Embed Size (px)
Citation preview

emedicine.medscape.com
eMedicine Specialties > Radiology > Musculoskeletal
Osteochondritis Dissecans Liem T Bui-Mansfield, MD, Clinical Associate in the Division of Radiologic Sciences, Department of Radiology, Wake Forest University School of Medicine
Updated: Aug 21, 2009
Introduction
Background
Osteochondritis dissecans (OCD) is a term for osteochondral fracture. An osteochondral fragment may be present in situ, incompletely
detached, or completely detached. A completely detached fragment is a loose body (see Images 1-2).[1 ]
Lateral radiograph of the knee reveals a calcified loose body (arrowhead) posterior to the knee and lucency (arrow) in the articular surface of the patella.
Página 1 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Anteroposterior radiograph of the knee demonstrates lucency (arrow) in the central and superior aspect of the patella.
Recent studies
Adachi et al evaluated the functional and radiographic outcome of retroarticular drilling without bone grafting in 12 patients with juvenile
osteochondritis dissecans after 6 months of unsuccessful nonoperative treatment. The mean Lysholm score significantly improved
postoperatively (from 72.3 to 95.8). All lesions except 1 healed after retroarticular drilling, and healing was achieved at a mean of 4.4
months on plain radiographs and 7.6 months on magnetic resonance imaging.[2 ]
Kijowski et al retrospectively compared the sensitivity and specificity of previously described magnetic resonance imaging criteria for the
detection of instability in patients with juvenile or adult osteochondritis dissecans of the knee, with arthroscopic findings as the reference
standard. Separately, previously described MR imaging criteria for detection of OCD instability were 0-88% sensitive and 21-100%
specific for juvenile OCD lesions and 27-54% sensitive and 100% specific for adult OCD lesions. When used together, the criteria were
100% sensitive and 11% specific for instability in juvenile OCD lesions and 100% sensitive and 100% specific for instability in adult OCD
lesions. The authors concluded from their findings that previously described MR imaging criteria for OCD instability have high specificity
for adult but not juvenile lesions of the knee.[3 ]
Pathophysiology
Osteochondritis dissecans (OCD) is a form of osteochondrosis limited to the articular epiphysis. Articular epiphyses fail as a result of
compression. Both trauma and ischemia probably are involved in the pathology. Trauma is most likely the primary insult, with ischemia
as secondary injury.[4,5 ]
Página 2 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Trauma may be direct, such as impaction fracture, or repetitive microtrauma, such as excessive normal compressive stress.[4,5 ]The
pathology of OCD may be described in 3 stages.
1. In the first stage (acute injury), thickened and edematous intra-articular and periarticular soft tissues are observed. Often, the
adjacent metaphysis reveals mild osteoporosis resulting from active hyperemia of the metaphysis.
2. In the second stage, the epiphysis reveals an irregular contour and a thinning of the subcortical zone of rarefaction. On
radiography, the epiphysis may demonstrate fragmentation. Blood vessels within the epiphysis are incompetent because of
thrombosis or microfractures of the trabeculae, which results in poor healing.
3. The third stage is the period of repair in which granulation tissue gradually replaces the necrotic tissue. Necrotic bone may lose its
structural support, which results in compression and flattening of the articular surface.
Injury of the articular cartilage allows an influx of synovial fluid into the epiphysis, creating a subchondral cyst (see Images 3-8). The
subchondral cyst and increased joint pressure may prevent healing.
Anteroposterior radiograph of the knee is unremarkable.
Página 3 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Anteroposterior radiograph of the knee 1 year after injury reveals an anterior cruciate ligament reconstruction (arrowheads) and lucency (arrow) in the lateral tibial plateau.
Página 4 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print
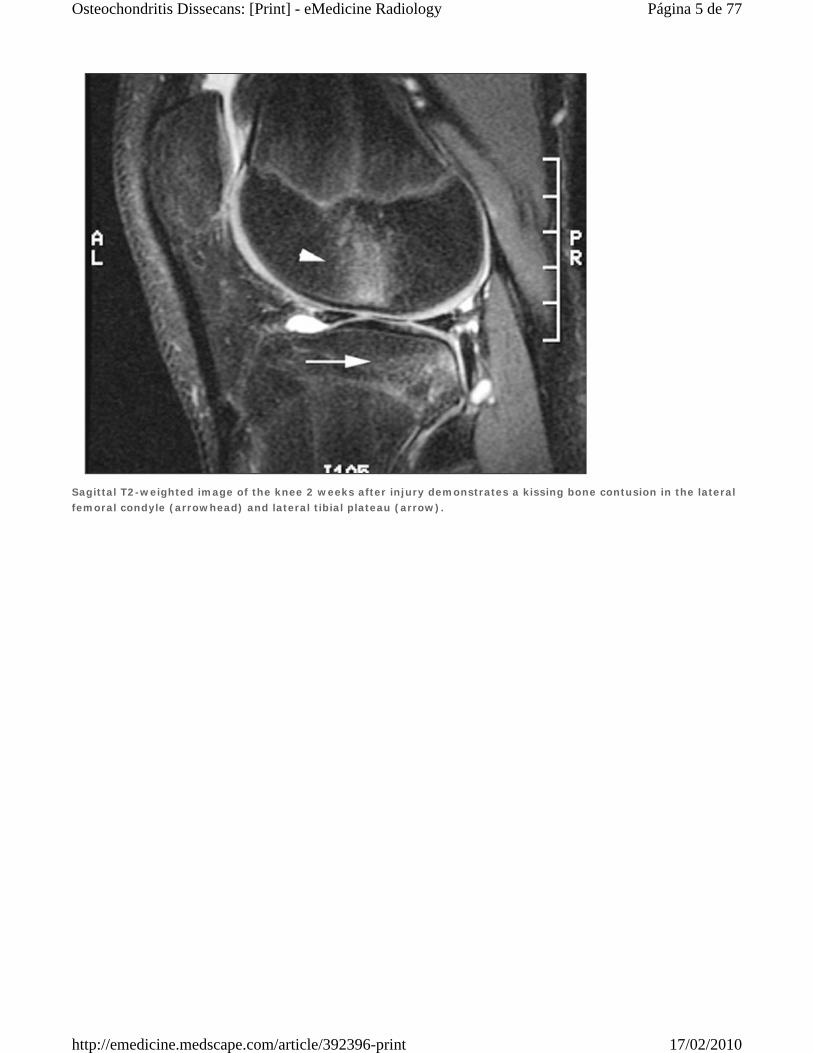
Sagittal T2-weighted image of the knee 2 weeks after injury demonstrates a kissing bone contusion in the lateral femoral condyle (arrowhead) and lateral tibial plateau (arrow).
Página 5 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Sagittal T2-weighted image 1 year after injury reveals a subchondral cyst (arrow), an articular defect in the lateral tibial plateau, and a large knee effusion (arrowhead).
Página 6 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Coronal T1-weighted image 2 weeks after injury is unremarkable.
Página 7 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Coronal T1-weighted image 1 year after injury demonstrates a subchondral cyst (arrowhead) in the lateral tibial plateau.
