Embed Size (px)
Citation preview

Vol. 113 No. 4 April 2012
Osteoinductive activity of biphasic calcium phosphate withdifferent rhBMP-2 doses in ratsJi-Woong Jang, DDS,a Jeong-Ho Yun, DDS, PhD,b Kwang-Il Lee, BS, MS,c Ju-Woong Jang, BS, PhD,c
Ui-Won Jung, DDS, PhD,d Chang-Sung Kim, DDS, PhD,d Seong-Ho Choi, DDS, PhD,d andKyoo-Sung Cho, DDS, PhD,d Seoul and Incheon, KoreaYONSEI UNIVERSITY, INHA UNIVERSITY, THE INSTITUTE OF BIO MATERIAL AND MEDICAL ENGINEERING
Objective. The aim of the current study was to determine whether a hydroxyapatite (HA)/beta-tricalcium phosphate (�-TCP)ratio of 20/80 impregnated with recombinant human bone morphogenetic protein (rhBMP-2) enhances new bone formationand to evaluate the dose-dependent response of rhBMP-2.Study Design. Critical-sized calvarial defects were made in rats, and biphasic calcium phosphate (BCP) with different rhBMP-2 doses was loaded into rat calvarial defects. The animals were allowed to heal for either 2 or 8 weeks.Results. The percentages of new bone after 2 and 8 weeks of healing were significantly greater in the rhBMP-2–treated groups(at all doses) than in the control groups. The percentage of remaining BCP was significantly lower at 8 weeks than at 2 weeksin all groups that included BCP.Conclusions. rhBMP-2 administered using a BCP carrier significantly induces new bone formation. A dose-dependent
response was not shown in the present study. (Oral Surg Oral Med Oral Pathol Oral Radiol 2012;113:480-487)Various bone substitutes have been used to reconstructbony defects. Autogenous bone grafts have been con-sidered the gold standard in reconstructive surgery be-cause of their osteogenic properties. Despite this ad-vantage, autogenous bone has many disadvantages,such as the limited availability of donor sites and as-sociated morbidity. On the other hand, allogeneic andxenogeneic bone grafts can be obtained easily, but theycan provoke an immune response. These limitationshave led to extensive investigation and development ofalloplastic materials. Alloplastic bone grafts are osteo-conductive and do not induce immunogenicity. Cal-cium phosphate ceramics have been investigated exten-sively because they resemble the chemical componentof human bone mineral.1 In general, hydroxyapatite(HA) is poorly bioresorbable, whereas beta-tricalciumphosphate (�-TCP) is more bioresorbable and is re-
This research was supported by the Basic Science Research Programthrough the National Research Foundation of Korea (NRF) funded bythe Ministry of Education, Science and Technology (2009-0073534).aResident, Department of Periodontology, Research Institute for Peri-odontal Regeneration, College of Dentistry, Yonsei University,Seoul, Korea.bAssistant Professor, Division of Periodontology, Department ofDentistry, School of Medicine, Inha University, Incheon, Korea.cPrincipal Researcher, Institute of Bio Material and Medical Engi-neering, Korea Bone Bank Co, Seoul, Korea.dProfessor, Department of Periodontology, Research Institute forPeriodontal Regeneration, College of Dentistry, Yonsei University,Seoul, Korea.Received for publication Feb 22, 2011; returned for revision Mar 29,2011; accepted for publication Apr 6, 2011.© 2012 Elsevier Inc. All rights reserved.2212-4403/$ - see front matter
doi:10.1016/j.tripleo.2011.04.013480
placed by new bone at a high rate.2 These propertiesmean that the rate of degradation and bioactivity can bemodulated by changing the HA/�-TCP ratio.3 Biphasiccalcium phosphate (BCP) ceramics, comprising a mix-ture of HA and �-TCP at various ratios, are known aseffective and biocompatible scaffolds. Previous studieshave shown that BCP has osteoconductive properties inspecific ratios of HA and �-TCP.4,5 Even when osteo-conduction is achieved, new bone formation is limitedowing to the lack of natural osteoinductivity. To re-solve this problem, it is necessary to combine an ap-propriate scaffold and an osteoinductive growth factor,such as bone morphogenetic protein (BMP). The opti-mal carrier to deliver recombinant human BMP 2 (rh-BMP-2) must fulfill various criteria, such as conditionsfor cellular and vascular growth, cellular attachment,biocompatibility, space maintenance, and release kinet-ics.6,7 In spite of the many preclinical and clinicalstudies involving various biomaterials, the ideal carrierhas not yet been found for the effective application ofBMP in dentistry. Absorbable collagen sponge is one ofthe most frequently used carriers for the applicationof rhBMP-2, but it has some shortcomings, such aspoor structural integrity, handling difficulties, and im-munogenicity.8 On the other hand, because the BCPceramics not only provide sufficient mechanical sup-port but also enable vascular and cellular ingrowth,they may enable the induction of new bone. The deg-radation of BCP results in calcium and phosphorousions being released into the biological environment,thus potentially providing a favorable environment forbone regeneration.9 A previous study showed that
BMP-loaded HA/�-TCP ceramics greatly accelerate
OOOO ORIGINAL ARTICLEVolume 113, Number 4 Jang et al. 481
bone formation.10 However, few studies have investi-gated the osteoinductive activity of BMP-loaded BCPwith a higher ratio of �-TCP to HA.
