Embed Size (px)
Citation preview
Dear HCPro Customer:
Enclosed is your latest supplement to the OSHA Program Manual for Medical Facilities. This supplement is designed tokeep your product up to date.
If you have any questions about your subscription, please contact our Customer Service department at 800-650-6787 ore-mail [email protected]. At HCPro, customer comments and suggestions are very important to us—let usknow how we can serve you better.
Please insert these new and revised pages as indicated, and keep these filing instructions at the front of your book.
FILING INSTRUCTIONS
Rev. 9/14 OPMFMF Supplement to OSHA Program Manual for Medical Facilities
VISIT www.hcmarketplace.com for the latest compliance and training information.
Remove Insert Reason for Change
Title page Title page updated
xv through xx xv through xxi OSHA Program Manual Contents—updated
Tab 6 Contents Tab 6 Contents updated
6-29 through 6-36 6-29 through 6-38 Tab 6: TB/Infection Prevention and Control Plan—updated
(Multidrug-Resistant Organisms (MDRO), CDC Classification of MDRO
Threats, MDRO Prevention and Control, Colonization vs. Infection,
MDRO Transmission, How Antibiotic Resistance Happens)
September 2014 Revisions

About the AuthorSheila Dunn, DA, MT (ASCP), holds a doctoral degree in clinical laboratory science from the Catholic
University of America in Washington, DC. She has helped thousands of outpatient medical facilities comply
with federal regulations such as CLIA and OSHA through her presentations at a nationwide seminar series.
She has written more than 150 articles about regulatory issues and healthcare delivery systems and serves
as an advisor to numerous companies.
14G
©2005–2014 HCPro, a division of BLR. All rights reserved, including right of reproduction. The author(s) and their agent(s) have made every reasonable effort in the preparation of this publication to ensure the accuracy of the information. However, the information in this book is sold without warranty, either expressed or implied. The authors, the editors, their agents, and the publishers will not be liable for any damages caused or alleged to be caused directly, indirectly, incidentally, or consequentially by the information in this publication. This publication cannot and does not provide specific information for a user’s exact situation. Users of this publication should exercise their own judgment and, where appropriate, seek the assistance of legal counsel regarding their particular situation.
HCPro, a division of BLR75 Sylvan Street, Suite A-101
Danvers, MA 01923Tel: 800/650-6787Fax: 800/639-8511
www.hcmarketplace.com
OSHAPROGRAMMANUALfor Medical Facilities
OSHA Program Manual for Medical Facilities is published by HCPro, a division of BLR.
Copyright © 2014 HCPro, a division of BLR.
All rights reserved. Printed in the United States of America. 5 4 3 2 1
ISBN: 978-1-60146-743-0
No part of this publication may be reproduced, in any form or by any means, without prior written consent of
HCPro, a division of BLR, or the Copyright Clearance Center (978-750-8400). Please notify us immediately
if you have received an unauthorized copy.
HCPro, a division of BLR, provides information resources for the healthcare industry.
HCPro, a division of BLR, is not affiliated in any way with The Joint Commission, which owns the JCAHO
and Joint Commission trademarks.
Sheila Dunn, DA, MT (ASCP), Author
Jay Kumar, Senior Managing Editor
Marge McFarlane, PhD, CHSP, CHFM, HEM, MEP, CHEP, Reviewer
Mike Mirabello, Senior Graphic Artist
Matt Sharpe, Senior Manager of Production
Elizabeth Petersen, Vice President
Advice given is general. Readers should consult professional counsel for specific legal, ethical, or
clinical questions.
Arrangements can be made for quantity discounts. For more information, contact:
HCPro, a division of BLR
75 Sylvan Street, Suite A-101
Danvers, MA 01923
Telephone: 800-650-6787 or 781-639-1872
Fax: 800-639-8511
E-mail: [email protected]
Visit HCPro online at: www.hcpro.com and www.hcmarketplace.com
9/14
Contents
xv
Respiratory Protection for Healthcare Workers: N95 Respirators or Medical Powered Air Purifying Respirators (PAPRs) ................ 610
Seal Checking N95 Respirators ......................................................................... 610Medical PAPRs ................................................................................................... 610
Employee TB Skin Testing (TST) ........................................................................................ 611Baseline Employee TST: The TwoStep Skin Test ...................................................... 612
TwoStep TST Interpretation ................................................................................ 612Interpreting the TST ..................................................................................................... 613
False Positive/False Negative TB Tests .............................................................. 613Workers Who Have Had BCG Vaccination .......................................................... 614
Periodic Retesting of Employees ................................................................................ 614Recording TST Results ............................................................................................... 614TST Record (Form 21) ................................................................................................ 615TST Declination (Form 22) .......................................................................................... 616
Evaluation and Management of Healthcare Employees Exposed to TB ............................. 617Employees with Symptoms of TB ................................................................................ 617Employees Who Have Been Exposed to a Known TB Patient .................................... 617Positive Employee Skin Tests and Skin Test Conversions ........................................... 617TB Exposure Log (Form 23) ......................................................................................... 619Decontaminating Patient Care Area and Equipment.................................................... 620
Employee Training ............................................................................................................... 620
Pandemic Influenza Plan and Other Infectious Diseases ........................ 6-21Prepandemic Planning ....................................................................................................... 621Once a Pandemic Is Announced .......................................................................................... 624OSHA Enforcement for a Pandemic .................................................................................... 626
Identifying Very High and High Exposure Risks .......................................................... 626Dealing with N95 Respirator Shortages ...................................................................... 627Prioritize Your Facility’s Use of N95 Respirators ......................................................... 627Documentation ............................................................................................................ 628
Pandemic Resources .......................................................................................................... 629
Multidrug-Resistant Organisms (MDRO) .................................................... 6-29CDC Classification of MDRO Threats ................................................................................ 629MDRO Prevention and Control ............................................................................................ 631Colonization vs. Infection .................................................................................................... 631MDRO Transmission ........................................................................................................... 632Patient Precautions ............................................................................................................. 632
Hand Hygiene ............................................................................................................. 633Contact Precautions .................................................................................................... 633
Environmental Cleaning ...................................................................................................... 634Infected Employees ............................................................................................................. 635MDRO Resources ............................................................................................................... 636
Pertussis and Worker Vaccination ............................................................. 6-36Supplement: How Antibiotic Resistance Happens ................................... 6-38Supplement: Guide to Infection Prevention in Outpatient Settings: Minimum Expectations for Safe Care ......................................................... S1–S10

Contents
xvi
TAB 7: The Hazard Communication StandardA Quick Look at HazCom ............................................................................. 7-1
Determining Which Chemicals Are Hazardous .................................................................... 71Routes of Exposure to Hazardous Substances ................................................................... 72
