Embed Size (px)
Citation preview

Clin Plastic Surg 31 (2004) 271–290
Orthodontic treatment for patients with clefts
Carla A. Evans, DDS, DMSc
Department of Orthodontics, The University of Illinois at Chicago, 801 South Paulina Street, MC 841,
Chicago, IL 60612-7211, USA
It has become increasingly evident that treatment and prosthetic replacement of missing teeth, but ma-
of oral clefts has many limitations and leaves more
than a scar on the lip. Adults who have treated clefts
often have characteristics that are visible at a distance
and give clues about the nature of the original con-
genital anomaly, such as shape of face, abnormal
animation of face, nasal asymmetry, unsightly teeth,
unclear and nasal speech, and chewing difficulties.
Just getting on the bus to go to work may be stressful
for individuals with treated clefts because of the
public’s responses to people with facial differences.
Marcusson [1] investigated quality of life, satisfaction
with treatment, prevalence of temporomandibular
disorders, psychosocial distress, and occlusal stability
in 68 Swedish adult patients with treated cleft lip/
palate for whom comprehensive treatment was con-
ducted under the national health system and for whom
follow-up records were available. Despite being so-
cially well adjusted and having relatively normal daily
lives, the patients with treated cleft lip/palate were
generally dissatisfied with their nose, lips, mouth,
profile, and overall facial appearance and reported
that their well-being and social lives were affected by
their condition. In addition, the occlusal result was
significantly unstable, irrespective of the type of
retention, but was not linked with temporomandibular
joint disturbances.
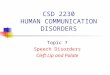
Fig. 1 shows an example of residual problems in
an adult patient with bilateral cleft lip and palate who
was treated in the United States. The patient had lip
and palate closure, columella lengthening, an Abbe
flap, orthognathic surgery to set back the mandible,
0094-1298/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S0094-1298(03)00125-1
E-mail address: [email protected]
jor functional, anatomic, and aesthetic shortcomings
remained. The patient’s lips were tight and didn’t
move well, her face was very flat with both maxillary
and mandibular retrusion, the premaxilla had not
been grafted and the mobility caused the dental
bridge to loosen, the dental occlusion was inefficient
for chewing, the oronasal fistulae allowed food and
secretions to move between the mouth and the nasal
passages, the palate was highly scarred, and the muco-
gingival condition was poor because the multiple
tight labial frenums caused gingival recession. Each
clinician individually had rendered state-of-the-art
treatment but had not worked with the others as a
team. This example adds to the evidence that treat-
ment of oral clefts is much more complex than just
closing the cleft space because so much is at stake in
terms of growth and function.
Because clinicians have reviewed treatment out-
comes in recent times, their recommendations regard-
ing therapy have become more focused on specific
problems [2–5], such as ways to promote normal
growth, advance the maxilla rather than set back the
mandible, retain as many natural teeth as possible,
and use implants for tooth replacement and as an-
chorage for dentofacial orthopedics. It is useful to
study the natural history of individuals who have
untreated clefts and compare this with normal indi-
viduals to understand the effects of treatment. For
example, the growth potential of the untreated cleft
maxilla was studied in 30 untreated nonsyndromic
Indian adults who had complete unilateral cleft lip
and palate [6], with the observation that the size and
position of the cleft maxilla compared favorably in
comparison to a control group of 30 non-cleft Indian
individuals who had a normal occlusion. Several texts
[7–14] provide basic information about clefts and
s reserved.

Fig. 1. (A–D) Problems remaining after a poorly coordinated treatment program include a retruded maxilla and mandible; tight
lips; mucogingival problems, with gingival recession; open oronasal fistulae; a mobile premaxilla; inefficient chewing; and a
loose dental bridge.
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290272
their treatment and show that conventional treatment
has many side effects. Thus, growth and function
must be considered in addition to short-term aes-
thetics in choosing a course of treatment that will lead
to long-term success.
Because of their education and experience, ortho-
dontists have much to contribute to the treatment
team in terms of knowledge of growth and develop-
ment and coordination of treatment. In addition to
providing orthodontic appliances to accomplish spe-
cific treatment objectives, orthodontists should par-
ticipate in long-term observations and analysis of
treatment outcomes. This article reviews various roles
of the orthodontist, namely recordkeeping, planning
and delivering treatment, and monitoring growth
and development.
Recordkeeping
Two important monographs available from the
American Cleft Palate-Craniofacial Association
[15,16] summarize current guidelines for providing
coordinated and comprehensive care to patients with
oral clefts. Topics include composition of the treat-
ment team, the acquisition of diagnostic records at
appropriate intervals, and the need for longitudinal
assessment. Typical orthodontic records include the
following: facial moulages; two- and three-di-
mensional facial and intraoral imaging; dental study
models in occlusion; measurements of height and
weight; and various radiographs, such as periapical,
panoramic, cephalometric, hand-wrist, and temporo-
mandibular joint films. Establishing the protocol for