The aims of the current study were threefold: (1) todetermine whether BMP with an HA/�-TCP ratio of20/80 (BCP 20/80) impregnated with rhBMP-2 en-hances new bone formation in rat calvarial defects, (2)to determine the dose-dependent response of rhBMP-2,and (3) to elucidate the relationship between theamount of new bone formed and graft degradation inBCP 20/80 at healing intervals of 2 and 8 weeks.
MATERIAL AND METHODSSprague-Dawley rats (n � 96, body weight 200-300 g)were included in this study. They were housed in plas-tic cages in a room with a 21-hour day/night cycle andan ambient temperature of 21°C, with ad libitum accessto water and a standard laboratory pellet diet. Animalselection and care, the surgical protocol, and the prep-aration procedures were certified by the InstitutionalAnimal Care and Use Committee, Yonsei Medical Cen-ter, Seoul, Korea.
rhBMP-2 implantBCP (MBCP plus, Biomatlante, Nantes, France) wasused as a carrier for rhBMP-2 in the present study. Thiscarrier comprises HA/�-TCP at a ratio of 20:80. rh-BMP-2 expressed by Chinese hamster ovary cells(Korea Bone Bank, Seoul, Korea) was reconstitutedand diluted in a buffer to obtain concentrations of0.025, 0.05, 0.1, and 0.2 mg/mL. The sterilized BCPceramics were loaded with 0.1 mL of rhBMP-2 solutionto obtain implanted concentrations of 2.5, 5.0, 10.0, and20.0 �g, respectively. For control experiments, theBCP was loaded with buffer alone. The BCP wasimpregnated with rhBMP-2 for 1 hour, and then im-planted into calvarial defects made in the rat skulls.
Surgical proceduresThe rats were anesthetized by intramuscular injection(5 mg/kg body weight) of a 4:1 solution of ketaminehydrochloride (Ketalar, Yuhan, Seoul, Korea) and xy-lazine (Rompun, Bayer, Korea, Seoul, Korea). Infiltrationanesthesia was performed at the surgical site. A linearincision was made sagittally at the midline and a full-thickness flap was reflected to expose the calvarial bone.A standardized, circular, transosseous, 8-mm diameterdefect was created on the cranium using a trephine drill (3iImplant Innovation, Palm Beach Gardens, FL) while be-ing irrigated copiously with saline. After removing thetrephined calvarial disk, the experimental and controltreatments were applied to the defects.
The animals were divided into 6 groups of 16 ani-
mals each and were allowed a healing period ofeither 2 (n � 8 animals per group) or 8 weeks (n �8 animals per group). Each group received one of thefollowing experimental conditions: (1) sham-surgerycontrol, (2) BCP control, (3) 2.5 �g rhBMP-2/BCP,(4) 5.0 �g rhBMP-2/BCP, (5) 10.0 �g rhBMP-2/BCP, or (6) 20.0 �g rhBMP-2/BCP. All of thesurgical sites were sutured with 4-0 Monosyn(glyconate absorbable monofilament, B-Braun, Aes-culap, Center Valley, PA) for primary-intention heal-ing. The animals were killed by CO2 suffocation ateither 2 or 8 weeks after the surgery.
Microcomputed tomographyThe specimens were fixed in 10% buffered formalin for10 days and scanned using microcomputed tomography(micro-CT; Skyscan 1,072, Skyscan, Aartselaar, Bel-gium) at a resolution of 35 �m (100 kV and 100 �A).The area of interest was reconstructed using Ondemand3D software (Cybermed, Seoul, Korea).
Histologic processing and histometricmeasurementsThe specimens were decalcified in 5% formic acid for14 days, and then embedded in paraffin. Serial 5-�m-thick sections were cut through the center of the circu-lar calvarial defects. The 2 most-central sections wereselected from each block and stained with hematoxylinand eosin and Masson’s trichrome. Each section wasexamined under a binocular microscope (Leica DMLB, Leica Microsystems, Wetzlar, Germany) equippedwith a camera (Leica DC300F, Leica Microsystems,Heerburgg, Switzerland).
After conventional microscopic examination, com-puter-assisted histometric measurements were made us-ing an automated image-analysis system (Image-ProPlus, Media Cybernetics, Silver Spring, MD). Twoparameters were measured: the percentage of new boneand the percentage of remaining BCP. The amount ofnew bone was measured by calculating the amount ofnewly formed mineralized bone (excluding bone mar-row and fibrovascular tissue) in the defect as a percent-age of the augmented area, which was measured as alltissues within the boundaries of the newly formed bone.The amount of remaining BCP was measured by cal-culating the amount of remaining grafting material as apercentage of the augmented area. The parameters formeasurements and the calculation methods are definedin Fig. 1.
