTS, but in addition the posterior cord would demonstrate numbness in the posterior arm and forearm, which would not be characteristic of CTS.37
Plexopathies involving the lower trunk and medial cord can lead •to weakness and subsequent atrophy of the thenar muscles, but paresthesias are confined to the ulnar innervated medial half of the ring finger and little finger. The numbness extends up the forearm in the medial antebrachial cutaneous territory which would not be seen in CTS.37
Ulnar Neuropathy
The ulnar nerve arises from the C8 and T1 nerve roots and continues through the lower trunk and medial cord. It continues through the epicondylar groove and on to the wrist where it innervates the hy-

10 Carpal Tunnel Syndrome from A to Z AANEM Course
pothenar and some dorsal and volar interosseous muscles. Sensation to the medial half of the forth digit and the fifth digit are the respon-sibility of the ulnar nerve.
There is a subjective nature when describing numbness secondary to CTS that often will include all fingers or the entire hand. Careful attention should be paid as to not miss an ulnar neuropathy in ad-dition to, or instead of, the CTS. In CTS the ulnar NCSs should be unaffected and it is a useful nerve for comparison studies.
Overuse Syndromes
Overuse syndrome (sometimes called repetitive stress disorder) is a condition in which a part of the body is injured by repeatedly overus-ing or exerting too much strain on that body part.
The term overuse syndrome identifies a large group of conditions that result from using the body in a repetitious way and causing injury by the amount it is done. These conditions are often focused on a joint and usually affect the muscle, bone, tendon, or bursa of the joint. However other anatomical features and areas can be stressed and their response to that strain can be an injury.38
Some common examples of overuse syndrome include:Tendonitis•Bursitis•Tennis elbow•Trigger finger•Blackberry thumb•Vibration white finger•
Each of these conditions can cause chronic pain and even disability. Sometimes the pain will even seem to follow the course of a nerve and is often mistaken as CTS. Seldom does a patient characterize numbness as they might in CTS. A detailed history and physical examination usually will prove an overuse syndrome and will include localized tenderness and pain with related movements. The NCSs should be unaffected in overuse syndromes. Often activity modifica-tion, splinting, and physical therapy will help patients with overuse syndromes.
Diagnostic Methods to Detect Other Lesions
While the NCS proves to be the industry standard for nerve entrap-ments, such as CTS, they do not have a high yield in musculoskel-etal conditions. X-rays can be useful when focusing on joint spaces. Magnetic resonance imaging (MRI) studies may be useful, especially if surgery is considered. Musculoskeletal ultrasound, likewise, can be useful before considering surgery for overuse syndromes.
NERVE CONDUCTION STUDIES FOR DIAGNOSIS OF CARPAL TUNNEL SYNDROME
Sensory Nerve Conduction Studies
There are several techniques used to evaluate CTS. Sensory tech-niques used in the diagnosis of CTS include:
Median conduction study from digit to wrist•Comparison of median and ulnar sensory (mixed) nerve con-•duction between wrist and palm (transcarpal technique)Median to radial latency difference from the thumb (“numb •thumb” technique)Median to ulnar latency difference from the ring finger•Short segment stimulation across the carpal tunnel (inching •technique)Cumulative summary index (CSI or Robinson index)•Median palm to wrist comparison (7 and 14 cm technique)•Others•
Median Conduction Study from Digit to Wrist
Median conduction study from digit to wrist is used regardless if the investigation is for CTS or some other reason, thus it is the standard study. When using this technique, patient recorded values are com-pared to laboratory normal values for latency, amplitude, and some-times conduction velocity. Orthodromic or antidromic techniques are equally reliable based on preference. It is critical, when using peak latency (verses conduction velocity) that a fixed distance be used; 13 or 14 cm are appropriately long enough distances to encompass the carpal tunnel from the digits.39
The antidromic technique to the index finger (see Fig. 2) is as follows:
Patient position Supine with arm extended at side
Skin preparation Abrade with alcohol or commercially available preparation and check tem perature as laboratory protocols dictate
13 or 14 cm
Figure 2 Median conduction study from digit to wrist (antidromic tech-nique from the index finger).