C.A. Evans / Clin Plastic Su
collecting diagnostic information about each type of
patient should be based on sound orthodontic con-
cepts and is a team decision.
Treatment
Neonates and infants
Orthopedic repositioning of the alveolar segments
or nasoalveolar molding preceed lip and palatal
surgery [17,18]. Surgeons who advocate presurgical
orthopedics emphasize that surgical closure is easier
after orthopedics because the dental arches and lips
are in better alignment than at birth, the cleft may
be smaller, and better symmetry is achieved. It is
not known how long the benefits are maintained af-
ter surgical correction or whether normal growth is
stimulated or better long-term outcomes are achieved.
The short-term benefit is important, however, given
the significance of the initial operations to the long-
term success of treatment.
Early bone grafting of the cleft alveolus [11,
19,20] is more controversial in that some methods
may be associated with midface growth inhibition.
Proponents argue, however, that the graft gives sta-
bility to the arches, prevents collapse of the alveolar
segments, guides tooth eruption, allows orthodontic
tooth movement, reduces the occurrence of oronasal
fistulae, and reduces the need for future surgical
procedures in that area. Critics note that the eventual
bridge of bone joining the alveolar segments may not
have sufficient volume to bear dental implants or
support the alar base; secondary bone grafting may
still be necessary.
Sometimes malpositioned or extra teeth are re-
moved at the time that the palate is closed and may be
erroneously assumed later to be congenitally absent.
The timing of palatal closure varies from one cleft
center to another.
Toddlers and preschool children
Oral health care for children with a cleft begins
with educating the childrens’ parents about dental
development, the importance of good oral hygiene
and a healthy diet, disturbances that may result from
the cleft, and how to avoid nursing-bottle caries.
Visits to the pediatric dentist begin at approximately
age 2 to ensure caries control; assess toothbrushing,
oral hygiene, and diet; evaluate oral habits; and
monitor tooth development and eruption. Sometimes
dental extractions are necessary.
Elementary school age
Secondary bone grafting has become a well-ac-
cepted procedure [21–28]. Orthodontists align the
dental arches and teeth in preparation for bone graft-
ing. If the procedure is performed between age 6 and
10, depending on maturation of teeth, unerupted per-
manent teeth may erupt into the graft and be pre-
served. Recent patient series [26–28] showed that
success was greatest when the graft was placed before
eruption of the permanent canines. Most of the per-
manent canines erupted spontaneously. Increased ex-
perience of the surgeon enhanced the rate of success
as measured by bone height, gingival health, and
space closure by orthodontic means [26].
Arch alignment before secondary bone grafting
can be obtained using various expanders. In young
children with unilateral clefts, a quadhelix (Figs. 2
and 3) achieves the desired change. In bilateral clefts,
bilateral symmetric expansion is usually needed and a
traditional expansion screw is effective (Fig. 4). The
unerupted teeth migrate quickly through the bone
graft if the graft is not placed too early or too late,
similar to Fanning’s [29] observations that the erup-
tion of premolars can be accelerated when their cor-
responding primary molars were extracted. In Fig. 2,
the permanent canine traveled through the graft
past the lateral incisor and emerged unexpectedly
next to the central incisor.
A trend has emerged to place alveolar bone grafts
at a younger age when suitable lateral incisors are
present [30–32]. Fig. 3 shows a highly successful
outcome. As seen in the occlusal radiograph, the
lateral incisor formed distal to the cleft. After moving
the lateral incisor through the graft into the dental
arch and building up the incisors with restorative
composite, a full, natural dentition was present in
this child who had a complete unilateral cleft lip and
palate. Grafting only restores the alveolar process,
however; no graft is placed in the palate and bone
does not form there. In a patient who lacked lateral
incisors (see Fig. 4), plastic teeth were added to an
orthodontic retainer. Afterwards, a bonded bridge was
used to maintain the result until growth was com-
pleted and either a fixed bridge or dental implants
could be placed. When preserving teeth is not an
objective or when lateral incisors are not present,
secondary bone grafting can be done later. Successful
grafting and subsequent tooth movement also have
been reported with other methods [33,34].
In children with a cleft who have mild midface
retrusion, orthopedic maxillary protraction may be
used [35–39], but palatal scarring and tightness of
the lips are likely to reduce the amount of skeletal
rg 31 (2004) 271–290 273

