Embed Size (px)
Citation preview


Nam
e of the Com
pany : ……
……
……
……
……
……
……
...……
…
Address : …
……
……
……
……
……
……
……
….…
.……
……
.......
Tel……
……
……
Mobile:…
……
……
……
..Fax……
…....…
……
…
Website..........…
……
…..............…
……
……
……
……
.....................
E-m
ail:……
……
……
……
……
……
…..............................................
ContactPerson.......................................................................................
Designation :…
……
……
……
……
…................................................
Product/Services on Display :…
……
……
……
……
……
……
……
…
Nam
e of the Facia : ……
……
……
……
……
……
……
....................
HE
RB
AL E
XP
O
SPACE APPLICATION FO
RM FO
R EXHIBITIO
N
PAR
TIC
IPAT
ION
FE
E
SHE
LL
SCH
EM
E :
Facility : Shell stalls are w
ith three side walls, Facia B
oard with
Com
pany name, O
ne Table, Two C
hairs, Floor Carpet, T
hree SpotL
ights, One Plug Point and one D
ust Bin w
ith White C
loth Ceiling.
Exhibitors need to get their ow
n display material.
No. of Stall
Area in Sq. M
trs.Tariff
One Stall
3m X
3m = 9 Sq. M
trs.R
s. 8,000/-
Two Stalls
6m X
3m = 18 Sq. M
trs.R
s. 15,000/-
Three Stalls
9m X
3m = 27 Sq. M
trs.R
s. 21,000/-
Osh
ad
hi-2
00
9
SPAC
E R
EQ
UIR
EM
EN
T :
Area R
equired ……
……
……
…. (Sq. M
tr.)
Paym
ent enclosed Rs. …
……
……
……
.......................... DD
/ Cheque (L
ocal)
No…
……
……
……
...……
.........................Dt...........…
……
……
…....D
rawn on
……
……
……
……
……
……
……
.……
.....……
in favour of “C.E
.O., A
.P.
Medicinal &
Arom
atic Plants Board”, payable at H
yderabad.
Please Send To :C
hief Executive O
fficer,A
P Medicinal &
Arom
atic Plants Board,
6th Floor, A
PGL
I Building, T
ilak Road,
Abids, H
yderabad – 500 001.A
uthorized SignatoryPhone : 040-40047795Tele fax N
o. : 040-66364094D
t:E
-mail : apm
aboard@gm
ail.com
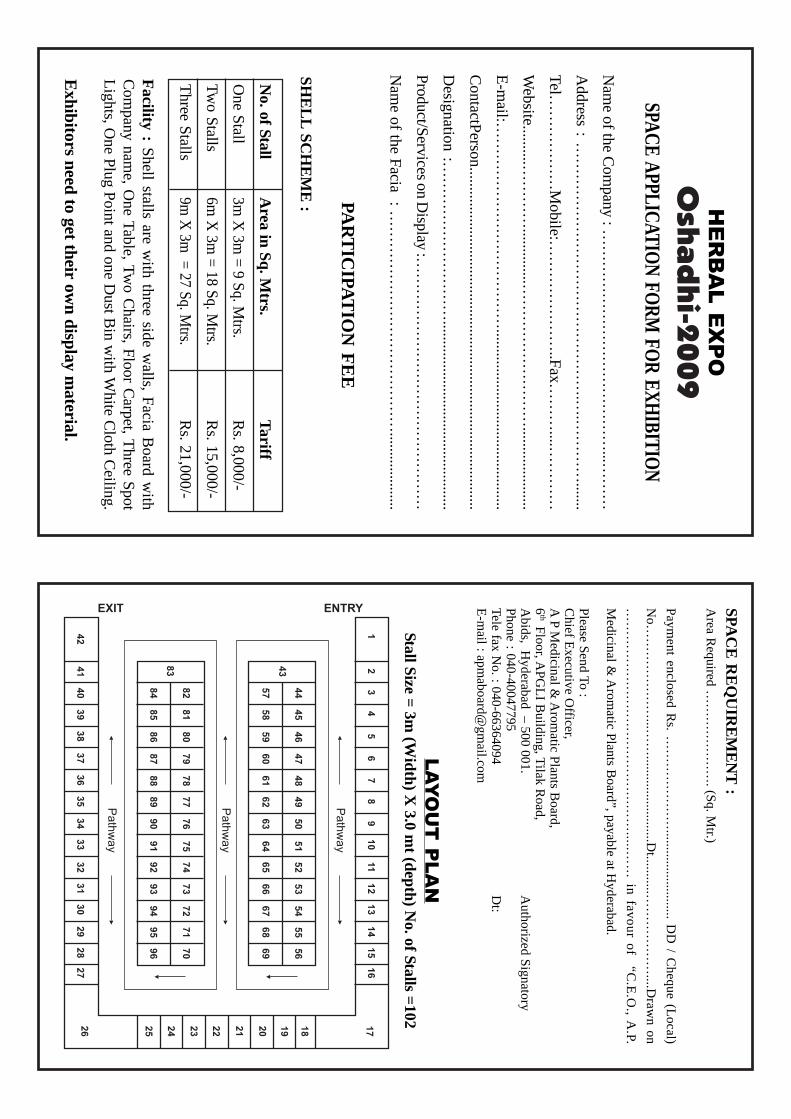
LA
YO
UT
P
LA
N
Stall Size = 3m (W
idth) X 3.0 m
t (depth) No. of Stalls =102

Nam
e of the Participant :
Full Address : __________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
Tel :……
……
……
……
……
Mobile :…
……
……
……
……
….......
Fax :……
……
……
…W
ebsite ……
……
……
……
……
……
……
.
E-m
ail :……
……
……
……
……
……
Present Activity:…
……
……
……
……
……
……
……
…..................
HE
RB
AL E
XP
O
DE
LE
GA
TE
RE
GIST
RA
TIO
N F
OR
MF
OR
SEM
INA
R
Osh
ad
hi-2
00
9D
EL
EG
AT
E F
EE
FO
R T
HE
SEM
INA
R
Kindly enroll m
e as a delegate for the Workshop
Payment enclosed R
s. ……
……
……
.................................................
DD
/Cheque (L
ocal) No…
……
……
……
……
…...............................
Dt. …
……
……
….. D
rawn on …
……
……
.……
......… in favour of
“C.E
.O., A
.P. ME
DIC
INA
L &
AR
OM
AT
IC PL
AN
TS B
OA
RD
”,
payable at Hyderabad.
Authorized Signatory
Dt:
To :
The C
hief Executive O
fficer,A
P Medicinal &
Arom
atic Plants Board,
6th Floor, A
PGL
I Building, T
ilak Road,
Abids, H
yderabad – 500 001.Phone : 040-40047795Tele fax N
o. : 040-66364094E
-mail : apm
aboard@gm
ail.com
Before 30
th Nov, 2009
:R
s. 500/- (For Single P
erson)A
fter 30th N
ov, 2009:
Rs. 600/- (F
or Single Person)
Spot Registration
:R
s. 700/- (For Single P
erson)




















![APGLI NEW Proposal Form[2]](https://img.dokumen.tips/doc/110x75/5571f40749795947648ee801/apgli-new-proposal-form2.jpg)