AANEM Course Carpal Tunnel Syndrome From A to Z 11
Recording site Active Ring electrode placed on the midportion of the proximal phalanx of the index finger
Reference Ring electrode placed on the midportion of the middle phalanx of the index finger
Ground Placed between the stimulating and recording electrodes on the dorsum of the hand
Stimulation Wrist Applied at 13 or 14 cm proximal to the recording electrode between the flexor carpi radialis (FCR) and palmaris longus (PL) tendons
Measurements Between active recording electrode and wrist; latency and amplitude for sensory nerve action potential (SNAP)
Calculations Sensory conduction velocity
The orthodromic technique from the index finger (see Fig. 3) is as
follows:
Patient position Supine with arm extended at side
Skin preparation Abrade with alcohol or commercially available preparation and check temperature
Recording site Active Placed at 13 or 14 cm proximal to the recording electrode between the FCR and PL tendons
Reference Placed 3 cm proximal to the recording electrode
Ground Placed between the stimulating and recording electrodes on the dorsum of the hand
Stimulation Wrist Applied ring electrode on midportion of the proximal phalanx of the index finger
Measurements Between active recording electrode and wrist; latency and amplitude for SNAP
Comparison of Median and Ulnar Sensory (Mixed) Nerve Conduction between Wrist and Palm (Transcarpal Technique)
Comparison of median and ulnar sensory nerve conduction between wrist and palm is a widely used technique. It is only used for the diagnosis of CTS and is a quick and easy comparison study. The main useful value is the peak difference between the median and ulnar recordings. Values vary between laboratories and may be 0.3 to 0.5 ms. As with any comparison, a carefully measured fixed dif-ference is important; usually 8 cm in this technique. Also, as with most comparison techniques, temperature is not as big a factor since there is less concern about absolute measurements and both nerves would be affected by the temperature equally. This technique (see Fig. 4) follows:
Patient position Supine with arm supinated and extended at side
Skin preparation Abrade with alcohol or commercially available preparation and check temperature
Median recording site Active Placed 2 cm proximal to the distal wrist crease between the FCR and PL tendons
Reference Placed 3 cm proximal to the active recording electrode along the median nerve
Ground Placed between the recording and stimulating electrodes on the dorsum of the hand
Stimulation Cathode/anode Applied 8 cm distal to the active recording electrode between the index and third digit. Anode is 2 cm distal to the cathode
Ulnar recording site Active Placed 2 cm proximal to the distal wrist crease, just anterior to the flexor carpi ulnaris (FCU) tendon
13 or 14 cm
Figure 3 Median conduction study from digit to wrist (orthodromic tech-nique from the index finger).

12 Carpal Tunnel Syndrome from A to Z AANEM Course
Reference Placed 3 cm proximal to the active re- cording electrode along the ulnar nerve
Ground Placed between the stimulating and recording electrodes on the dorsum of the hand
Stimulation Cathode/anode Applied 8 cm distal to the active recording electrode between the fourth and fifth digit. Anode is 2 cm distal to the cathode
Measurements Distance between active recording electrode and cathode; latency and amplitude of SNAP
Calculations Latency difference between the two nerves
Median to Radial Latency Difference from the Thumb (“Numb Thumb” Technique)
Median to radial latency difference from the thumb uses the radial nerve as a comparison. It is useful when an ulnar lesion is suspected. The main useful value is the peak difference between the median and radial recordings. Values vary between laboratories and may be 0.3 to 0.5 ms. As with any comparison, a carefully measured fixed dif-ference is important; usually 10 cm in this technique. Also, as with most comparison techniques, temperature is not as big a factor since there is less concern about absolute measurements and both nerves would be affected by the temperature equally. This technique (Fig. 5) follows:
Patient position Supine with arm pronated and extended at side
Skin preparation Abrade with alcohol or commercially available preparation and check temperature
Recording site Active Ring electrode placed on the midportion of the proximal phalanx of the thumb
Reference Ring electrode placed on the midportion of the distal phalanx of the thumb
Ground Placed between the stimulating and recording electrodes on the dorsum of the hand
Stimulation Median Applied 10 cm proximal to the recording electrode in the wrist between the FCR and PL tendons
Radial Applied 10 cm proximal to the recording electrode over the dorsolateral aspect of the radius
Measurements Between active recording electrode and wrist; latency and amplitude for SNAP. Latency difference between the two sites
8 cm
8 cm
Figure 4 Comparison of median and ulnar sensory (mixed) nerve conduc-tion between wrist and palm (transcarpal technique).
Figure 5 Median to radial latency difference from the thumb (“numb thumb” technique).