Fig. 2. Management of a collapsed lesser segment in a patient with a unilateral cleft lip and palate. (A–D) Initial malocclusion
and maxillary expansion, with a quadhelix orthodontic appliance. (E) Removal of an erupted supernumerary incisor in the distal
segment, followed by alveolar bone grafting. (F) The remarkable path of eruption of the canine to a position between the central
and lateral incisors.
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290274

Fig. 3. A classic example of a successful secondary bone graft with preservation of the lateral incisor. (A, B) Alignment of the
dental arches after removal of the orthodontic expansion appliance and alveolar bone grafting. (C) Radiograph showing the width
of the bone bridge and position of the lateral incisor. (D, E, F) Arrangement of the teeth after active orthodontic tooth movement,
before and after prosthetic restoration of normal incisor shapes and sizes.
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290 275
maxillary advancement achieved as compared with
treatment of children without clefts. Even in normal
children with malocclusion, maxillary protraction has
limited effectiveness. In addition, because the devices
are usually attached to teeth, a moderate amount of
dental advancement is observed. It has been demon-
strated that protraction using implants is possible [40]
and that this method avoids the unfavorable dental
changes. In the future, new protraction devices may
use short-duration dynamic forces rather than continu-
ous forces as they are currently delivered, because
current research on the mechanobiology of sutures is
exploring the response of cells to oscillating mechani-
cal signals [41].

Fig. 4. Management of a patient with a bilateral cleft. (A, B) Expansion with a tooth-borne (hyrax) expander and alveolar bone
grafting. (C, D) A removable orthodontic retainer with plastic teeth. (E, F) A bonded bridge that involves little preparation of the
teeth and doesn’t interfere with tooth eruption or growth.
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290276
Adolescents and adults
Surgical assistance may be valuable in the treat-
ment of the protruding premaxilla in adolescent and
adult patients who have bilateral clefts [42]. In a
child, the premaxilla may still be mobile (Fig. 5).
After expansion, an extrusion orthodontic archwire
may be used to guide the premaxilla into the proper
position for secondary bone grafting. In a more ma-
ture individual who has more rigid skeletal attach-
ments (Fig. 6), palatal expansion was facilitated by
zygomatic buttress osteotomies [43,44], followed by
a premaxillary osteotomy [45,46] at the time of
alveolar bone grafting. In individuals who have clefts,
the zygomatic buttresses become very stiff to resist
masticatory force; they also resist attempts at palatal

C.A. Evans / Clin Plastic Surg 31 (2004) 271–290 277
expansion with orthodontic appliances. Surgical re-
leasing osteotomies improve the stability of expan-
sion and facilitate rotational movements.
In adolescent or adult patients with clefts who
need orthognathic repositioning of the jaw, emphasis
is placed on advancing the maxilla rather than setting
back the mandible [47–50]. Before satisfactory sur-
gical methods were available to advance the maxilla
Fig. 5. Management of a protrusive and mobile premaxilla. (A)
incisors in infraclusion. (B, C) Pretreatment dental occlusion with
lip. (D, E) Treatment photos showing an expander that causes
helix to improve archform and vertical guidance of the premaxilla
bone grafting.
sufficiently, compromise treatment plans sometimes
involved setting back normal mandibles to resolve
negative overjet, jeopardizing facial appearance and,
potentially, breathing.
In mature patients who will have orthognathic
surgery, it may be necessary to undo previous ortho-
dontic treatment. For example, one patient who had
many years of orthodontic treatment to improve her
Pretreatment cephalometric radiograph showing retroclined
maxillary incisors in the bulging premaxilla just under the
anterior expansion. (F) Continued expansion with a quad-
with an extrusion arch. (G, H) Anterior views after alveolar

Fig. 5 (continued).
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290278
malocclusion was dissastisfied with her cleft appear-
ance (Fig. 7). First, additional orthodontic treatment
was performed to decompensate the teeth and retract
the maxillary anterior teeth into extraction spaces to
permit maxillary advancement. The nasal changes
Fig. 6. Management of a protrusive maxilla and transverse max
dental occlusion. (C, D) After surgically assisted (buttress osteotom
of the premaxilla, as shown in the diagram.
occurred as a consequence of the Le Fort I advance-
ment; no other nasal surgery was performed.
Surgical intervention to mobilize posterior seg-
ments may be warranted to decrease the size of a
fistula or advance a segment to minimize prosthetic
illary deficiency in a mature patient. (A, B) Pretreatment
ies) maxillary expansion followed by surgical repositioning