Statistical analysisHistomorphometric measurements of the samples incalvarial defects were used to calculate group mean andSD values. A 2-way analysis of variance was used to
evaluate the effects of time and experimental condi-
ORAL AND MAXILLOFACIAL SURGERY OOOO482 Jang et al. April 2012
tions. The post hoc Scheffé test was used to evaluatethe differences between groups. The level of statisticalsignificance was set at P less than .05.
RESULTSThe postoperative period passed uneventfully in boththe rhBMP-2 groups and the control groups. In total, 96specimens were included for histomorphometric inves-tigation.
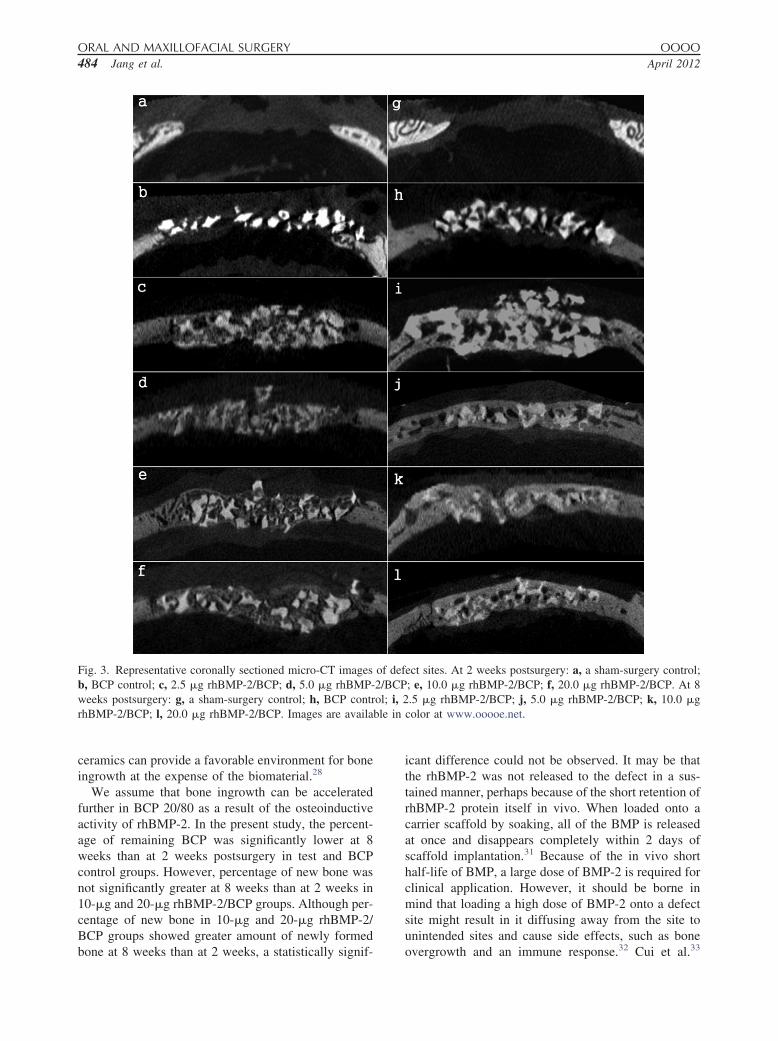
Micro-CT findingsThe defect coverage was minimal in the sham-operatedanimals. Most of the space around the BCP particleswas radiolucent at both 2 and 8 weeks postsurgery inthe BCP control group. On the other hand, bone regen-eration was marked in all of the rhBMP-2–treatedgroups. After 2 weeks of healing, radiopacity was in-creased not only near to the upper and lower defectborders but also adjacent to the BCP particles in coro-nal sections. However, defect coverage was not yetcomplete. After 8 weeks of surgery, the radiopacity hadprogressed further compared with at 2 weeks. Markedincreases in bone density were visible in the upper andlower defect borders, and the defect coverage wasalmost complete in coronal sections. The defect marginand the newly formed bone could not be differentiatedbecause of increased radiodensity of the regeneratedbone (Figs. 2 and 3).
Histologic findingsIn the sham-operated control animals, a minimalamount of new bone was detected at the defect marginat both 2 and 8 weeks postsurgery. Thin and looseconnective tissue filled the defect. In the BCP control, at2 weeks postsurgery there was limited new bone forma-tion evident at the periphery of the defect margin andaround the BCP particles. Most of the defect was occupiedby chronic inflammatory cells and fibrovascular tissues.There was significantly more new bone formation at 8
Fig. 1. Schematic drawing for the histometric analysis of thecalvarial defect model. Image is available in color at www.ooooe.net.
weeks postsurgery than at 2 weeks (Fig. 4).
In the rhBMP-2–treated groups, all of the defectsexhibited bone ingrowth into the BCP particles, and noinflammatory markers or foreign-body reactions werevisible. After 2 weeks of healing, newly formed wovenbone was deposited in close contact with the BCPparticles (Fig. 5). Lacunae containing osteoblasts andvascularized connective tissue were observed withinthe medullary space in the newly formed bone. After 8weeks of healing, newly formed bone completely filledthe defect and mature bone marrow could be seen. Thewoven bone was gradually replaced by lamellar boneand mature lamellar bone, which could be seenthroughout the implant area. It was difficult to distin-guish between the new bone and the defect margin atthis time point (Fig. 6).