10 cm – Median
10 cm – Radial

AANEM Course Carpal Tunnel Syndrome From A to Z 13
Calculations None required, although some may calculate the conduction velocity (CV) from cathode to recording electrode
Median to Ulnar Latency Difference from the Ring Finger
Median to ulnar latency difference from the ring finger is one of the oldest and most specific comparison studies for CTS. The author does not use it as often because it involves the patient taking off rings that may have been in place for years. The main useful value is the peak difference between the median and radial recordings. Values vary between labs and may be 0.3 to 0.5 ms. As with any comparison, a carefully measured fixed difference is important; usually 12-14 cm in this technique. Also, as with most comparison techniques, temperature is not as big a factor since there is less concern about absolute measurements and both nerves would be affected by the temperature equally. This technique (see Fig. 6) follows:
Patient position Supine with arm pronated and extended at side
Skin preparation Abrade with alcohol or commercially available preparation and check temperature
Recording site Active Ring electrode placed on the midportion of the proximal phalanx of the ring finger
Reference Ring electrode placed on the midportion of the middle phalanx of the ring finger
Ground Placed between the stimulating and recording electrodes on the dorsum of the hand
Stimulation Median Applied 12 cm proximal to the recording electrode in the wrist between the FCR and PL tendons
Ulnar Applied 12 cm proximal to the recording electrode in the wrist anterior to the FCU tendon
Measurements Between active recording electrode and wrist. Latency and amplitude for SNAP. Latency difference between the two sites
Calculations None required, although some may calculate the CV from cathode to re cording electrode
Short Segment Stimulation across the Carpal Tunnel (Inching Technique)
Short segment stimulation across the carpal tunnel, first described by Kimura, helps localize the exact location of the entrapment in CTS. It uses sequential antidromic stimulation of the median sensory nerve at 1-cm intervals across the carpal tunnel recording to the index finger. In Kimura’s reports this technique localized the abnormality of median sensory conduction in most CTS pa-tients to the distal edge of the carpal ligament. Look for a sharply localized latency increase across the 1 cm segments.40 This is the technique (see Fig. 7):
Patient position Supine with arm pronated and extended at side
Skin preparation Abrade with alcohol or commercially available preparation and check temperature
Figure 6 Median to ulnar latency difference from the ring finger.
12 cm – Median
12 cm – Ulnar
Figure 7 Short segment stimulation across the carpal tunnel (inching technique).

Recording site Active Ring electrode placed on the midportion of the proximal phalanx of the index finger
Reference Ring electrode placed on the midportion of the middle phalanx of the index finger
Ground Placed between the stimulating and recording electrodes on the dorsum of the hand
Stimulation Start at the “zero” mark (corresponds to the origin of the transverse carpal ligament) at the distal crease of the wrist and make a mark, then mark five 1 cm increments both proximal and distal to this “zero” mark; stimulate these 11 positions, starting distal and moving proximal
Measurements Look for segmental changes in latency or amplitude that is asymmetrical as compared to the others segments
Cumulative Summary Index (CSI or Robinson Index)
The CSI is a combination of three sensory conduction comparison studies that adds reliability and sensitivity to the CTS study. It is gener-ally recommended that abnormal results should be found through two methods before making the diagnosis of CTS, and when the results are clearly abnormal this is simple to do. When the results are borderline, however, the CSI can identify normal or abnormal results by adding together the results of the three techniques: transcarpal, ring finger comparison, and median to radial thumb comparison. This method provides a statistical advantage when a single study is borderline. The reliability of diagnosis can be 95% using the CSI. Dr. Robinson recom-mends the lower limits of normal be 1.0 ms.41 Here is an example:
Transcarpal median to ulnar difference 0.3 ms
Ring finger median to ulnar difference 0.4 ms
Thumb median to radial difference 0.4 ms
= 1.1 ms (positive for CTS)
Median Palm to Wrist Comparison (7 and 14 cm technique)
Median palm to wrist comparison is a useful technique when a patient has an underlying peripheral neuropathy. It can separate out the peripheral neuropathy and place the focus on the CTS.
Place the recording electrodes on the index or middle finger and measure up 7 cm into the palm and an additional 7 cm (14 cm total) to the wrist. Record waveforms at both sites and compare velocity or latency of the distal segment (palm to finger) with the proximal segment (wrist to palm). If it is slower across the carpal tunnel than it
is in the distal segment, it suggests the slowing is because of the carpal tunnel rather than the peripheral neuropathy. See Figure 8.