Knee: In the knee joint, the medial femoral condyle is the most commonly involved site (see Images 9-10). Potential locations are
the lateral aspect of the medial femoral condyle (75%), the weightbearing surface of the medial (10%) and lateral femoral
condyles (10%), and the anterior intercondylar groove or patella (5%) (see Images 1-2, Images 11-13). Rarely, OCD occurs in the
medial tibial plateau (see Images 14-15).[6,7,8,9,10,11,12,13,14,15,16 ]
Página 8 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Anteroposterior radiograph of the knee reveals osteochondritis dissecans in the lateral aspect (arrowhead) of the medial femoral condyle.
Página 9 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Axial CT of the knee demonstrates a completely detached osteochondral fracture (arrowhead) in the lateral aspect of the medial femoral condyle.
Elbow: In the elbow joint, the most common site of OCD occurs in the anterolateral aspect of the capitellum. Singer and Roy
proposed that repeated valgus stress and a tenuous blood supply within the capitellum explain the frequent occurrence of OCD in
this location.[17 ]In a cadaveric study of the articular surfaces of the radiocapitellar joint, Schenck et al demonstrated significant
topographic differences in the mechanical properties and thickness of cartilage in the capitellum and radial head.[18 ]Disparity in
the mechanical properties of the central radial head and lateral capitellum probably is a factor in the initiation and localization of
OCD of the capitellum (see Images 16-23).[19,20 ]
Página 10 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Drawing of osteochondritis dissecans of the capitellum with localized subchondral bony flattening and a normal articular surface.
Página 11 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Drawing of osteochondritis dissecans of the capitellum with a nondisplaced osteochondral fragment.
Página 12 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Drawing of osteochondritis dissecans of the capitellum with a slightly displaced fragment.
Ankle: In the ankle joint, OCD occurs more frequently in the talus (see Images 24-32) than in the tibial plafond (see Images 33-36)
and is 4-14 times more common.[21,22 ]Disparity in frequency results from the biomechanical topography of the human ankle
cartilage, since tibial cartilage is stiffer than talar cartilage. The usual sites of OCD of the talar dome are the posteromedial aspect
(56%) and the anterolateral aspect (44%) of the talus. Occasionally, mirror-image osteochondral defects of the talus and distal
tibia occur, suggesting trauma as a potential cause of both lesions.[7,23,24,25,26,27,28 ]
Página 13 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Anteroposterior radiograph of the leg reveals osteochondritis dissecans in the medial talar dome (arrowhead).
Mortise view of the ankle reveals lucency in the central portion of the tibial plafond (arrowhead).
Tarsal navicular: Occasionally, OCD of the tarsal navicular (see Images 37-40) is seen on ankle radiographs. Osteochondral
fracture of the tarsal navicular is not as rare as previously reported in the radiologic literature. Radiographic findings can be subtle
and, in some patients, may mimic Mueller-Weiss syndrome or stress fracture of the tarsal navicular. CT or MRI helps confirm the
diagnosis. OCD of the tarsal navicular is limited to the proximal articular surface. Tarsal navicular OCD does not demonstrate the
classic radiographic appearance of Mueller-Weiss syndrome, which includes comma-shaped deformity of the navicular resulting
from collapse of the lateral portion of the bone, bipartite navicular resulting from fracture, or protrusion of portions of the bone or
Página 14 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

the entire navicular bone, medially or dorsally. In addition, tarsal OCD does not demonstrate either partial or complete sagittal
fracture line on CT or MRI.[29 ]
Lateral radiograph of the ankle reveals a cortical depression and loss of the sharp cortical line in the proximal articular surface of the tarsal navicular (arrowhead).
Página 15 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Sagittal T1-weighted image of the ankle confirms osteochondritis dissecans of the tarsal navicular (arrowhead).
Hip joint: In the hip joint, OCD occurs overwhelmingly in the femoral capital epiphysis. Only case reports exist of patients with
OCD of the acetabulum. Many patients with OCD of the femoral capital epiphysis have a prior history of Legg-Calve-Perthes
Disease. OCD is observed in approximately 3% of adults who had Legg-Calvé-Perthes disease as children. However, this
complication cannot be predicted during the early stages of the Legg-Calvé-Perthes process and may present years later.[25,30,31,32,33 ]
Shoulder joint: OCD rarely occurs in the shoulder joint, where it involves either the humeral head or the glenoid. Only 7 patients
with OCD of the humeral head have been reported. All of the patients were men, ranging from age 12-44 years. Five of the
patients (71%) demonstrated lesions in the right shoulder, suggesting an association with right-handedness. Locations of
involvement were the anterosuperior, posterosuperior, posteromedial, superior, and medio-inferior aspects of the humeral head.[34,35,36,37 ]
Glenoid: OCD of the glenoid is best detected on MRI. A developmental defect of the glenoid is a normal variant that may be
mistaken for OCD of the glenoid (see Images 41-42). Developmental defect of the glenoid is a small focal defect within the center
of the glenoid and without associated subchondral bone marrow edema. OCD of the glenoid usually is a much larger and
eccentrically located lesion (see Images 43-46).
Página 16 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Oblique, coronal T2-weighted image of the right shoulder demonstrates a developmental defect in the glenoid filled with fluid (arrowhead). Note the central location and absence of subchondral bone marrow edema. This is a normal variant.
Página 17 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Sagittal T2-weighted image of the right shoulder reveals a central depression within the glenoid (arrowhead) without associated subchondral bone marrow edema. This is a normal variant.
Wrist joint: OCD of the wrist joint is rare and primarily occurs in the scaphoid. It may occur in either the distal or proximal pole and
in either the distal or proximal articular surface of the scaphoid and may be bilateral. OCD of the scaphoid has been observed in
bakers, boxers, pelota players, acrobats, and pneumatic drill workers, all of whom are subjected to repeated minor trauma of the
wrist. One report of OCD of the distal radioulnar joint exists.[38,39,40,41 ]
Frequency
United States
Overall prevalence of osteochondritis dissecans is unknown; however, the prevalence of OCD in specific joints has been reported. In
femoral condyles, OCD has been estimated to occur in 6 per 10,000 men and in 3 per 10,000 women younger than 50 years. OCD of the
ankle occurs in 0.002 per 1000, regardless of age and sex. Nielsen reported a frequency of 4.1% for OCD of the elbow.[42 ]In general,
OCD occurs more commonly in the convex surface than in the concave surface of a joint.
Overall, the knee is most frequently involved in OCD.[8 ]In a large series of patients with OCD, OCD of the elbow, ankle, and hip
comprising approximately 6%, 4%, and 2% of OCD patients, respectively, was reported. Since the advent of cross-sectional imaging (CT
and MRI), OCD of the talus has been diagnosed more frequently and, in future series, may represent the most frequent site of OCD.
Mortality/Morbidity
Pain is the primary symptom in osteochondritis dissecans. Osteoarthritis is a common long-term complication.
Página 18 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Race
No racial predilection is recognized in osteochondritis dissecans.
Sex
No sex predilection is reported in osteochondritis dissecans.