Histometric analysisThe percentages of new bone after 2 and 8 weeks ofhealing were significantly greater in the BMP-2–treatedgroups (at all doses) than in the control groups, andsignificantly greater after 8 weeks than after 2 weeks ofhealing in all except the 10-�g and 20-�g rhBMP-2/BCP groups (Table I). The percentage of remainingBCP differed significantly after 8 and 2 weeks in boththe rhBMP-2–treated groups and the BCP controlgroup. However, there was no significant difference inthe percentage of BCP remaining after 2 and 8 weeks ofhealing (Table II).
rhBMP-2 induced significantly more new bone for-mation than in the control groups, irrespective of thedose. The BCP ceramics had degraded significantlymore after 8 weeks of healing than after 2 weeks,regardless of the presence of rhBMP-2.
DISCUSSIONThis study has revealed that the combination of rh-BMP-2 and BCP can significantly increase the amountof newly formed bone in rat calvarial defects, and doesnot induce in any adverse effects. Neither sham surgerynor administration of BCP without rhBMP-2 producedsignificant new bone formation. Thus, rhBMP-2 plays acritical role in the osteogenic process, acting as a potentosteoinductive molecule. Micro-CT imaging showedthat the initial, less-radiopaque bone formation wasfollowed by more radiodense bone, and ultimatelycomplete bony bridging after 8 weeks of healing. In allof the rhBMP-2–treated groups, although limited boneregeneration was observed at 2 weeks, the defect areawas completely covered after 8 weeks of healing. Thus,the rhBMP-2–treated groups exhibited remarkablebone regeneration compared with the control groups onmicro-CT. However, visualization of closure through-out the defect on micro-CT does not necessarily corre-
late with the degree of mineralization, and so histologic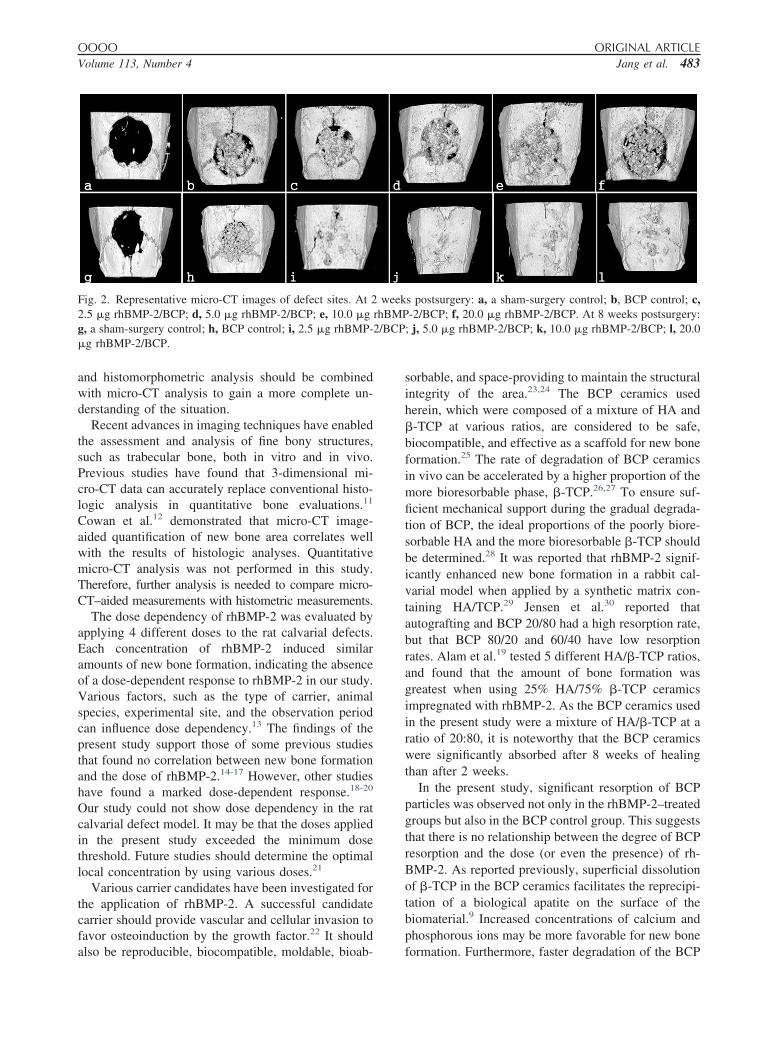
OOOO ORIGINAL ARTICLEVolume 113, Number 4 Jang et al. 483
and histomorphometric analysis should be combinedwith micro-CT analysis to gain a more complete un-derstanding of the situation.
Recent advances in imaging techniques have enabledthe assessment and analysis of fine bony structures,such as trabecular bone, both in vitro and in vivo.Previous studies have found that 3-dimensional mi-cro-CT data can accurately replace conventional histo-logic analysis in quantitative bone evaluations.11
Cowan et al.12 demonstrated that micro-CT image-aided quantification of new bone area correlates wellwith the results of histologic analyses. Quantitativemicro-CT analysis was not performed in this study.Therefore, further analysis is needed to compare micro-CT–aided measurements with histometric measurements.