Motor Nerve Conduction Studies
The motor conduction techniques used in the diagnosis of CTS include:
Median motor distal latency•Median motor conduction study between wrist and palm•Median, 2nd lumbrical comparison to ulnar 2nd dorsal in-•terosseous (2L2IO)Median thenar to ulnar thenar latency difference (TTLD)•Median thenar to ulnar hypothenar latency difference (THLD)•
Median Motor Distal Latency
Median motor distal latency is the “standard” median motor record-ing performed in most EMG laboratories. A fixed distance of 6 to 8 cm is used and the distal latency value is compared to the normal values. This technique (see Fig. 9) follows:
Patient position Supine with arm supinated and extended at side
Skin preparation Abrade with alcohol or commercially available preparation and check temperature
7 cm
14 cm
Figure 8 Median palm to wrist comparison (7 and 14 cm technique).
14 Carpal Tunnel Syndrome from A to Z AANEM Course

AANEM Course Carpal Tunnel Syndrome From A to Z 15
Recording site Active Placed over the belly of the abductor pollicis brevis (APB), half the distance between the metacarpophalangeal (MCP) joint of thumb and the mid point of the distal wrist crease; occa sionally this needs to be moved to obtain an initial negative deflection
Reference Placed on the distal phalanx of the thumb
Ground Placed between the stimulating and recording electrodes
Stimulation Wrist Applied 6-8 cm proximal to the recording electrode between the FCR and the PL tendons
Elbow Applied at the elbow crease, just medial to biceps tendon
Measurements Between active recording electrode and wrist.; between wrist and elbow; latency and amplitude for compound muscle action potential (CMAP) recordings
Calculations CV wrist to elbow
Median Motor Conduction Study between the Wrist and Palm
Median motor conduction study between the wrist and palm in-cludes stimulating the recurrent motor branch of the median nerve in the palm and calculating velocity across the carpal ligament. Looking at the CMAP amplitude ratio below and above the carpal tunnel may be useful, as well. The median motor response is recorded over the APB with stimulation of the median nerve at the wrist. Stimulation in the palm makes it possible to identify median motor nerve con-duction slowing or block across the carpal tunnel. The technique is
technically difficult because simultaneous stimulation of the ulnar nerve in the palm can alter the CMAP amplitude or change the CV, which, over the short distance, can be misleading.39 This technique (see Fig. 10) follows:
Patient position Supine with arm supinated and extended at side
Skin preparation Abrade with alcohol or commercially available preparation and check temperature
Recording site Active Placed over the belly of the APB, half the distance between the metacarp- phalangeal (MCP) joint of thumb and the midpoint of the distal wrist crease; occasionally this needs to be moved to obtain an initial negative deflection
Reference Placed on the distal phalanx of the thumb
Ground Placed between the stimulating and recording electrodes
Figure 9 Median motor distal latency.
Figure 10 Median motor conduction study between wrist and palm.

Stimulation Palm Applied at the point in the palm where the middle finger touches the lifeline
Wrist Applied 6-8 cm proximal to the recording electrode between the FCR and the PL tendons
Measurements Between palm and wrist; latency and amplitude for CMAP recordings
Calculations CV palm to wrist
Median, Second Lumbrical Comparison to Ulnar Second Dorsal Interosseous (2L2IO)
The median 2L2IO technique (see Fig. 11) is useful when no median response can be elicited from sensory comparison studies.
Patient position Supine with arm supinated and extended at side
Skin preparation Abrade with alcohol or commercially available preparation and check temperature
Recording parameters Motor NCS
Filters: 2 Hz-10k Hz, or as your laboratory standards dictate Timebase/sweep speed: 2 or 5 ms/div Gain/sensitivity: 5 mV/div (starting point)
Recording site (the same for both median and ulnar)
Active Placed between the 2nd and 3rd metacarpal bones in the palm of the hand
Reference Distally over the proximal interphalange joint (PIP) of the 2nd or 3rd digit
Ground Placed between the recording and stimulating electrodes or on the dorsum of the hand
Median stimulation Cathode/anode: Applied 10 cm distal to the active recording electrode in the middle of the wrist between the flexor carpi radialis tendon and the palmaris longus tendon.
Ulnar stimulation Cathode/anode Applied 10 cm distal to the active recording electrode in the medial portion of the wrist along side the flexor carpi ulnaris tendon
Stimulation parameters Motor NCS
Stimulus duration: 0.05 ms (50 µs) or as necessary
Intensity: enough to acquire supramaximal amplitude
Measurements Latency and amplitude of CMAP
Calculations Latency difference between the two nerves
Median Thenar to Ulnar Thenar Latency Difference (TTLD)
The median TTLP technique is a simple motor comparison study. Simply leave the recording electrodes over the thenar eminence after the routine median motor study and stimulate the ulnar nerve 1 cm proximal to the distal wrist crease. Remember the flexor pollicis brevis (one of the three thenar muscles) has ulnar innervation. The onset will be positive and the latency should be taken from this point. If the latency difference is more than 1.4 ms, with median stimula-tion being more prolonged, consider CTS.42
Figure 11 Median, 2nd lumbrical comparison to ulnar 2nd dorsal in-terosseous (2L2IO).