Age
Osteochondritis dissecans tends to affect young patients. In OCD of the elbow, patient age averages 23 years and ranges from 4-47
years. In OCD of the ankle, patient age averages 20 years and ranges from 8-50 years. In OCD of the hip, patient age averages 24
years and ranges from 14-39 years.[43 ]
Presentation
Patients with osteochondritis dissecans usually report pain at the extremes of motion range. Periarticular edema is often present with
slight warmth to the touch. When a lower extremity is involved, patients often limp. Symptoms usually improve with protected
immobilization of the joint.
Preferred Examination
Staging classifications of osteochondral lesions have been described best in the talus. Arthroscopic classifications of osteochondral
lesions are the criterion standard. Two arthroscopic classifications of osteochondral lesions of the talus are reported. Both surgical
classifications are based on the appearance of the overlying articular cartilage as seen on arthroscopy
The Pritsch arthroscopic staging of osteochondral lesions of the talus is as follows[44 ]:
Grade I - Intact, firm, shiny articular cartilage
Grade II - Intact but soft articular cartilage
Grade III - Frayed articular cartilage
The Cheng arthroscopic staging of osteochondral lesions of the talus is as follows[45 ]:
Grade A - Articular cartilage is smooth and intact but may be soft or ballottable
Grade B - Articular cartilage has a rough surface
Grade C - Articular cartilage has fibrillations or fissures
Grade D - Articular cartilage with a flap or exposed bone
Grade E - Loose, nondisplaced osteochondral fragment
Grade F - Displaced osteochondral fragment
Radiographic findings correspond with arthroscopic staging in 56% of patients, because fibrosis may provide stability in osseous
separation. MRI correlates best with surgical staging.
Differential Diagnoses
Avascular Necrosis, Femoral Head
Osteoarthritis, Primary
Stress Fracture
Radiography
Página 19 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Lateral radiograph of the knee reveals a calcified loose body (arrowhead) posterior to the knee and lucency (arrow) in the articular surface of the patella.
Página 20 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Anteroposterior radiograph of the knee is unremarkable.
Página 21 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Anteroposterior radiograph of the knee 1 year after injury reveals an anterior cruciate ligament reconstruction (arrowheads) and lucency (arrow) in the lateral tibial plateau.
Anteroposterior radiograph of the knee reveals osteochondritis dissecans in the lateral aspect (arrowhead) of the medial femoral condyle.
Página 22 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Anteroposterior radiograph of the leg reveals osteochondritis dissecans in the medial talar dome (arrowhead).
Lateral view of the ankle reveals loss of the sharp cortical line (arrowhead) in the posterior aspect of the tibial plafond.
Página 23 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Lateral radiograph of the ankle reveals a cortical depression and loss of the sharp cortical line in the proximal articular surface of the tarsal navicular (arrowhead).
Findings
On conventional radiographs, osteochondral lesions may appear normal. When detectable, osteochondral lesions appear as lucencies in
the articular epiphysis. Osteochondritis dissecans is suggested by a loss of the sharp cortical line of the articular surface.[7,20,46 ]
The Berndt and Harty radiographic classification of osteochondral lesions of the talus is as follows[47 ]:
Stage I - Normal radiograph (subchondral compression fracture of the talus with no ligamentous sprain)
Stage II - Partially detached osteochondral fragment
Stage III - Complete, nondisplaced fracture remaining within the bony crater
Stage IV - Detached, loose osteochondral fragment
Computed Tomography
Página 24 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Axial CT of the knee demonstrates a completely detached osteochondral fracture (arrowhead) in the lateral aspect of the medial femoral condyle.
Página 25 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Axial CT of the ankle reveals osteochondritis dissecans in the posteromedial aspect of the talar dome.
Página 26 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Coronal CT of the ankle demonstrates a nondisplaced osteochondral fragment.
Axial CT at the level of the ankle joint demonstrates lytic defect in the central and posterior portions of the tibial plafond.
Página 27 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Coronal CT of the ankle demonstrates a cortical depression in the tibial plafond.
Findings
In the ankle joint, helical CT has multiplanar capability. CT is obtained in the direct axial and coronal planes at 1.5-mm slice thickness
with sagittal reformations. Cystic lesion of the talar dome, cortical depression, or a loose bony fragment within the osteochondral defect
may be demonstrated.
The Ferkel and Sgaglione CT classification of osteochondral lesions of the talus is as follows[25 ]:
Stage I - Cystic lesion of the talar dome with an intact roof
Stage IIa - Cystic lesion with communication to the talar dome surface
Stage IIb - Open articular surface lesion with an overlying, nondisplaced fragment
Stage III - Nondisplaced lesion with lucency
Stage IV - Displaced osteochondral fragment
Magnetic Resonance Imaging
Página 28 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Sagittal T2-weighted image of the knee 2 weeks after injury demonstrates a kissing bone contusion in the lateral femoral condyle (arrowhead) and lateral tibial plateau (arrow).
Página 29 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Sagittal T2-weighted image 1 year after injury reveals a subchondral cyst (arrow), an articular defect in the lateral tibial plateau, and a large knee effusion (arrowhead).
Página 30 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Coronal T1-weighted image 2 weeks after injury is unremarkable.
Página 31 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Coronal T1-weighted image 1 year after injury demonstrates a subchondral cyst (arrowhead) in the lateral tibial plateau.
Página 32 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Axial T1-weighted image at the level of the ankle joint demonstrates abnormal low-signal intensity in the anterolateral aspect of the talus (arrowhead).
Página 33 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Coronal T2-weighted image demonstrates an articular defect and abnormal high-signal intensity in the lateral talar dome consistent with osteochondritis dissecans.
Página 34 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Oblique, coronal T2-weighted image of the right shoulder demonstrates a developmental defect in the glenoid filled with fluid (arrowhead). Note the central location and absence of subchondral bone marrow edema. This is a normal variant.
Página 35 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Sagittal T2-weighted image of the right shoulder reveals a central depression within the glenoid (arrowhead) without associated subchondral bone marrow edema. This is a normal variant.
Página 36 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Oblique coronal T2-weighted fat-suppression image demonstrates a hyperintense osteochondral lesion in the inferior half of the glenoid. Note the fluid in the subacromial/subdeltoid bursa and the supraspinatus tendon tear.
Página 37 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Axial-gradient recall image reveals an osteochondral lesion in the anterior half of the glenoid.
Findings
MRI detects radiographically occult lesions that also may not be evident on CT. A short tau-inversion recovery sequence is the most
sensitive.[7,19,43 ]
The Anderson MRI classification of osteochondral lesions of the talus is as follows[48 ]:
Stage I - Bone marrow edema (subchondral trabecular compression; radiograph results are negative with positive bone-scan
findings)
Stage IIa - Subchondral cyst
Stage IIb - Incomplete separation of the osteochondral fragment
Stage III - Fluid around an undetached, undisplaced osteochondral fragment
Stage IV - Displaced osteochondral fragment
Ultrasonography
Página 38 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Anterior longitudinal sonogram reveals a stable lesion with localized subchondral bony flattening (arrows) and a normal outline of the articular cartilage (corresponding to Picture 16 in Multimedia; courtesy of Dr Masatoshi Takahara).
Posterior longitudinal sonogram demonstrates a stable lesion with a nondisplaced bone fragment (asterisk), intact articular surface (arrowheads), and a narrow gap formation (arrow; corresponding to Picture 17 in Multimedia; courtesy of Dr Masatoshi Takahara).