Material Safety Data Sheets/Safety Data Sheets ........................................ 7-3Examples of Substances Requiring MSDS (SDS) ............................................................... 73Substances Not Requiring MSDS (SDS) ............................................................................. 73MSDS (SDS) Flowchart Determination ................................................................................ 74Information Required on MSDS (SDS) ................................................................................ 74How to Get MSDS (SDS) ..................................................................................................... 75Where to Keep MSDS (SDS) .............................................................................................. 75
Classification of Hazardous Substances ................................................... 7-6Flammable & Combustible Liquids ...................................................................................... 76
Storage of Hazardous Substances .............................................................. 7-7Hazardous Chemicals with Permissible Exposure Limits (PEL) ............. 7-8Labeling Hazardous Substances ................................................................ 7-8
HazCom Pictograms and Hazard Statements ..................................................................... 78Pictograms ........................................................................................................................... 79NFPA Label System ............................................................................................................. 710
Safety Tips for Working with Hazardous Substances ............................... 7-10Hazardous Chemical Waste Packaging & Disposal .................................. 7-11Medications Security & Disposal ................................................................ 7-12
Security for Prescription Drugs ............................................................................................ 712Security for Controlled Substances ...................................................................................... 712Disposal of Prescription Drugs ............................................................................................ 713Disposal of Hazardous Drugs .............................................................................................. 713
Medical Consultation & Injury Evaluation .................................................. 7-13HazCom Recordkeeping .............................................................................. 7-14
TAB 8: DecontaminationA Quick Look at Decontamination .............................................................. 8-1Routine Housekeeping Procedures ............................................................ 8-1
Decontaminating Work Surfaces ......................................................................................... 81Sample Housekeeping Schedule (Form 7) .......................................................................... 83
Spill Containment Plan ................................................................................. 8-4Spill Cleanup Procedures ................................................................................................... 84Spills That Contain Broken Glass or Sharp Objects ............................................................ 85Chemical Spill Cleanup Procedures ................................................................................... 85Chemical Exposure to Skin ................................................................................................. 85Mercury Spills ...................................................................................................................... 86Cytotoxic Drug Spill Cleanup .............................................................................................. 86
Contents
xvii
Decontamination of Medical Instruments & Equipment ........................... 8-7When to Sterilize .................................................................................................................. 87Precleaning Instruments Prior to HighLevel Disinfection or Sterilization ............................ 88Sterilization .......................................................................................................................... 89Quality Checks for Sterilization ............................................................................................ 89HighLevel Disinfecting ........................................................................................................ 810
Using Glutaraldehyde .................................................................................................. 811Sterilant Safety ............................................................................................................ SupplementGlutaraldehyde Spills ................................................................................................... 813Sources for Chemical Air Monitoring ........................................................................... 814Testing the Potency of Glutaraldehyde ....................................................................... 814Disposing of Glutaraldehyde ....................................................................................... 814
Cleaning Transvaginal and Transrectal Ultrasound Probes ................................................ 814Disinfect Transvaginal and Transrectal Probes After Each Use .................................. 815Cleaning Ultrasound Transducers ............................................................................... 815
Decontaminating Vaginal Specula ....................................................................................... 815Keeping Employees Safe During Instrument Disinfection ................................................... 816Decontaminating Semicritical Patient Care Equipment ...................................................... 816Decontaminating Noncritical Patient Care Equipment ....................................................... 817Decontaminating Personal Protective Equipment (PPE) ..................................................... 818
Eyewashes ..................................................................................................... 8-18Number & Placement of Eyewash Stations ......................................................................... 818Eyewash Maintenance ........................................................................................................ 819
Waste Disposal ............................................................................................. 8-20Biomedical Waste Disposal ................................................................................................. 820Hazardous Waste Disposal ................................................................................................. 821Waste Handling & Storage ................................................................................................... 823
TAB 9: Specialty ServicesAbout this Section ........................................................................................ 9-1Working Safely with Cytotoxic Drugs ......................................................... 9-1
NIOSH Hazardous Drug List for Healthcare ........................................................................ 91Effects of CD Exposure on Health ....................................................................................... 91Safe Work Practices ............................................................................................................ 92Clothing ................................................................................................................................ 92Drug Preparation & Administration ...................................................................................... 92Sample List of Drugs that Should be Handled as Hazardous ............................................. Supplement
Selecting Biological Safety Cabinets (BSC) ................................................................ 93Cleaning the Drug Preparation Area ............................................................................ 94
Caring for Patients Receiving CDs ...................................................................................... 94Waste Disposal .................................................................................................................... 94Spill Cleanup ....................................................................................................................... 95
Suggested Spill Kit Components ................................................................................. 95CD Receiving ....................................................................................................................... 96CD Storage .......................................................................................................................... 96CD Transport ....................................................................................................................... 96
Contents
xviii
Employee Training ............................................................................................................... 96Employee Medical Surveillance ........................................................................................... 97Employee Exposure ............................................................................................................. 97