16 Carpal Tunnel Syndrome from A to Z AANEM Course
AANEM Course Carpal Tunnel Syndrome From A to Z 17
Median Thenar to Ulnar Uypothenar Latency Difference (THLD)
The THLD method is straightforward and calculates the difference (THLD) between the distal latency of the CMAP recorded over the APB with median nerve stimulation at the wrist and the distal latency of the CMAP recorded over the abductor digiti minimi (ADM) with ulnar nerve stimulation at the wrist.39 In the author’s laboratory, they use the normal value of < 1.8 ms where the median latency is greater.
PITFALLS
Temperature
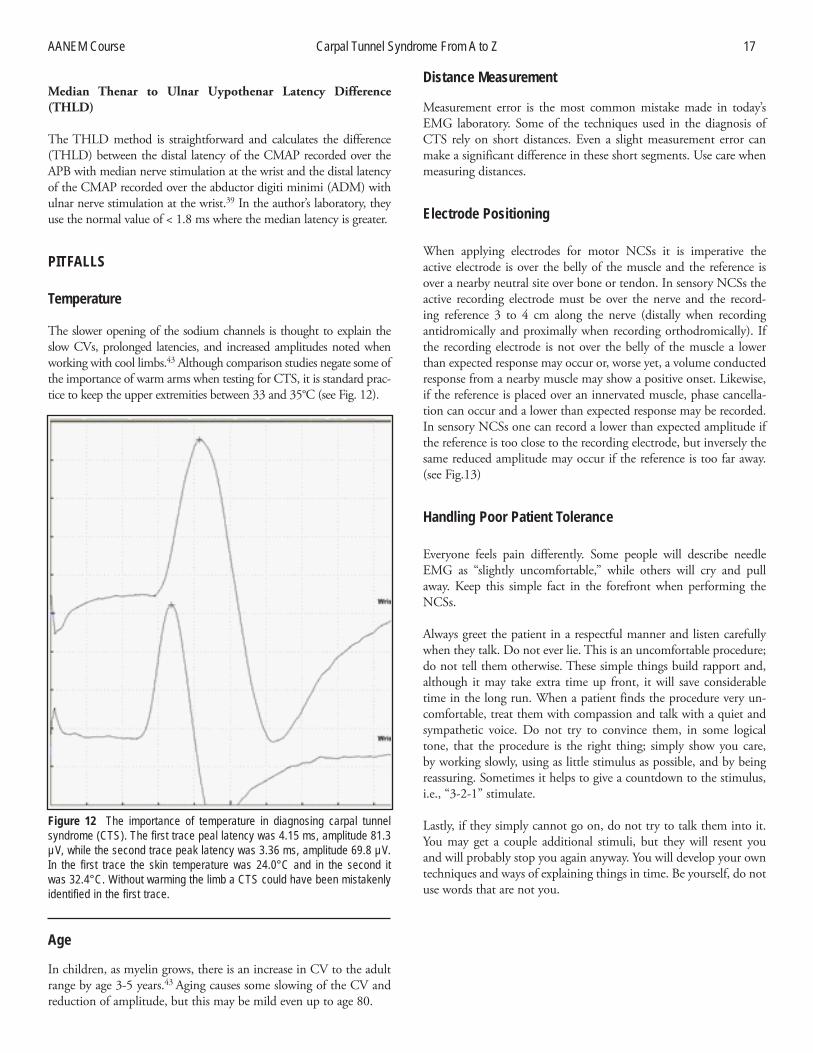
The slower opening of the sodium channels is thought to explain the slow CVs, prolonged latencies, and increased amplitudes noted when working with cool limbs.43 Although comparison studies negate some of the importance of warm arms when testing for CTS, it is standard prac-tice to keep the upper extremities between 33 and 35°C (see Fig. 12).
Age
In children, as myelin grows, there is an increase in CV to the adult range by age 3-5 years.43 Aging causes some slowing of the CV and reduction of amplitude, but this may be mild even up to age 80.