Página 39 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Posterior longitudinal sonogram reveals an unstable lesion with a slightly displaced fragment (asterisk) and a wide gap formation (arrows; corresponding to Picture 18 in Multimedia; courtesy of Dr Masatoshi Takahara).
Anterior longitudinal sonogram demonstrates an unstable lesion with a capitellar defect (arrow; corresponding to Picture 19 in Multimedia; courtesy of Dr Masatoshi Takahara).
Findings
Sonography has been used to evaluate osteochondritis dissecans of the knee and humeral capitellum. The advantage of sonography is
dynamic scanning with motion of the evaluated joint. In one study, sonographic assessment of OCD of the humeral capitellum agreed
Página 40 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

with radiographic assessment in 23 of 27 patients (85%), MRI assessment in 9 of 10 (90%), and surgical findings in 14 of 15 (93%).
The sonographic appearance of OCD of the capitellum is as follows:
Stable - Localized, subchondral bony flattening and normal articular surface
Stable - Lesion with nondisplaced osteochondral fragment
Unstable - Capitellar osteochondral defect with loose intra-articular fragment
Unstable - Lesion with slightly displaced osteochondral fragment
Nuclear Imaging
Findings
Scintigraphic findings are nonspecific, demonstrating a mild-to-marked increase in focal uptake in the involved bone, depending on the
age of the osteochondritis dissecans. Dynamic bone scintigraphy is twice as sensitive as static scintigraphy in the detection of OCD of
the femoral condyles. The scintigraphic appearance is probably a result of the slow repair process around an OCD, involving only the
bone tissue surrounding the lesion, and is not a result of the OCD itself.[9,49 ]
Intervention
Treatment consists of discontinuation of the injurious activity, protected immobilization of the joint, and administration of nonsteroidal
anti-inflammatory medications. Surgery may be required to remove the intra-articular loose body and/or correct the resulting
degenerative changes.[14,26,30,40,44 ]
Multimedia
Página 41 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 1: Lateral radiograph of the knee reveals a calcified loose body (arrowhead) posterior to the knee and lucency (arrow) in the articular surface of the patella.
Página 42 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print
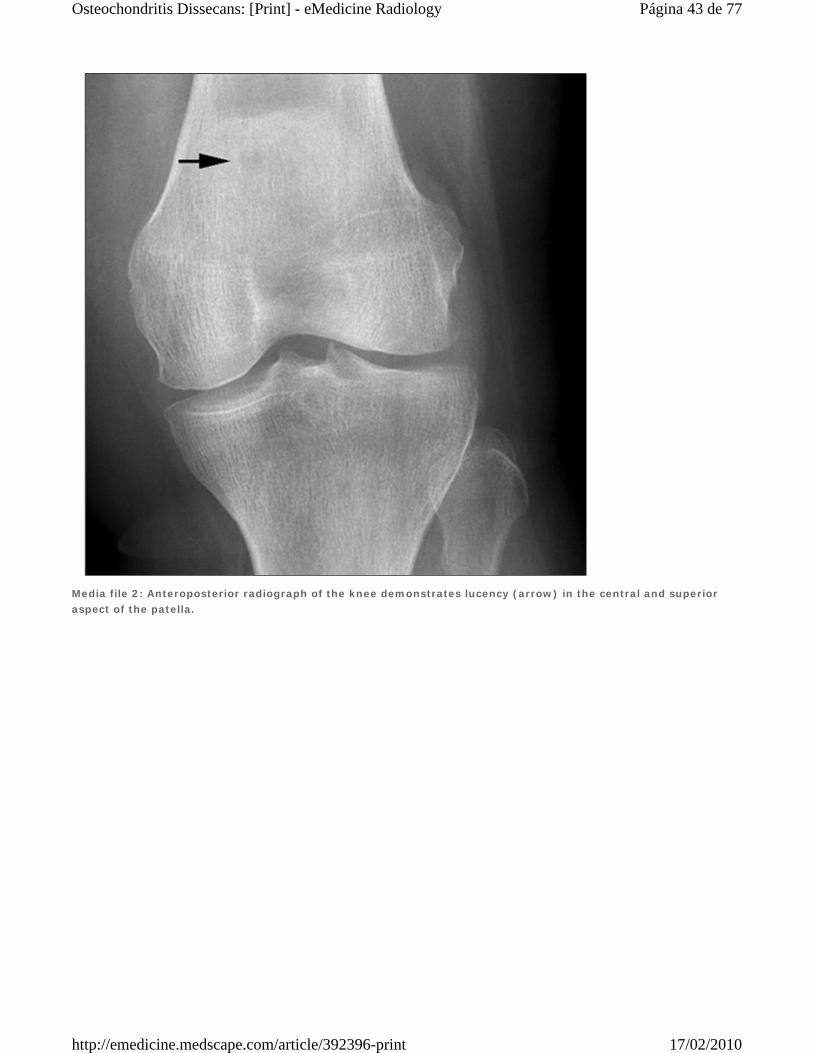
Media file 2: Anteroposterior radiograph of the knee demonstrates lucency (arrow) in the central and superior aspect of the patella.
Página 43 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print
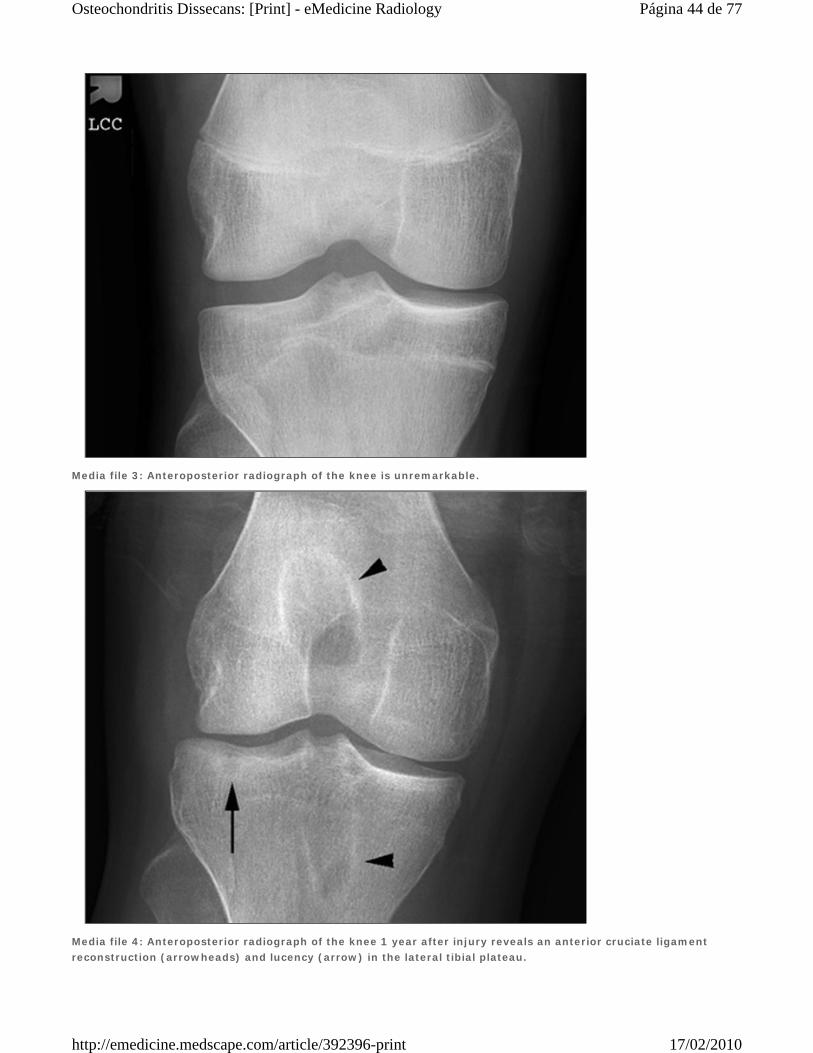
Media file 3: Anteroposterior radiograph of the knee is unremarkable.