Gas Cylinder Safety ...................................................................................... 9-7Electrosurgical Safety (Laser, LEEPs) ........................................................ 9-9
Safe Work Practices ............................................................................................................ 910
Surgical Safety .............................................................................................. 9-11General PPE Indications for Surgery ................................................................................... 911
Surgical Gowns ........................................................................................................... 911Surgical Gloves ........................................................................................................... 912Face and Eye Protection ............................................................................................. 912Headwear .................................................................................................................... 913Shoe Covers ................................................................................................................ 913Surgical Drapes ........................................................................................................... 913
Safe Sharp Strategies for the Surgical Setting .................................................................... 913Scalpels ....................................................................................................................... 913Suture Needles ........................................................................................................... 913
Transferring Sharps Safely .................................................................................................. 914How to Use the Neutral Zone (NZ) .............................................................................. 914Tips for Minimally Invasive Surgeries .......................................................................... 915Safety Techniques for Operating on Patients Infected with Known Bloodborne Pathogens .................................................................................... 915
Preventing Surgical Fires .................................................................................................... 915
Laboratory Safety ......................................................................................... 9-16Laboratory Specimen Transport .......................................................................................... 917
Radiation Safety ............................................................................................ 9-18Regulation of the Medical Use of Nuclear Byproducts ........................................................ 918The “ALARA” Principle ......................................................................................................... 918Radiation Safety Guidelines for Personnel........................................................................... 919Radiation Safety Policies for the Facility .............................................................................. 919Ionizing Radiation Exposure Limits ...................................................................................... 920Special Precautions for Pregnant Workers .......................................................................... 920Lowlevel Radioactive Waste Disposal ................................................................................ 921NRC Notification, Reports, and Record ................................................................................ 921NRC Resources and Publications ........................................................................................ 922
Working Safely with Cryogenic Liquids ..................................................... 9-23Precautions for Handling Liquid Nitrogen ............................................................................ 923Storing Liquid Nitrogen ........................................................................................................ 924Personal Protective Equipment ........................................................................................... 924Liquid Nitrogen Disposal ...................................................................................................... 924Steps to Take if There Is Accidental Exposure .................................................................... 925
First Aid (cryogenic burns) ........................................................................................... 925First Aid (anoxia) .......................................................................................................... 925
Safe Vaccine Handling and Storage ........................................................... 9-26
Contents
xix
Waste Anesthetic Gases .............................................................................. 9-28Where Exposures Occur ...................................................................................................... 929Preventing Exposures .......................................................................................................... 929
Controls ....................................................................................................................... 930Medical Surveillance ............................................................................................................ 930Recordkeeping .................................................................................................................... 931More Information .................................................................................................................. 931
TAB 10: Employee TrainingA Quick Look at the Employee Training Program ..................................... 10-1Training Format ............................................................................................ 10-1
Checklist for an Effective Safety Training Session ............................................................... 102Interactive Safety Training Exercises .................................................................................. 102
General Safety ............................................................................................................. 103Fire Safety ................................................................................................................... 103Bloodborne Pathogens Safety ..................................................................................... 103Chemical Safety ........................................................................................................... 103TB Safety ..................................................................................................................... 104
Annual Employee Retraining ....................................................................... 10-5Bloodborne Pathogens Annual Training Contents ............................................................... 106Respiratory Protection Annual Training Contents ................................................................ 106Hazard Communication Annual Training Contents .............................................................. 107
New Employee Orientation .......................................................................... 10-7New Employee OSHA Orientation Checklist (Form 26) ...................................................... 108
Sample Tests with Answer Keys ................................................................. 10-10OSHA Annual Retraining: Sample Essay Test Questions (Form 28) ................................... 1011OSHA Annual Retraining: Sample Essay Test—Answer Key .............................................. 1012OSHA Annual Retraining: Sample Multiple Choice Test Questions (Form 29) .................... 1013OSHA Annual Retraining: Sample Multiple Choice Test—Answer Key ............................... 1015OSHA Annual Retraining: Sample True/False Test Questions (Form 30) ............................ 1016OSHA Annual Retraining: Sample True/False Test—Answer Key ....................................... 1017
Documenting Employee Training ................................................................ 10-17Annual Safety Training Record (Form 27) ................................................... 10-18
TAB 11: Master Record FormsGeneral Equipment and Facility Records
Safety Report ....................................................................................................................... Form 1Autoclave Log ...................................................................................................................... Form 2Eyewash Station Weekly Check Log ................................................................................... Form 2AAnnual OSHA Program (Exposure Control Plan) Review ................................................... Form 3Weekly Facility Review Checklist ........................................................................................ Form 4AMonthly Facility Review Checklist ....................................................................................... Form 4BAnnual Facility Review Checklist ......................................................................................... Form 5