Distance Measurement
Measurement error is the most common mistake made in today’s EMG laboratory. Some of the techniques used in the diagnosis of CTS rely on short distances. Even a slight measurement error can make a significant difference in these short segments. Use care when measuring distances.
Electrode Positioning
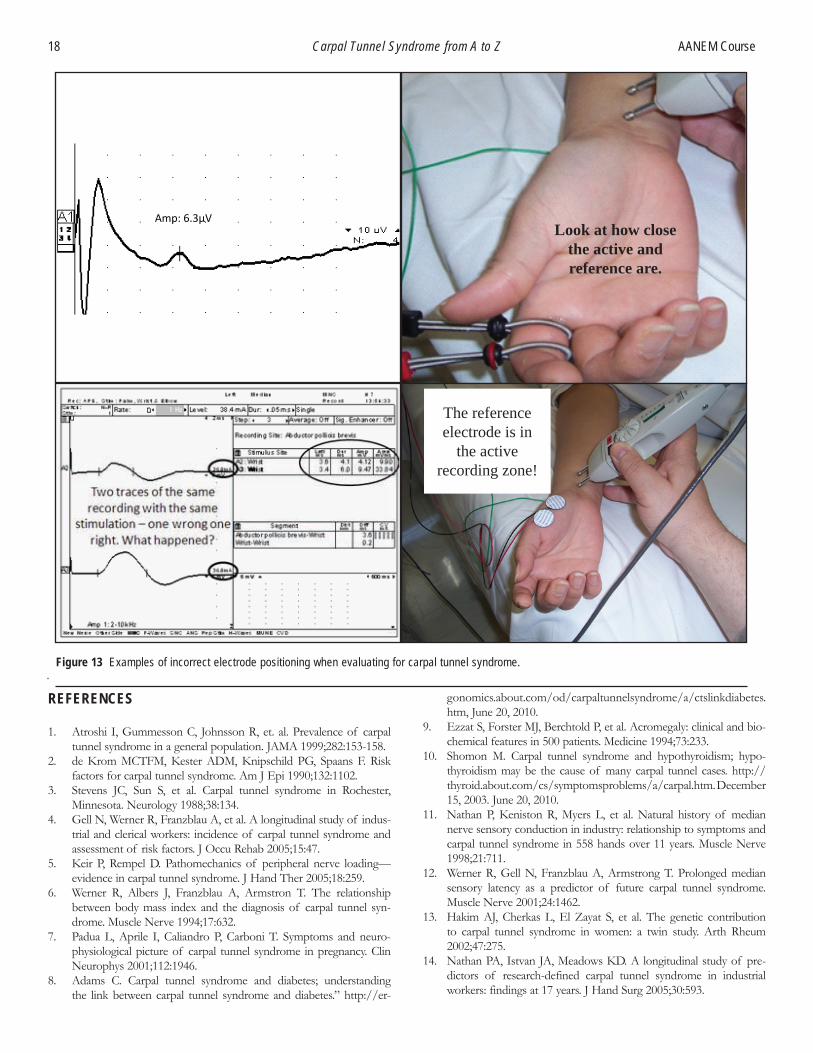
When applying electrodes for motor NCSs it is imperative the active electrode is over the belly of the muscle and the reference is over a nearby neutral site over bone or tendon. In sensory NCSs the active recording electrode must be over the nerve and the record-ing reference 3 to 4 cm along the nerve (distally when recording antidromically and proximally when recording orthodromically). If the recording electrode is not over the belly of the muscle a lower than expected response may occur or, worse yet, a volume conducted response from a nearby muscle may show a positive onset. Likewise, if the reference is placed over an innervated muscle, phase cancella-tion can occur and a lower than expected response may be recorded. In sensory NCSs one can record a lower than expected amplitude if the reference is too close to the recording electrode, but inversely the same reduced amplitude may occur if the reference is too far away. (see Fig.13)
Handling Poor Patient Tolerance
Everyone feels pain differently. Some people will describe needle EMG as “slightly uncomfortable,” while others will cry and pull away. Keep this simple fact in the forefront when performing the NCSs.
Always greet the patient in a respectful manner and listen carefully when they talk. Do not ever lie. This is an uncomfortable procedure; do not tell them otherwise. These simple things build rapport and, although it may take extra time up front, it will save considerable time in the long run. When a patient finds the procedure very un-comfortable, treat them with compassion and talk with a quiet and sympathetic voice. Do not try to convince them, in some logical tone, that the procedure is the right thing; simply show you care, by working slowly, using as little stimulus as possible, and by being reassuring. Sometimes it helps to give a countdown to the stimulus, i.e., “3-2-1” stimulate.