The dose dependency of rhBMP-2 was evaluated byapplying 4 different doses to the rat calvarial defects.Each concentration of rhBMP-2 induced similaramounts of new bone formation, indicating the absenceof a dose-dependent response to rhBMP-2 in our study.Various factors, such as the type of carrier, animalspecies, experimental site, and the observation periodcan influence dose dependency.13 The findings of thepresent study support those of some previous studiesthat found no correlation between new bone formationand the dose of rhBMP-2.14-17 However, other studieshave found a marked dose-dependent response.18-20
Our study could not show dose dependency in the ratcalvarial defect model. It may be that the doses appliedin the present study exceeded the minimum dosethreshold. Future studies should determine the optimallocal concentration by using various doses.21
Various carrier candidates have been investigated forthe application of rhBMP-2. A successful candidatecarrier should provide vascular and cellular invasion tofavor osteoinduction by the growth factor.22 It should
Fig. 2. Representative micro-CT images of defect sites. At 22.5 �g rhBMP-2/BCP; d, 5.0 �g rhBMP-2/BCP; e, 10.0 �gg, a sham-surgery control; h, BCP control; i, 2.5 �g rhBMP-�g rhBMP-2/BCP.
also be reproducible, biocompatible, moldable, bioab-
sorbable, and space-providing to maintain the structuralintegrity of the area.23,24 The BCP ceramics usedherein, which were composed of a mixture of HA and�-TCP at various ratios, are considered to be safe,biocompatible, and effective as a scaffold for new boneformation.25 The rate of degradation of BCP ceramicsin vivo can be accelerated by a higher proportion of themore bioresorbable phase, �-TCP.26,27 To ensure suf-ficient mechanical support during the gradual degrada-tion of BCP, the ideal proportions of the poorly biore-sorbable HA and the more bioresorbable �-TCP shouldbe determined.28 It was reported that rhBMP-2 signif-icantly enhanced new bone formation in a rabbit cal-varial model when applied by a synthetic matrix con-taining HA/TCP.29 Jensen et al.30 reported thatautografting and BCP 20/80 had a high resorption rate,but that BCP 80/20 and 60/40 have low resorptionrates. Alam et al.19 tested 5 different HA/�-TCP ratios,and found that the amount of bone formation wasgreatest when using 25% HA/75% �-TCP ceramicsimpregnated with rhBMP-2. As the BCP ceramics usedin the present study were a mixture of HA/�-TCP at aratio of 20:80, it is noteworthy that the BCP ceramicswere significantly absorbed after 8 weeks of healingthan after 2 weeks.
In the present study, significant resorption of BCPparticles was observed not only in the rhBMP-2–treatedgroups but also in the BCP control group. This suggeststhat there is no relationship between the degree of BCPresorption and the dose (or even the presence) of rh-BMP-2. As reported previously, superficial dissolutionof �-TCP in the BCP ceramics facilitates the reprecipi-tation of a biological apatite on the surface of thebiomaterial.9 Increased concentrations of calcium andphosphorous ions may be more favorable for new bone
s postsurgery: a, a sham-surgery control; b, BCP control; c,-2/BCP; f, 20.0 �g rhBMP-2/BCP. At 8 weeks postsurgery:
; j, 5.0 �g rhBMP-2/BCP; k, 10.0 �g rhBMP-2/BCP; l, 20.0
weekrhBMP2/BCP
formation. Furthermore, faster degradation of the BCP
ble in
ORAL AND MAXILLOFACIAL SURGERY OOOO484 Jang et al. April 2012
ceramics can provide a favorable environment for boneingrowth at the expense of the biomaterial.28
We assume that bone ingrowth can be acceleratedfurther in BCP 20/80 as a result of the osteoinductiveactivity of rhBMP-2. In the present study, the percent-age of remaining BCP was significantly lower at 8weeks than at 2 weeks postsurgery in test and BCPcontrol groups. However, percentage of new bone wasnot significantly greater at 8 weeks than at 2 weeks in10-�g and 20-�g rhBMP-2/BCP groups. Although per-centage of new bone in 10-�g and 20-�g rhBMP-2/BCP groups showed greater amount of newly formed
Fig. 3. Representative coronally sectioned micro-CT imagesb, BCP control; c, 2.5 �g rhBMP-2/BCP; d, 5.0 �g rhBMP-weeks postsurgery: g, a sham-surgery control; h, BCP contrrhBMP-2/BCP; l, 20.0 �g rhBMP-2/BCP. Images are availa
bone at 8 weeks than at 2 weeks, a statistically signif-
icant difference could not be observed. It may be thatthe rhBMP-2 was not released to the defect in a sus-tained manner, perhaps because of the short retention ofrhBMP-2 protein itself in vivo. When loaded onto acarrier scaffold by soaking, all of the BMP is releasedat once and disappears completely within 2 days ofscaffold implantation.31 Because of the in vivo shorthalf-life of BMP, a large dose of BMP-2 is required forclinical application. However, it should be borne inmind that loading a high dose of BMP-2 onto a defectsite might result in it diffusing away from the site tounintended sites and cause side effects, such as bone
ect sites. At 2 weeks postsurgery: a, a sham-surgery control;; e, 10.0 �g rhBMP-2/BCP; f, 20.0 �g rhBMP-2/BCP. At 8.5 �g rhBMP-2/BCP; j, 5.0 �g rhBMP-2/BCP; k, 10.0 �g
color at www.ooooe.net.