Media file 4: Anteroposterior radiograph of the knee 1 year after injury reveals an anterior cruciate ligament reconstruction (arrowheads) and lucency (arrow) in the lateral tibial plateau.
Página 44 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 5: Sagittal T2-weighted image of the knee 2 weeks after injury demonstrates a kissing bone contusion in the lateral femoral condyle (arrowhead) and lateral tibial plateau (arrow).
Página 45 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 6: Sagittal T2-weighted image 1 year after injury reveals a subchondral cyst (arrow), an articular defect in the lateral tibial plateau, and a large knee effusion (arrowhead).
Página 46 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 7: Coronal T1-weighted image 2 weeks after injury is unremarkable.
Media file 8: Coronal T1-weighted image 1 year after injury demonstrates a subchondral cyst (arrowhead) in the
Página 47 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

lateral tibial plateau.
Media file 9: Anteroposterior radiograph of the knee reveals osteochondritis dissecans in the lateral aspect (arrowhead) of the medial femoral condyle.
Página 48 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 10: Axial CT of the knee demonstrates a completely detached osteochondral fracture (arrowhead) in the lateral aspect of the medial femoral condyle.
Media file 11: Lateral radiograph of the knee reveals a calcified loose body (white arrowhead) in the infrapatellar
Página 49 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

fat pad and lucency in the articular surface of the patella (black arrowhead).
Media file 12: Sagittal T2-weighted image of the knee demonstrates a calcified loose body (white arrowhead) in the infrapatellar fat pad.
Página 50 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 13: Sagittal T2-weighted image of the knee (adjacent to the image in Picture 12) reveals subchondral bone marrow edema (white arrowhead) and an articular cartilage defect in the patella.
Página 51 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 14: Coronal T1-weighted image of the knee demonstrates subchondral bone marrow edema (arrowhead) in the medial tibial plateau.
Media file 15: Sagittal T2-weighted image of the knee reveals an articular defect (arrow) and subchondral bone marrow edema (arrowhead) in the medial tibial plateau.
Página 52 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 16: Drawing of osteochondritis dissecans of the capitellum with localized subchondral bony flattening and a normal articular surface.
Página 53 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 17: Drawing of osteochondritis dissecans of the capitellum with a nondisplaced osteochondral fragment.
Página 54 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 18: Drawing of osteochondritis dissecans of the capitellum with a slightly displaced fragment.
Media file 19: Drawing of osteochondritis dissecans of the capitellum with a capitellar defect.
Página 55 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 20: Anterior longitudinal sonogram reveals a stable lesion with localized subchondral bony flattening (arrows) and a normal outline of the articular cartilage (corresponding to Picture 16 in Multimedia; courtesy of Dr Masatoshi Takahara).
Media file 21: Posterior longitudinal sonogram demonstrates a stable lesion with a nondisplaced bone fragment (asterisk), intact articular surface (arrowheads), and a narrow gap formation (arrow; corresponding to Picture 17 in Multimedia; courtesy of Dr Masatoshi Takahara).
Página 56 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 22: Posterior longitudinal sonogram reveals an unstable lesion with a slightly displaced fragment (asterisk) and a wide gap formation (arrows; corresponding to Picture 18 in Multimedia; courtesy of Dr Masatoshi Takahara).
Media file 23: Anterior longitudinal sonogram demonstrates an unstable lesion with a capitellar defect (arrow; corresponding to Picture 19 in Multimedia; courtesy of Dr Masatoshi Takahara).
Página 57 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 24: Anteroposterior radiograph of the leg reveals osteochondritis dissecans in the medial talar dome (arrowhead).
Media file 25: Lateral radiograph of the leg demonstrates osteochondritis dissecans in the posterior aspect of the talar dome (arrowhead).
Página 58 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print
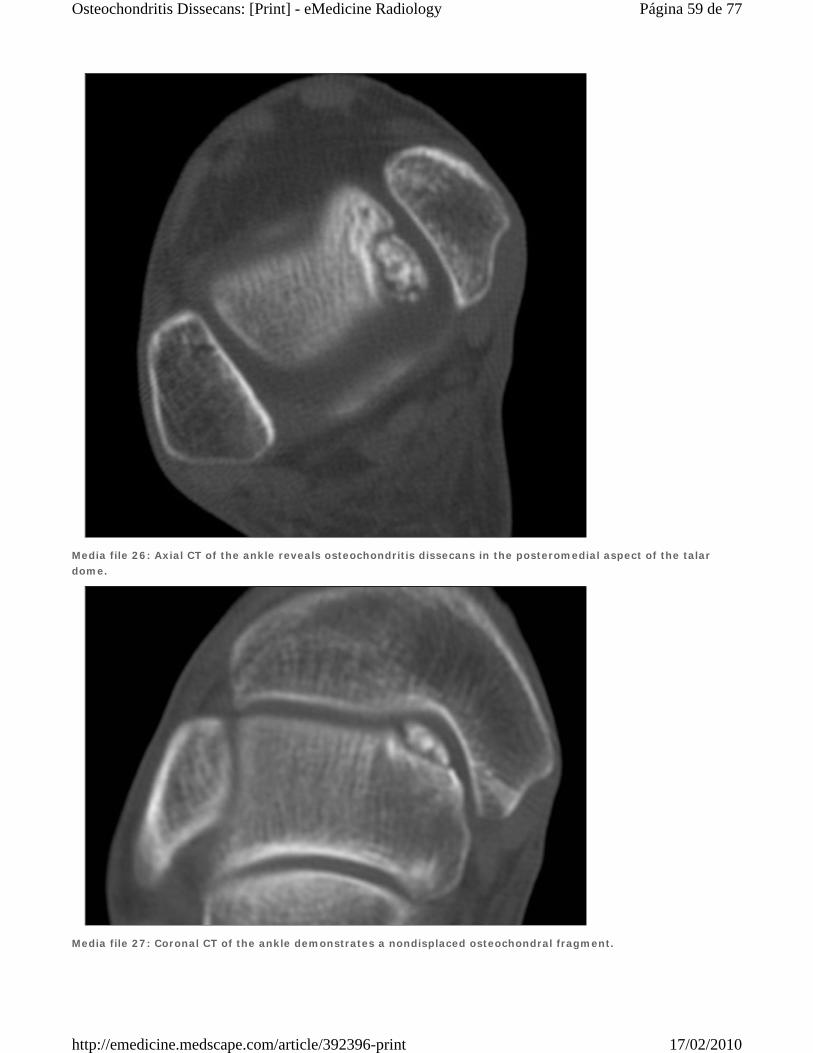
Media file 26: Axial CT of the ankle reveals osteochondritis dissecans in the posteromedial aspect of the talar dome.