Fig. 7. Orthodontic decompensation before maxillary advancement. (A, B) Facial photos after completion of the first orthodon-
tic treatment, which was directed at modifying tooth position to fit the skeletal relationship. (C, D) Facial photos after maxillary
advancement. (E–G) A second orthodontic treatment was initiated (at a time matching A and B) to retract the maxillary ante-
rior teeth into extraction spaces and the result after maxillary advancement. (H ) The dental occlusion before cosmetic bonding.
(I ) Lateral radiograph matching (E). (J ) Lateral radiograph matching (F). (K) Superposition of tracings of (I ) and (J ) showing
amount of advancement.
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290 279

Fig. 7 (continued).
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290280
replacement of teeth. Fig. 8 shows how a posterior
maxillary osteotomy was used to advance the lesser
segment in a patient with a unilateral cleft lip and
palate. Such movements also may be accomplished
using osteodistraction techniques [51,52].
Maxillary distraction is particularly valuable in
patients with clefts in whom palatal scarring may
limit the amount of advancement possible at the time
of the osteotomy [53–55]. Figs. 9, 10 show two
patients who underwent maxillary distraction. The
first patient (see Fig. 9) was in the stage of early
mixed dentition and marked advancement was ob-
tained. Just as in frontofacial advancement for patients
with craniofacial synostosis, however, the maxilla is
unlikely to grow normally after repositioning and ad-
ditional interventions are likely to solve the aesthetic

Fig. 7 (continued).
Fig. 8. Surgical advancement of the lesser segment was p
fistula. (A, B) The initial malocclusion. (C, D) The expansio
(G, H) Postoperative views.
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290 281
and occlusal issues that will recur with future growth.
Fig. 10 shows an example of maxillary distraction in a
mature person. There is marked facial improvement,
but some dental compensation resulted from using the
maxillary teeth as anchors for the device and from
using class III elastics to finalize the occlusal relation-
ships. One solution to avoid the dental side effects
may be to use implants for anchorage in distraction
patients as has been done for protraction facemask
therapy [40].
erforme
n applia
Stability is an issue following both standard
orthognathic procedures and distraction osteogenesis.
After Le Fort I osteotomies in patients with unilateral
and bilateral cleft lip and palate, a relapse of approxi-
mately 9% horizontally and 17% vertically was noted
in both groups [56]. It has been suggested that wear-
ing a facemask postoperatively will enhance stability
and provide an alternative to class III orthodontic
elastics [57]. The resolution of third molar problems
also should be accomplished before the end of the
retention period.
Monitoring growth and development
Orthodontists monitor growth and development of
the face, dental arches, and teeth by comparing the
individual patient’s condition to normal standards and
expected patterns for comparable patients as reported
in the literature. A general theme throughout the lit-
erature on patients who have treated clefts [58–66] is
that it is difficult to make clear distinctions between
outcomes of specific procedures because individual
variability is high and experimental groups usually
are small. Two persistent questions therefore have not
been answered adequately: timing of surgical inter-
ventions and predicting growth. Cases can be found
to demonstrate advantages of early or late treatment,
but generalizable conclusions based on analysis of
sufficient data from scientifically selected treatment
groups are sparse. Clinicians want to be able to pre-
dict the outcome for treatment planning and for other
concerns [67–70], such as linking the initial arch-
form or early occlusal relationships with later severity
of malocclusion, being able to tell prospective parents
d to close the edentulous space and eliminate the oronasal
nce. (E, F) Views before surgical movement of the segment.

Fig. 8 (continued).
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290282
if they have increased chances for cleft offspring
because of their own distinctive craniofacial mor-
phology, and determining ultimate costs of treatment
in financial terms.
Tooth anomalies present in cleft lip/palate in-
volve all phases of tooth development and result in
abnormalities in number, shape, size, color, timing
of development, and position [71–78] (Fig. 11). Teeth
may be missing because of natural exfoliation, agene-
sis, or iatrogenic reasons. Some patterns of agene-
sis have been linked to mutations in PAX 9 and
MSX1 homeodomains.
The literature’s reported rates of missing teeth in
patients with clefts may include some iatrogenic
losses, such as those maxillary anterior teeth or their
anlagen removed during early surgical procedures. In
addition, specific teeth are absent on the non-cleft
side at rates greater than occur in normal individuals,
which is of great interest in terms of etiology. Solis
et al [72] found that teeth adjacent to clefts had de-
layed maturation relative to their antimeres in the
same mouth and as compared with control values;
this information is important when determining the
optimal time for secondary bone grafts by ratings of