Contents
xx
Fire Drill Evaluation Form .................................................................................................... Form 5AEmployee Fire Drill Participation Signup Sheet ................................................................. Form 5BRisk Assessment for Workplace Violence ............................................................................ Form 6Housekeeping Schedule ...................................................................................................... Form 7Emergency Telephone List .................................................................................................. Form 7AHealthcare Facility Slip, Trip, and Fall Hazard Checklist ..................................................... Form 7B
Bloodborne Pathogens RecordsBloodborne Pathogens Exposure Determination List #1 ..................................................... Form 8Bloodborne Pathogens Exposure Determination List #2 ..................................................... Form 9Bloodborne Pathogens PPE Compliance Checklist ............................................................ Form 9AFailure to Use PPE .............................................................................................................. Form 9A1Bloodborne Pathogens Compliance Checklist: ECP, Training, and Records ...................... Form 9BSafety Needle/Syringe Evaluation ....................................................................................... Form 10Phlebotomy Device Evaluation ............................................................................................ Form 11Generic Safety Device Evaluation ....................................................................................... Form 12Sharps Disposal Container Locations .................................................................................. Form 12ASharps Evaluation Results ................................................................................................... Form 13Exposure Prevention Checklist ............................................................................................ Form 13A
Bloodborne Pathogens Employee Medical RecordsIncident Report/Sharps Injury .............................................................................................. Form 14Sharps Injury Log ................................................................................................................. Form 14AHBV Vaccination Declination Form ...................................................................................... Form 15HBV Employee Vaccination Form ........................................................................................ Form 16Postexposure Checklist ...................................................................................................... Form 17Postexposure Medical Evaluation Declination Form .......................................................... Form 18Source Patient Testing Consent Form ................................................................................. Form 18A
Hazard Communication Records Hazardous Substances List ................................................................................................. Form 19
TB/Infection Control Records TB Risk Assessment Results Form ..................................................................................... Form 20TST Record ......................................................................................................................... Form 21TST Declination Form .......................................................................................................... Form 22TB Exposure Log ................................................................................................................. Form 23Influenza Vaccine Log .......................................................................................................... Form 24Influenza Vaccine Declination Form (Seasonal and H1N1) ................................................ Form 25AChecklist for Infection Prevention for Outpatient Settings ................................................... Form 25B List of Infection Prevention Contact Persons and Roles/Responsibilities ................................ Form 25C
Training RecordsNew Employee OSHA Orientation Checklist ....................................................................... Form 26Annual Employee Training Record ...................................................................................... Form 27OSHA Annual Retraining (Sample Essay Test) ................................................................... Form 28 OSHA Annual Retraining (Sample Multiple Choice Test) .................................................... Form 29OSHA Annual Retraining (Sample True/False Test) ............................................................ Form 30Respiratory Protection Training Record ............................................................................... Form 31Qualitative Respirator Fit Test Report .................................................................................. Form 31AChecklist for Decreasing Surgical Fire Risks ....................................................................... Form 32

TAB 12: OSHA Regulations & Key ContactsOSHA Regulations
Bloodborne Pathogens Standard ........................................................................................ 121Amended Bloodborne Pathogens Standard (Sharps Safety) .............................................. 1213Hazard Communication Standard ........................................................................................ 1214Exit Routes, Emergency Action Plans, and Fire Prevention Plans ...................................... 1229Ionizing Radiation ................................................................................................................ 1233Table of Other OSHA Standards for Outpatient Medical Facilities ...................................... 1241
Additional OSHA ResourcesHealthcare Worker Vaccination Recommendations (Revised 2011) ................................... 1242Suggested Work Restrictions for Employees ...................................................................... 1244
Key ContactsState OSHA Consultative Services Directory ....................................................................... 1248Directory of States with Approved OSHA Plans ................................................................... 1251
Acronyms used in the OSHA Program Manual ......................................... 12-53
xxi
Contents

TAB 6: TB/INFECTION PREVENTION AND CONTROL PLAN
Contents
A Quick Look At TB ......................................................................................... 6-1TB Transmission .................................................................................................................... 6-1Risk Factors for Developing Active TB ................................................................................... 6-2
TB Exposure Control Plan Policy ................................................................... 6-3Overview: How to Protect Staff from Contracting TB at Work ................................................ 6-4TB Risk Assessment .............................................................................................................. 6-4
TB Risk Assessment Results Form (Form 20) ............................................................... 6-5Early Identification of Patients with Active TB ........................................................................ 6-6
Symptoms of TB ............................................................................................................. 6-6Handout: Cover Your Cough/Clean Your Hands .................................................................... 6-8Managing Patients with Suspected or Confirmed TB ............................................................. 6-9
TB Isolation Procedures for Cough Inducing and Aerosol-Generating Procedures ....... 6-9Respiratory Protection for Healthcare Workers: N-95 Respirators or Medical Powered Air Purifying Respirators (PAPRs) ................... 6-10
Seal Checking N-95 Respirators ............................................................................ 6-10Medical PAPRs ...................................................................................................... 6-10
Employee TB Skin Testing (TST) ........................................................................................... 6-11Baseline Employee TST: The Two-Step Skin Test ......................................................... 6-12
Two-Step TST Interpretation ................................................................................... 6-12Interpreting the TST ........................................................................................................ 6-13
False Positive/False Negative TB Tests ................................................................. 6-13Workers Who Have Had BCG Vaccination ............................................................. 6-14