Media file 27: Coronal CT of the ankle demonstrates a nondisplaced osteochondral fragment.
Página 59 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 28: Sagittal reformatted image of the ankle reveals a nondisplaced osteochondral fragment.
Media file 29: Mortise view of the ankle demonstrates a linear calcified loose body (arrowhead) in the talofibular joint and lucency in the lateral talar dome (arrow).
Página 60 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 30: Lateral view of the ankle reveals a linear calcified loose body (arrowhead).
Página 61 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 31: Axial T1-weighted image at the level of the ankle joint demonstrates abnormal low-signal intensity in the anterolateral aspect of the talus (arrowhead).
Página 62 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 32: Coronal T2-weighted image demonstrates an articular defect and abnormal high-signal intensity in the lateral talar dome consistent with osteochondritis dissecans.
Página 63 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 33: Mortise view of the ankle reveals lucency in the central portion of the tibial plafond (arrowhead).
Media file 34: Lateral view of the ankle reveals loss of the sharp cortical line (arrowhead) in the posterior aspect of the tibial plafond.
Página 64 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print
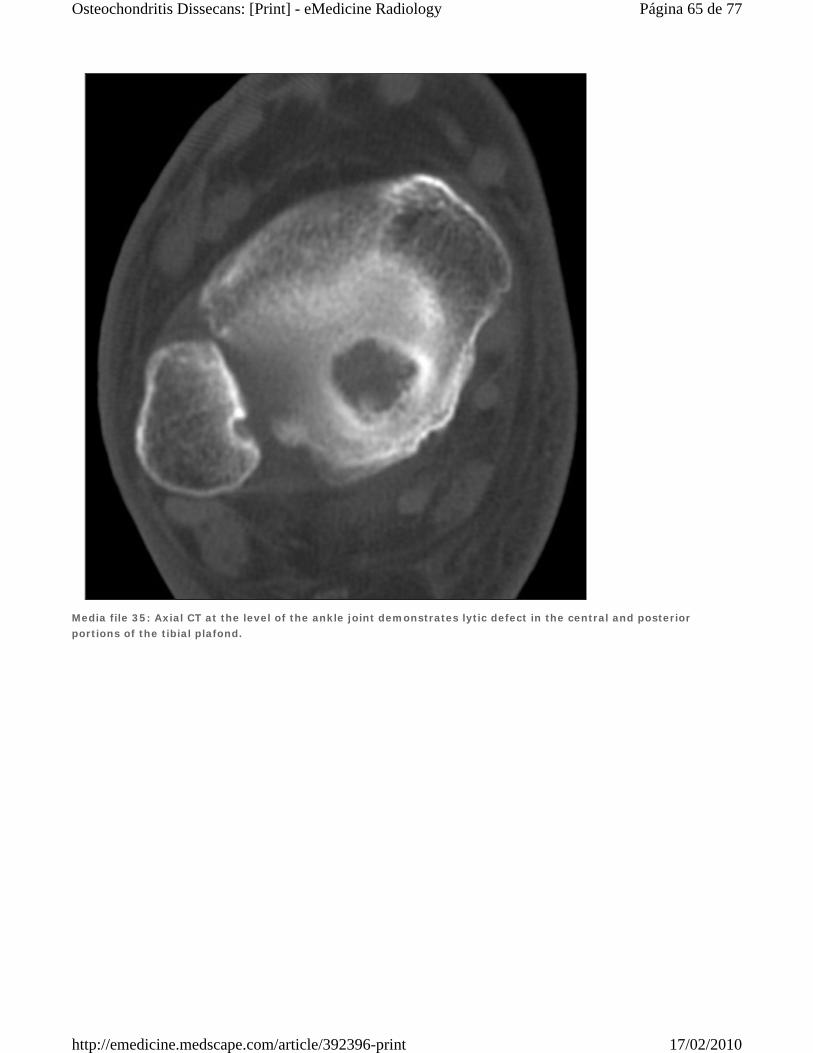
Media file 35: Axial CT at the level of the ankle joint demonstrates lytic defect in the central and posterior portions of the tibial plafond.
Página 65 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 36: Coronal CT of the ankle demonstrates a cortical depression in the tibial plafond.
Media file 37: Lateral radiograph of the ankle reveals a cortical depression and loss of the sharp cortical line in the proximal articular surface of the tarsal navicular (arrowhead).
Página 66 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 38: Sagittal T1-weighted image of the ankle confirms osteochondritis dissecans of the tarsal navicular (arrowhead).
Página 67 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 39: Coronal T2-weighted image of the ankle reveals a central depression in the tarsal navicular (arrowhead) consistent with osteochondritis dissecans.
Página 68 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 40: Axial T2-weighted image of the ankle demonstrates subchondral bone marrow edema (arrowhead) in the proximal aspect of the tarsal navicular.
Página 69 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 41: Oblique, coronal T2-weighted image of the right shoulder demonstrates a developmental defect in the glenoid filled with fluid (arrowhead). Note the central location and absence of subchondral bone marrow edema. This is a normal variant.
Página 70 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print
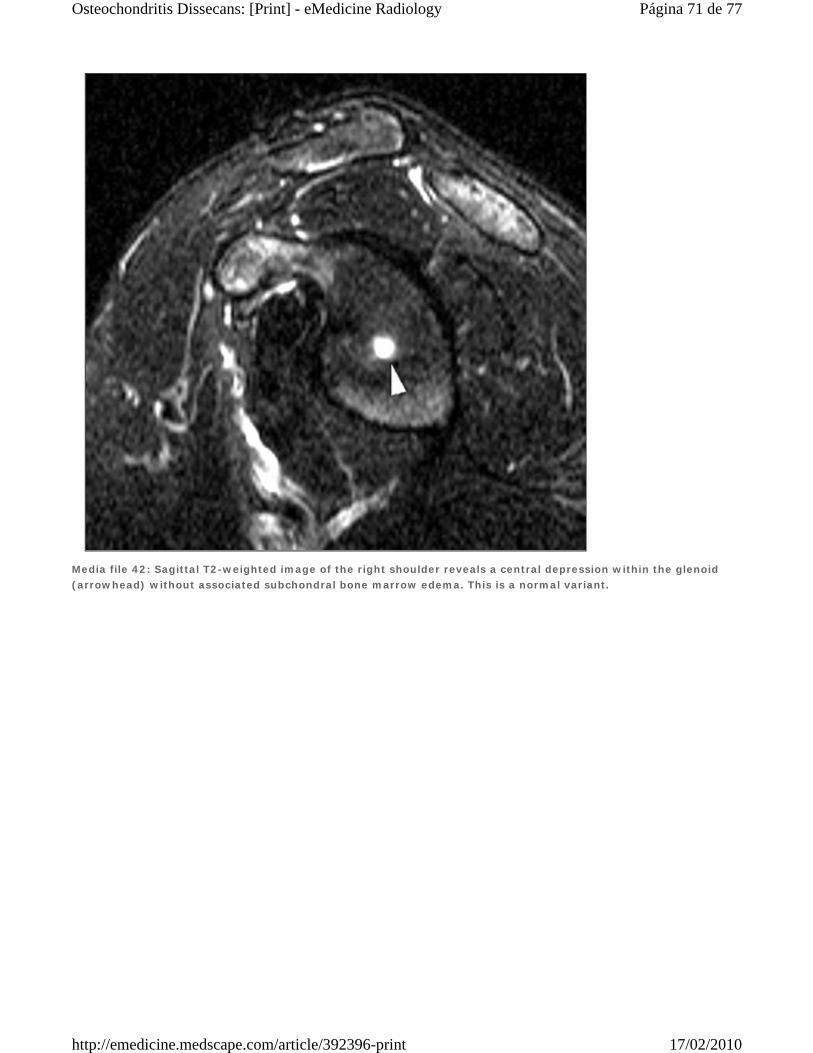
Media file 42: Sagittal T2-weighted image of the right shoulder reveals a central depression within the glenoid (arrowhead) without associated subchondral bone marrow edema. This is a normal variant.