of def2/BCPol; i, 2
overgrowth and an immune response.32 Cui et al.33

OOOO ORIGINAL ARTICLEVolume 113, Number 4 Jang et al. 485
reported that long-term delivery of BMP-2 providesmore enhanced new bone formation than short-termdelivery at an equivalent dose. Therefore, the gradualdegradation of scaffolds with the sustained release ofrhBMP-2 might be critical in reducing the dose forclinical applications and inducing successful bone for-mation effectively.
The BCP 20/80 used in this study exhibited signifi-
Fig. 4. Representative photomicrographs of defect sites receiBCP control at 2 weeks (c) and 8 weeks (d) (arrowheads �40). Images are available in color at www.ooooe.net.
Fig. 5. Representative photomicrographs of defect sites recrhBMP-2/BCP; c, d, 5.0 �g rhBMP-2/BCP; e, f, 10.0 �g rhmargin; NB, new bone; OB, original bone; Masson’s trichro�100). Images are available in color at www.ooooe.net.
cant degradation, but the level of new bone formation
was not significantly greater at 8 weeks than at 2 weekspostsurgery in several of the BMP groups. This findingsuggests that there is no relationship between theamount of new bone and the degree of graft degradationof BCP 20/80 within this study.
The current study found that rhBMP-2 in combina-tion with BCP induced effective new bone formation,but additional studies are needed to investigate the
e sham surgery control at 2 weeks (a), 8 weeks (b), and themargin; Masson’s trichrome stain, original magnification �
the rhBMP-2/BCP. At 2 weeks postsurgery: a, b, 2.5 �g2/BCP; g, h, 20.0 �g rhBMP-2/BCP (arrowheads � defectin, original magnification a, c, e, and g �40; b, d, f, and h
ving thdefect
eivingBMP-me sta
optimal conditions required for the slow and continued

ORAL AND MAXILLOFACIAL SURGERY OOOO486 Jang et al. April 2012
release of rhBMP-2. Moreover, studies assessing dif-ferent ratios of HA/�-TCP with rhBMP-2 are requiredto determine the optimum HA/�-TCP composition.
CONCLUSIONSrhBMP-2 applied using a BCP 20/80 carrier signifi-cantly induces bone formation in the rat calvarial defect
Fig. 6. Representative photomicrographs of defect sites rerhBMP-2/BCP; c, d, 5.0 �g rhBMP-2/BCP; e, f, 10.0 �g rhmargin; NB, new bone; OB, original bone; Masson’s trichro�100).
Table I. Amounts of new bone as percentages of theaugmented area at 2 and 8 weeks after surgery (mean �SD values; n � number of specimens)
Group
2 wkpostsurgery
(n)
8 wkpostsurgery
(n)
Sham-surgery control 5.27 � 0.97 (8) 12.19 � 3.01*(8)BCP control 9.85 � 3.47 (8) 23.06 � 5.31* (8)2.5 �g rhBMP-2/BCP 44.34 � 7.64†‡ (8) 54.91 � 8.25†‡* (8)5.0 �g rhBMP-2/BCP 47.64 � 8.63†‡ (8) 58.67 � 3.93†‡* (8)10.0 �g rhBMP-2/BCP 50.34 � 19.87†‡ (8) 62.65 � 9.67†‡ (8)20.0 �g rhBMP-2/BCP 50.87 � 5.93†‡ (8) 57.59 � 8.50†‡ (8)
*Significant different from sham control group (P � .05).†Significant different from BCP control group (P � .05).‡Significant difference between at 2 and 8 weeks postsurgery(P � .05).
model. An rhBMP-2 dose-dependent response was not
evident in the present study, and there was no mean-ingful relationship between the amount of new bonedeposited and the degree of graft degradation of BCP20/80. BCP 20/80 may be considered an effective andbiocompatible carrier for rhBMP-2.
REFERENCES1. Gauthier O, Bouler JM, Aguado E, Pilet P, Daculsi G. Macro-
porous biphasic calcium phosphate ceramics: influence of mac-ropore diameter and macroporosity percentage on bone ingrowth.
the rhBMP-2/BCP at 8 weeks postsurgery. a, b, 2.5 �g2/BCP; g, h, 20.0 �g rhBMP-2/BCP (arrowheads � defectin, original magnification a, c, e, and g �40; b, d, f, and h
Table II. Amounts of BCP remaining as percentages ofthe augmented area at 2 and 8 weeks after surgery(mean � SD values; n � number of specimens)
Group
2 wkpostsurgery
(n)
8 wkpostsurgery
(n)
BCP control 49.39 � 9.11 (8) 31.15 � 7.03* (8)2.5 �g rhBMP-2/BCP 51.59 � 9.55 (8) 35.20 � 10.40* (8)5.0 �g rhBMP-2/BCP 48.33 � 10.07 (8) 32.68 � 5.63* (8)10.0 �g rhBMP-2/BCP 47.21 � 20.01 (8) 28.46 � 11.30* (8)20.0 �g rhBMP-2/BCP 47.31 � 5.04 (8) 35.07 � 9.83* (8)
*Significant difference between at 2 and 8 weeks postsurgery(P � .05).
ceivingBMP-me sta
Biomaterials 1998;19:133-9.