Lastly, if they simply cannot go on, do not try to talk them into it. You may get a couple additional stimuli, but they will resent you and will probably stop you again anyway. You will develop your own techniques and ways of explaining things in time. Be yourself, do not use words that are not you.
Figure 12 The importance of temperature in diagnosing carpal tunnel syndrome (CTS). The first trace peal latency was 4.15 ms, amplitude 81.3 µV, while the second trace peak latency was 3.36 ms, amplitude 69.8 µV. In the first trace the skin temperature was 24.0°C and in the second it was 32.4°C. Without warming the limb a CTS could have been mistakenly identified in the first trace.
REFERENCES
1. Atroshi I, Gummesson C, Johnsson R, et. al. Prevalence of carpal tunnel syndrome in a general population. JAMA 1999;282:153-158.
2. de Krom MCTFM, Kester ADM, Knipschild PG, Spaans F. Risk factors for carpal tunnel syndrome. Am J Epi 1990;132:1102.
3. Stevens JC, Sun S, et al. Carpal tunnel syndrome in Rochester, Minnesota. Neurology 1988;38:134.
4. Gell N, Werner R, Franzblau A, et al. A longitudinal study of indus-trial and clerical workers: incidence of carpal tunnel syndrome and assessment of risk factors. J Occu Rehab 2005;15:47.
5. Keir P, Rempel D. Pathomechanics of peripheral nerve loading—evidence in carpal tunnel syndrome. J Hand Ther 2005;18:259.
6. Werner R, Albers J, Franzblau A, Armstron T. The relationship between body mass index and the diagnosis of carpal tunnel syn-drome. Muscle Nerve 1994;17:632.
7. Padua L, Aprile I, Caliandro P, Carboni T. Symptoms and neuro-physiological picture of carpal tunnel syndrome in pregnancy. Clin Neurophys 2001;112:1946.
8. Adams C. Carpal tunnel syndrome and diabetes; understanding the link between carpal tunnel syndrome and diabetes.” http://er-
gonomics.about.com/od/carpaltunnelsyndrome/a/ctslinkdiabetes.htm, June 20, 2010.
9. Ezzat S, Forster MJ, Berchtold P, et al. Acromegaly: clinical and bio-chemical features in 500 patients. Medicine 1994;73:233.
10. Shomon M. Carpal tunnel syndrome and hypothyroidism; hypo-thyroidism may be the cause of many carpal tunnel cases. http://thyroid.about.com/cs/symptomsproblems/a/carpal.htm. December 15, 2003. June 20, 2010.
11. Nathan P, Keniston R, Myers L, et al. Natural history of median nerve sensory conduction in industry: relationship to symptoms and carpal tunnel syndrome in 558 hands over 11 years. Muscle Nerve 1998;21:711.
12. Werner R, Gell N, Franzblau A, Armstrong T. Prolonged median sensory latency as a predictor of future carpal tunnel syndrome. Muscle Nerve 2001;24:1462.
13. Hakim AJ, Cherkas L, El Zayat S, et al. The genetic contribution to carpal tunnel syndrome in women: a twin study. Arth Rheum 2002;47:275.
14. Nathan PA, Istvan JA, Meadows KD. A longitudinal study of pre-dictors of research-defined carpal tunnel syndrome in industrial workers: findings at 17 years. J Hand Surg 2005;30:593.
18 Carpal Tunnel Syndrome from A to Z AANEM Course
Amp: 6.3µV
Figure 13 Examples of incorrect electrode positioning when evaluating for carpal tunnel syndrome.
Look at how close the active and reference are.
The reference electrode is in
the active recording zone!

AANEM Course Carpal Tunnel Syndrome From A to Z 19
15. Armstrong T, Dale AM, Franzblau A, Evanoff BA. Risk factors for carpal tunnel syndrome and median neuropathy in a working popula-tion. J Occu Environ Med 2008;50:1355.
16. Thomsen JF, Gerr F, Atroshi I. Carpal tunnel syndrome and the use of computer mouse and keyboard: a systematic review. Musculoskel Disord 2008;9:134.
17. Vessey M, Villard-Mackintosh L, Yeates D. Epidemiology of carpal tunnel syndrome in women of childbearing age. Findings in a large cohort study. Internat J Epi 1990;19:655.
18. Albani G, Priano L, Campanelli L, et al. Carpal tunnel syndrome and oral contraceptive drugs: risk or protective factor? J Peri Nerv Syst 2003;8:207.