Página 71 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 43: Oblique sagittal T2-weighted fat-suppression image reveals a large lesion in the anterior and inferior aspects of glenoid.
Media file 44: Oblique coronal T1-weighted image demonstrates a hypointense lesion in the inferior half of the glenoid.
Página 72 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 45: Oblique coronal T2-weighted fat-suppression image demonstrates a hyperintense osteochondral lesion in the inferior half of the glenoid. Note the fluid in the subacromial/subdeltoid bursa and the supraspinatus tendon tear.
Página 73 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Media file 46: Axial-gradient recall image reveals an osteochondral lesion in the anterior half of the glenoid.
References
1. Pappas AM. Osteochondrosis dissecans. Clin Orthop. Jul-Aug 1981;(158):59-69. [Medline].
2. Adachi N, Deie M, Nakamae A, Ishikawa M, Motoyama M, Ochi M. Functional and radiographic outcome of stable juvenile
osteochondritis dissecans of the knee treated with retroarticular drilling without bone grafting. Arthroscopy. Feb 2009;25(2):145-
52. [Medline].
3. Kijowski R, Blankenbaker DG, Shinki K, Fine JP, Graf BK, De Smet AA. Juvenile versus adult osteochondritis dissecans of the
knee: appropriate MR imaging criteria for instability. Radiology. Aug 2008;248(2):571-8. [Medline].
4. Douglas G, Rang M. The role of trauma in the pathogenesis of the osteochondroses. Clin Orthop. Jul-Aug 1981;(158):28-
32. [Medline].
5. Omer GE Jr. Primary articular osteochondroses. Clin Orthop. Jul-Aug 1981;(158):33-40. [Medline].
6. Aichroth P. Osteochondritis dissecans of the knee. A clinical survey. J Bone Joint Surg [Br]. Aug 1971;53(3):440-7. [Medline].
7. Bachmann G, Jurgensen I, Siaplaouras J. [The staging of osteochondritis dissecans in the knee and ankle joints with MR
tomography. A comparison with conventional radiology and arthroscopy]. Rofo Fortschr Geb Rontgenstr Neuen Bildgeb
Verfahr. Jul 1995;163(1):38-44. [Medline].
8. Gregersen HE, Rasmussen OS. Ultrasonography of osteochondritis dissecans of the knee. A preliminary report. Acta
Radiol. Sep-Oct 1989;30(5):552-4. [Medline].
9. Linden B, Nilsson BE. Strontium-85 uptake in knee joints with osteochondritis dissecans. Acta Orthop Scand. Dec 1976;47
(6):668-71. [Medline].
10. Stoffelen D, Renson L, Fabry G. Osteochondritis dissecans of the acetabulum. A report of two cases. J Pediatr
Orthop. 1992;12:91-2.
11. Wood JB, Klassen RA, Peterson HA. Osteochondritis dissecans of the femoral head in children and adolescents: a report of 17
cases. J Pediatr Orthop. May-Jun 1995;15(3):313-6. [Medline].
12. Choi YS, Cohen NA, Potter HG, Mintz DN. Magnetic resonance imaging in the evaluation of osteochondritis dissecans of the
patella. Skeletal Radiol. Oct 2007;36(10):929-35. [Medline].
13. Crawford DC, Safran MR. Osteochondritis dissecans of the knee. J Am Acad Orthop Surg. Feb 2006;14(2):90-100. [Medline].
14. Kocher MS, Tucker R, Ganley TJ, Flynn JM. Management of osteochondritis dissecans of the knee: current concepts review. Am
J Sports Med. Jul 2006;34(7):1181-91. [Medline].
15. Linden B. The incidence of osteochondritis dissecans in the condyles of the femur. Acta Orthop Scand. Dec 1976;47(6):664-
7. [Medline].
16. Detterline AJ, Goldstein JL, Rue JP, Bach BR Jr. Evaluation and treatment of osteochondritis dissecans lesions of the knee. J
Knee Surg. Apr 2008;21(2):106-15. [Medline].
17. Singer KM, Roy SP. Osteochondrosis of the humeral capitellum. Am J Sports Med. Sep-Oct 1984;12(5):351-60. [Medline].
18. Schenck RC Jr, Athanasiou KA, Constantinides G. A biomechanical analysis of articular cartilage of the human elbow and a
potential relationship to osteochondritis dissecans. Clin Orthop. Feb 1994;(299):305-12. [Medline].
19. Kijowski R, De Smet AA. MRI findings of osteochondritis dissecans of the capitellum with surgical correlation. AJR Am J
Roentgenol. Dec 2005;185(6):1453-9. [Medline].
20. Kijowski R, De Smet AA. Radiography of the elbow for evaluation of patients with osteochondritis dissecans of the
capitellum. Skeletal Radiol. May 2005;34(5):266-71. [Medline].
Página 74 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

21. Bui-Mansfield LT, Kline M, Chew FS. Osteochondritis dissecans of the tibial plafond: imaging characteristics and a review of the
literature. AJR Am J Roentgenol. Nov 2000;175(5):1305-8. [Medline].
22. Canosa J. Mirror image osteochondral defects of the talus and distal tibia. Int Orthop. 1994;18(6):395-6. [Medline].
23. Athanasiou KA, Niederauer GG, Schenck RC Jr. Biomechanical topography of human ankle cartilage. Ann Biomed Eng. Sep-
Oct 1995;23(5):697-704. [Medline].
24. Bauer M, Jonsson K, Linden B. Osteochondritis dissecans of the ankle. A 20-year follow-up study. J Bone Joint Surg
[Br]. Jan 1987;69(1):93-6. [Medline].
25. Lindholm TS, Osterman K, Vankka E. Osteochondritis dissecans of elbow, ankle and hip: a comparison survey. Clin
Orthop. May 1980;(148):245-53. [Medline].
26. Ferkel RD, Sgaglione NA. Arthroscopic treatment of osteochondral lesions of the talus: Long-term results. Orthop Trans. 1993-
4;17:1011.