Periodic Retesting of Employees ................................................................................... 6-14Recording TST Results .................................................................................................. 6-14TST Record (Form 21) ................................................................................................... 6-15TST Declination (Form 22) ............................................................................................. 6-16
Evaluation and Management of Healthcare Employees Exposed to TB ............................... 6-17Employees with Symptoms of TB ................................................................................... 6-17Employees Who Have Been Exposed to a Known TB Patient ....................................... 6-17Positive Employee Skin Tests and Skin Test Conversions ............................................. 6-17TB Exposure Log (Form 23) ........................................................................................... 6-19Decontaminating Patient Care Area and Equipment ...................................................... 6-20
Employee Training ................................................................................................................. 6-20
Page

Pandemic Influenza Plan and Other Infectious Diseases ............................ 6-21Pre-pandemic Planning ......................................................................................................... 6-21Once a Pandemic Is Announced ............................................................................................ 6-24OSHA Enforcement for a Pandemic ...................................................................................... 6-26
Identifying Very High and High Exposure Risks ............................................................. 6-26Dealing with N95 Respirator Shortages ......................................................................... 6-27Prioritize Your Facility’s Use of N95 Respirators ............................................................ 6-27Documentation ............................................................................................................... 6-28
Pandemic Resources ............................................................................................................. 6-29
Multidrug-Resistant Organisms (MDRO) ....................................................... 6-29CDC Classification of MDRO Threats ................................................................................... 6-29MDRO Prevention and Control .............................................................................................. 6-31Colonization vs. Infection ....................................................................................................... 6-31MDRO Transmission .............................................................................................................. 6-32Patient Precautions ................................................................................................................ 6-32
Hand Hygiene ................................................................................................................ 6-33Contact Precautions ....................................................................................................... 6-33
Environmental Cleaning ......................................................................................................... 6-34Infected Employees ............................................................................................................... 6-35MDRO Resources .................................................................................................................. 6-36
Pertussis and Worker Vaccination ................................................................ 6-36Supplement: How Antibiotic Resistance Happens ...................................... 6-38Supplement: Guide to Infection Prevention in Outpatient Settings: Minimum Expectations for Safe Care ............................................................ S1-S10
Contents

6-29
OSHA Program Manual for Medical Facilities
Pandemic Resources
1. Enforcement Procedures for High to Very High Occupational Exposure Risk to 2009 H1N1 Influenza, OSHA (www.osha.gov/OshDoc/Directive_pdf/CPL_02_02-075.pdf)
2. Centers for Disease Prevention and Control, CDC (www.flu.gov)3. OSHA Pandemic Influenza Web page (www.osha.gov/dsg/topics/pandemicflu)4. CDC: Middle East Respiratory Syndrome (MERS) (www.cdc.gov/CORONAVIRUS/
MERS)
Multidrug-Resistant Organisms (MDRO)Multidrug-resistant organisms (MDRO) are bacteria that have become resistant to certain antibiotics, which means these antibiotics can no longer be used to control or kill the bacteria. Widespread penicillin resistance was first identified in the early 1950s in Staphylococcus aureus, a common bacteria that causes sores, boils, and cellulitis. By the 1980s, more than half of the S. aureus infections in hospitals were resistant to methicillin. Methicillin-resistant S. aureus (MRSA) has long been associated with healthcare-acquired infections (HAI) but is now commonly acquired outside the healthcare setting. The widespread use of antibiotics over time has led to the development of many other MDROs.
In April 2013, the Centers for Disease Control and Prevention (CDC) released a report on Antibiotic Resistance Threats in the United States. The stated purpose of the report was to highlight the seriousness of the threat that antibiotic-resistant organisms pose to high-risk groups, including those with chronic illnesses. CDC estimates that more than 2 million people are sickened by MDRO infections every year resulting in at least 23,000 deaths. CDC states that the estimates are low because it is difficult to determine when someone’s death is primarily caused by infection with antibiotic-resistant bacteria or when other co-existing illnesses may have contributed to or caused death. Even when alternative treatments exist, the data has shown that patients with resistant infections are much more likely to die, and survivors have significantly longer hospital stays, delayed recovery and long-term effects.(see www.cdc.gov/drugresistance/threat-report-2013/pdf.)
CDC Categories of MDRO Threats
The CDC has prioritized the MDRO threats into one of three categories: urgent, serious, and concerning. Criteria used to categorize the threats include clinical and economic impact, incidence (rate of infection), 10-year projection on incidence, transmissibility, availability of antibiotics, and barriers to prevention. Bacteria in the CDCs urgent category include:
6-30
OSHA Program Manual for Medical Facilities
Clostridium difficile Although C. difficile is not currently resistant to antibiotics used to treat it, it was included in the CDC assessment because of its unique connection with antibiotic use and the high illness and death rate. CDC estimates that there are at least 250,000 illnesses and 14,000 deaths from C. difficile annually.
Carbapenem-resistant Enterobacteriaceae (CRE)CDC indicates that gram-negative bacteria are particularly worrisome because they are becoming resistant to nearly all drugs that would be considered for treatment. The most serious gram-negative infections are healthcare-associated, and the most common pathogens are Enterobacteriaceae, such as Klebsiella, Pseudomonas aeruginosa, and Acinetobacter. Treating infections with these organisms is identified as an increasing challenge for healthcare because the few remaining effective antibiotics are more toxic, less effective, and often more expensive.
There are 12 bacteria considered to be serious threats. This list includes:
Methicillin-resistant Staphylococcus aureus (MRSA)Methicillin-resistant Staphylococcus aureus (MRSA) causes a range of illnesses, from skin and wound infections to pneumonia and bloodstream infections that can cause sepsis and death. “Staph” bacteria, including MRSA infections can be very serious and are one of the most common causes of healthcare associated infections. CDC estimates there were more than 80,000 invasive (serious) MRSA infections and 11,000 related deaths in 2011. It is unknown how many lesser infections occur each year.
Staph is commonly found on the skin and nasal mucous membranes of healthy people. It may also be found in chronic sores such as those caused by psoriasis or eczema.
Drug-resistant Streptococcus pneumoniaStreptococcus pneumonia is the leading cause of bacterial pneumonia and meningitis in the U.S. It can also cause bloodstream, ear, and sinus infections. It is estimated that pneumococcal disease causes 4 million disease episodes and 22,000 deaths annually. Pneumococcal ear infections (otitis media) are the most common type of pneumococcal disease among children, causing 1.5 million infections that often result in antibiotic use. It is estimated that the hospitalization costs associated with pneumococcal disease are greater than $96 million each year. Pneumococcal vaccines introduced in 2010 protect against infections with the most resistant strains. This has led to a decrease in the number of infections with resistant strains. If this trend continues, this threat might be reclassified to “concerning.” Drug-resistant tuberculosisInfections with multidrug-resistant and extensively drug-resistant tuberculosis (MDR and XDR TB) are increasing threats outside of the U.S. In the U.S., infections are uncommon because of prevention and protection programs. Healthcare workers are educated about risks and TB skin testing is a routine part of healthcare hiring practices.