Fig. 9. Maxillary distraction in a patient with a cleft in the early mixed dentition stage. (A, B) Pretreatment. (C, D) After
advancement of the maxilla. (E, F) Pre- and postadvancement views of the dental occlusion. (G) Superposition of pre- and post-
treatment cephalometric tracings. (H, I) Fabrication of the attachment apparatus from an orthodontic headgear frame and
orthodontic bands.
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290 283

Fig. 9 (continued).
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290284

Fig. 10. Maxillary distraction in a mature patient with a cleft. (A–D) Pre- and post-treatment facial photos. (E–G) Initial, during
distraction, and post-treatment cephalometric radiographs. (H, I) Pre- and postdistraction dental occlusion.
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290 285

Fig. 10 (continued).
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290286

Fig. 11. (A–C) Tooth anomalies present in individuals with clefts may involve number, shape, size, color, timing of devel-
opment, or position.
C.A. Evans / Clin Plastic Surg 31 (2004) 271–290 287
root development. Characteristic malocclusions ac-
company each type of repaired cleft and these vary
from malocclusions occurring in comparable untreat-
ed individuals who have clefts.
Summary
Orthodontic strategies continue to evolve as new
methods and treatment concepts more directly ad-
dress the specific problems of patients who have
clefts. By continual review of treatment outcomes
and comparing outcomes with patients’ problem lists
and treatment objectives, clinicians will identify areas
of treatment needing improvement and formulate
hypotheses for future research.
Acknowledgments
The author thanks Adriana Da Silveira, Budi
Kusnoto, Keum-Ryung Kim, Leslie Heffez, Mimis
Cohen, John P. Kelly, and John B. Mulliken for their
participation in the treatments shown in this article.
References
[1] Marcusson A. Adult patients with treated complete
cleft lip and palate. Methodological and clinical studies.
Swed Dent J Suppl 2001;145:1–57.
[2] Vig KWL, Turvey TA. Orthodontic-surgical interaction
in the management of cleft lip and palate. Clin Plast
Surg 1985;12:735–48.
[3] Friede H, Katsaros C. Current knowledge in cleft lip
and palate treatment from an orthodontist’s point of
view. J Orofac Orthop 1998;59:313–30.
[4] Figueroa AA, Polley JW, Cohen M. Orthodontic man-
agement of the cleft lip and palate patient. Clin Plast
Surg 1993;20:733–53.
[5] Vig K, Turvey T, Fonseca RJ. Facial clefts and cranio-
synostosis, principles and management. Philadelphia:
WB Saunders; 1996.
[6] Shetye P, Evans C. Midfacial growth in adult unoper-
ated complete unilateral cleft lip and palate patients
(personal communication).
[7] Berkowitz S. Cleft lip and palate with an introduction
to other craniofacial anomalies: perspectives in man-
agement. San Diego, CA: Singular; 1996.
[8] Moller KT, Starr CD. Cleft palate: interdisciplinary
issues and treatment—for clinicians, by clinicians.
Austin, TX: Pro-Ed; 1993.