19. Sabour MS, Fadel HE. The carpal tunnel syndrome—a new compli-cation ascribed to the “pill.” Am J Obstet Gynecol 1970;107:1265.
20. Geoghegan JM, Clark DI, Bainbridge LC, et al. Risk factors in carpal tunnel syndrome. J Hand Surg 2004; 29:315.
21. Nathan PA, Meadows KD, Istvan JA. Predictors of carpal tunnel syndrome: an 11-year study of industrial workers. J Hand Surg 2002;27:644.
22. Nathan PA, Keniston RC, Lockwood RS, Meadows KD. Tobacco, caffeine, alcohol, and carpal tunnel syndrome in American indus-try. A cross-sectional study of 1464 workers. J Occu Environ Med 1996;38:290.
23. Abbas M, Afifi A, Zhang Z, Kraus J. Meta-analysis of published studies of work-related carpal tunnel syndrome. Inter J Occu Environ Health 1998;4:160.
24. Bland JD. Carpal tunnel syndrome. Curr Opin Neuro 2005;18:581.25. Amirfeyz R, Gozzard C, Leslie IJ. Hand elevation test for assessment
of carpal tunnel syndrome. Journal of Hand Surgery 2005; 30:361.26 Keir, P, Rempel, D. “Pathomechanics of peripheral nerve loading -
Evidence in carpal tunnel syndrome.” J Hand Ther 2005;18:259.27. Seradge H, Jia Y, Owens W. In vivo measurement of carpal tunnel
pressure in the functioning hand. J Hand Surg 1995;20:855.28. Szabo R, Chidgey L. Stress carpal tunnel pressures in patients
with carpal tunnel syndrome and normal patients. J Hand Surg 1989;14:624.
29. Weiss N, Gordon L, Bloom T, et al. Position of the wrist associated with the lowest carpal-tunnel pressure: Implications for splint design. J Bone Joint Surg 1995;77:1695.
30. Keir P, Wells R, Ranney D, Lavery W. The effects of tendon load and posture on carpal tunnel pressure. J Hand Surg 1997;22:628.
31. Mackinnon SE, Dellon AL, Hudson AR, Hunter DA. Chronic human nerve compression—a histological assessment. Neuropath Appl Neurobiol 1986;12:547.
32. Donato G, Galasso O, Valentino P, et al. Pathological findings in subsynovial connective tissue in idiopathic carpal tunnel syndrome. Clin Neuropath 2009;28:129.
33. Preston D, Shapiro B. Electromyography and neuromuscular disor-ders: clinical-electrophysiologic correlations, 2nd ed. Philadelphia: Elsevier; 2005. 255-278.
34. Bland JD. Carpal tunnel syndrome. Br Med J 2007;335:343.35. Muller M, Tsui D, Schnurr R, et. al. Effectiveness of hand therapy
interventions in primary management of carpal tunnel syndrome. J Hand Ther 2004;17:210.
36. Preston D, Shapiro B. Electromyography and neuromuscular disor-ders: clinical-electrophysiologic correlations, 2nd ed. Philadelphia: Elsevier; 2005. 478.
37. Preston D, Shapiro B. Electromyography and neuromuscular disor-ders: clinical-electrophysiologic correlations, 2nd ed. Philadelphia: Elsevier; 2005. 481-482.
38. Adams C. What is overuse syndrome? http://ergonomics.about.com/od/repetitivestressinjuries/f/whatisos.htm. June 20, 2010.
39. Jablecki CK, et al., eds. Practice parameter and literature review of the usefulness of nerve conduction studies and needle electromyo-graphy for the evaluation of patients with carpal tunnel syndrome. Muscle Nerve 2002;25:918-922.
40. Kimura J. Electrodiagnosis in diseases of the nerve and muscle, principles and practice, 3rd ed. Philadelphia: Oxford University Press; 2001. 137-141.
41. Robinson LR. Bringing electrodiagnosis of CTS to the next level. Electrodiagnosis and clinical neurophysiology: a high intensity review. Rehabilitation Institute of Chicago and Northwestern Feinberg School of Medicine. Chicago. 2009.
42. Williams FH, Andary MT. Carpal tunnel syndrome: techniques for diagnosis. AANEM Workshop. AANEM, Rochester, MN. 2001.
43. Kimura J. Electrodiagnosis in diseases of the nerve and muscle, principles and practice, 3rd ed. Philadelphia: Oxford University Press; 2001. 109-112.