6-31
OSHA Program Manual for Medical Facilities
If the infection rates of MDR and XDR TB increase within the U.S., this antibiotic-resistant threat will change to urgent as TB is readily transmitted via respiratory secretions and treatment options are limited.
Bacteria in the concerning threats include:
Vancomycin-resistant Staphylococcus aureus (VRSA)
Erythromycin-resistant Group A Streptococcus
Clindamycin-resistant Group B Streptococcus
Although there are multiple effective treatment options at this time, these organisms cause severe illness and require monitoring. In some cases, rapid outbreak response might be required.
MDRO Prevention and ControlIn general, healthy people are at low risk of becoming infected with MDROs. The risk of infection is increased if you have:
An existing severe illness.
A hospital or nursing home admission in the previous year, with at least one underlying chronic illness such as diabetes, chronic kidney disease, skin lesions, or HIV.
Previous prolonged use of antibiotics.
Previous MDRO infection or colonization.
A suppressed immune system or are elderly.
Frequent procedures, such as hemodialysis.
Colonization vs. Infection
Colonization refers to the presence of microorganisms with growth and multiplication, but without tissue invasion or damage. In the case of MRSA, the body site most commonly colonized is the anterior nares (nose). Other body sites often colonized with MRSA include open wounds, the respiratory tract, perineum, upper extremities, umbilicus (in infants), urinary tract, and axilla (armpits). MRSA colonization can serve as a reservoir for the spread of these microorganisms to others and can lead to infection in the host. Colonized patients are also known as asymptomatic carriers.
Infection is the entry and multiplication of microorganisms in the tissues of the host, leading to local or systemic signs and symptoms of infection.
6-32
OSHA Program Manual for Medical Facilities
MDRO Transmission
MDRO infections can occur anywhere on/in the body:
Skin
Bloodstream
Urinary tract
Wounds
Surgical site
Several factors make for easy MDRO transmission. NIOSH has identified these factors as the five Cs:
Crowding.
Frequent skin-to-skin Contact.
Compromised skin (i.e., cuts or abrasions).
Contaminated items or surfaces.
Lack of Cleanliness.
Patients who already have an MDRO infection or who carry the bacteria on their bodies but do not have symptoms (i.e., are colonized) are the most common sources of transmission.
Effective efforts to eliminate MDRO transmission are guided by four main tenets:
Using proper precautions when treating MDRO patients in the facility.
Decreasing the probability of harboring MDROs in the environment.
Taking appropriate actions if employees are infected with MDROs.
Eliminating the overuse of antibiotics.
Patient Precautions
Flag records of MDRO-positive patients. Treat patients formerly infected with MDRO as potentially contagious, unless three or more surveillance cultures indicate otherwise.
When possible, schedule a patient who is known to have MDRO as the last appointment of the day. If the patient cannot be scheduled at the end of the day, add 15 minutes onto the appointment time to allow for adequate decontamination following the patient visit.
Provide staff members with education and training in patient precautions that aid in the prevention of MDRO transmission. Perform staff training during initial workplace
6-33
OSHA Program Manual for Medical Facilities
orientation and also during periodic educational updates for dental personnel. Refer to specific organizational experience with resistant bacteria and prevention strategies whenever applicable.
Hand Hygiene
The main mode of transmission for most MDROs is via hands (especially healthcare workers’ hands), which may become contaminated by contact with:
Colonized or infected patients.
Colonized or infected body sites of the personnel themselves, or devices, items, or environmental surfaces contaminated with body fluids containing MDROs.
Handwashing is the first and best step to stopping the spread of MDROs. Staff members will:
Wash hands using soap and water or alcohol-based hand sanitizers. It is important to note that the spores of C. difficile are not killed by alcohol-based hand sanitizers. Soap and water is always required for potential contact with C. difficile.
Wash and dry hands thoroughly before and after contact with every patient.
Wash and dry hands thoroughly after handling any potentially contaminated equipment.
Wash and dry hands thoroughly after removing gloves.
Wash and dry hands before touching items such as keyboards, instrument controls, exam tables, and positioners for x-rays or MRIs to avoid cross-contamination.
The leadership and healthcare providers should be accountable for implementing a culture that supports and promotes appropriate hand hygiene practices.
Contact Precautions
MDRO-infected patients can be cared for safely. Contact precautions are necessary to prevent cross-contamination to other patients and dental workers:
Wear gloves when touching blood, body fluids, secretions, excretions, and contaminated items. During the course of providing care for a patient, change gloves after having contact with infective material that may contain high concentrations of MDROs (e.g., non-intact skin, fecal material, wound drainage, and mucous membranes). Because environmental surfaces may be contaminated, don gloves before or upon entry to a patient area. Remove gloves before leaving the patient area and wash hands immediately. Dry hands completely. After glove removal and handwashing, ensure that hands do not touch potentially contaminated environmental surfaces or items in the patient’s environment to avoid transfer of microorganisms to other patients and environments.
6-34
OSHA Program Manual for Medical Facilities
Wear a surgical mask and eye protection or a face shield to protect mucous membranes of the eyes, nose, and mouth during procedures and patient care activities that are likely to generate splashes or sprays of blood, body fluids, secretions, and excretions.
Wear a gown to protect skin and prevent soiling of clothes during procedures and patient care activities that are likely to generate splashes or sprays of blood, body fluids, secretions, and excretions or cause soiling of clothing. Examples are if the patient is incontinent or has diarrhea, an ileostomy, a colostomy, or wound drainage not contained by a dressing. Don the gown upon entry to the patient area and remove it before leaving.