C.A. Evans / Clin Plastic Surg 31 (2004) 271–290288
[9] Bardach J, Morris HL. Multidisciplinary manage-
ment of cleft lip and palate. Philadelphia: WB Saun-
ders; 1990.
[10] Clifford E. The cleft palate experience: new perspec-
tives on management. Springfield, IL: Thomas; 1987.
[11] Kernahan DA, Rosenstein SW. Cleft lip and palate: a
system of management. Baltimore, MD: Williams &
Wilkins; 1990.
[12] Ross RB, Johnston MC. Cleft lip and palate. Hunting-
ton, NY: Krieger; 1978.
[13] Cooper Sr HK, Harding RL, Krogman WM, Mazaheri
M, Millard RT. Cleft palate and cleft lip: a team
approach to clinical management and rehabilitation of
the patient. Philadelphia: WB Saunders; 1979.
[14] Grabb WC, Rosenstein SW, Bzoch KR, editors. Cleft
lip and palate. Boston: Little, Brown; 1971.
[15] American Cleft Palate-Craniofacial Association.
Core curriculum for cleft lip/palate and other cra-
niofacial anomalies. Available at: http://www.
cleftpalate-cranio facial.org. AccessedOctober 7, 2003.
[16] American Cleft Palate-Craniofacial Association. Pa-
rameters for evaluation and treatment of patients with
cleft lip/palate or other craniofacial anomalies. Cleft
Palate Craniofac J 1993;30(Suppl):S1–13.
[17] Prahl-Anderson B. Dental treatment of predental and
infant patients with clefts and craniofacial anomalies.
Cleft Palate Craniofac J 2000;37:528–32.
[18] Grayson BH, Santiago PE, Brecht LE, Cutting CB. Pre-
surgical nasoalveolar molding in infants with cleft lip
and palate. Cleft Palate Craniofac J 1999;36:486–98.
[19] Nordin K-E, Larson O, Nylen B, Eklund G. Early bone
grafting in complete cleft lip and palate cases follow-
ing maxillofacial orthopedics, I – IV. Scand J Plast
Reconstr Surg 1983;17:33–50.
[20] Rosenstein S, Dado DV, Kernahan D, Griffith BH,
Grasseschi M. The case for early bone grafting in cleft
lip and palate: a second report. Plast Reconstr Surg
1991;87:644–54.
[21] Enemark H, Sindet-Pedersen S, Bundgaard M, Krantz
Simonsen K. Combined orthodontic-surgical treatment
of alveolar clefts. Ann Plast Surg 1988;21:127–33.
[22] Troxell JB, Fonseca RJ, Osbon DB. A retrospective
study of alveolar cleft grafting. J Oral Maxillofac Surg
1982;40:721–5.
[23] El Deeb M, Messer LB, Lehnert MW, Hebda TW,
Waite DE. Canine eruption into grafted bone in maxil-
lary alveolar cleft defects. Cleft Palate J 1982;19:9–16.
[24] Wolfe SA, Berkowitz S. The use of cranial bone grafts
in the closure of alveolar and anterior palatal clefts.
Plast Reconstr Surg 1983;72:659–71.
[25] Jackson IT, Scheker LR, Vandervord JG, McLennan
JG. Bone marrow grafting in the secondary closure
of alveolar-palatal defects in children. Br J Plast Surg
1981;34:422–5.
[26] Kalaaji A, Lilja J, Friede H, Elander A. Bone grafting
in the mixed and permanent dentition in cleft lip and
palate patients: long-term results and the role of the
surgeon’s experience. J Craniomaxillofac Surg 1996;
24:29–35.
[27] Da Silva Filho OG, Teles SG, Ozawa TO, Filho LC.
Secondary bone graft and eruption of the permanent
canine in patients with alveolar clefts: literature review
and case report. Angle Orthod 2000;70:174–8.
[28] Dewinter G, Quirynen M, Heidbuchel K, Verdonck A,
Willems G, Carels C. Dental abnormalities, bone graft
quality, and periodontal conditions in patients with
unilateral cleft lip and palate at different phase of
orthodontic treatment. Cleft Palate Craniofac J 2003;
40:343–50.
[29] Fanning EA. Effect of extraction of deciduous molars
on the formation and eruption of their successors.
Angle Orthod 1962;32:44–53.
[30] Shashua D, Omnell ML. Radiographic determination of
the position of the maxillary lateral incisor in the cleft
alveolus and parameters for assessing its habilitation
prospects. Cleft Palate Craniofac J 2000;37:21–5.
[31] Lilja J, Kalaaji A, Friede H, Elander A. Combined
bone grafting and delayed closure of the hard palate
in patients with unilateral cleft lip and palate: facili-
tation of lateral incisor eruption and evaluation of
indicators for timing of the procedure. Cleft Palate
Craniofac J 2000;37:98–105.
[32] Opitz C, Meier B, Stoll C, Subklew D. Radiographic
evaluation of the transplant bone height in patients
with clefts of the lip/alveolus/palate after secondary
bone grafting. J Orofac Orthop 1999;60:383–91.
[33] Yilmaz S, Kilic AR, Keles A, Efeoglu E. Reconstruc-
tion of an alveolar cleft for orthodontic tooth move-
ment. Am J Orthod Dentofacial Orthop 2000;117:
156–63.
[34] Rabie AB, Chay SH. Clinical applications of compos-
ite intramembranous bone grafts. Am J Orthod Dento-
facial Orthop 2000;117:375–83.
[35] Buschang PH, Porter C, Genecov E, Genecov D, Say-
ler KE. Facemask therapy of preadolescents with unilat-
eral cleft lip and palate. Angle Orthod 1994;64:145–50.
[36] Tindlund RS. Skeletal response to maxillary protrac-
tion in patients with cleft lip and palate before age
10 years. Cleft Palate Craniofac J 1994;31:295–308.
[37] So LL. Effects of reverse headgear treatment on sagit-
tal correction in girls born with unilateral complete
cleft lip and cleft palate—skeletal and dental changes.
Am J Orthod Dentofacial Orthop 1996;109:140–7.
[38] Ishikawa H, Kitazawa S, Iwasaki H, Nakamura S.
Effects of maxillary protraction combined with chin-
cap therapy in unilateral cleft lip and palate patients.
Cleft Palate Craniofac J 2000;37:92–7.
[39] Kawakami M, Yagi T, Takada K. Maxillary expansion
and protraction in correction of midface retrusion in a
complete unilateral cleft lip and palate patient. Angle
Orthod 2002;72:355–61.
[40] Singer SL, Henry PJ, Rosenberg I. Osteointegrated
implants as an adjunct to facemask therapy: a case
report. Angle Orthod 2000;70:253–62.
[41] Mao JJ. Mechanobiology of craniofacial sutures. J Dent
Res 2002;81:810–6.
[42] Byrd HS. Cleft lip I: primary deformities. Selected
Readings Plast Surg 1987;4:1–26.

