Embed Size (px)
Citation preview

Distribution: Chart Copy
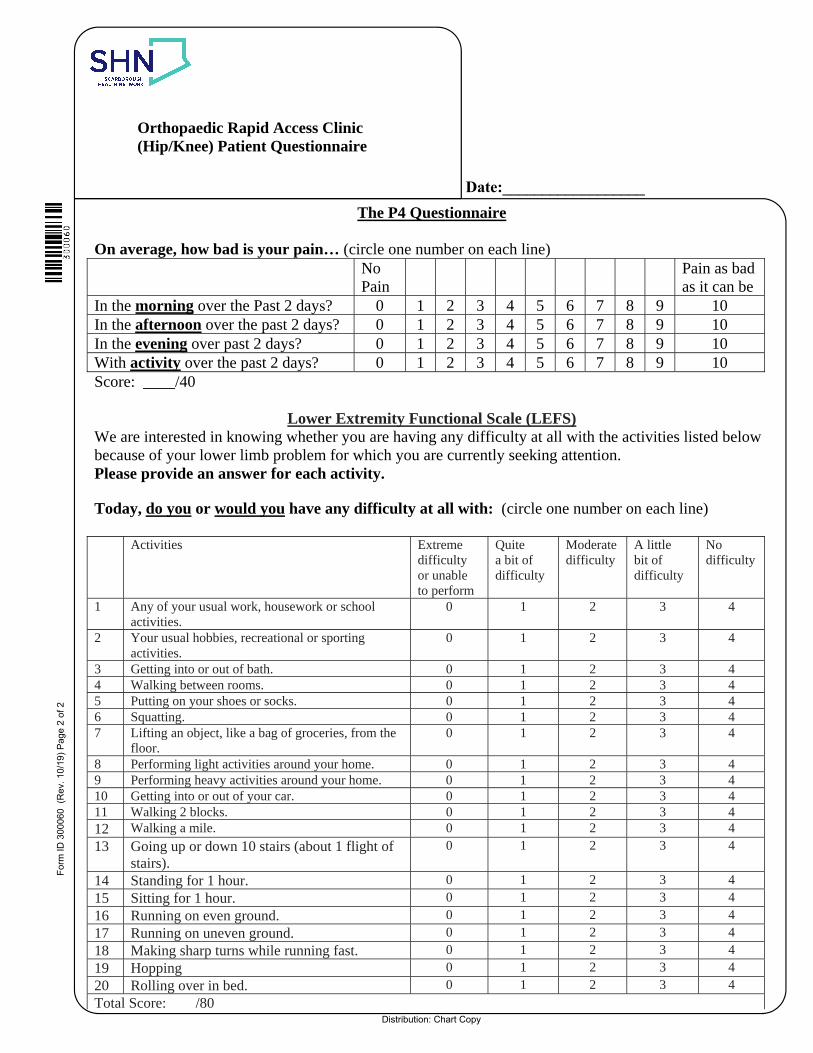
Orthopaedic Rapid Access Clinic (Hip/Knee) Patient Questionnaire
Form
ID 3
0006
0 (
Rev
. 10/19
) P
age
1 of
2
Medical History: Do you have any of the following?
Diabetes Yes No Personal history of Cancer Yes No
Kidney Disease Yes No Seizure disorder Yes No
Heart Disease/Problems/Pacemaker Yes No Take blood thinners Yes No
Breathing problems Yes No Sleep disorder Yes No
Dementia or forgetfulness Yes No Family history of arthritis Yes No
High Blood Pressure Yes No Low Blood Pressure Yes No
Other Medical Conditions:
Height: _________________ Weight: ________________
List any surgeries you have had:
List your medications:
List any allergies:
List any specialists you see:
Home Setup: house type _____________________ □ stairs □stair lift □home support
Do you use any homecare services? □ PS W □ Nursing □ OT □ PT
Assistive Devices (e.g. walker, cane, orthotics, bath chair, brace)
Do you have to climb stairs? Yes No
Do you have support at home? Yes No
Do you use home care? Yes No Do you have someone to translate?
Do you have refugee status? Yes NoAre you a dialysis patient? Yes No Do you take care of anyone? Yes No
□ Social Work Follow‐up Recommended □ Physiotherapy Recommended
Instructions to Surgeon’s Office:
1. IF Social Work Follow‐up OR Physiotherapy is recommended, complete the Prehab Referral Form.
2. Fax completed referral plus THIS ORAC Assessment (both sides) to Prehab at 416‐284‐3171.
Do you have another way to get to
appointments besides driving
yourself?
Do you understand written or
spoken English?
Do you have any financial concerns
(renting equipment etc?)
To be completed by Physiotherapist:
Consider responses to above questions and functional mobility reported on the LEFS. IF patient is
booked for surgery, will s/he benefit from Social Work or Prehabilitation?
Yes No
Yes NoYes No
Yes No
Date:__________________
Distribution: Chart Copy
Orthopaedic Rapid Access Clinic (Hip/Knee) Patient Questionnaire
The P4 Questionnaire
On average, how bad is your pain… (circle one number on each line) NoPain
Pain as bad as it can be
In the morning over the Past 2 days? 0 1 2 3 4 5 6 7 8 9 10 In the afternoon over the past 2 days? 0 1 2 3 4 5 6 7 8 9 10 In the evening over past 2 days? 0 1 2 3 4 5 6 7 8 9 10 With activity over the past 2 days? 0 1 2 3 4 5 6 7 8 9 10 Score: ____/40
Lower Extremity Functional Scale (LEFS) We are interested in knowing whether you are having any difficulty at all with the activities listed below because of your lower limb problem for which you are currently seeking attention. Please provide an answer for each activity.
Today, do you or would you have any difficulty at all with: (circle one number on each line)
Activities Extreme difficulty or unable to perform
Quite a bit of difficulty
Moderate difficulty
A little bit of difficulty
No difficulty
1 Any of your usual work, housework or school activities.
0 1 2 3 4
2 Your usual hobbies, recreational or sporting activities.
0 1 2 3 4
3 Getting into or out of bath. 0 1 2 3 4 4 Walking between rooms. 0 1 2 3 4 5 Putting on your shoes or socks. 0 1 2 3 4 6 Squatting. 0 1 2 3 4 7 Lifting an object, like a bag of groceries, from the
floor. 0 1 2 3 4
8 Performing light activities around your home. 0 1 2 3 4 9 Performing heavy activities around your home. 0 1 2 3 4 10 Getting into or out of your car. 0 1 2 3 4 11 Walking 2 blocks. 0 1 2 3 4 12 Walking a mile. 0 1 2 3 4
13 Going up or down 10 stairs (about 1 flight of stairs).
0 1 2 3 4
14 Standing for 1 hour. 0 1 2 3 4
15 Sitting for 1 hour. 0 1 2 3 4
16 Running on even ground. 0 1 2 3 4
17 Running on uneven ground. 0 1 2 3 4
18 Making sharp turns while running fast. 0 1 2 3 4
19 Hopping 0 1 2 3 4
20 Rolling over in bed. 0 1 2 3 4
Total Score: /80
Form
ID 3
0006
0 (
Rev
. 10/19
) P
age
2 of
2
Date:__________________





