27. Perumal V, Wall E, Babekir N. Juvenile osteochondritis dissecans of the talus. J Pediatr Orthop. Oct-Nov 2007;27(7):821-
5. [Medline].
28. Elias I, Zoga AC, Morrison WB, Besser MP, Schweitzer ME, Raikin SM. Osteochondral lesions of the talus: localization and
morphologic data from 424 patients using a novel anatomical grid scheme. Foot Ankle Int. Feb 2007;28(2):154-61. [Medline].
29. Bui-Mansfield LT, Lenchik L, Rogers LF. Osteochondritis dissecans of the tarsal navicular bone: imaging findings in four
patients. J Comput Assist Tomogr. Sep-Oct 2000;24(5):744-7. [Medline].
30. Bowen JR, Kumar VP, Joyce JJ 3d. Osteochondritis dissecans following Perthes' disease. Arthroscopic- operative treatment. Clin
Orthop. Aug 1986;(209):49-56. [Medline].
31. Goldman AB, Hallel T, Salvati EM. Osteochondritis dissecans complicating Legg-Perthes disease. A report of four
cases. Radiology. Dec 1976;121(3 Pt. 1):561-6. [Medline].
32. Kamhi E, MacEwen GD. Osteochondritis dissecans in Legg-Calve-Perthes disease. J Bone Joint Surg [Am]. Jun 1975;57(4):506-
9. [Medline].
33. Lindén B, Jonsson K, Redlund-Johnell I. Osteochondritis dissecans of the hip. Acta Radiol. Jan 2003;44(1):67-71. [Medline].
34. Hamada S, Hamada M, Nishiue S. Osteochondritis dissecans of the humeral head. Arthroscopy. 1992;8(1):132-7. [Medline].
35. Takahara M, Ogino T, Tsuchida H. Sonographic assessment of osteochondritis dissecans of the humeral capitellum. AJR Am J
Roentgenol. Feb 2000;174(2):411-5. [Medline].
36. Debeer P, Brys P. Osteochondritis dissecans of the humeral head: clinical and radiological findings. Acta Orthop
Belg. Aug 2005;71(4):484-8. [Medline].
37. Mahirogullari M, Chloros GD, Wiesler ER, Ferguson C, Poehling GG. Osteochondritis dissecans of the humeral head. Joint Bone
Spine. Aug 31 2007;[Medline].
38. Aghasi M, Rzetelni V, Axer A. Osteochondritis dissecans of the carpal scaphoid. J Hand Surg [Am]. Jul 1981;6(4):351-
2. [Medline].
39. Guelpa G, Chamay A, Lagier R. Bilateral osteochondritis dissecans of the carpal scaphoid. A radiological and anatomical study of
one case. Int Orthop. 1980;4(1):25-30. [Medline].
40. Viegas SF. Arthroscopic treatment of osteochondritis dissecans of the scaphoid. Arthroscopy. 1988;4(4):278-81. [Medline].
41. Ishibe M, Ogino T, Sato Y. Osteochondritis dissecans of the distal radioulnar joint. J Hand Surg [Am]. Sep 1989;14(5):818-
21. [Medline].
42. Nielsen NA. Osteochondritis dissecans capituli humeri. Acta Orthop Scand. 1933;4:307.
Página 75 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

43. Pill SG, Ganley TJ, Milam RA, Lou JE, Meyer JS, Flynn JM. Role of magnetic resonance imaging and clinical criteria in predicting
successful nonoperative treatment of osteochondritis dissecans in children. J Pediatr Orthop. Jan-Feb 2003;23(1):102-
8. [Medline].
44. Pritsch M, Horoshovski H, Farine I. Arthroscopic treatment of osteochondral lesions of the talus. J Bone Joint Surg
[Am]. Jul 1986;68(6):862-5. [Medline].
45. Cheng MS, Ferkel RD, Applegate GR. Osteochondral lesion of the talus: A radiologic and surgical comparison. Paper presented
at: Annual Meeting of the Academy of Orthopaedic Surgeons;. February 1995;New Orleans, LA.
46. Keats T. Atlas of Normal Roentgen Variants That May Simulate Disease. 6th ed. Mosby-Year Book;1996:357.
47. Berndt AL, Harty M. Transchondral fracture (osteochondritis dissecans) of the talus. J Bone Joint Surg [Am]. 1959;41(A):988-
1020.
48. Anderson IF, Crichton KJ, Grattan-Smith T. Osteochondral fractures of the dome of the talus. J Bone Joint Surg
[Am]. Sep 1989;71(8):1143-52. [Medline].
49. McCullough RW, Gandsman EJ, Litchman HE. Dynamic bone scintigraphy in osteochondritis dissecans. Int Orthop. 1988;12
(4):317-22. [Medline].
Keywords
osteochondritis dissecans, osteochondral fracture, osteochondrosis, osteochondral defect, osteochondral lesion, OCD
Contributor Information and Disclosures
Author
Liem T Bui-Mansfield, MD, Clinical Associate in the Division of Radiologic Sciences, Department of Radiology, Wake Forest University
School of Medicine
Liem T Bui-Mansfield, MD is a member of the following medical societies: American Roentgen Ray Society, Radiological Society of North
America, and Society of Skeletal Radiology
Disclosure: Nothing to disclose.
Medical Editor
Leon Lenchik, MD, Director, Densitometry Minifellowship, Assistant Professor, Department of Radiology, Wake Forest University
Medical Center
Leon Lenchik, MD is a member of the following medical societies: American College of Radiology, American Roentgen Ray Society, and
Radiological Society of North America
Disclosure: Nothing to disclose.
Pharmacy Editor
Bernard D Coombs, MB, ChB, PhD, Consulting Staff, Department of Specialist Rehabilitation Services, Hutt Valley District Health
Board, New Zealand
Disclosure: Nothing to disclose.
Managing Editor
Javier Beltran, MD, Chair, Department of Radiology, Maimonides Medical Center
Disclosure: Nothing to disclose.
CME Editor
Robert M Krasny, MD, Consulting Staff, Department of Radiology, The Angeles Clinic and Research Institute
Robert M Krasny, MD is a member of the following medical societies: American Roentgen Ray Society and Radiological Society of North
America
Disclosure: Nothing to disclose.
Chief Editor
Página 76 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print

Felix S Chew, MD, MBA, EdM, Professor, Department of Radiology, Vice Chairman for Radiology Informatics, Section Head of
Musculoskeletal Radiology, University of Washington
Felix S Chew, MD, MBA, EdM is a member of the following medical societies: American Roentgen Ray Society, Association of University
Radiologists, and Radiological Society of North America
Disclosure: Nothing to disclose.
Further Reading
Related eMedicine topics Osteochondritis Dissecans [Orthopedic Surgery] Osteochondral Lesions of the Talus Humeral Capitellum Osteochondritis Dissecans Knee Osteochondritis Dissecans Clinical guideline ACR Appropriateness Criteria® nontraumatic knee pain
© 1994- 2010 by Medscape. All Rights Reserved (http://www.medscape.com/public/copyright)
Página 77 de 77Osteochondritis Dissecans: [Print] - eMedicine Radiology
17/02/2010http://emedicine.medscape.com/article/392396-print





