OOOO ORIGINAL ARTICLEVolume 113, Number 4 Jang et al. 487
2. Jensen SS, Broggini N, Hjorting-Hansen E, Schenk R, Buser D. Bonehealing and graft resorption of autograft, anorganic bovine bone andbeta-tricalcium phosphate. A histologic and histomorphometric study inthe mandibles of minipigs. Clin Oral Implants Res 2006;17:237-43.
3. LeGeros RZ, Lin S, Rohanizadeh R, Mijares D, LeGeros JP.Biphasic calcium phosphate bioceramics: preparation, propertiesand applications. J Mater Sci Mater Med 2003;14:201-9.
4. Fellah BH, Gauthier O, Weiss P, Chappard D, Layrolle P. Os-teogenicity of biphasic calcium phosphate ceramics and boneautograft in a goat model. Biomaterials 2008;29:1177-88.
5. Lee JH, Jung UW, Kim CS, Choi SH, Cho KS. Histologic andclinical evaluation for maxillary sinus augmentation using mac-roporous biphasic calcium phosphate in human. Clin Oral Im-plants Res 2008;19:767-71.
6. Kim CS, Kim JI, Kim J, Choi SH, Chai JK, Kim CK, et al. Ectopicbone formation associated with recombinant human bone morphoge-netic proteins-2 using absorbable collagen sponge and beta tricalciumphosphate as carriers. Biomaterials 2005;26:2501-7.
7. Hyun SJ, Han DK, Choi SH, Chai JK, Cho KS, Kim CK, et al. Effectof recombinant human bone morphogenetic protein-2, -4, and -7 onbone formation in rat calvarial defects. J Periodontol 2005;76:1667-74.
8. Barboza EP, Duarte ME, Geolas L, Sorensen RG, Riedel GE,Wikesjo UM, et al. Ridge augmentation following implantationof recombinant human bone morphogenetic protein-2 in the dog.J Periodontol 2000;71:488-96.
9. Yamada S, Heymann D, Bouler JM, Daculsi G. Osteoclasticresorption of biphasic calcium phosphate ceramic in vitro.J Biomed Mater Res 1997;37:346-52.
10. Ono I, Gunji H, Kaneko F, Saito T, Kuboki Y. Efficacy ofhydroxyapatite ceramic as a carrier for recombinant human bonemorphogenetic protein. J Craniofac Surg 1995;6:238-44.
11. Thomsen JS, Laib A, Koller B, Prohaska S, Mosekilde L, Gowin W, etal. Stereological measures of trabecular bone structure: comparison of3D micro computed tomography with 2D histological sections in hu-man proximal tibial bone biopsies. J Microsc 2005;218:171-9.
12. Cowan CM, Aghaloo T, Chou YF, Walder B, Zhang X, Soo C,et al. MicroCT evaluation of three-dimensional mineralization inresponse to BMP-2 doses in vitro and in critical sized rat cal-varial defects. Tissue Eng 2007;13:501-12.
13. Hasegawa Y, Sato S, Takayama T, Murai M, Suzuki N, Ito K, etal. Short-term effects of rhBMP-2-enhanced bone augmentationbeyond the skeletal envelope within a titanium cap in rabbitcalvarium. J Periodontol 2008;79:348-54.
14. Wikesjo UM, Guglielmoni P, Promsudthi A, Cho KS, TrombelliL, Selvig KA, et al. Periodontal repair in dogs: effect of rhBMP-2concentration on regeneration of alveolar bone and periodontalattachment. J Clin Periodontol 1999;26:392-400.
15. Tatakis DN, Koh A, Jin L, Wozney JM, Rohrer MD, WikesjoUM, et al. Peri-implant bone regeneration using recombinanthuman bone morphogenetic protein-2 in a canine model: a dose–response study. J Periodontal Res 2002;37:93-100.
16. Lee JH, Kim CS, Choi KH, Jung UW, Yun JH, Choi SH, et al.The induction of bone formation in rat calvarial defects andsubcutaneous tissues by recombinant human BMP-2, producedin Escherichia coli. Biomaterials 2010;31:3512-9.
17. Pang EK, Im SU, Kim CS, Choi SH, Chai JK, Kim CK, et al. Effect ofrecombinant human bone morphogenetic protein-4 dose on bone for-mation in a rat calvarial defect model. J Periodontol 2004;75:1364-70.