Disinfect reusable patient care equipment according to the manufacturer’s directions or discard single-use items that are soiled with blood, body fluids, secretions, or excretions. An appropriate disinfectant is a 1:10 solution of ordinary household bleach, made up fresh daily, or an equivalent EPA-approved commercial product. Consider using disposable patient care items (e.g., blood pressure cuffs and tourniquets) for a known MDRO patient.
Handle, transport, and process used linen soiled with blood, body fluids, secretions, or excretions in a biohazardous labeled container.
Use care when giving injections or placing IVs. Ensure that the site is covered immediately and blood from the puncture wound does not contact the pads or table. Clean and decontaminate any soiled areas immediately.
Have patients change into clean or disposable garments prior to their examination.
Note: Suspect and confirmed cases of tuberculosis require airborne precautions regardless of whether the TB is multidrug resistant.
Environmental Cleaning
By decreasing the probability of harboring MDRO, in the environment, the risk of transmitting MDROs is reduced.
Clean rooms and equipment with an EPA-approved hospital-level disinfectant; follow the manufacturer’s instructions. Focus on obviously soiled surfaces and frequently touched surfaces. There is no need to routinely clean and disinfect walls, window drapes, and other vertical surfaces unless visibly soiled. Discard solutions used for cleaning and disinfection after use.
Environmental cleaning procedures should include the following:
Visually inspect all exam tables, exam chairs, pads, etc., between patients. If body fluids are noted, disinfect immediately.
Clean all surfaces of exam tables, exam chairs, pads, etc., with an appropriate disinfectant at least daily.
6-35
OSHA Program Manual for Medical Facilities
Once per month, inspect exam tables, exam chairs, and pads to check for fraying or tearing. If present, replace or repair since torn surfaces are not easily cleaned and disinfected.
Enclose any pillows used in waterproof coverings. Decontaminate covers daily (or immediately, if body fluids are noted).
If a patient has an open wound or history of MDROs, completely clean and disinfect the exam table, exam chair, and any pads, etc., before the next patient.
Periodically clean the upholstered furniture and furnishings in patient waiting areas.
Keep the environment as clean and dry as possible. Clean and dry all equipment after use.
Infected Employees
Workers in all healthcare settings, clinical and nonclinical, may be colonized or infected similarly to individuals from communities where MDROs are present. For example, community-acquired MRSA (CA-MRSA) is becoming increasingly prevalent. It should not be assumed that a healthcare worker with MRSA has been infected from the workplace.
Unless advised by a healthcare provider, workers should not be routinely excluded from going to work, according to the CDC. Employees will keep areas of the skin affected by MRSA covered. A worker with wound drainage (i.e., pus) will cover the area with clean, dry bandages and follow his or her healthcare provider’s instructions on proper care of the wound. Since pus from infected wounds can contain MRSA, keeping the infection covered will help prevent the spread of MRSA to others.
Work exclusions should be reserved for:
Employees with wound drainage that cannot be reliably contained by a dressing or other barrier method or workers who cannot maintain good hygiene practices.
Employees with active infections who participate in activities in which skin-to-skin contact with affected skin areas is likely to occur.
Employees that work in sterile areas or participate in invasive procedures.
Employees that are febrile or show other symptoms of MDRO infection.
Culturing to establish colonization is generally not indicated. No work restrictions are necessary for colonized personnel unless they have been epidemiologically implicated in Staphylococcus aureus transmission within the facility.
If there is evidence linking a healthcare staff member to ongoing transmission of any MDRO, obtain the proper cultures from the individual for evaluation. In the case of MRSA, use one sterile swab moistened with sterile saline. Gently swirl the swab in each anterior nare (i.e., the opening of each nostril) for two to three seconds. The same swab can be used for both nares.
6-36
OSHA Program Manual for Medical Facilities
Place the swab in a transport system and label prior to shipping to a qualified laboratory for identification and susceptibility testing. The laboratory should be instructed to screen the specimen for MRSA only.
Treatment of a MRSA carrier state among dental workers appears to have no effect on the spread of MRSA. Therefore, routine decolonization of staff members is not recommended.
MDRO Resources
1. Antibiotic Resistance Threats in the United States, 2013, CDC2. CDC Campaign to Prevent Antimicrobial Resistance in HealthCare Settings3. OSHA Hospital eTool—MRSA. www.osha.gov/SLTC/etools/hospital/hazards/mro/
mrsa/mrsa.html.4. CDC Guideline for Isolation Precautions: Preventing Transmission of Infectious
Agents in Healthcare Settings 2007. www.cdc.gov/ncidod/dhqp/gl_isolation.html.5. CDC: Management of Multidrug-Resistant Organisms in Healthcare Settings,
2006. www.cdc.gov/ncidod/dhqp/pdf/ar/mdroguideline2006.pdf.
6. NIOSH: “MRSA and the Workplace.” www.cdc.gov/niosh/topics/mrsa.
Pertussis and Worker VaccinationReports of whooping cough (pertussis) were at an all-time high in the U.S. during 2010 and 2011, according to the CDC. The ongoing pertussis reports prompted the Advisory Committee on Immunization Practices (ACIP) to update the vaccination guidelines for healthcare workers in February 2011.
ACIP recommends a single dose of Tdap for healthcare personnel who have not previously received Tdap as an adult regardless of age and have direct patient contact Tdap vaccination can protect healthcare personnel against pertussis and help prevent them from spreading it to their patients. Priority should be given to vaccinating those who have direct contact with babies under 12 months of age.
This change is included in the Healthcare Worker Vaccination Recommendations Revised 2011) table in Tab 12 of the OSHA Program Manual. Tdap can be administered regardless of interval since the previous Td dose.