C.A. Evans / Clin Plastic Surg 31 (2004) 271–290 289
[43] Northway WM, Meade Jr JB. Surgically assisted
rapid maxillary expansion: a comparison of tech-
nique, response, and stability. Angle Orthod 1997;
67:309–20.
[44] Pogrel MA, Kaban LB, Vargervik K, Baumrind S. Sur-
gically assisted rapid maxillary expansion in adults. Int
J Adult Orthod Orthognath Surg 1992;7:37–41.
[45] Heidbuchel KL, Kuijpers-Jagtman AM, Freihofer HP.
An orthodontic and cephalometric study on the results
of the combined surgical-orthodontic approach of the
protruded premaxilla in bilateral clefts. J Craniomaxil-
lofac Surg 1993;21:60–6.
[46] Brouns J, Egyedi P. Osteotomy of the premaxilla.
J Maxillofac Surg 1980;8:182–6.
[47] Marsh JL, Galic M. Maxillofacial osteotomies for pa-
tients with cleft lip and palate. Clin Plast Surg 1989;
16:803–13.
[48] Posnick JC, Tompson B. Cleft-orthognathic surgery:
complications and long-term results. Plast Reconstr
Surg 1995;96:255–66.
[49] Rosen HM. Segmental osteotomies of the maxilla. Clin
Plast Surg 1989;16:785–94.
[50] Neal HA. Reconstruction of the maxillary alveolar cleft
palate. In: Sheldon DW, Irby WB, editors. Current
advances in oral and maxillofacial surgery: orthog-
nathic surgery, vol. 5. St. Louis, MO: Mosby; 1986.
p. 229–87.
[51] Yen SL-K, Gross J, Wang P, Yamashita D-D. Closure
of a large alveolar cleft by bony transport of a poste-
rior segment using orthodontic archwires attached to
bone: report of a case. J Oral Maxillofac Surg 2001;59:
688–91.
[52] Liou EJ, Chen PK, Huang CS, Chen YR. Interdental
distraction osteogenesis and rapid orthodontic tooth
movement: a novel approach to approximate a wide
alveolar cleft or bony defect. Plast Reconstr Surg
2000;105:1262–72.
[53] Molina F, Ortiz Monasterio F, de la Paz Aguilar M,
Barrera J. Maxillary distraction: aesthetic and func-
tional benefits in cleft lip-palate and prognathic pa-
tients during the mixed dentition. Plast Reconstr Surg
1998;101:951–63 [comment: 1999;103:1090].
[54] Figueroa AA, Polley JW, Ko EW. Maxillary distraction
for the management of cleft maxillary hypoplasia with
a rigid external distraction system. Semin Orthod 1999;
5:46–51.
[55] Swennen G, Colle F, De May A, Malevez C. Maxillary
distraction in cleft lip palate patients: a review of six
cases. J Craniofac Surg 1999;10:117–22.
[56] Heliovaara A, Ranta R, Hukki J, Rintala A. Skeletal
stability of Le Fort I osteotomy in patients with isolated
cleft palate and bilateral cleft lip and palate. Int J Oral
Maxillofac Surg 2002;31:358–63.
[57] Gaukroger MJ, Bounds G, Noar JH. The use of a face
mask for postoperative retention in cleft lip and palate
patients. Int J Adult Orthod Orthognath Surg 2000;15:
114–8.
[58] Han B-J, Suzuki A, Tashiro H. Longitudinal study of
craniofacial growth in subjects with cleft lip and pal-
ate: from cheiloplasty to 8 years of age. Cleft Palate
Craniofac J 1995;32:156–66.
[59] Ross RB. Treatment variables affecting facial growth
in complete unilateral cleft lip and palate. Part 7: an
overview of treatment and facial growth. Cleft Palate J
1989;24:71–7.
[60] Rosenstein SW, Grasseschi M, Dado DV. A long-term
retrospective outcome assessment of facial growth,
secondary surgical need, and maxillary lateral incisor
status in a surgical-orthodontic protocol for complete
clefts. Plast Reconstr Surg 2003;111:1–13.