18. Kenley R, Marden L, Turek T, Jin L, Ron E, Hollinger JO, et al.Osseous regeneration in the rat calvarium using novel deliverysystems for recombinant human bone morphogenetic protein-2(rhBMP-2). J Biomed Mater Res 1994;28:1139-47.
19. Alam I, Asahina I, Ohmamiuda K, Enomoto S. Comparative study of
biphasic calcium phosphate ceramics impregnated with rhBMP-2 asbone substitutes. J Biomed Mater Res 2001;54:129-38.
20. Kanatani M, Sugimoto T, Kaji H, Kobayashi T, Nishiyama K,Fukase M, et al. Stimulatory effect of bone morphogenetic pro-tein-2 on osteoclast-like cell formation and bone-resorbing ac-tivity. J Bone Miner Res 1995;10:1681-90.
21. Hong SJ, Kim CS, Han DK, Cho IH, Jung UW, Choi SH, et al.The effect of a fibrin-fibronectin/beta-tricalcium phosphate/re-combinant human bone morphogenetic protein-2 system on boneformation in rat calvarial defects. Biomaterials 2006;27:3810-6.
22. Brekke JH, Toth JM. Principles of tissue engineering applied toprogrammable osteogenesis. J Biomed Mater Res 1998;43:380-98.
23. Wikesjo UM, Xiropaidis AV, Thomson RC, Cook AD, SelvigKA, Hardwick WR, et al. Periodontal repair in dogs: space-providing ePTFE devices increase rhBMP-2/ACS-induced boneformation. J Clin Periodontol 2003;30:715-25.
24. Han DK, Kim CS, Jung UW, Chai JK, Choi SH, Kim CK, et al.Effect of a fibrin-fibronectin sealing system as a carrier forrecombinant human bone morphogenetic protein-4 on bone for-mation in rat calvarial defects. J Periodontol 2005;76:2216-22.
25. Schopper C, Ziya-Ghazvini F, Goriwoda W, Moser D, Wan-schitz F, Spassova E, et al. HA/TCP compounding of a porousCaP biomaterial improves bone formation and scaffold degrada-tion—a long-term histological study. J Biomed Mater Res BAppl Biomater 2005;74:458-67.
26. Daculsi G. Biphasic calcium phosphate concept applied to arti-ficial bone, implant coating and injectable bone substitute. Bio-materials 1998;19:1473-8.
27. Jung UW, Choi SY, Pang EK, Kim CS, Choi SH, Cho KS, et al.The effect of varying the particle size of beta tricalcium phos-phate carrier of recombinant human bone morphogenetic pro-tein-4 on bone formation in rat calvarial defects. J Periodontol2006;77:765-72.
28. Daculsi G, Laboux O, Malard O, Weiss P. Current state of the artof biphasic calcium phosphate bioceramics. J Mater Sci MaterMed 2003;14:195-200.
29. Jung RE, Weber FE, Thoma DS, Ehrbar M, Cochran DL, HammerleCH, et al. Bone morphogenetic protein-2 enhances bone formationwhen delivered by a synthetic matrix containing hydroxyapatite/trical-cium phosphate. Clin Oral Implants Res 2008;19:188-95.
30. Jensen SS, Bornstein MM, Dard M, Bosshardt DD, Buser D.Comparative study of biphasic calcium phosphates with differentHA/TCP ratios in mandibular bone defects. A long-term histo-morphometric study in minipigs. J Biomed Mater Res B ApplBiomater 2009;90:171-81.
31. Kanematsu A, Yamamoto S, Ozeki M, Noguchi T, Kanatani I,Ogawa O, et al. Collagenous matrices as release carriers ofexogenous growth factors. Biomaterials 2004;25:4513-20.
32. Ma Z, Kotaki M, Inai R, Ramakrishna S. Potential of nanofiber matrixas tissue-engineering scaffolds. Tissue Eng 2005;11:101-9.
33. Cui W, Li X, Zhu X, Yu G, Zhou S, Weng J, et al. Investigation of drugrelease and matrix degradation of electrospun poly(D,L-lactide) fiberswith paracetanol inoculation. Biomacromolecules 2006;7:1623-9.
Reprint requests:
Kyoo-Sung Cho, DDS, PhDDepartment of PeriodontologyResearch Institute for Periodontal RegenerationCollege of DentistryYonsei University250, Seongsanno, Seodeamun-guSeoul 120–752, Korea
[email protected]
![Silicon Substitution in Biphasic Calcium Phosphate ......Si-substituted calcium phosphates with respect to unsubstituted calcium phosphates [15],[16],[17]. Various methods of synthesis](https://img.dokumen.tips/doc/110x75/606853c6531e020f385e429b/silicon-substitution-in-biphasic-calcium-phosphate-si-substituted-calcium.jpg)










![Scientific Studies · calcium and phosphate ions, and precipitation of biological apatite). This phenomenon was largely known and published for biphasic calcium phosphate [12,13]](https://img.dokumen.tips/doc/110x75/60772edce0335e343572d1a7/scientific-studies-calcium-and-phosphate-ions-and-precipitation-of-biological-apatite.jpg)
