Note from APIC Recommendations: Healthcare personnel include but are not limited to physicians and medical students, other primary care providers, nurses and nursing students, aides, respiratory therapies, radiology and laboratory technicians, dental professionals and students, social workers, chaplains, volunteers, dietary, clerical workers, and support staff.

6-37
OSHA Program Manual for Medical Facilities
ACIP also made amended post-exposure prophylaxis recommendations for healthcare personnel who have already received Tdap vaccine. Staff members who “are exposed and are expected to have contact with persons at high-risk of severe pertussis disease (e.g., hospitalized neonates and pregnant women) need to receive post-exposure prophylaxis,” according to ACIP. If a vaccinated staff member has been exposed but is not in contact with at-risk patients, the facility has the option of providing postexposure prophylaxis or monitoring the worker for 21 days after exposure and treating at the onset of signs and symptoms of pertussis.
The ACIP changes are recommendations only. There is no specific requirement under federal OSHA to provide the Tdap vaccination to potentially exposed workers, but OSHA could cite the employer under the General Duty Clause for failing to protect workers from hazards that were known to be present in the workplace. It is important to note that pregnant women should receive a Tdap during each pregnancy to provide material pertussis antibodies for the newborn. Even though the DTaP immunization series begins at two months of age, newborns are at high risk for pertussis until they are over 12 months and they have had three of the five DTaP immunizations. Family members of the newborn are also encouraged to be up to date with their Tdap Immunizations.
Employers should also check with their state health department for regulations specific to pertussis vaccination: www2a.cdc.gov/nip/StateVaccApp.
6-38
OSHA Program Manual for Medical Facilities
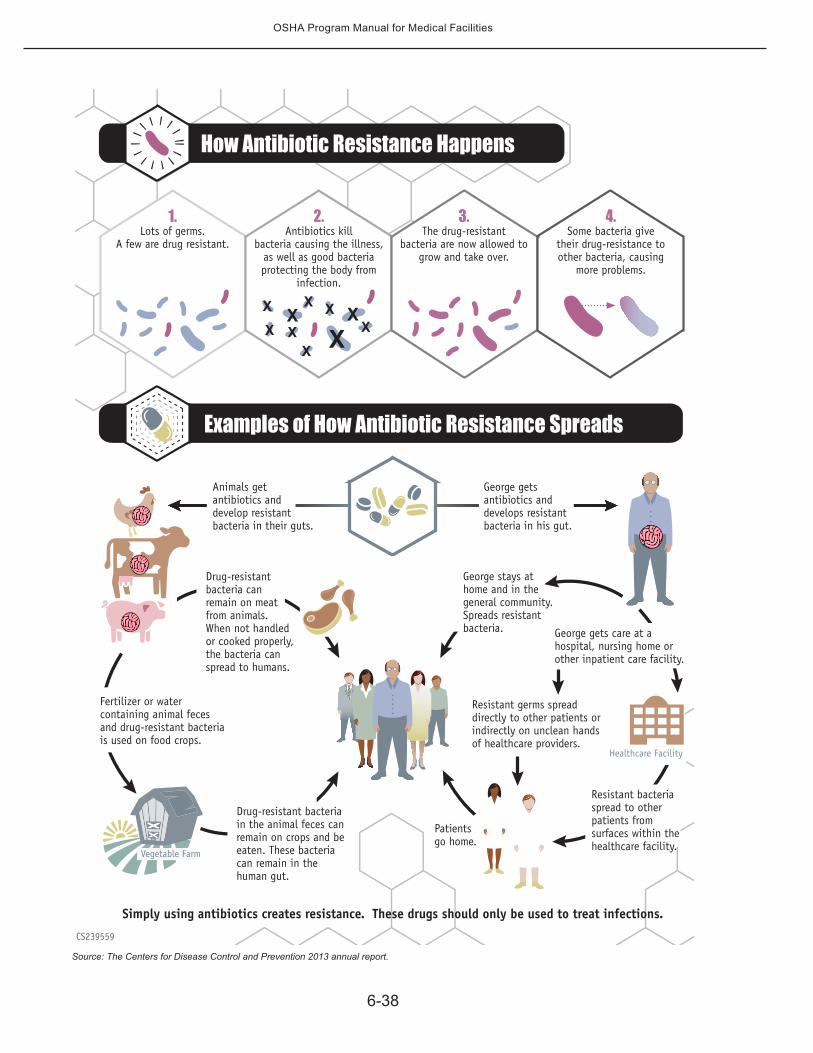
Simply using antibiotics creates resistance. These drugs should only be used to treat infections.
Fertilizer or water containing animal feces and drug-resistant bacteria is used on food crops.
Animals get antibiotics and develop resistant bacteria in their guts.
George gets antibiotics and develops resistant bacteria in his gut.
Drug-resistant bacteria in the animal feces can remain on crops and be eaten. These bacteria can remain in the human gut.
Drug-resistant bacteria can remain on meat from animals. When not handled or cooked properly, the bacteria can spread to humans.
Healthcare Facility
Resistant bacteria spread to other patients from surfaces within the healthcare facility.
Resistant germs spread directly to other patients or indirectly on unclean hands of healthcare providers.
George stays at home and in the general community. Spreads resistant bacteria. George gets care at a
hospital, nursing home or other inpatient care facility.
Vegetable Farm
Patientsgo home.
How Antibiotic Resistance Happens
Examples of How Antibiotic Resistance Spreads
4.Some bacteria give
their drug-resistance to other bacteria, causing
more problems.
3.The drug-resistant
bacteria are now allowed to grow and take over.
1. Lots of germs.
A few are drug resistant.
2. Antibiotics kill
bacteria causing the illness, as well as good bacteria protecting the body from
infection.
CS239559
Source: The Centers for Disease Control and Prevention 2013 annual report.





