[61] Hathaway RR, Eppley BL, Hennon DK, Nelson CL,
Sadove AM. Primary alveolar cleft bone grafting in
unilateral cleft lip and palate: arch dimensions at
age 8. J Craniofac Surg 1999;10:58–67, 68–72.
[62] Berkowitz S. A comparison of treatment results in
complete bilateral cleft lip and palate using a con-
servative approach versus Millard-Latham PSOT pro-
cedure. Semin Orthod 1996;2:169–84.
[63] HenkelKO,GundlachKK.Analysis of primary gingivo-
periosteoplasty in alveolar cleft repair. Part I: facial
growth. J Craniomaxillofac Surg 1997;25:266–9.
[64] Roberts-Harry D, Semb G, Hathorn I, Killingback N.
Facial growth in patients with unilateral clefts of the lip
and palate: a two-center study. Cleft Palate Craniofac J
1996;33:489–93.
[65] Wood RJ, Grayson BH, Cutting CB. Gingivoperiosteo-
plasty and midfacial growth. Cleft Palate Craniofac J
1997;34:17–20 [comment: 363–4].
[66] Levitt T, Long Jr RE, Trotman CA. Maxillary growth
in patientswith clefts following secondary alveolar bone
grafting. Cleft Palate Craniofac J 1999;36:398–406.
[67] Evans CA. Index may show outcome differences in
unilateral cleft lip and palate patients at 5-years of
age [commentary]. Evidence Based Dent 1999;1:7.
[68] Kalha AS. Are there characteristic features of the
craniofacial skeleton in parents of children who have
orofacial clefting (OFC)? Evidence-Based Dent 2003;
4:16.
[69] Perlyn CA, Brownstein JN, Huebener DV, Marsh JL,
Nissen RJ, Pilgram T. Occlusal relationship in patients
with bilateral cleft lip and palate during the mixed
dentition state: does neonatal maxillary arch configu-
ration predetermine outcome? Cleft Palate Craniofac J
2002;39:317–21.
[70] Pfeifer TM, Grayson BH, Curring CB. Nasoalveolar
molding and gingivoperiosteoplasty versus alveolar
bone graft: an outcome analysis of costs in the treat-
ment of unilateral cleft alveolus. Cleft Palate Craniofac
J 2002;39:26–9 [comment, discussion: 570–1].
[71] Suzuki A, Watanabe M, Nakano M, Takahama Y.
Maxillary lateral incisors of subjects with cleft lip
and/or palate: part 2. Cleft Palate Craniofac J 1992;
29:380–4.
[72] Solis A, Figueroa AA, Cohen M, Polley JW, Evans
CA. Maxillary dental development in complete unilat-
eral alveolar clefts. Cleft Palate Craniofac J 1998;35:
320–8.
[73] Vieira AR. Oral clefts and syndromic forms of tooth

C.A. Evans / Clin Plastic Surg 31 (2004) 271–290290
agenesis as models for genetics of isolated tooth agene-
sis. J Dent Res 2003;82:162–5.
[74] Shapira Y, Lubit E, Kuftinec MM. Hypodontia in chil-
dren with various types of clefts. Angle Orthod 2000;
70:16–21.
[75] Hellquist R, LinderAronson S, Norling M, Ponten B,
Stenberg T. Dental abnormalities in patients with al-
veolar clefts, operated upon with or without primary
periosteoplasty. Eur J Orthod 1979;1:169–80.
[76] Isono H, Kaida K, Hamada Y, Kokubo Y, Ishihara M,
Hirashita A, et al. The reconstruction of bilateral clefts
using endosseous implants after bone grafting. Am J
Orthod Dentofacial Orthop 2002;121:403–10.
[77] Melissaratou A, Friede H. Dental arches and occlusion
in bilateral cleft lip and palate patients after two differ-
ent routines for palatal surgery. J Orofac Orthop 2002;
63:300–14.
[78] Shapira Y, Lubit E, Kuftinec MM. Congenitally mis-
sing second premolars in cleft lip and cleft palate
children. Am J Orthod Dentofacial Orthop 1999;115:
396–400.